
The Impact of Respiratory Symptoms on the Risk of Serious Bacterial Infection in Febrile Infants < 60 Days Old
 , ,
, ,
Abstract
:
1. Introduction
2. Methods
2.1. Study Design
- Demographics: gender, age on admission, ethnicity, and Arab or Jew.
- Clinical data: presence of respiratory symptoms upon presentation (e.g., cough, wheezing, rhinorrhea) and clinical appearance (ill/appearing well) upon admission (judged by the ED physician upon presentation).
- Microbiological studies:
- Viral polymerase chain reaction (PCR) for the following viruses: RSV, influenza A, influenza B, parainfluenza, human metapneumovirus (HMPV), adenovirus, rhinovirus, and SARS-CoV-2.
- Blood cultures.
- Urine cultures.
- CSF cultures.
- Blood tests (taken on admission):
- White blood cell count (WBC); leukocytosis was defined as a WBC > 15,000/µL. C-reactive protein (CRP); a high CRP was defined as >2 mg/dL.
- Outcome: The main outcome was the diagnosis of SBIs based on microbiological reports. SBIs were defined by a diagnosis of bacteremia (positive blood culture), meningitis (positive CSF culture), or a UTI (urine culture with >10,000 colony-forming units/mL of uropathogens from a catheterized specimen or any growth from a supra-pubic aspiration [8]). The incidence of an invasive bacterial infection (IBI), defined as bacteremia or meningitis, was also examined. Blood and CSF cultures with the growth of commensal bacteria (e.g., coagulase-negative staphylococci, viridans streptococci, etc.) when the patient was not treated with antibiotics were considered contaminated.
2.2. Statistical Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huppler, A.R.; Eickhoff, J.C.; Wald, E.R. Performance of low-risk criteria in the evaluation of young infants with fever: Review of the literature. Pediatrics 2010, 125, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Bachur, R.G.; Harper, M.B. Predictive model for serious bacterial infections among infants younger than 3 months of age. Pediatrics 2001, 108, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Caspe, W.B.; Chamudes, O.; Louie, B. The evaluation and treatment of the febrile infant. Pediatr. Infect. Dis. J. 1983, 2, 131–135. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, C. Iatrogenic Risks and Financial Costs of Hospitalizing Febrile Infants. Arch. Pediatr. Adolesc. Med. 1983, 137, 1146. [Google Scholar] [CrossRef] [PubMed]
- Pantell, R.H.; Roberts, K.B.; Adams, W.G.; Dreyer, B.P.; Kuppermann, N.; O’leary, S.T.; Okechukwu, K.; Woods, C.R.; Infants, S.O.F. Clinical Practice Guideline: Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old. Pediatrics 2021, 148, e2021052228. [Google Scholar] [CrossRef] [PubMed]
- Smitherman, H.F.; Caviness, A.C.; Macias, C.G. Retrospective review of serious bacterial infections in infants who are 0 to 36 months of age and have influenza A infection. Pediatrics 2005, 115, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.A.; Platt, S.L.; Dayan, P.S.; Macias, C.G.; Zorc, J.J.; Krief, W.; Schor, J.; Bank, D.; Fefferman, N.; Shaw, K.N.; et al. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics 2004, 113, 1728–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Tekgül, S. Urinary Tract Infections in Children: EAU/ESPU Guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef]
- Greenfield, B.W.; Lowery, B.M.; Starke, H.E.; Mayorquin, L.; Stanford, C.; Camp, E.A.; Cruz, A.T. Frequency of serious bacterial infections in young infants with and without viral respiratory infections. Am. J. Emerg. Med. 2021, 50, 744–747. [Google Scholar] [CrossRef]
- Krief, W.I.; Levine, D.A.; Platt, S.L.; Macias, C.G.; Dayan, P.S.; Zorc, J.J.; Feffermann, N.; Kuppermann, N.; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Influenza Virus Infection and the Risk of Serious Bacterial Infections in Young Febrile Infants. Pediatrics 2009, 124, 30–39. [Google Scholar] [CrossRef]
- Mahajan, P.; Browne, L.R.; Levine, D.A.; Cohen, D.M.; Gattu, R.; Linakis, J.G.; Anders, J.; Borgialli, D.; Vitale, M.; Dayan, P.S.; et al. Risk of Bacterial Coinfections in Febrile Infants 60 Days Old and Younger with Documented Viral Infections. J. Pediatr. 2018, 203, 86–91.e2. [Google Scholar] [CrossRef]
- Committee on Infectious Diseases; Maldonado, Y.A.; Zaoutis, T.E.; Banerjee, R.; Barnett, E.D.; Campbell, J.D.; Caserta, M.T.; Gerber, J.S.; Kourtis, A.P.; Lynfield, R.; et al. Recommendations for prevention and control of influenza in children, 2019–2020. Pediatrics 2019, 144, e20192478. [Google Scholar] [CrossRef] [Green Version]
- Rogers, B.B.; Shankar, P.; Jerris, R.C.; Kotzbauer, D.; Anderson, E.J.; Watson, J.R.; O’Brien, L.A.; Uwindatwa, F.; McNamara, K.; Bost, J.E. Impact of a rapid respiratory panel test on patient outcomes. Arch. Pathol. Lab. Med. 2015, 139, 636–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.K.; Friedlander, S.; Fleischman, R.J.; Zangwill, K.M. Length of Stay and Complications Associated With Febrile Infants < 90 Days of Age Hospitalized in the United States, 2000–2012. Hosp. Pediatr. 2018, 8, 746–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibby, H.L.; de Koning, L.; Seiden-Long, I.; Zelyas, N.; Church, D.L.; Berenger, B.M. A pragmatic randomized controlled trial of rapid on-site influenza and respiratory syncytial virus PCR testing in paediatric and adult populations. BMC Infect. Dis. 2022, 22, 854. [Google Scholar] [CrossRef]
- Orfanos, I.; Alfvén, T.; Mossberg, M.; Tenland, M.; Fernandez, J.S.; Eklund, E.A.; Elfving, K. Age- and sex-specific prevalence of serious bacterial infections in febrile infants ≤60 days, in Sweden. Acta Paediatr. 2021, 110, 3069–3076. [Google Scholar] [CrossRef] [PubMed]
- Prais, D.; Shoov-Furman, R.; Amir, J. Is ritual circumcision a risk factor for neonatal urinary tract infections? Arch. Dis. Child. 2009, 94, 191–194. [Google Scholar] [CrossRef]
- Oray-Schrom, P.; Phoenix, C.; St Martin, D.; Amoateng-Adjepong, Y. Sepsis Workup in Febrile Infants 0–90 Days of Age With Respiratory Syncytial Virus Infection. Pediatr. Emerg. Care 2003, 19, 314–319. [Google Scholar] [CrossRef]
- Coyle, C.; Brock, G.; Wallihan, R.; Leonard, J.C. Cost Analysis of Emergency Department Criteria for Evaluation of Febrile Infants Ages 29 to 90 Days. J. Pediatr. 2021, 231, 94–101.e2. [Google Scholar] [CrossRef]
- Aronson, P.L.; McCulloh, R.J.; Tieder, J.S.; Nigrovic, L.E.; Leazer, R.C.; Alpern, E.R.; Feldman, E.A.; Balamuth, F.; Browning, W.L.; Neuman, M.I. Application of the Rochester Criteria to Identify Febrile Infants With Bacteremia and Meningitis. Pediatr. Emerg. Care 2019, 35, 22–27. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Young, B.R.; Alabaster, A.; Vinson, D.R.; Mark, D.G.; Van Winkle, P.; Sharp, A.L.; Shan, J.; Rauchwerger, A.S.; Greenhow, T.L.; et al. Using AAP Guidelines for Managing Febrile Infants Without C-Reactive Protein and Procalcitonin. Pediatrics 2022, 151, e2022058495. [Google Scholar] [CrossRef]
- Harper, M.B. Update on the management of the febrile infant. Clin. Pediatr. Emerg. Med. 2004, 5, 5–12. [Google Scholar] [CrossRef]
- Burstein, B.; Alathari, N.; Papenburg, J. Guideline-Based Risk Stratification for Febrile Young Infants Without Procalcitonin Measurement. Pediatrics 2022, 149, e2021056028. [Google Scholar] [CrossRef] [PubMed]
- Kuppermann, N.; Mahajan, P.; Dayan, P.S. Fever, Absolute Neutrophil Count, Procalcitonin, and the AAP Febrile Infant Guidelines. Pediatrics 2023, 151, e2022059862. [Google Scholar] [CrossRef]
- Shen, Z.; Zhang, Y.; Li, H.; Du, L. Rapid typing diagnosis and clinical analysis of subtypes A and B of human respiratory syncytial virus in children. Virol. J. 2022, 19, 15. [Google Scholar] [CrossRef]
- Lee, J.S.; Ahn, J.J.; Kim, S.J.; Yu, S.Y.; Koh, E.J.; Sung, H.S.; Huh, J.W.; Hwang, S.Y. POCT Detection of 14 Respiratory Viruses Using Multiplex RT-PCR. Biochip. J. 2021, 15, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Srugo, I.; Klein, A.; Stein, M.; Golan-Shany, O.; Kerem, N.; Chistyakov, I.; Genizi, J.; Glazer, O.; Yaniv, L.; German, A.; et al. Validation of a novel assay to distinguish bacterial and viral infections. Pediatrics 2017, 140, e20163453. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
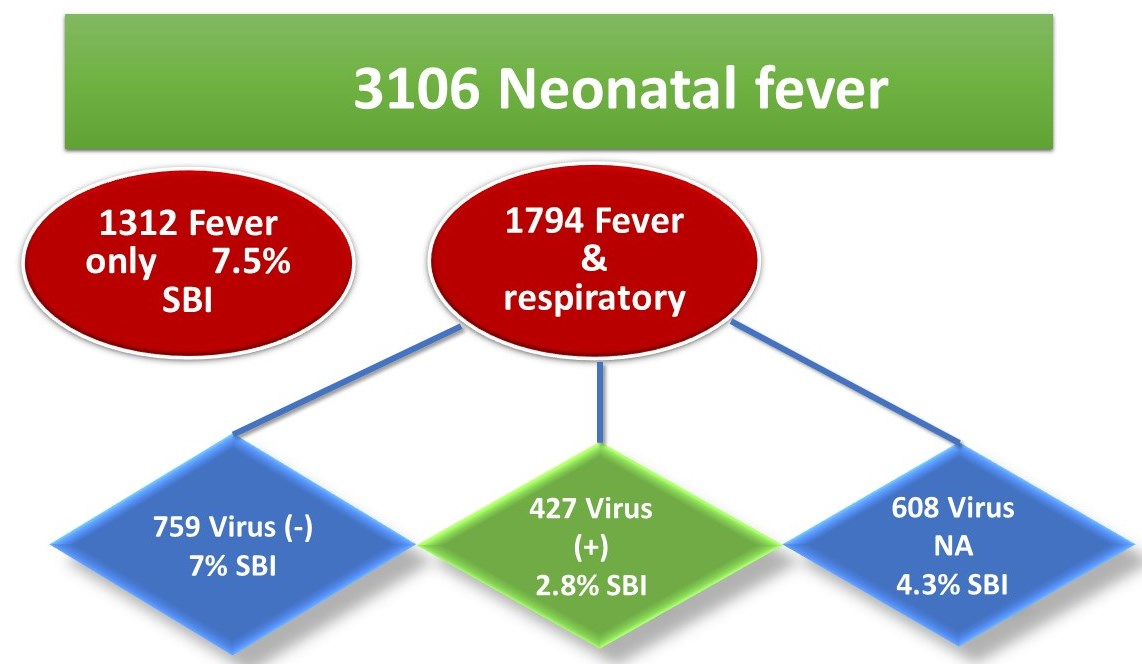
| Fever Only (n = 1312) | Fever and Resp, Virus (−) (n = 759) | Fever and Resp, Virus (+) (n = 427) | Fever and Resp, Virus NA (n = 608) | p-Value | |
|---|---|---|---|---|---|
| SBI | 99 (7.5) Reference | 53 (7.0) p-value * = 0.516 | 12 (2.8) p-value * = 0.001 OR = 0.35 95% CI = 0.19–0.65 | 26 (4.3) p-value * = 0.005 OR = 0.49 95% CI = 0.29–0.81 | 0.001 |
| IBI Bacteremia Meningitis | 21 (1.6) 20 (1.6) 6 (1.6) | 14 (1.8) 12 (1.6) 3 (1.0) | 2 (0.5) 1 (0.3) 1 (0.9) | 9 (1.5) 9 (1.7) 1 (0.9) | 0.282 0.247 NA |
| UTI | 83 (6.8) Reference | 40 (5.5) p-value * = 0.203 | 10 (3.0) p-value * = 0.010 OR = 0.43 95% CI = 0.22–0.83 | 19 (3.8) p-value * = 0.017 OR = 0.49 95% CI = 0.27–0.89 | 0.014 |
| P Uni (χ2 Test) | P Multi (Binary Regression) | Adjusted OR (95% CI) | |
|---|---|---|---|
| Gender—male | 0.002 | 0.056 | 1.49 (0.99–2.25) |
| Age < 1 month | 0.000 | 0.000 | 2.74 (1.83–4.10) |
| WBC > 15,000 | 0.000 | 0.000 | 2.64 (1.74–3.99) |
| CRP > 2 mg/dL | 0.000 | 0.000 | 4.78 (3.19–7.15) |
| Fever w/o respiratory | 0.004 | 0.001 | 1.92 (1.29–2.85) |
| Fever Only Total = 1312 N (%) | Fever and Respiratory Total = 1794 N (%) | p-Value * | OR (95% CI) | |||
|---|---|---|---|---|---|---|
| No SBI N (%) | SBI N (%) | No SBI N (%) | SBI N (%) | |||
| Whole cohort | 1213 (92.5) | 99 (7.5) | 1703 (94.9) | 91 (5.1) | 0.004 | 0.65 (0.49–0.88) |
| Gender, male | 673 (90.7) | 69 (9.3) | 971 (94.2) | 60 (5.8) | 0.005 | 0.60 (0.42–0.86) |
| Gender, female | 540 (94.7) | 30 (5.3%) | 732 (95.9) | 31 (4.1) | 0.300 | |
| Age < 1 m | 487 (87) | 73 (13) | 610 (91.5) | 57 (8.5) | 0.011 | 0.62 (0.43–0.9) |
| Age 1–2 m | 726 (96.5) | 26 (3.5) | 1093 (97) | 34 (3) | 0.595 | |
| Ethnicity, Jew | 717 (92.2) | 61 (7.8) | 1085 (94.9) | 58 (5.1) | 0.014 | 0.63 (0.43–0.91) |
| Ethnicity, Arab | 482 (94.9) | 26 (5.1) | 399 (93) | 30 (7) | 0.228 | |
| WBC < 15,000/μL a | 877 (95) | 46 (5) | 1232 (96) | 51 (4) | 0.254 | |
| WBC > 15,000/μL | 185 (78.7) | 50 (21.3) | 236 (88.4) | 31 (11.6) | 0.003 | 0.49 (0.30–0.74) |
| CRP < 2 mg/dL b | 366 (95.8) | 16 (4.2) | 872 (96) | 36 (4) | 0.852 | |
| CRP > 2 mg/dL | 87 (65.4) | 46 (34.6) | 253 (88.5) | 33 (11.5) | <0.001 | 0.25 (0.15–0.41) |
| Appears ill | 63 (91.3) | 6 (8.7) | 99 (92.5) | 8 (7.5) | 0.770 | |
| Appears well | 981 (92.1) | 84 (7.9) | 1571 (95) | 83 (5) | 0.002 | 0.62 (0.45–0.84) |
| Discharge | 218 (93.2) | 16 (6.8) | 330 (97.1) | 10 (2.9) | 0.027 | 0.41 (0.13–0.93) |
| Hospitalization | 995 (92.3) | 83 (7.7) | 1373 (94.4) | 81 (5.6) | 0.031 | 0.70 (0.51–0.97) |
| LOS (days) | 3.6 ± 4.9 | 3.1 ± 2.5 | 3.4 ± 4.4 | 3.3 ± 3.2 | 0.540 | |
| PICU admission | 68 (5.6) | 4 (4) | 80 (4.7) | 3 (3.3) | 0.393 | |
| Fever and Resp Virus (−) Total = 759 N (%) | Fever and Resp Virus (+) Total = 427 N (%) | |||||
|---|---|---|---|---|---|---|
| No SBI N (%) | SBI N (%) | No SBI N (%) | SBI N (%) | p-Value * | OR (95% CI) | |
| Whole cohort | 706 (93) | 51 (7) | 415 (97.2) | 12 (2.8) | 0.002 | 0.39 (0.2–0.73) |
| Gender, male | 408 (92.1) | 35 (7.9) | 232 (97.1) | 7 (2.9) | 0.01 | 0.35 (0.15–0.80) |
| Gender, female | 298 (94.3) | 18 (5.7) | 183 (97.3) | 5 (2.7) | 0.14 | |
| Age < 1 m | 291 (90.4) | 31 (9.6) | 155 (95.7) | 7 (4.3) | 0.041 | 0.42 (0.18–0.99) |
| Age 1–2 m | 415 (95) | 22 (5) | 260 (98.1) | 5 (1.9) | 0.036 | 0.36 (0.14–0.97) |
| Ethnicity, Jews | 491 (93.5) | 34 (6.5) | 249 (97.3) | 7 (2.7) | 0.028 | 0.40 (0.18–0.93) |
| Ethnicity, Arabs | 158 (92.4) | 13 (7.6) | 136 (96.5) | 5 (3.5) | 0.126 | |
| WBC < 15,000/μL a | 542 (94.4) | 32 (5.6) | 293 (97.7) | 7 (2.3) | 0.028 | 0.40 (0.18–0.93) |
| WBC > 15,000/μL | 124 (87.3) | 18 (12.7) | 42 (93.3) | 3 (6.7) | 0.266 | |
| CRP > 2 mg/dL b | 504 (95.5) | 24 (4.5) | 206 (96.7) | 7 (3.3) | 0.438 | |
| CRP > 2 mg/dL | 116 (82.9) | 24 (17.1) | 84 (97.7) | 2 (2.3) | 0.001 | 0.12 (0.03–0.50) |
| Appears ill | 24 (85.7) | 4 (14.3) | 44 (93.6) | 3 (6.4) | 0.413 | |
| Appears well | 678 (93.3) | 49 (6.7) | 366 (97.6) | 9 (2.4) | 0.002 | 0.34 (0.17-0.70) |
| Discharge | 132 (96.4) | 5 (3.6) | 71 (98.6) | 1 (1.4) | NA | |
| Hospitalization | 574 (92.3) | 48 (7.7) | 344 (96.9) | 11 (3.1) | 0.004 | 0.38 (0.2-0.75) |
| LOS (days) | 3.3 ± 4.4 | 3.5 ± 3.5 | 3.6 ± 4.4 | 2.8 ± 1.4 | 0.541 | |
| PICU admission | 31 (4.4) | 1 (1.9) | 23 (5.5) | 1 (8.3) | 0.764 ** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarweh, K.; Bentur, L.; Bar-Yoseph, R.; Kassis, I.; Dabaja-Younis, H.; Gur, M. The Impact of Respiratory Symptoms on the Risk of Serious Bacterial Infection in Febrile Infants < 60 Days Old. J. Clin. Med. 2023, 12, 4636. https://doi.org/10.3390/jcm12144636
Masarweh K, Bentur L, Bar-Yoseph R, Kassis I, Dabaja-Younis H, Gur M. The Impact of Respiratory Symptoms on the Risk of Serious Bacterial Infection in Febrile Infants < 60 Days Old. Journal of Clinical Medicine. 2023; 12(14):4636. https://doi.org/10.3390/jcm12144636
Chicago/Turabian StyleMasarweh, Kamal, Lea Bentur, Ronen Bar-Yoseph, Imad Kassis, Halima Dabaja-Younis, and Michal Gur. 2023. "The Impact of Respiratory Symptoms on the Risk of Serious Bacterial Infection in Febrile Infants < 60 Days Old" Journal of Clinical Medicine 12, no. 14: 4636. https://doi.org/10.3390/jcm12144636