

Determination of Correlated Color Temperature in Ex Vivo Porcine Eyes during Intraocular Illumination


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gea, M.; Schilirò, T.; Iacomussi, P.; Degan, R.; Bonetta, S.; Gilli, G. Cytotoxicity and genotoxicity of light emitted by incandescent, halogen, and LED bulbs on ARPE-19 and BEAS-2B cell lines. J. Toxicol. Environ. Health A 2018, 81, 998–1014. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Meyer, C.H. A trichrome RGB endoillumination prototype system: A novel application for chromovitrectomy. Ophthalmologica 2013, 230 (Suppl. S2), 73–76. [Google Scholar] [CrossRef]
- Brambilla, A.; Hu, W.; Samangouei, R.; Cadorin, R.; Davis, W. How correlated colour temperature manipulates human thermal perception and comfort. Build. Environ. 2020, 177, 106929. [Google Scholar] [CrossRef]
- Chaopu, Y.; Wenqing, F.; Jiancheng, T.; Fan, Y.; Yanfeng, L.; Chun, L. Change of blue light hazard and circadian effect of LED backlight displayer with color temperature and age. Opt. Express 2018, 26, 27021–27032. [Google Scholar] [CrossRef] [PubMed]
- Mohammadian, F.; Mehri, A.; Abedi, K.; Ebrahimi, H.; Laal, F.; Falahi, H. A Simplified Approach to Evaluate Retinal Blue Light Hazard Using the Correlated Color Temperature of LED Light Sources. J. Environ. Health Sci. Eng. 2021, 9, 299–310. [Google Scholar] [CrossRef]
- Bullough, J.D.; Bierman, A.; Rea, M.S. Evaluating the blue-light hazard from solid state lighting. Int. J. Occup. Saf. Ergon. 2019, 25, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Li, X.; Yan, F.; Chen, W.; Jiang, L.; Zhang, X. The effects of low-color-temperature dual-primary-color light-emitting diodes on three kinds of retinal cells. J. Photochem. Photobiol. B Biol. 2021, 214, 112099. [Google Scholar] [CrossRef]
- Xie, C.; Zhu, H.; Chen, S.; Wen, Y.; Jin, L.; Zhang, L.; Tong, J.; Shen, Y. Chronic retinal injury induced by white LED light with different correlated color temperatures as determined by microarray analyses of genome-wide expression patterns in mice. J. Photochem. Photobiol. B Biol. 2020, 210, 111977. [Google Scholar] [CrossRef] [PubMed]
- Litorja, M.; Brown, S.; Ohno, Y.; Lin, C. Illumination with Enhanced Contrast as a Visualization Tool for Clinical Diagnostics and Surgery; Litorja, M., Brown, S., Ohno, Y., Lin, C., Eds.; Biomedical Optics: San Jose, CA, USA, 2009. [Google Scholar]
- Argyraki, A.; Clemmensen, L.K.H.; Petersen, P.M. Does correlated color temperature affect the ability of humans to identify veins? J. Opt. Soc. Am. A 2016, 33, 141–148. [Google Scholar] [CrossRef]
- Hürzeler, D. Blue light endoscopy. Laryngoscope 1975, 85, 1374–1378. [Google Scholar] [CrossRef]
- Gono, K.; Obi, T.; Yamaguchi, M.; Ohyama, N.; Machida, H.; Sano, Y.; Yoshida, S.; Hamamoto, Y.; Endo, T. Appearance of enhanced tissue features in narrow-band endoscopic imaging. J. Biomed. Opt. 2004, 9, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Litorja, M.; Brown, S.W.; Nadal, M.E.; Allen, D.; Gorbach, A. Development of surgical lighting for enhanced color contrast. In Proceedings of the SPIE—The International Society for Optical Engineering, San Diego, CA, USA, 17–22 February2007; Volume 6515, pp. 65150K-1–65150K-11. [Google Scholar] [CrossRef]
- Charles, S. Illumination and phototoxicity issues in vitreoretinal surgery. Retina 2008, 28, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sarao, V.; Veritti, D.; Borrelli, E.; Sadda, S.V.R.; Poletti, E.; Lanzetta, P. A comparison between a white LED confocal imaging system and a conventional flash fundus camera using chromaticity analysis. BMC Ophthalmol. 2019, 19, 231. [Google Scholar] [CrossRef] [PubMed]
- Mundinger, J.J.; Houser, K.W. Adjustable correlated colour temperature for surgical lighting. Light. Res. Technol. 2019, 51, 280–290. [Google Scholar] [CrossRef]
- Koelbl, P.S.; Sieber, N.; Lingenfelder, C.; Koch, F.H.J.; Deuchler, S.; Hessling, M. Pressure dependent direct transtissue transmission of eyewall, sclera and vitreous body in the range of 350–1050 nm. Z. Med. Phys. 2020, 30, 201–210. [Google Scholar] [CrossRef]
- Fehler, N.; Lingenfelder, C.; Kupferschmid, S.; Hessling, M. Intraocular reflectance of the ocular fundus and its impact on increased retinal hazard. Zeitschrift für Medizinische Physik 2022, 32, 453–465. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Dlugos, C.; Nuffer, R.; Birngruber, R. Optical properties of human sclera, and their consequences for transscleral laser applications. Lasers Surg. Med. 1991, 11, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Sieber, N.; Kölbl, P.; Lingenfelder, C.; Stucke-Straub, K.; Kupferschmid, S.; Hessling, M. Measurement of the retinal irradiation exposure during diaphanoscopic illumination. Curr. Dir. Biomed. Eng. 2020, 6, 276–279. [Google Scholar] [CrossRef]
- Chan, E.K.; Sorg, B.; Protsenko, D.; O’Neil, M.; Motamedi, M.; Welch, A.J. Effects of compression on soft tissue optical properties. IEEE J. Sel. Top. Quantum Electron. 1996, 2, 943–950. [Google Scholar] [CrossRef]
- Koelbl, P.S.; Klante, P.; Koch, F.; Lingenfelder, C.; Werner, J.U.; Enders, C.; Hessling, M. Location and pressure dependent transmission of human and porcine sclera: An anterior to posterior examination. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 2185–2198. [Google Scholar] [CrossRef] [PubMed]
- Hessling, M.; Koelbl, P.S.; Lingenfelder, C.; Koch, F. Miniature LED Endoilluminators For Vitreoretinal Surgery. In Medical Laser Applications and Laser-Tissue Interactions VII: Proceedings of the European Conference on Biomedical Optics 2015, Munich, Germany, 21–25 June 2015; SPIE Proceedings Paper 95421A; Optica Publishing Group: Washington, DC, USA, 2015; Volume 9542. [Google Scholar]
- Nicoli, S.; Ferrari, G.; Quarta, M.; Macakuso, C.; Govoni, P.; Dallatana, D.; Santi, P. Porcine sclera as a model of human sclera for in vitro transport experiments histology, SEM, and comparative permeability. Mol. Vis. 2009, 15, 259–266. [Google Scholar] [PubMed]
- Sanchez, I.; Martin, R.; Ussa, F.; Fernandez-Bueno, I. The parameters of the porcine eyeball. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 475–482. [Google Scholar] [CrossRef]
- Beauchemin, M.L. The fine structure of the pig′s retina. Graefes Arch. Clin. Exp. Ophthalmol. 1974, 190, 27–45. [Google Scholar] [CrossRef]
- Olsen, T.W.; Sanderson, S.; Feng, X.; Hubbard, W.C. Porcine sclera: Thickness and surface area. Investig. Ophthalmol. Vis. Sci. 2002, 43, 2529–2532. [Google Scholar]
- De Schaepdrijver, L.; Simoens, P.; Pollet, L.; Lauwers, H.; De Laey, J.-J. Morphologic and clinical study of the retinal circulation in the miniature pig. B: Fluorescein angiography of the retina. Exp. Eye Res. 1992, 54, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Chandler, M.J.; Smith, P.J.; Samuelson, D.A.; MacKay, E.O. Photoreceptor density of the domestic pig retina. Vet. Ophthalmol. 1999, 2, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Koelbl, P.S.; Werner, J.U.; Enders, C.; Lingenfelder, C.; Koch, F.H.J.; Hessling, M. Short-Term Intraocular Pressure Rise during Locally Induced Force by Ophthalmologic Surgery Applications. Ophthalmic Res. 2019, 61, 159–167. [Google Scholar] [CrossRef]
- Fehler, N.; Lingenfelder, C.; Kupferschmid, S.; Hessling, M. Determination of the intraocular irradiance and potential retinal hazards at various positions in the eye during transscleral equatorial illumination for different applied pressures. Z. Med. Phys. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bashkatov, A.N.; Tuchin, V.V.; Genina, E.A.; Sinichkin, Y.P.; Lakodina, N.A.; Kochubey, V.I. Human sclera dynamic spectra: In-vitro and in-vivo measurements. In Proceedings of the SPIE 3591, Ophthalmic Technologies IX, San Jose, CA, USA, 18 June 1999; Volume 3591, p. 311. [Google Scholar] [CrossRef]
- Smith, R.S.; Stein, M.N. Ocular Hazards of Transscleral Laser Radiation. Am. J. Ophtalmol. 1968, 66, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Menon, I.A.; Wakeham, D.C.; Persad, S.D.; Avaria, M.; Trope, G.E.; Basu, P.K. Quantitative determination of the melanin contents in ocular tissues from human blue and brown eyes. J. Ocul. Pharmacol. Ther. 1992, 8, 35–42. [Google Scholar] [CrossRef]
- Durairaj, C.; Chastain, J.E.; Kompella, U.B. Intraocular distribution of melanin in human, monkey, rabbit, minipig and dog eyes. Exp. Eye Res. 2012, 98, 23–27. [Google Scholar] [CrossRef]
- Bashkatov, A.N.; Genina, E.A.; Kochubey, V.I.; Tuchin, V.V. Optical properties of human sclera in spectral range 370–2500 nm. Opt. Spectrosc. 2010, 109, 197–204. [Google Scholar] [CrossRef]
- Rönnerstam, R. Fundus Examination Using Transscleral Illumination. Graefes Arch. Clin. Exp. Ophthalmol. 1977, 201, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.H. Study of transillumination of the eye. Arch. Ophthalmol. 1939, 22, 653–666. [Google Scholar] [CrossRef]
- Terasaki, H.; Miyake, Y.; Awaya, S.; Arai, M.; Ando, F.; Kyogane, I. Identification of Anterior Uveal Tumor Border by Transscleral Transillumination and an Ophthalmic Endoscope. Am. J. Ophthalmol. 1997, 123, 138–140. [Google Scholar] [CrossRef]
- Laqua, H.; Völcker, H.E. Pars plana vitrectomy in eyes with malignant melanoma. Graefes Arch. Clin. Exp. Ophthalmol. 1983, 220, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Finger, P.T.; Iezzi, R.; Romero, J.M.; Rosen, R.B.; Szechter, A.; Hegde, H. Plaque-mounted diode-light transillumination for localization around intraocular tumors. Arch. Ophthalmol. 1999, 117, 179–183. [Google Scholar] [CrossRef]
- Krohn, J.; Seland, J.H.; Monge, O.R.; Rekstad, B.L. Transillumination for accurate placement of radioactive plaques in brachytherapy of choroidal melanoma. Am. J. Ophthalmol. 2001, 132, 418–419. [Google Scholar] [CrossRef]
- Wecker, T.; Jordan, J.F.; van Oterendorp, C. Diaphanoskopie bei der Zyklophotokoagulation. Ophthalmologe 2016, 113, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.C.; Nietgen, G.W.; Hesse, L.; Kroll, P. External diaphanoscopic illuminator: A new device for visualization in pars plana vitrectomy. Retina 2000, 20, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Veckeneer, M.; Wong, D. Visualising vitreous through modified trans-scleral illumination by maximising the Tyndall effect. Br. J. Ophthalmol. 2009, 93, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.H.; Scholtz, S.; Koss, M.; Krueger, H.; Lambert, M.; Al Saraireh, F.; Al-Ahmar, Y.; Pfister, M.; Deuchler, S.; Singh, P. External Illumination Options for Vitreoretinal Service Provided in the Operating Room, an Ambulatory Surgery Center or in the Office. Investig. Ophthalmol. Vis. Sci. 2011, 52, 544. [Google Scholar]
- Shanmugam, P.M.; Ramanjulu, R.; Mishra, K.C.D.; Sagar, P. Novel techniques in scleral buckling. Indian J. Ophthalmol. 2018, 66, 909–915. [Google Scholar] [CrossRef]
- Mariacher, S.; Khalil, H.; Bolz, M. Enhancing scleral buckling surgery using an illuminated scleral depressor. Retina 2021. [Google Scholar] [CrossRef]
- Lytvynchuk, L.M.; Grzybowski, A.; Lorenz, B.; Ansari-Shahrezaei, S.; Binder, S. New Scleral Depressor Marker for Retinal Detachment Surgery. Ophthalmol. Retin. 2019, 3, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Ham, W.T.; Mueller, H.A.; Sliney, D.H. Retinal sensitivity to damage from short wavelength light. Nature 1976, 260, 153–155. [Google Scholar] [CrossRef]
- Ham, W.T.; Ruffolo, J.J.; Mueller, H.A.; Clarke, A.M.; Moon, M.E. Histologic analysis of photochemical lesions produced in rhesus retina by short-wave-length light. Investig. Ophthalmol. Vis. Sci. 1978, 17, 1029–1035. [Google Scholar]
- Ueda, T.; Nakanishi-Ueda, T.; Yasuhara, H.; Koide, R.; Dawson, W.W. Eye damage control by reduced blue illumination. Exp. Eye Res. 2009, 89, 863–868. [Google Scholar] [CrossRef]
- Shang, Y.-M.; Wang, G.-S.; Sliney, D.H.; Yang, C.-H.; Lee, L.-L. Light-emitting-diode induced retinal damage and its wavelength dependency in vivo. Int. J. Ophthalmol. 2017, 10, 191–202. [Google Scholar] [CrossRef]
- ISO 15004-2:2007; DIN Deutsches Institut für Normung e. V. Ophthalmische Instrumente—Grundlegende Anforderungen und Prüfverfahren-Teil 2: Schutz Gegen Gefährdung Durch Licht. Deutsche Fassung EN ISO 15004-2:2007. Beuth Verlag GmbH: Berlin, Germany, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
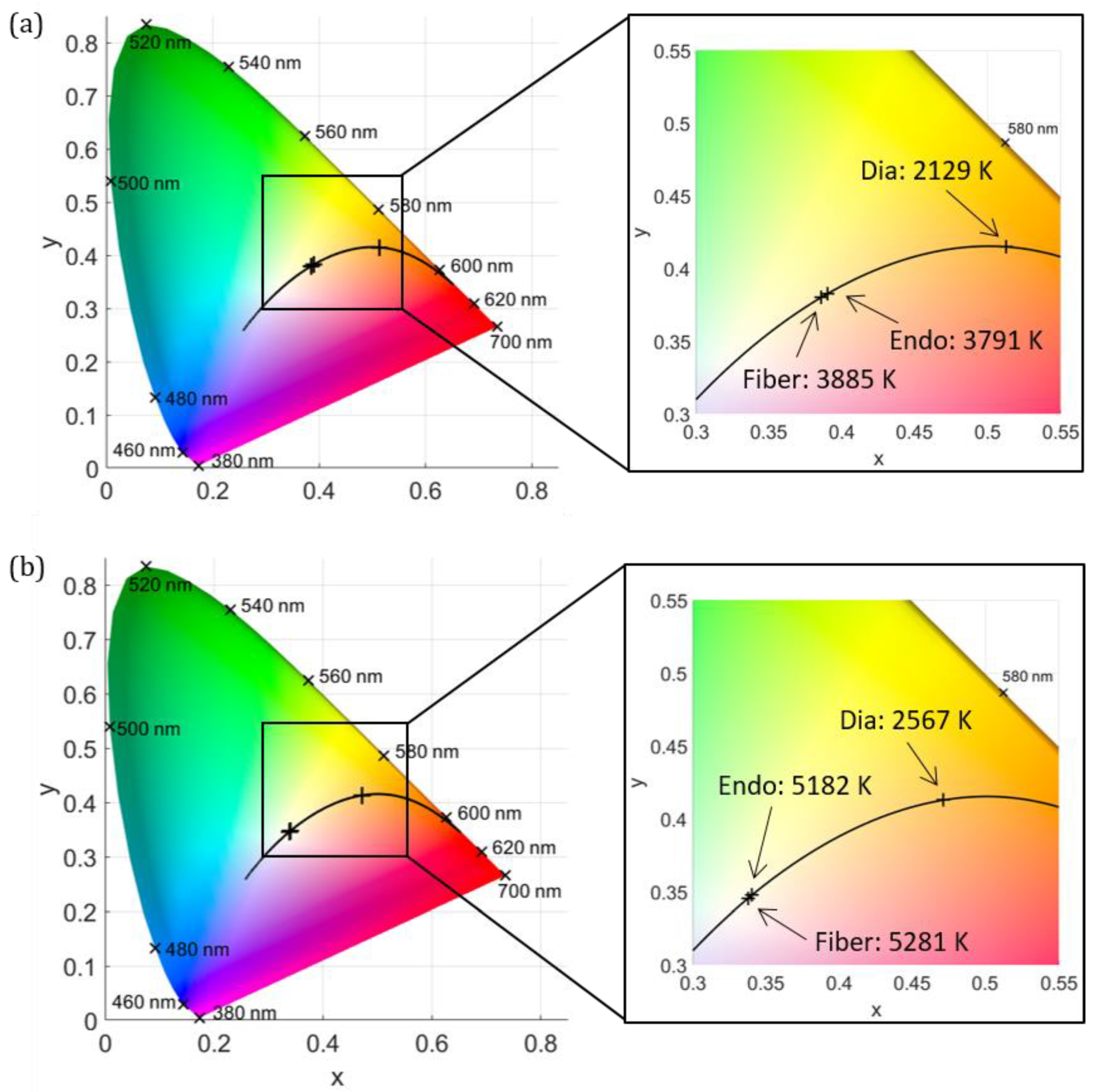
| CCT (K) | Fiber Emission | Endoillumination | Diaphanoscopy |
|---|---|---|---|
| Halogen lamp | 3885 ± 62 | 3791 ± 213 | 2129 ± 134 |
| Xenon lamp | 5281 ± 100 | 5182 ± 406 | 2567 ± 197 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fehler, N.; Hessling, M. Determination of Correlated Color Temperature in Ex Vivo Porcine Eyes during Intraocular Illumination. J. Clin. Med. 2023, 12, 3034. https://doi.org/10.3390/jcm12083034
Fehler N, Hessling M. Determination of Correlated Color Temperature in Ex Vivo Porcine Eyes during Intraocular Illumination. Journal of Clinical Medicine. 2023; 12(8):3034. https://doi.org/10.3390/jcm12083034
Chicago/Turabian StyleFehler, Nicole, and Martin Hessling. 2023. "Determination of Correlated Color Temperature in Ex Vivo Porcine Eyes during Intraocular Illumination" Journal of Clinical Medicine 12, no. 8: 3034. https://doi.org/10.3390/jcm12083034