
Use of Recombinant Activated Factor VII in Bleeding Lung Transplant Patients Undergoing Perioperative ECMO Therapy †
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
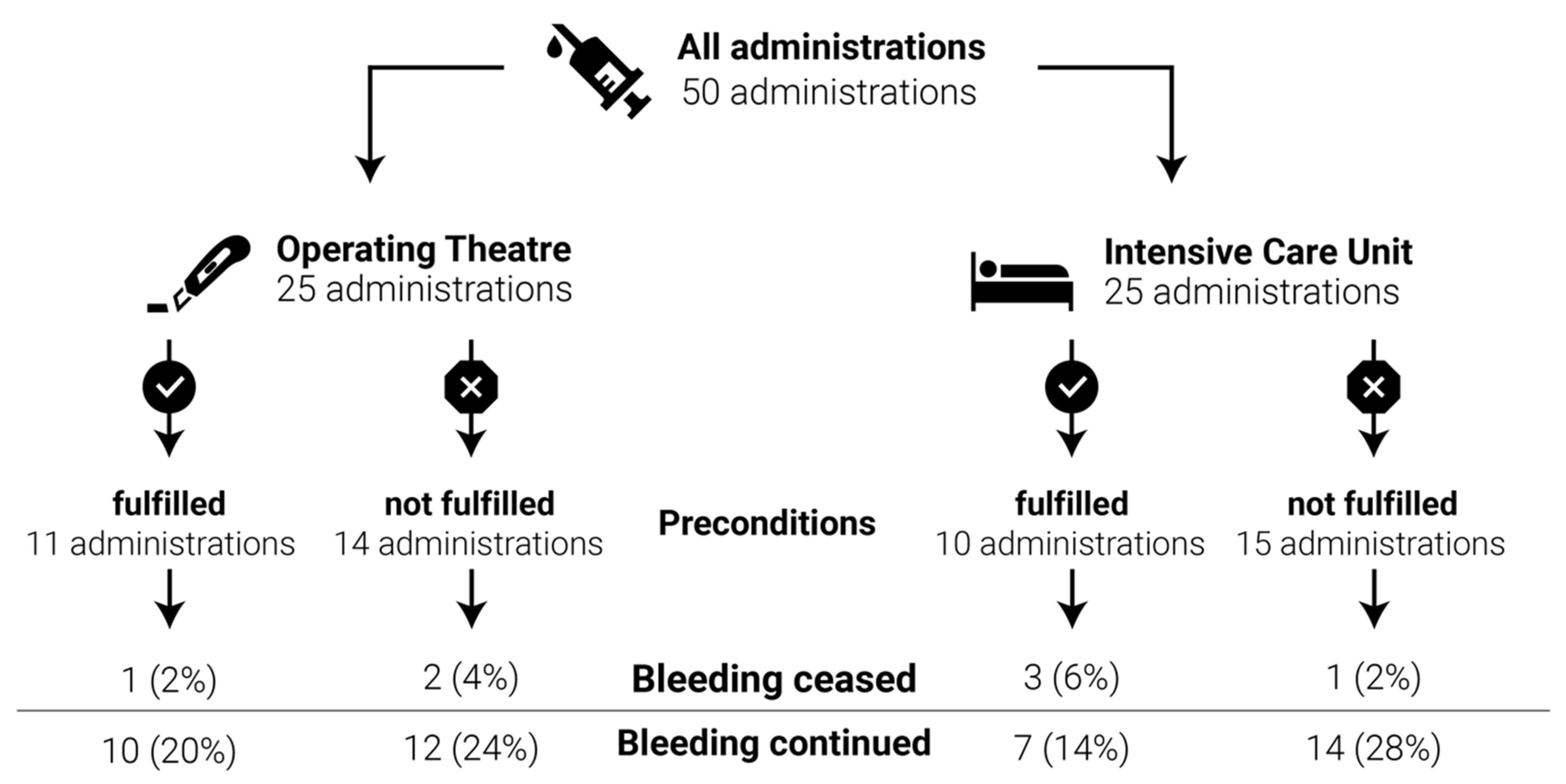
3.2. Efficacy of rFVIIa
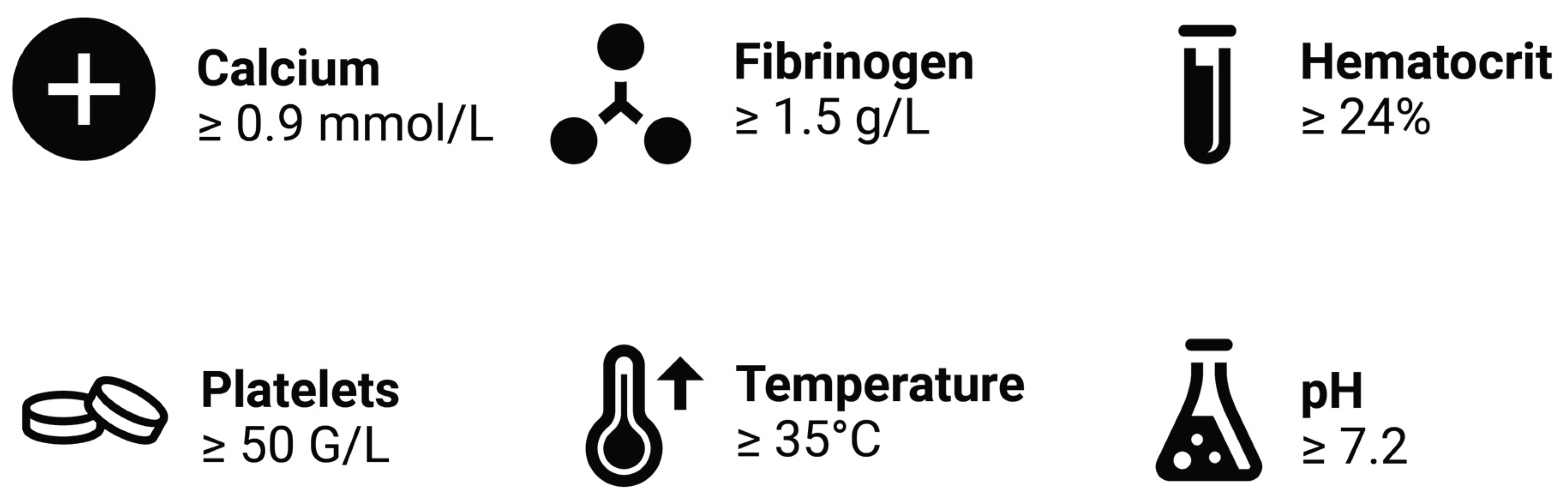
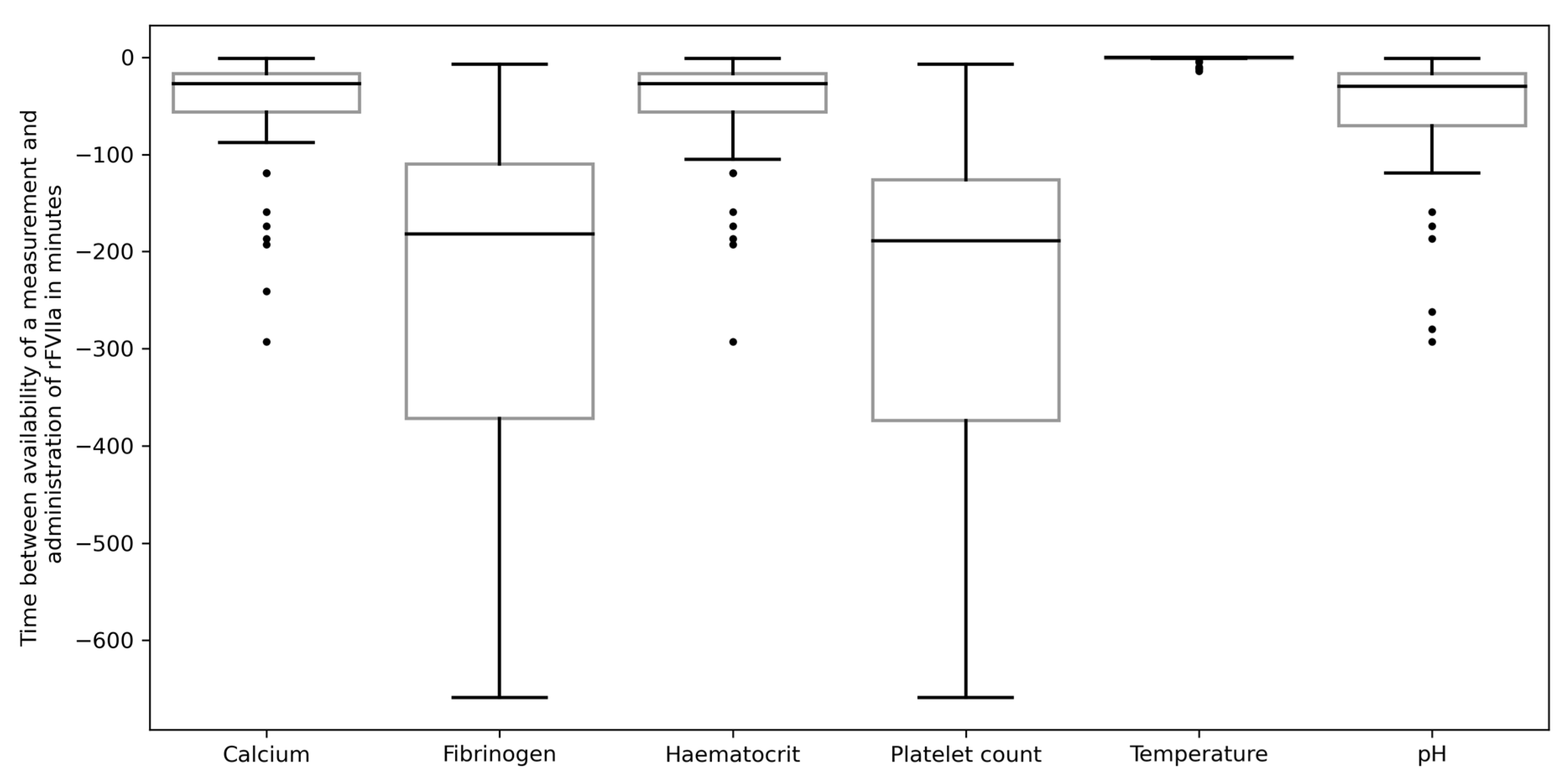
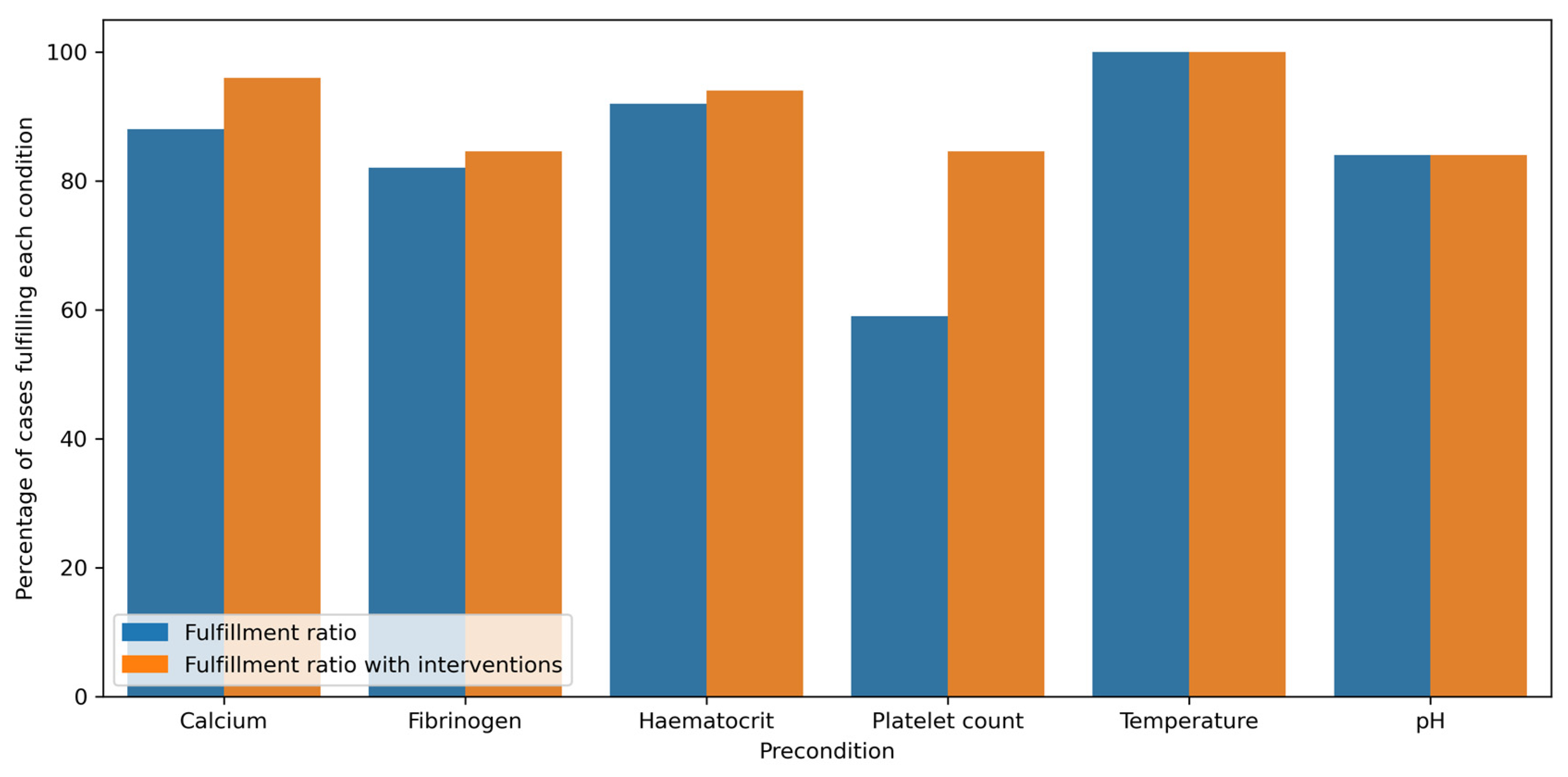
3.3. Fulfillment of Recommended Preconditions
3.4. Incidence of Thromboembolic Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Annich, G.M. Extracorporeal Life Support: The Precarious Balance of Hemostasis. J. Thromb. Haemost. 2015, 13, S336–S342. [Google Scholar] [CrossRef]
- NovoSeven Product Information 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/novoseven-epar-product-information_en.pdf (accessed on 31 August 2022).
- Aigner, C.; Wisser, W.; Taghavi, S.; Lang, G.; Jaksch, P.; Czyzewski, D.; Klepetko, W. Institutional Experience with Extracorporeal Membrane Oxygenation in Lung Transplantation. Eur. J. Cardiothorac. Surg. 2007, 31, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Hoetzenecker, K.; Donahoe, L.; Yeung, J.C.; Azad, S.; Fan, E.; Ferguson, N.D.; Del Sorbo, L.; de Perrot, M.; Pierre, A.; Yasufuku, K.; et al. Extracorporeal Life Support as a Bridge to Lung Transplantation-Experience of a High-Volume Transplant Center. J. Thorac. Cardiovasc. Surg. 2018, 155, 1316–1328.e1. [Google Scholar] [CrossRef] [PubMed]
- Hoetzenecker, K.; Schwarz, S.; Muckenhuber, M.; Benazzo, A.; Frommlet, F.; Schweiger, T.; Bata, O.; Jaksch, P.; Ahmadi, N.; Muraközy, G.; et al. Intraoperative Extracorporeal Membrane Oxygenation and the Possibility of Postoperative Prolongation Improve Survival in Bilateral Lung Transplantation. J. Thorac. Cardiovasc. Surg. 2018, 155, 2193–2206.e3. [Google Scholar] [CrossRef] [PubMed]
- Ius, F.; Kuehn, C.; Tudorache, I.; Sommer, W.; Avsar, M.; Boethig, D.; Fuehner, T.; Gottlieb, J.; Hoeper, M.; Haverich, A.; et al. Lung Transplantation on Cardiopulmonary Support: Venoarterial Extracorporeal Membrane Oxygenation Outperformed Cardiopulmonary Bypass. J. Thorac. Cardiovasc. Surg. 2012, 144, 1510–1516. [Google Scholar] [CrossRef]
- Thomas, J.; Kostousov, V.; Teruya, J. Bleeding and Thrombotic Complications in the Use of Extracorporeal Membrane Oxygenation. Semin. Thromb. Hemost. 2018, 44, 020–029. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.B.V.; Ryerson, L.M.; Ratano, D.; Fan, E.; Faraoni, D.; Annich, G.M. 2021 ELSO Adult and Pediatric Anticoagulation Guidelines. ASAIO J. 2022, 68, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Nunez, J.I.; Gosling, A.F.; O’Gara, B.; Kennedy, K.F.; Rycus, P.; Abrams, D.; Brodie, D.; Shaefi, S.; Garan, A.R.; Grandin, E.W. Bleeding and Thrombotic Events in Adults Supported with Venovenous Extracorporeal Membrane Oxygenation: An ELSO Registry Analysis. Intensive Care Med. 2021, 48, 213–224. [Google Scholar] [CrossRef]
- Ruszel, N.; Kiełbowski, K.; Piotrowska, M.; Kubisa, M.; Grodzki, T.; Wójcik, J.; Kubisa, B. Central, Peripheral ECMO or CPB? Comparsion between Circulatory Support Methods Used during Lung Transplantation. J. Cardiothorac. Surg. 2021, 16, 341. [Google Scholar] [CrossRef]
- Kozek-Langenecker, S.A.; Ahmed, A.B.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Fries, D.; et al. Management of Severe Perioperative Bleeding: Guidelines from the European Society of Anaesthesiology: First Update 2016. Eur. J. Anaesthesiol. 2017, 34, 332–395. [Google Scholar] [CrossRef]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European Guideline on Management of Major Bleeding and Coagulopathy Following Trauma: Fifth Edition. Critical Care 2019, 23, 98. [Google Scholar] [CrossRef] [PubMed]
- Gratz, J.; Pausch, A.; Schaden, E.; Baierl, A.; Jaksch, P.; Erhart, F.; Hoetzenecker, K.; Wiegele, M. Low Molecular Weight Heparin versus Unfractioned Heparin for Anticoagulation during Perioperative Extracorporeal Membrane Oxygenation: A Single Center Experience in 102 Lung Transplant Patients. Artif. Organs 2020, 44, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Bui, J.D.; Despotis, G.D.; Trulock, E.P.; Patterson, G.A.; Goodnough, L.T. Fatal Thrombosis after Administration of Activated Prothrombin Complex Concentrates in a Patient Supported by Extracorporeal Membrane Oxygenation Who Had Received Activated Recombinant Factor VII. J. Thorac. Cardiovasc. Surg. 2002, 124, 852–854. [Google Scholar] [CrossRef] [PubMed]
- Puentes, W.; Roscoe, A.; Cypel, M.; Wasowicz, M. Successful Use of Recombinant Activated Coagulation Factor VII in a Patient with Veno-Venous ECMO after Lung Transplantation. Anaesthesiol. Intensive Ther. 2015, 47, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Repessé, X.; Au, S.M.; Bréchot, N.; Trouillet, J.-L.; Leprince, P.; Chastre, J.; Combes, A.; Luyt, C.-E. Recombinant Factor VIIa for Uncontrollable Bleeding in Patients with Extracorporeal Membrane Oxygenation: Report on 15 Cases and Literature Review. Crit. Care 2013, 17, R55. [Google Scholar] [CrossRef]
- Anselmi, A.; Guinet, P.; Ruggieri, V.G.; Aymami, M.; Lelong, B.; Granry, S.; Malledant, Y.; Le Tulzo, Y.; Gueret, P.; Verhoye, J.-P.; et al. Safety of Recombinant Factor VIIa in Patients under Extracorporeal Membrane Oxygenation. Eur. J. Cardiothorac. Surg 2016, 49, 78–84. [Google Scholar] [CrossRef]
- Ratano, D.; Alberio, L.; Delodder, F.; Faouzi, M.; Berger, M.M. Agreement between Activated Partial Thromboplastin Time and Anti-Xa Activity in Critically Ill Patients Receiving Therapeutic Unfractionated Heparin. Thromb. Res. 2019, 175, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Swayngim, R.; Preslaski, C.; Burlew, C.C.; Beyer, J. Comparison of Clinical Outcomes Using Activated Partial Thromboplastin Time versus Antifactor-Xa for Monitoring Therapeutic Unfractionated Heparin: A Systematic Review and Meta-Analysis. Thromb. Res. 2021, 208, 18–25. [Google Scholar] [CrossRef]
- Lier, H.; Krep, H.; Schroeder, S.; Stuber, F. Preconditions of Hemostasis in Trauma: A Review. The Influence of Acidosis, Hypocalcemia, Anemia, and Hypothermia on Functional Hemostasis in Trauma. J. Trauma 2008, 65, 951–960. [Google Scholar] [CrossRef]
- Grottke, O.; Mallaiah, S.; Karkouti, K.; Saner, F.; Haas, T. Fibrinogen Supplementation and Its Indications. Semin. Thromb. Hemost. 2020, 46, 038–049. [Google Scholar] [CrossRef]
- O’Connell, K.A.; Wood, J.J.; Wise, R.P.; Lozier, J.N.; Braun, M.M. Thromboembolic Adverse Events After Use of Recombinant Human Coagulation Factor VIIa. JAMA 2006, 295, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Brogan, T.V.; Thiagarajan, R.R.; Rycus, P.T.; Bartlett, R.H.; Bratton, S.L. Extracorporeal Membrane Oxygenation in Adults with Severe Respiratory Failure: A Multi-Center Database. Intensive Care Med. 2009, 35, 2105–2114. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.A.; Hockings, L.E.; Andrews, R.K.; Aubron, C.; Gardiner, E.E.; Pellegrino, V.A.; Davis, A.K. Extracorporeal Membrane Oxygenation—Hemostatic Complications. Transfus. Med. Rev. 2015, 29, 90–101. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| n | 17 |
| Age, mean (SD) | 38.71 (14.22) |
| Sex = M, % | 64.71% |
| Weight [kg], mean (SD) | 63.35 (18.58) |
| BMI, mean (SD) | 21.35 (5.08) |
| LuTX Indication, no. (%) | |
| Cystic Fibrosis | 4 (23.53%) |
| Primary Pulmonary Hypertension | 4 (23.53%) |
| Chronic Lung Allograft Dysfunction | 3 (17.65%) |
| Interstitial Lung Disease | 3 (17.65%) |
| CTEPH | 2 (11.76%) |
| Primary Ciliary Dyskinesia | 1 (5.88%) |
| Transfusions during ECMO, mean (SD) | |
| pRBC [U] | 24.29 (16.48) |
| Platelet Concentrates [U] | 5.88 (7.11) |
| Fresh Frozen Plasma [U] | 18.35 (19.12) |
| Prothrombin Complex Concentrates [IU] | 6029.41 (3882.94) |
| ICU LOS, mean (SD) | 48 days (30 days) |
| ICU Death, no. (%) | 8 (47.06%) |
| Hospital LOS, mean (SD) | 57 days (32 days) |
| Hospital Mortality, no. (%) | 9 (52.94%) |
| rFVIIa dose μg/kg, mean (SD) | 81.59 (35.44) |
| rFVIIa | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Age | Sex | LuTX-Indication | OR | ICU | Dose [mg] | pRBC [U] | Thromboembolic Event | ICU LOS [Days] | ICU Death |
| 1 | 26 | F | Cystic Fibrosis | 0 | 12 | 60 | 57 | - | 36 | yes |
| 2 | 60 | M | Interstitial Lung Disease | 1 | 0 | 3 | 8 | Right SFA occlusion | 54 | no |
| 3 | 48 | M | Primary Ciliary Dyskinesia | 2 | 0 | 10 | 29 | - | 80 | yes |
| 4 | 31 | M | CTEPH | 1 | 1 | 10 | 39 | Pulmonary embolism | 22 | yes |
| 5 | 24 | F | Cystic Fibrosis | 2 | 0 | 10 | 15 | - | 106 | no |
| 6 | 58 | M | CTEPH | 1 | 3 | 20 | 60 | ECMO circuit clotting | 42 | yes |
| 7 | 38 | M | Primary Pulmonary Hypertension | 0 | 1 | 5 | 21 | Thrombosis of the right atrial appendage | 54 | yes |
| 8 | 40 | M | Primary Pulmonary Hypertension | 1 | 0 | 10 | 16 | - | 34 | no |
| 9 | 26 | F | Primary Pulmonary Hypertension | 1 | 3 | 15 | 25 | - | 31 | no |
| 10 | 57 | M | Interstitial Lung Disease | 1 | 0 | 5 | 5 | - | 106 | no |
| 11 | 37 | F | Primary Pulmonary Hypertension | 3 | 0 | 15 | 5 | - | 4 | yes |
| 12 | 33 | F | Cystic Fibrosis | 0 | 2 | 7.2 | 27 | Pulmonary embolism | 75 | no |
| 13 | 34 | M | Chronic Lung Allograft Dysfunction | 3 | 0 | 15 | 19 | Pulmonary embolism | 6 | yes |
| 14 | 66 | M | Interstitial Lung Disease | 0 | 2 | 10 | 35 | - | 73 | no |
| 15 | 19 | F | Cystic Fibrosis | 4 | 0 | 13 | 16 | - | 30 | no |
| 16 | 36 | M | Chronic Lung Allograft Dysfunction | 4 | 1 | 20 | 30 | - | 47 | yes |
| 17 | 25 | M | Chronic Lung Allograft Dysfunction | 1 | 0 | 5 | 6 | - | 33 | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laxar, D.; Schaden, E.; Wiegele, M.; Hötzenecker, K.; Schwarz, S.; Gratz, J. Use of Recombinant Activated Factor VII in Bleeding Lung Transplant Patients Undergoing Perioperative ECMO Therapy. J. Clin. Med. 2023, 12, 3020. https://doi.org/10.3390/jcm12083020
Laxar D, Schaden E, Wiegele M, Hötzenecker K, Schwarz S, Gratz J. Use of Recombinant Activated Factor VII in Bleeding Lung Transplant Patients Undergoing Perioperative ECMO Therapy. Journal of Clinical Medicine. 2023; 12(8):3020. https://doi.org/10.3390/jcm12083020
Chicago/Turabian StyleLaxar, Daniel, Eva Schaden, Marion Wiegele, Konrad Hötzenecker, Stefan Schwarz, and Johannes Gratz. 2023. "Use of Recombinant Activated Factor VII in Bleeding Lung Transplant Patients Undergoing Perioperative ECMO Therapy" Journal of Clinical Medicine 12, no. 8: 3020. https://doi.org/10.3390/jcm12083020