
Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes

 ,
,  ,
,  ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
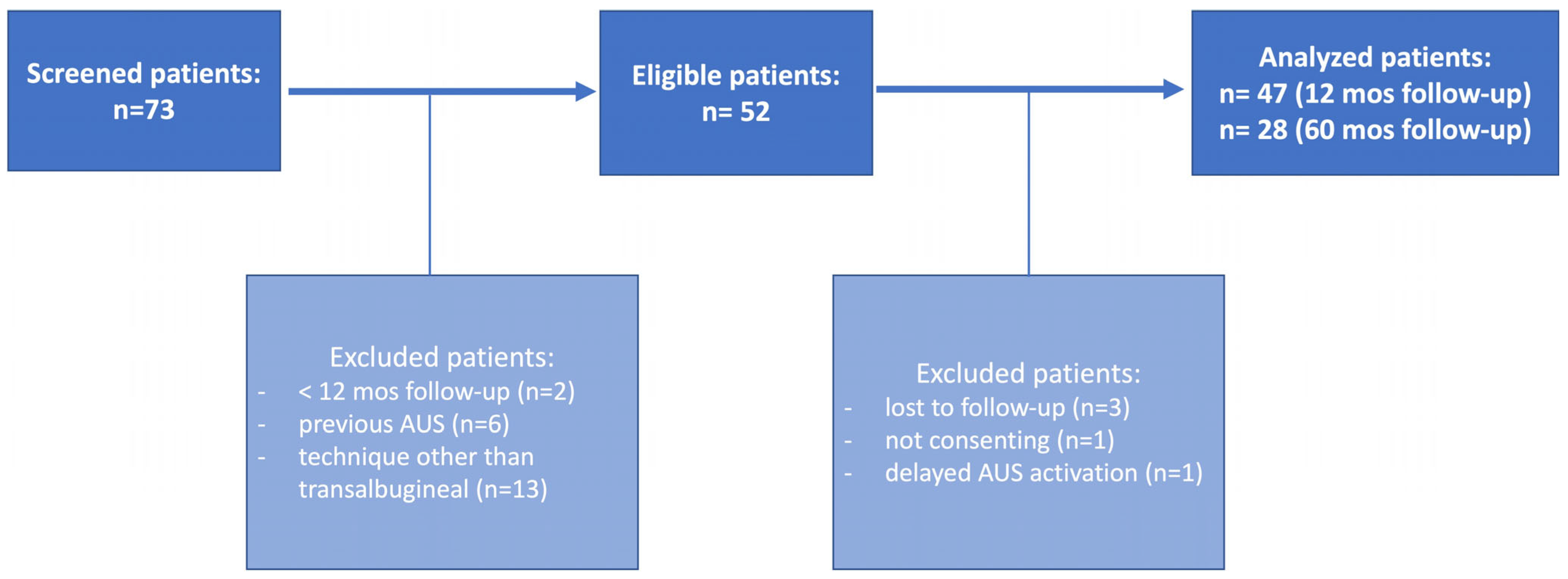
2.1. Patient Recruitment and Data Items
- -
- preoperative data: age, body mass index (BMI), Charlson Comorbidity Index (CCI), history of diabetes mellitus, use of anticoagulants, previous irradiation and prostate or pelvic surgery, previous anti-incontinence procedures or urethrotomy, incontinence severity and quality-of-life impact, main findings of the preoperative work-out, and erectile function;
- -
- perioperative data: operative time, cuff size and location, type and location of the pressure-regulating balloon (PRB), and intraoperative complications;
- -
- postoperative data: catheterization time, pain score, the time interval from implantation to activation, postoperative complications, continence, and sexual outcomes.
2.2. Preoperative Evaluation
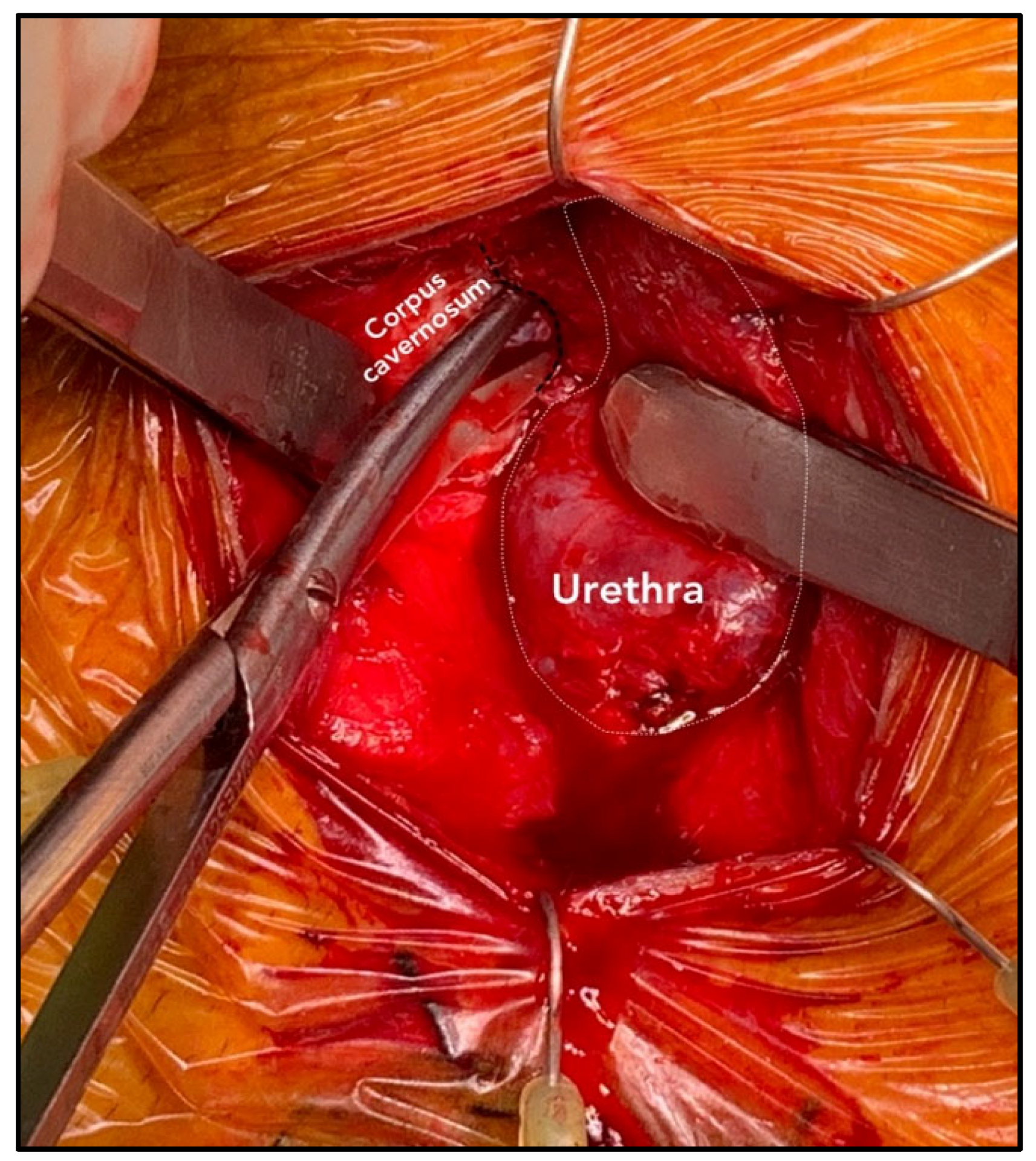
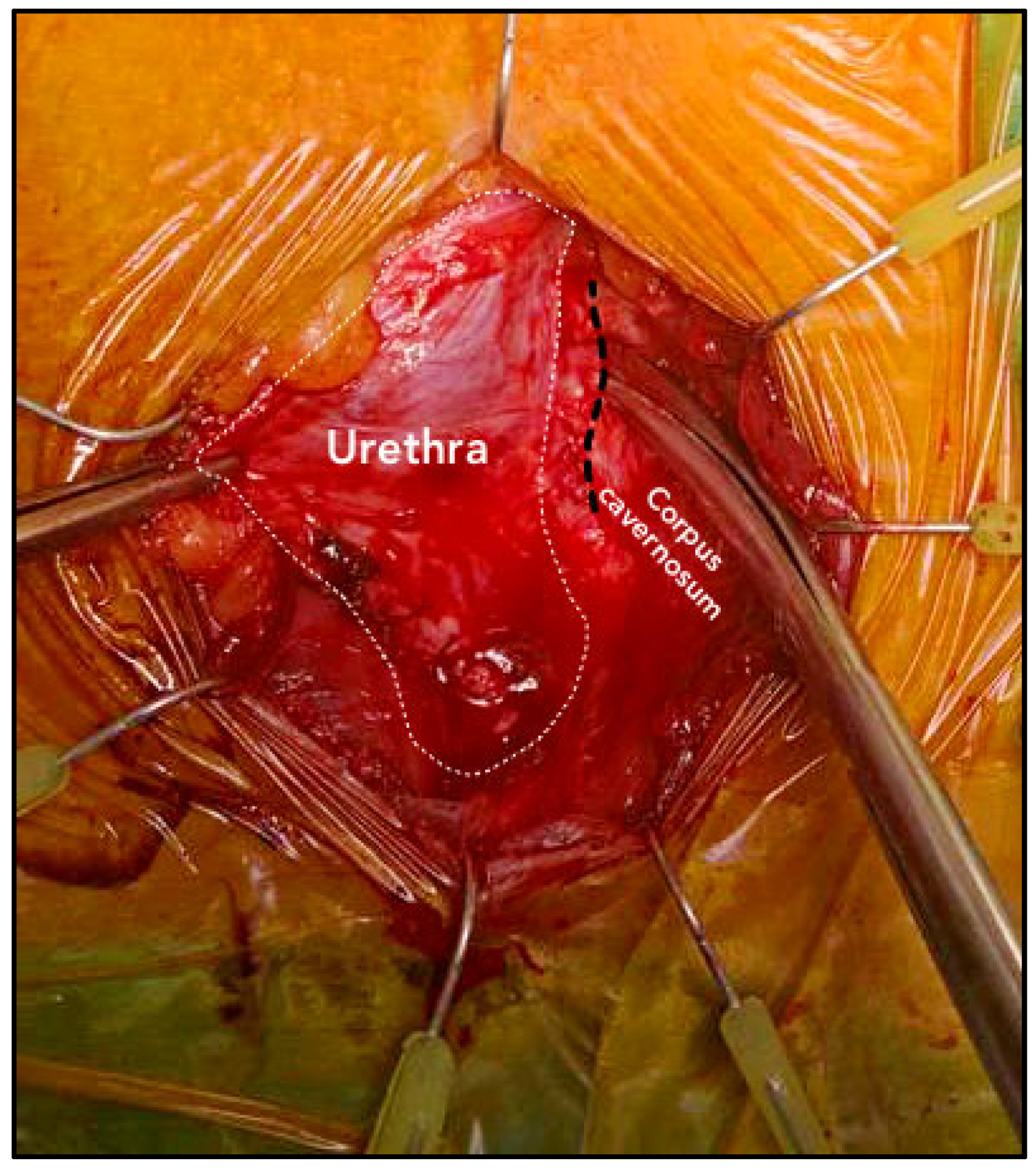
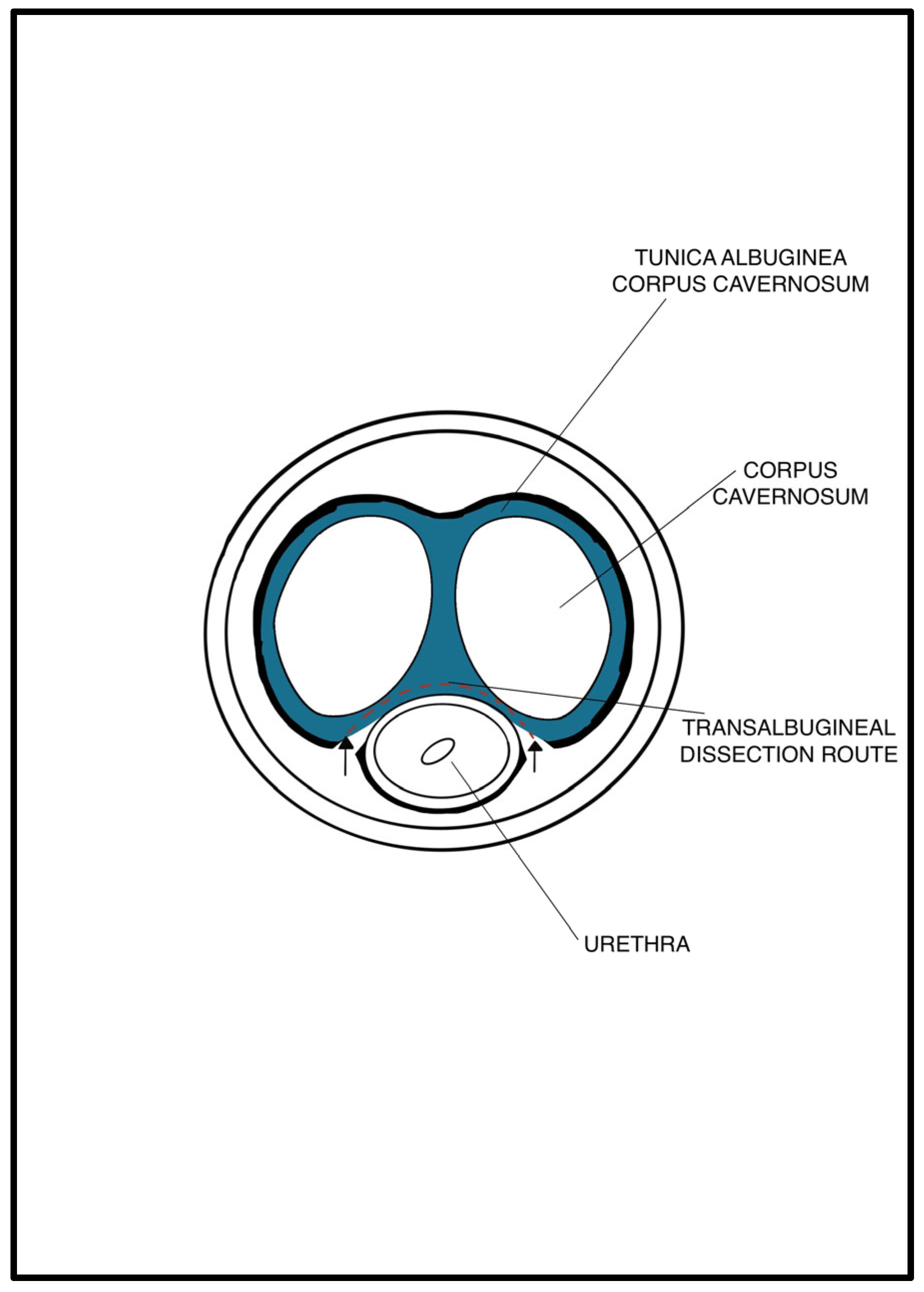
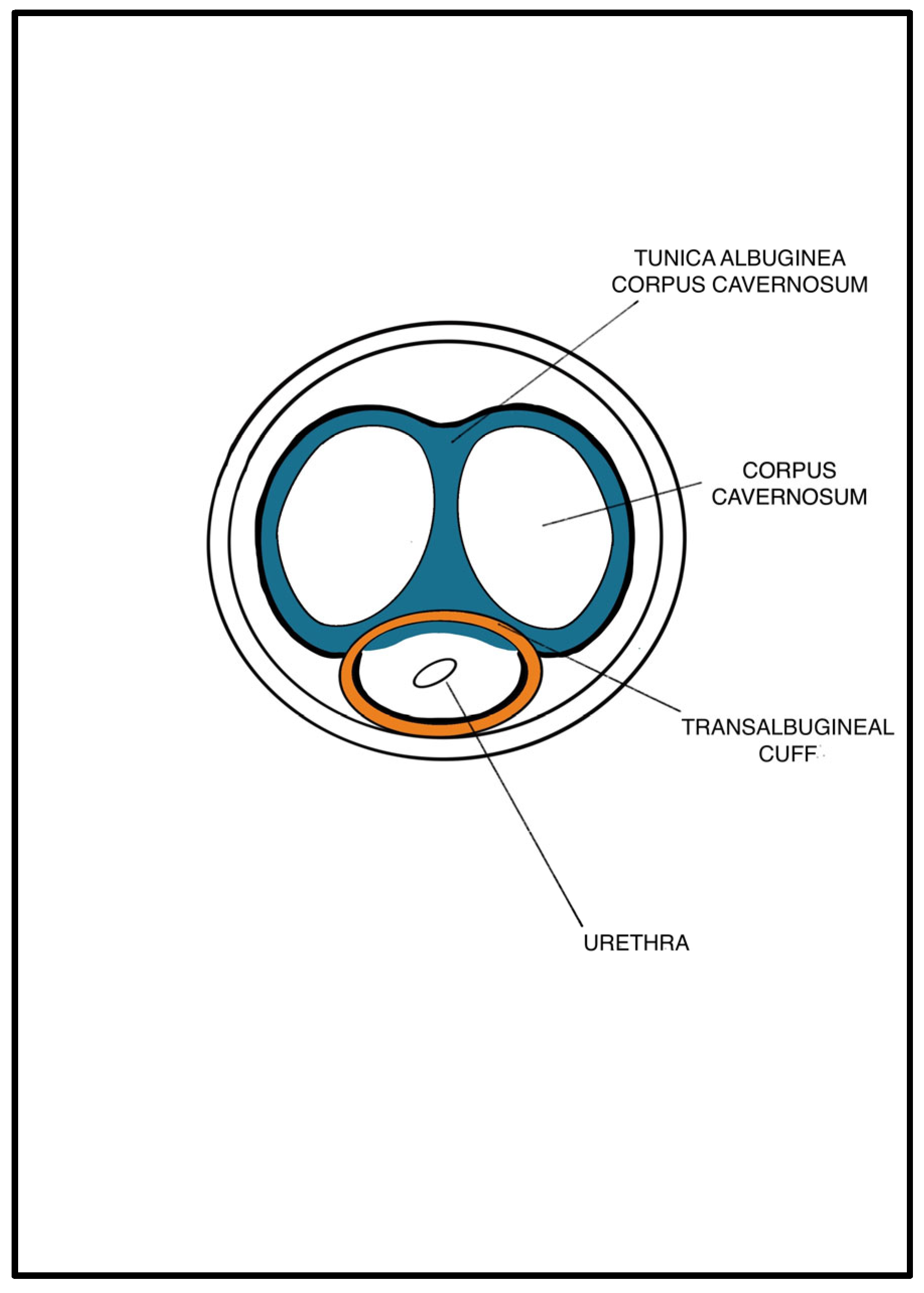
2.3. Patient Preparation and Surgical Technique
2.4. Postoperative Management and Follow-Up
2.5. Outcome Measures
2.6. Statistical Analysis and Reporting
3. Results
3.1. Baseline Patient Characteristics
3.2. Intraoperative and Early Postoperative Outcomes
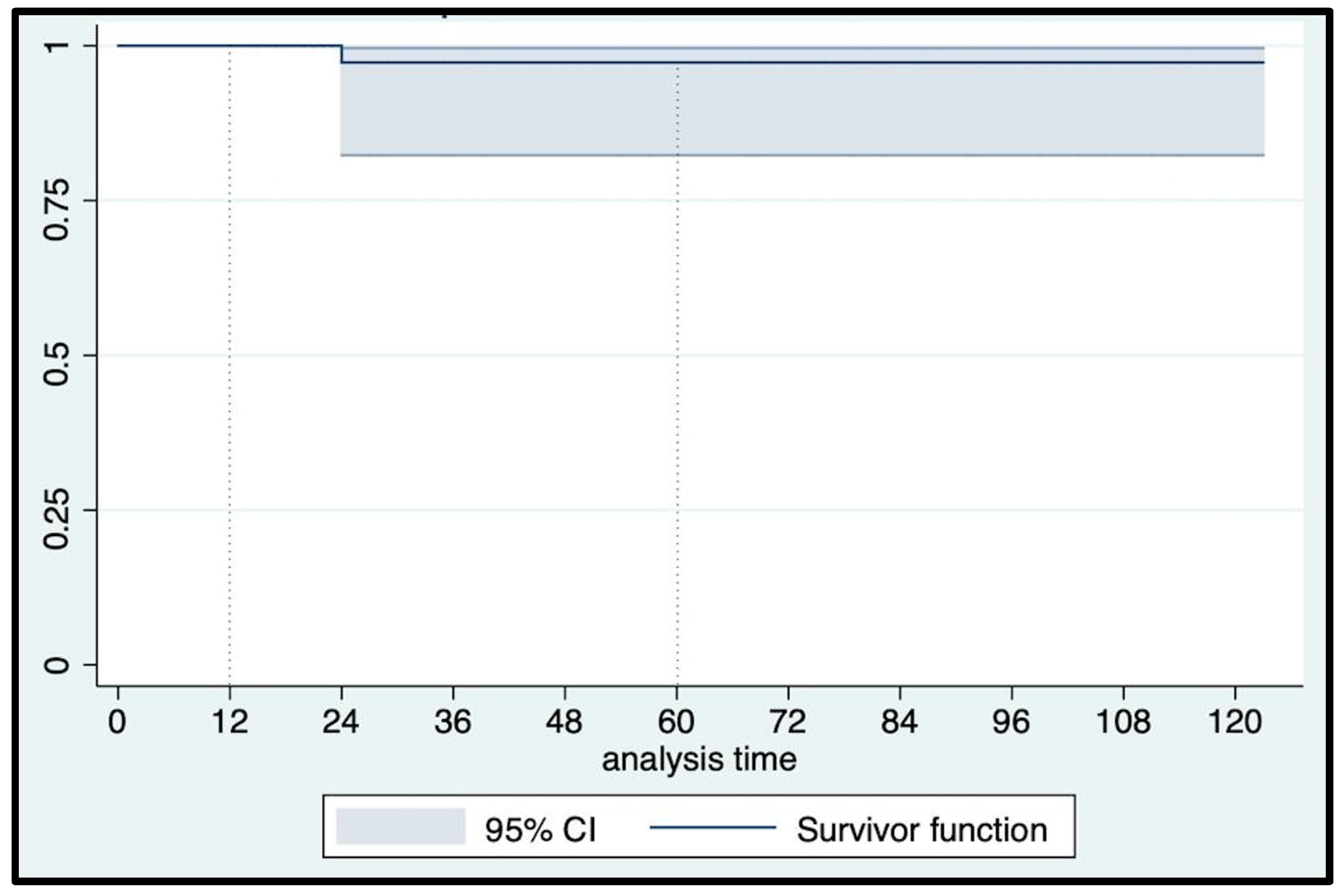
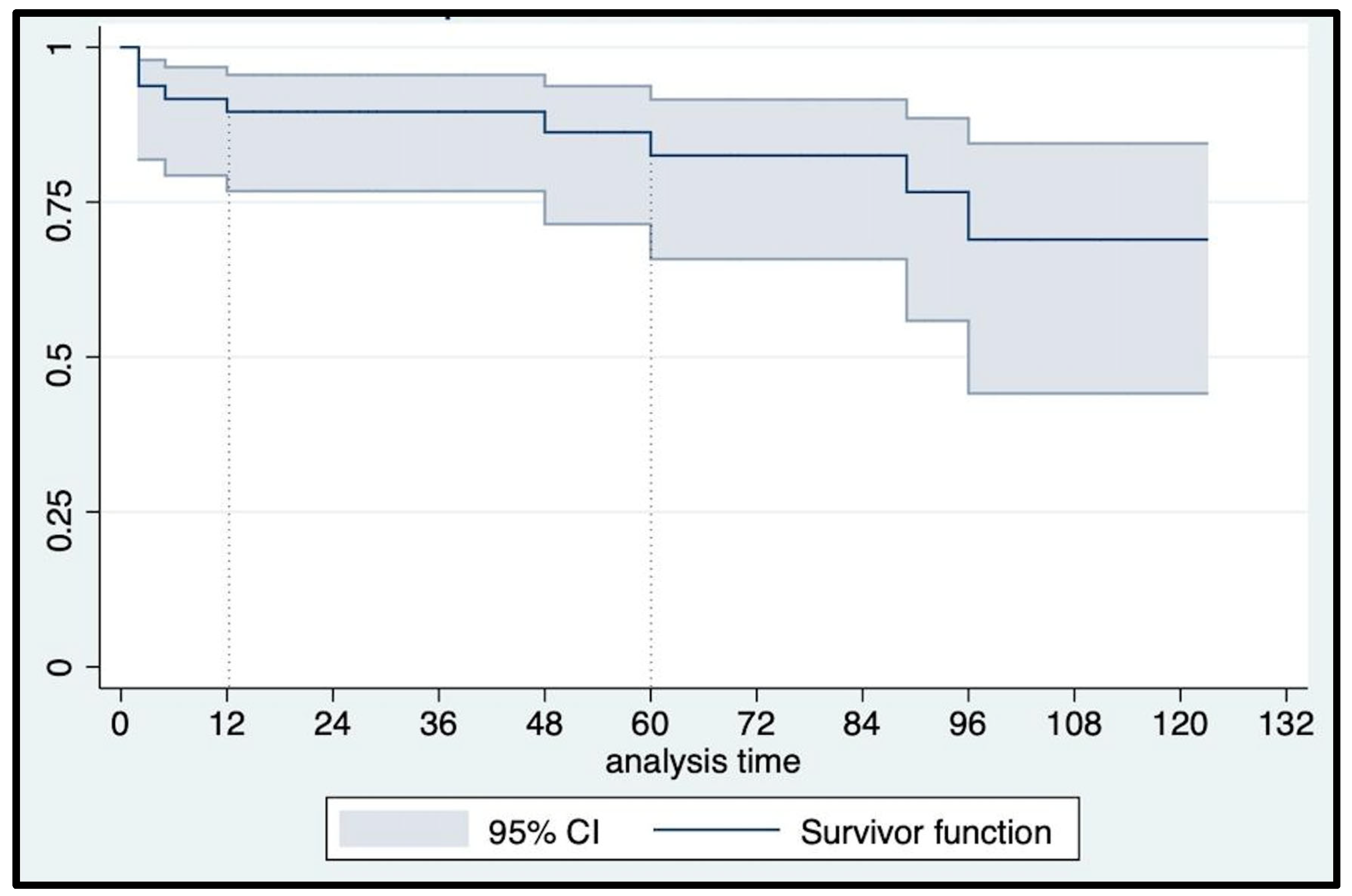
3.3. Late Complications and Primary Outcome
3.4. Functional Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buckley, B.S.; Lapitan, M.C. Epidemiology Committee of the Fourth International Consultation on Incontinence, Paris, 2008. Prevalence of urinary incontinence in men, women, and children-current evidence: Findings of the Fourth International Consultation on Incontinence. Urology 2010, 76, 265–270. [Google Scholar] [CrossRef]
- Sacco, E.; Prayer-Galetti, T.; Pinto, F.; Fracalanza, S.; Betto, G.; Pagano, F.; Artibani, W. Urinary incontinence after radical prostatectomy: Incidence by definition, risk factors and temporal trend in a large series with a long-term follow-up. BJU Int. 2006, 97, 1234–1241. [Google Scholar] [CrossRef]
- Martens, F.; Van der Aa, F.; Heesakkers, J.; Nilsen, O.; Zachoval, R.; Romero-Otero, J.; Kort de, L.; van Renthergem, K.; Martinez-Salamanca, J.; Castro-Díaz, D.; et al. Prospective multi center registry for patients undergoing surgery for male stress urinary incontinence (SATURN): 1 year follow-up in 500 patients. Continence 2022, 2, 100191. [Google Scholar] [CrossRef]
- Bientinesi, R.; Recupero, S.M.; Palermo, G.; D’Agostino, D.; Bassi, P.F.; Sacco, E. Chirurgia dell’incontinenza urinaria maschile: A che punto siamo? [Surgery for male urinary incontinence: Where are we now and what is in the pipeline?]. Urologia 2015, 82, 139–150. [Google Scholar] [CrossRef]
- Gravas, S.; Cornu, J.N.; Gacci, M.; Gratzke, T.R.W.; Hermann, S.; Madersbacher, C.; Mamoulakis, K.A.O.; Tikkinen, M.; Karavitakis, I.; Kyriazis, S.; et al. European Association of Urology (EAU) Guidelines on Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO). Available online: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts (accessed on 20 November 2022).
- Sacco, E.; Gandi, C.; Marino, F.; Totaro, A.; Di Gianfrancesco, L.; Palermo, G.; Pierconti, F.; Racioppi, M.; Bassi, P.F. Artificial urinary sphincter significantly better than fixed sling for moderate post-prostatectomy stress urinary incontinence: A propensity score-matched study. BJU Int. 2021, 127, 229–237. [Google Scholar] [CrossRef]
- Scott, F.B.; Bradley, W.E.; Timm, G.W. Treatment of urinary incontinence by implantable prosthetic sphincter. Urology 1973, 1, 252–259. [Google Scholar] [CrossRef]
- Kretschmer, A.; Nitti, V. Surgical Treatment of Male Postprostatectomy Incontinence: Current Concepts. Eur. Urol. Focus 2017, 3, 364–376. [Google Scholar] [CrossRef]
- Herschorn, S. The artificial urinary sphincter is the treatment of choice for post-radical prostatectomy incontinence. Can. Urol. Assoc. J. 2008, 2, 536–539. [Google Scholar] [CrossRef]
- Flynn, B.J.; Webster, G.D. Evaluation and surgical management of intrinsic sphincter deficiency after radical prostatectomy. Rev. Urol. 2004, 6, 180–186. [Google Scholar]
- Wang, R.; McGuire, E.J.; He, C.; Faerber, G.J.; Latini, J.M. Long-term outcomes after primary failures of artificial urinary sphincter implantation. Urology 2012, 79, 922–928. [Google Scholar] [CrossRef]
- Danforth, T.L.; Ginsberg, D.A. Artificial Urinary Sphincter. In Hinman’s Atlas of Urologic Surgery, 4th ed.; Smith, J.A., Howards, S.S., Preminger, G.M., Dmochowski, R.R., Eds.; Elsevier: Philadelphia, PA, USA, 2017. [Google Scholar]
- Guralnick, M.L.; Miller, E.; Toh, K.L.; Webster, G.D. Transcorporal artificial urinary sphincter cuff placement in cases requiring revision for erosion and urethral atrophy. J. Urol. 2002, 167, 2075–2078. [Google Scholar] [CrossRef]
- Wiedemann, L.; Cornu, J.N.; Haab, E.; Peyrat, L.; Beley, S.; Cathelineau, X.; Haab, F. Transcorporal artificial urinary sphincter implantation as a salvage surgical procedure for challenging cases of male stress urinary incontinence: Surgical technique and functional outcomes in a contemporary series. BJU Int. 2013, 112, 1163–1168. [Google Scholar] [CrossRef]
- Miller, D.; Pekala, K.; Zhang, X.; Orikogbo, O.; Rogers, D.; Fuller, T.W.; Maganty, A.; Rusilko, P. Outcomes of Initial Transcorporal Versus Standard Placement of Artificial Urinary Sphincter in Patients With Prior Radiation. Cureus 2022, 31, e25519. [Google Scholar] [CrossRef]
- Smith, P.J.; Hudak, S.J.; Scott, J.F.; Zhao, L.C.; Morey, A.F. Transcorporal artificial urinary sphincter cuff placement is associated with a higher risk of postoperative urinary retention. Can. J. Urol. 2013, 20, 6773–6777. [Google Scholar]
- Brock, G.; Hsu, G.L.; Nunes, L.; von Heyden, B.; Lue, T.F. The anatomy of the tunica albuginea in the normal penis and Peyronie’s disease. J. Urol. 1997, 157, 276–281. [Google Scholar] [CrossRef]
- Shafik, A.; El-Sharkawy, A.; Khamis, A.; Zaghloul, S.; Gawad, M.A.; Elwy, D. Histologic study of the tunica albuginea of the penis and mode of cavernosus muscles’ insertion in it. Arch. Androl. 2006, 52, 1–8. [Google Scholar] [CrossRef]
- Hajebrahimi, S.; Corcos, J.; Lemieux, M.C. International consultation on incontinence questionnaire short form: Comparison of physician versus patient completion and immediate and delayed self-administration. Urology 2004, 63, 1076–1078. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot Res. 1999, 11, 319–326. [Google Scholar] [CrossRef]
- Stoffel, J.T.; Barrett, D.M. The artificial genitourinary sphincter. BJU Int. 2008, 102, 644–658. [Google Scholar] [CrossRef]
- James, M.H.; McCammon, K.A. Artificial urinary sphincter for post-prostatectomy incontinence: A review. Int. J. Urol. 2014, 21, 536–543. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Sacco, E.; Gandi, C.; Vaccarella, L.; Recupero, S.; Racioppi, M.; Pinto, F.; Totaro, A.; Foschi, N.; Palermo, G.; Pierconti, F.; et al. Titanized Transobturator Sling Placement for Male Stress Urinary Incontinence Using an Inside-out Single-incision Technique: Minimum 12-Months Follow-up Study. Urology 2018, 115, 144–150. [Google Scholar] [CrossRef]
- Gacci, M.; Sakalis, V.I.; Karavitakis, M.; Cornu, J.N.; Gratzke, C.; Herrmann, T.R.W.; Kyriazis, I.; Malde, S.; Mamoulakis, C.; Rieken, M.; et al. European Association of Urology Guidelines on Male Urinary Incontinence. Eur. Urol. 2022, 82, 387–398. [Google Scholar] [CrossRef]
- Van der Aa, F.; Drake, M.J.; Kasyan, G.R.; Petrolekas, A.; Cornu, J.N. Young Academic Urologists Functional Urology Group. The artificial urinary sphincter after a quarter of a century: A critical systematic review of its use in male non-neurogenic incontinence. Eur. Urol. 2013, 63, 681–689. [Google Scholar] [CrossRef]
- Cheung, F.; Fathollahi, A.; Vertosick, E.; Jarvis, T.R.; Katz, D.; Sandhu, J.S. Dorsolateral fibromuscular tissue preservation during artificial urinary sphincter cuff placement is associated with low infection and erosion rates. BJU Int. 2019, 123, 328–334. [Google Scholar] [CrossRef]
- Ortiz, N.M.; Wolfe, A.R.; Baumgarten, A.S.; Ward, E.E.; VanDyke, M.E.; Hudak, S.J.; Morey, A.F. Artificial Urinary Sphincter Cuff Erosion Heat Map Shows Similar Anatomical Characteristics for Transcorporal and Standard Approach. J. Urol. 2020, 204, 1027–1032. [Google Scholar] [CrossRef]
- Moser, D.C.; Kaufman, M.R.; Milam, D.F.; Johnsen, N.V.; Cleves, M.A.; Broghammer, J.A.; Brant, W.O.; Jones, L.A.; Brady, J.D.; Gross, M.S.; et al. Impact of Radiation and Transcorporeal Artificial Sphincter Placement in Patients with Prior Urethral Cuff Erosion: Results from a Retrospective Multicenter Analysis. J. Urol. 2018, 200, 1338–1343. [Google Scholar] [CrossRef]
- Brant, W.O.; Erickson, B.A.; Elliott, S.P.; Powell, C.; Alsikafi, N.; McClung, C.; Myers, J.B.; Voelzke, B.B.; Smith, T.G., 3rd; Broghammer, J.A. Risk factors for erosion of artificial urinary sphincters: A multicenter prospective study. Urology 2014, 84, 934–938. [Google Scholar] [CrossRef]
- McGeady, J.B.; McAninch, J.W.; Truesdale, M.D.; Blaschko, S.D.; Kenfield, S.; Breyer, B.N. Artificial urinary sphincter placement in compromised urethras and survival: A comparison of virgin, radiated and reoperative cases. J. Urol. 2014, 192, 1756–1761. [Google Scholar] [CrossRef]
- Brant, W.O.; Martins, F.E. Artificial urinary sphincter. Transl. Androl. Urol. 2017, 6, 682–694. [Google Scholar] [CrossRef]
- Maurer, V.; Dahlem, R.; Howaldt, M.; Riechardt, S.; Fisch, M.; Ludwig, T.A.; Engel, O. Transcroporal Artificial Urinary Sphincter Placement with Closure of Corporal Bodies—A Long-Term Analysis of Functional Outcomes. Front. Surg. 2022, 1, 918011. [Google Scholar] [CrossRef]
- Lee, D.; Zafirakis, H.; Shapiro, A.; Westney, O.L. Intermediate outcomes after transcorporal placement of an artificial urinary sphincter. Int. J. Urol. 2012, 19, 861–866. [Google Scholar] [CrossRef]
- Serra, A.C.; Domínguez-Escrig, J.; Gómez-Ferrer, Á.; Miranda, E.B.; Rubio-Briones, J.; Narbón, E.S. Prospective follow-up study of artificial urinary sphincter placement preserving the bulbospongiosus muscle. Neurourol. Urodyn. 2017, 36, 1387–1394. [Google Scholar] [CrossRef]
- Kaiho, Y.; Masuda, H.; Takei, M.; Hirayama, T.; Mitsui, T.; Yokoyama, M.; Kitta, T.; Kawamorita, N.; Nakagawa, H.; Iwamura, M.; et al. Surgical and Patient Reported Outcomes of Artificial Urinary Sphincter Implantation: A Multicenter, Prospective, Observational Study. J. Urol. 2018, 199, 245–250. [Google Scholar] [CrossRef]
- Lai, H.H.; Hsu, E.I.; The, B.S.; Butler, E.B.; Boone, T.B. 13 years of experience with artificial urinary sphincter implantation at Baylor College of Medicine. J. Urol. 2007, 177, 1021–1025. [Google Scholar] [CrossRef]
- Rocha, F.T.; Gomes, C.M.; Mitre, A.I.; Arap, S.; Srougi, M. A prospective study evaluating the efficacy of the artificial sphincter AMS 800 for the treatment of postradical prostatectomy urinary incontinence and the correlation between preoperative urodynamic and surgical outcomes. Urology 2008, 71, 85–89. [Google Scholar] [CrossRef]
- Suskind, A.M.; Walter, L.C.; Jin, C.; Boscardin, J.; Sen, S.; Cooperberg, M.R.; Finlayson, E. Impact of frailty on complications in patients undergoing common urological procedures: A study from the American College of Surgeons National Surgical Quality Improvement database. BJU Int. 2016, 117, 836–842. [Google Scholar] [CrossRef]
- Heah, N.H.; Tan, R.B.W. Management of urethral atrophy after implantation of artificial urinary sphincter: What are the weaknesses? Asian J. Androl. 2020, 22, 60–63. [Google Scholar] [CrossRef]
- Kim, S.P.; Sarmast, Z.; Daignault, S.; Faerber, G.J.; McGuire, E.J.; Latini, J.M. Long-term durability and functional outcomes among patients with artificial urinary sphincters: A 10-year retrospective review from the University of Michigan. J. Urol. 2008, 179, 1912–1916. [Google Scholar] [CrossRef] [PubMed]
- Sacco, E.; Bientinesi, R.; Gandi, C.; Di Gianfrancesco, L.; Pierconti, F.; Racioppi, M.; Bassi, P.F. Patient pad count is a poor measure of urinary incontinence compared with 48-h pad test: Results of a large-scale multicentre study. BJU Int. 2019, 123, E69–E78. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | |
|---|---|
| Age, years | 76 (72–78) |
| BMI, kg/m2 | 28 (25–30) |
| CCI | 3 (2–3) |
| Diabetes mellitus, n (%) | 3 (6.38) |
| Oral anticoagulant/antiplatelet, n (%) | 18 (38.29) |
| Median duration of UI, mos | 60 (36–84) |
| Median 24 h PAD weighing test, grams | 750 (655–1200) |
| Median 24 h PAD use, n | 6 (5–6) |
| UI clinical type, n (%) | |
| SUI | 39 (82.97) |
| MUI | 8 (17.02) |
| Previous prostate surgery, n (%) | |
| RARP | 12 (23.53) |
| RRP | 24 (51.06) |
| LRP | 8 (17.02) |
| TURP | 2 (4.25) |
| OSP | 1 (2.13) |
| Previous UI procedures, n (%) | |
| Fixed sling 1 | 8 (17.02) |
| Bulking agent | 13 (27.65) |
| Botulinum toxin | 2 (4.25) |
| Previous pelvic RT, n (%) | 22 (46.80) |
| Previous urethrotomy, n (%) | 18 (38.29) |
| Main urodynamic findings, n (%) 2 | |
| Detrusor overactivity | 9 (24.32) |
| Detrusor underactivity | 13 (35.13) |
| Bladder outlet obstruction | 1 (2.70) |
| Stress incontinence | 37 (100) |
| Maximum cystometric capacity, cmH2O | 300 (180–400) |
| Intraoperative Data | |
|---|---|
| Median operative time (IQR), min | 90 (70–120) |
| Cuff size, n (%) | |
| 3.5 cm | 2 (4.25) |
| 4.0 cm | 14 (29.78) |
| 4.5 cm | 24 (51.06) |
| 5.0 cm | 7 (14.89) |
| Single cuff, n (%) | 43 (91.48) |
| Double cuff, n (%) | 4 (8.51) |
| Associated endoscopic uretrothomy, n (%) | 3 (6.38) |
| Early complications | |
| Scrotal hematoma, n (%) | 2 (4.25) |
| Migrated pump, n (%) | 2 (4.25) |
| Liquid leakage from the connector, n (%) | 1 (2.12) |
| Clavien–Dindo early complications grade, n (%) | |
| Grade 1 | 14 (29.79) |
| Grade ≥ 2 | 3 (6.38) |
| Time Point | 24 h Pad Number | 24 h Pad Weight | ICIQ-SF | ICIQ-QoL | EQ-5D-5L | IIEF-5 * |
|---|---|---|---|---|---|---|
| Baseline (n = 47) | 5.85 ± 1.99 | 984 ± 557.35 | 17.97 ± 2.21 | 8.4 ± 1.48 | 72 ± 14.9 | 13.25± 3.83 |
| 12 mos (n = 47) | 0.72 ± 0.77 (p < 0.0001) | 21.48 ± 40.68 (p < 0.0001) | 4.60 ± 4.61 (p < 0.0001) | 1.78 ± 2.47 (p < 0.0001) | 81 ± 14.2 (p = 0.0002) | 13.75 ± 3.93 (p = 0.76) |
| 5 yrs (n = 28) | 0.84 ± 0.89 (p < 0.0001) | 25.46 ± 46.03 (p < 0.0001) | 4.46 ± 4.83 (p < 0.0001) | 2.28 ± 2.85 (p < 0.0001) | 76 ± 12 (p = 0.0002) | 13.75 ± 3.93 (p = 0.76) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacco, E.; Marino, F.; Gandi, C.; Bientinesi, R.; Totaro, A.; Moretto, S.; Gavi, F.; Campetella, M.; Racioppi, M. Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes. J. Clin. Med. 2023, 12, 3021. https://doi.org/10.3390/jcm12083021
Sacco E, Marino F, Gandi C, Bientinesi R, Totaro A, Moretto S, Gavi F, Campetella M, Racioppi M. Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes. Journal of Clinical Medicine. 2023; 12(8):3021. https://doi.org/10.3390/jcm12083021
Chicago/Turabian StyleSacco, Emilio, Filippo Marino, Carlo Gandi, Riccardo Bientinesi, Angelo Totaro, Stefano Moretto, Filippo Gavi, Marco Campetella, and Marco Racioppi. 2023. "Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes" Journal of Clinical Medicine 12, no. 8: 3021. https://doi.org/10.3390/jcm12083021