
Coronary Microvascular Dysfunction: Features and Prognostic Value
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dynamic Single-Photon Emission Computed Tomography (SPECT)
2.3. Echocardiography
2.4. Blood Sampling and Biochemical Analysis
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical and Demographic Characteristics
3.2. Echocardiographic and Dynamic SPECT Parametrs
3.3. The Levels of Biomarkers
3.4. Diagnostic Value
3.5. Correlative Links
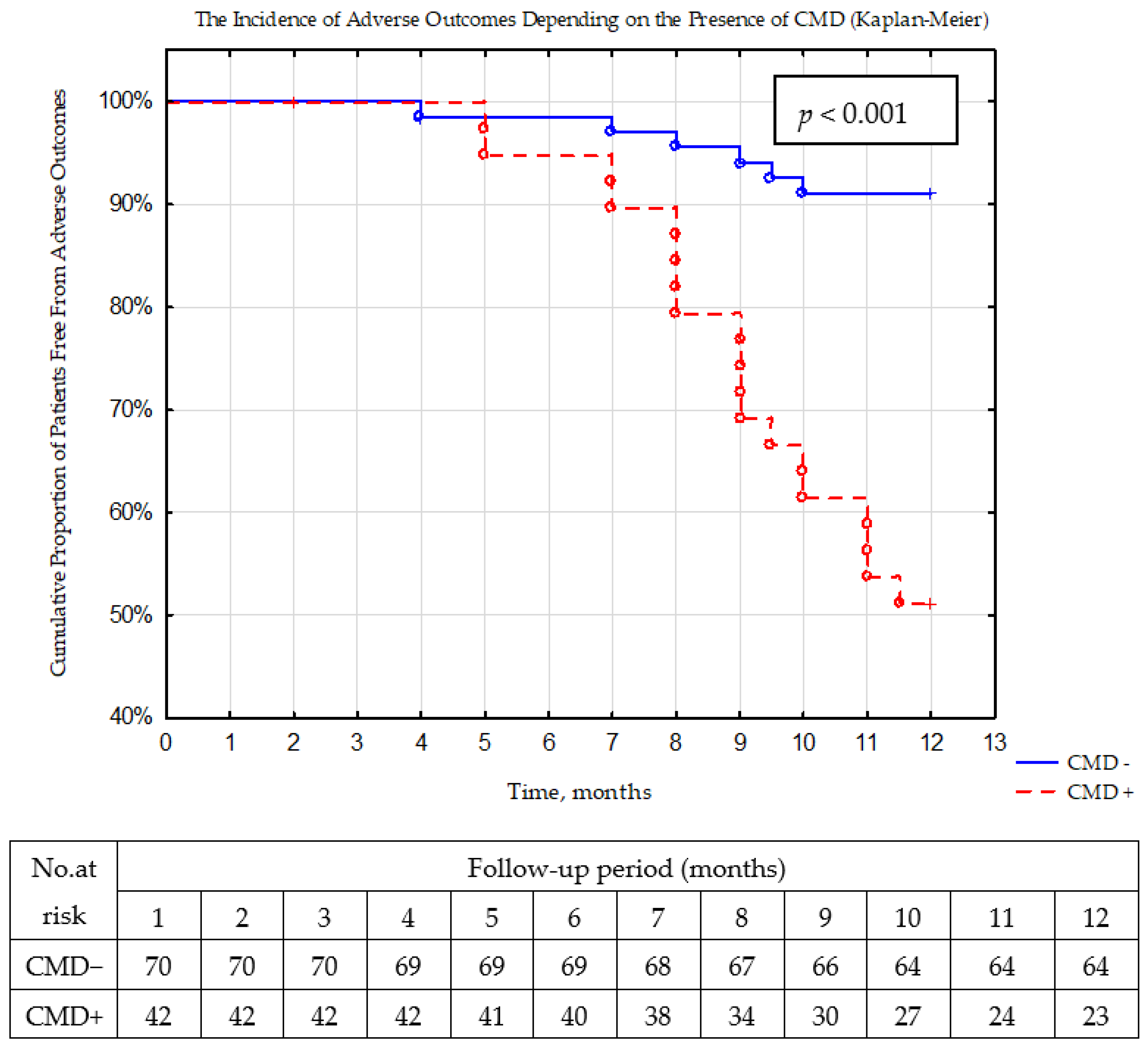
3.6. Prognostic Value
4. Discussion
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masi, S.; Rizzoni, D.; Taddei, S.; Widmer, R.J.; Montezano, A.C.; Lüscher, T.F.; Schiffrin, E.L.; Touyz, R.M.; Paneni, F.; Lerman, A.; et al. Assessment and pathophysiology of microvascular disease: Recent progress and clinical implications. Eur. Heart J. 2021, 42, 2590–2604. [Google Scholar] [CrossRef] [PubMed]
- Houben, A.J.; Stehouwer, C.D. Microvascular dysfunction: Determinants and treatment, with a focus on hyperglycemia. Endocr. Metab. Sci. 2021, 2, 100073. [Google Scholar] [CrossRef]
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1625–1637. [Google Scholar] [CrossRef] [PubMed]
- Likoff, W.; Segal, B.L.; Kasparian, H. Paradox of normal selective coronary arteriograms in patients considered to have unmistakable coronary heart disease. N. Engl. J. Med. 1967, 276, 1063–1066. [Google Scholar] [CrossRef]
- Borbély, A.; van der Velden, J.; Papp, Z.; Bronzwaer, J.G.F.; Edes, I.; Stienen, G.J.M.; Paulus, W.J. Cardiomyocyte stiffness in diastolic heart failure. Circulation 2005, 111, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.L.; Naya, M.; Taqueti, V.R.; Foster, C.R.; Gaber, M.; Hainer, J.; Dorbala, S.; Blankstein, R.; Rimoldi, O.; Camici, P.G.; et al. Effects of sex on coronary microvascular dysfunction and cardiac outcomes. Circulation 2014, 129, 2518–2527. [Google Scholar] [CrossRef] [PubMed]
- Mileva, N.; Nagumo, S.; Mizukami, T.; Sonck, J.; Berry, C.; Gallinoro, E.; Monizzi, G.; Candreva, A.; Munhoz, D.; Vassilev, D.; et al. Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients with Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2022, 11, e023207. [Google Scholar] [CrossRef] [PubMed]
- Rush, C.J.; Berry, C.; Oldroyd, K.G.; Rocchiccioli, J.P.; Lindsay, M.M.; Touyz, R.M.; Murphy, C.L.; Ford, T.J.; Sidik, N.; McEntegart, M.B.; et al. Prevalence of Coronary Artery Disease and Coronary Microvascular Dysfunction in Patients with Heart Failure With Preserved Ejection Fraction. JAMA Cardiol. 2021, 6, 1130–1143. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Lam, C.S.P.; Svedlund, S.; Saraste, A.; Hage, C.; Tan, R.; Beussink-Nelson, L.; Faxén, U.L.; Fermer, M.L.; Broberg, M.A.; et al. Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF. Eur. Heart J. 2018, 39, 3439–3450. [Google Scholar] [CrossRef]
- Liga, R.; Neglia, D.; Kusch, A.; Favilli, B.; Giorgetti, A.; Gimelli, A. Prognostic Role of Dynamic CZT Imaging in CAD Patients: Interaction Between Absolute Flow and CAD Burden. JACC Cardiovasc. Imaging 2022, 15, 540–542. [Google Scholar] [CrossRef]
- Kato, S.; Saito, N.; Kirigaya, H.; Gyotoku, D.; Iinuma, N.; Kusakawa, Y.; Iguchi, K.; Nakachi, T.; Fukui, K.; Futaki, M.; et al. Impairment of coronary flow reserve evaluated by phase contrast cine-magnetic resonance imaging in patients with heart failure with preserved ejection fraction. J. Am. Heart Assoc. 2016, 5, e002649. [Google Scholar] [CrossRef]
- Mohammed, S.F.; Hussain, S.; Mirzoyev, S.A.; Edwards, W.D.; Maleszewski, J.J.; Redfield, M.M. Coronary microvascular rarefaction and myocardial fibrosis in heart failure with preserved ejection fraction. Circulation 2015, 131, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.T.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankstein, R.; et al. Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction. Eur. Heart J. 2018, 39, 840–849. [Google Scholar] [CrossRef]
- Yang, J.H.; Obokata, M.; Reddy, Y.N.; Redfield, M.M.; Lerman, A.; Borlaug, B.A. Endothelium-dependent and independent coronary microvascular dysfunction in patients with heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2020, 22, 432–441. [Google Scholar] [CrossRef]
- Zavadovsky, K.V.; Mochula, A.V.; Boshchenko, A.A.; Vrublevsky, A.V.; Baev, A.E.; Krylov, A.L.; Gulya, M.O.; Nesterov, E.A.; Liga, R.; Gimelli, A. Absolute myocardial blood flows derived by dynamic CZT scan vs invasive fractional flow reserve: Correlation and accuracy. J. Nucl. Cardiol. 2021, 28, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Henzlova, M.J.; Duvall, W.L.; Einstein, A.J.; Travin, M.I.; Verberne, H.J. ASNC imaging guidelines for SPECT nuclear cardiology procedures: Stress, protocols, and tracers. J. Nucl. Cardiol. 2016, 23, 606–639. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart: A Statement for Healthcare Professionals from the Cardiac Imaging. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Jovanovic, I.; Tesic, M.; Giga, V.; Dobric, M.; Boskovic, N.; Vratonjic, J.; Orlic, D.; Gudelj, O.; Tomasevic, M.; Dikic, M.; et al. Impairment of coronary flow velocity reserve and global longitudinal strain in women with cardiac syndrome X and slow coronary flow. J. Cardiol. 2020, 76, 1–8. [Google Scholar] [CrossRef]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726, Erratum in Eur. Heart J. 2021, 42, 4901. [Google Scholar] [CrossRef] [PubMed]
- Weerts, J.; Mourmans, S.G.J.; Aizpurua, A.B.; Schroen, B.L.M.; Knackstedt, C.; Eringa, E.; Houben, A.J.H.M.; van Empel, V.P.M. The Role of Systemic Microvascular Dysfunction in Heart Failure with Preserved Ejection Fraction. Biomolecules 2022, 12, 278. [Google Scholar] [CrossRef]
- Obokata, M.; Reddy, Y.N.; Melenovsky, V.; Kane, G.C.; Olson, T.P.; Jarolim, P.; Borlaug, B.A. Myocardial injury and cardiac reserve in patients with heart failure and preserved ejection fraction. J. Am. Coll. Cardiol. 2018, 72, 29–40. [Google Scholar] [CrossRef]
- Ahmad, A.; Corban, M.T.; Toya, T.; Verbrugge, F.H.; Sara, J.D.; Lerman, L.O.; Borlaug, B.A.; Lerman, A. Coronary microvascular dysfunction is associated with exertional haemodynamic abnormalities in patients with heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2021, 23, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Rahman, H.; Webb, A.; Shah, A.M.; Perera, D. Untangling the pathophysiologic link between coronary microvascular dysfunction and heart failure with preserved ejection fraction. Eur. Heart J. 2021, 42, 4431–4441. [Google Scholar] [CrossRef]
- Boden, W.E.; O’Rourke, R.A.; Teo, K.K.; Hartigan, P.M.; Maron, D.J.; Kostuk, W.J.; Knudtson, M.; Dada, M.; Casperson, P.; Harris, C.L.; et al. Optimal medical therapy with or without PCI for stable coronary disease. N. Engl. J. Med. 2007, 356, 1503–1516. [Google Scholar] [CrossRef]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial invasive or conservative strategy for stable coronary disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Shimokawa, H.; Suda, A.; Takahashi, J.; Berry, C.; Camici, P.G.; Crea, F.; Escaned, J.; Ford, T.; Yii, E.; Kaski, J.C.; et al. Clinical characteristics and prognosis of patients with microvascular angina: An international and prospective cohort study by the Coronary Vasomotor Disorders International Study (COVADIS) Group. Eur. Heart J. 2021, 42, 4592–4600. [Google Scholar] [CrossRef]
- Schroder, J.; Michelsen, M.M.; Mygind, N.D.; E Suhrs, H.; Bove, K.B.; Bechsgaard, D.F.; Aziz, A.; Gustafsson, I.; Kastrup, J.; Prescott, E. Coronary flow velocity reserve predicts adverse prognosis in women with angina and no obstructive coronary artery disease: Results from the iPOWER study. Eur. Heart J. 2021, 42, 228–239. [Google Scholar] [CrossRef]
- Kato, S.; Fukui, K.; Kodama, S.; Azuma, M.; Nakayama, N.; Iwasawa, T.; Kimura, K.; Tamura, K.; Utsunomiya, D. Cardiovascular magnetic resonance assessment of coronary flow reserve improves risk stratification in heart failure with preserved ejection fraction. J. Cardiovasc. Magn. Reson. 2021, 23, 112. [Google Scholar] [CrossRef]
- Gallinoro, E.; Paolisso, P.; Candreva, A.; Bermpeis, K.; Fabbricatore, D.; Esposito, G.; Bertolone, D.; Fernandez Peregrina, E.; Munhoz, D.; Mileva, N.; et al. Microvascular Dysfunction in Patients with Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve. Front. Cardiovasc. Med. 2021, 8, 765071. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Merz, C.N.B.; Beltrame, J.F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Camici, P.G. The parallel tales of microvascular angina and heart failure with preserved ejection fraction: A paradigm shift. Eur. Heart J. 2017, 38, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Filali, Y.; Kesäniemi, A.; Ukkola, O. Soluble ST2, a biomarker of fibrosis, is associated with multiple risk factors, chronic diseases and total mortality in the OPERA study. Scand. J. Clin. Lab. Investig. 2021, 81, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Rehan, R.; Yong, A.; Ng, M.; Weaver, J.; Puranik, R. Coronary microvascular dysfunction: A review of recent progress and clinical implications. Front. Cardiovasc. Med. 2023, 10, 1111721. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | CMD+ n = 47 | CMD− n = 73 | p-Value |
|---|---|---|---|
| Age, years | 61 (56; 68.5) | 61.5 (59; 67.5) | 0.123 |
| Male sex, n (%) | 26 (57.8) | 44 (60.3) | 0.901 |
| Body mass index, kg/m2 | 29.9 (27.8; 31.9) | 30.2 (27.9; 32.1) | 0.276 |
| Hypertension, n (%) | 37 (82.2) | 46 (63.0) | 0.069 |
| Type 2 diabetes mellitus, n (%) | 11 (24.4) | 6 (8.2) | 0.007 |
| History of COVID-19, n (%) | 7 (15.6) | 12 (16.4) | 0.318 |
| COPD, n (%) | 7 (15.6) | 13 (17.8) | 0.723 |
| Paroxysmal AF, n (%) | 7 (15.6) | 11 (15.1) | 0.769 |
| HFpEF, n (%) | 34 (75.6) | 24 (32.9) | <0.001 |
| Smokers, n (%) | 11 (24.4) | 5 (6.8) | 0.009 |
| eGFR (mL/min/1.73 m2) | 77.2 (63.2; 81.2) | 77.0 (64.0; 85.0) | 0.543 |
| Total cholesterol, mmol/L | 4.635 (3.67; 5.25) | 4.33 (3.54; 4.98) | 0.898 |
| LDL-C, mmol/L | 3.12 (2.15; 3.51) | 2.87 (2.25; 3.87) | 0.456 |
| HDL-C, mmol/L | 1.05 (0.83; 1.32) | 1.05 (0.96; 1.26) | 0.887 |
| Triglyceride, mmol/L | 1.67 (1.23; 1.89) | 1.59 (1.22; 1.86) | 0.835 |
| Hemoglobin, g/dL | 134 (121; 143) | 137 (128; 142) | 0.464 |
| Potassium, mmol/L | 4.64 (4.12; 5.01) | 4.81 (4.43; 5.21) | 0.517 |
| Fibrinogen, g/L | 3.27 (3.14; 3.14) | 3.10 (2.86; 3.43) | 0.767 |
| HbA1c, % | 5.9 (5.1; 6.9) | 5.8 (5.1; 6.4) | 0.098 |
| β-blockers, n (%) | 8 (17.8) | 10 (13.7) | 0.876 |
| ACE inhibitors/ARBs, n (%) | 5 (11.1) | 9 (12.0) | 0.879 |
| Diuretics, n (%) | 3 (6.7) | 8 (10.9) | 0.546 |
| Statins, n (%) | 8 (17.8) | 15 (20.5) | 0.547 |
| Amiodarone, n (%) | 2 (4.4) | 5 (6.8) | 0.358 |
| ARA, n (%) | 2 (4.4) | 4 (5.5) | 0.269 |
| Parameter | CMD+ n = 47 | CMD− n = 73 | p-Value |
|---|---|---|---|
| Echocardiographic parametrs | |||
| Left ventricle ejection fraction, % | 62 (58.5; 65.0) | 63 (61; 66) | 0.183 |
| End-systolic dimension, mm | 40 (38; 43) | 38.5 (36.5; 41.5) | 0.524 |
| End-diastolic dimension, mm | 51.0 (48.7; 53.0) | 50.5 (47.5; 52.5) | 0.307 |
| LVMMi, g/m2 | 98.0 (88.5; 114.5) | 92 (85.5; 106.5) | 0.276 |
| E/A ratio | 1.04 (0.79; 1.3) | 0.97 (0.74; 1.2) | 0.516 |
| Lateral e′, sm/s | 5.56 (4.78; 6.45) | 8.56 (8.01; 9.14) | 0.009 |
| TRV, m/s | 2.99 (2.95; 3.01) | 2.63 (2.3; 2.76) | 0.011 |
| E/e′ ratio | 14 (13.5; 15.0) | 11 (10; 12) | 0.041 |
| LAVI, mL/m2 | 38.3 (35.7; 51.1) | 29.7 (27.5; 47.9) | 0.038 |
| LV global longitudinal strain, % | −14.7 (−12.9; −16.9) | −20.9 (16.1; 21.6) | 0.005 |
| Diastolic dysfunction, n (%) | 37 (88.1) | 26 (37.1) | <0.001 |
| Dynamic SPECT parametrs | |||
| Stress-MBF, mL/min/g | 1.14 (0.67; 1.49) | 1.63 (1.19; 1.83) | <0.001 |
| Rest-MBF, mL/min/g | 0.75 (0.54; 0.99) | 0.52 (0.40; 0.69) | <0.001 |
| Myocardial flow reserve | 1.39 (1.11; 1.96) | 2.69 (2.15; 3.78) | <0.001 |
| Standard semi-quantitative indices of myocardial perfusion imaging | |||
| Summed stress score | 3 (0.5; 4) | 2.5 (0; 5) | 0.753 |
| Summed rest scores | 2 (0; 3) | 1 (0; 2) | 0.537 |
| Difference between stress and rest score | 2 (0; 3) | 2 (0; 4) | 0.975 |
| Parameter | CMD+ n = 47 | CMD− n = 73 | p-Value |
| NT-proBNP, pg/mL | 404.2 (249.5; 1533.4) | 156.3 (135.26; 274.7) | 0.004 |
| IL-10, pg/mL (N < 10 pg/mL) | 2.87 (2.58; 3.57) | 3.67 (3.32; 4.04) | 0.048 |
| IL-1β, pg/mL (N < 11 pg/mL) | 3.19 (1.64; 5.47) | 1.2 (0.74; 1.48) | 0.046 |
| IL-6, pg/mL (N < 31 pg/mL) | 2.65 (1.98; 3.98) | 2.48 (1.87; 3.76) | 0.842 |
| hsCRP, g/L (N < 12 g/L) | 4.1 (3.0; 11.4) | 2.3 (1.1; 8.7) | 0.009 |
| Soluble ST2, ng/mL | 33.67 (27.65; 38.9) | 27.5 (21.78; 30.09) | <0.001 |
| TIMP-1, ng/mL | 287.4 (107.38; 371.8) | 123.64 (58.66; 232.9) | 0.011 |
| MMP-9, ng/mL | 2109 (1145.7; 3235) | 1104 (721.5; 1731.9) | 0.012 |
| Tetranectin, ng/mL | 6.83 (6.31; 7.68) | 7.03 (6.29; 7.82) | 0.786 |
| FGF-23, ng/mL | 0.691 (0.465; 1.042) | 0.672 (0.509; 0.976) | 0.567 |
| Parameter | Odds Ration | 95% CI | p-Value |
|---|---|---|---|
| Univariate regression analysis | |||
| Type 2 diabetes mellitus | 1.43 | 1.17–3.57 | 0.012 |
| NT-proBNP (<760.5/≥760.5 pg/mL) | 2.13 | 1.78–4.87 | 0.009 |
| hsCRP (<3.2/≥3.2 g/L) | 1.63 | 0.98–2.54 | 0.013 |
| Diastolic dysfunction | 3.18 | 1.16–4.12 | <0.001 |
| Smoking | 2.01 | 0.99–2.43 | 0.043 |
| Soluble ST2 (<31.4/≥31.4 ng/mL) | 1.97 | 1.16–5.12 | 0.003 |
| Multivariate regression analysis | |||
| Diastolic dysfunction | 3.27 | 2.26–5.64 | <0.001 |
| NT-proBNP (<760.5/≥760.5 pg/mL) | 1.67 | 1.12–4.15 | 0.021 |
| Soluble ST2 (<31.4/≥31.4 ng/mL) | 1.33 | 1.08–3.19 | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopeva, K.; Grakova, E.; Maltseva, A.; Mochula, A.; Gusakova, A.; Smorgon, A.; Zavadovsky, K. Coronary Microvascular Dysfunction: Features and Prognostic Value. J. Clin. Med. 2023, 12, 2964. https://doi.org/10.3390/jcm12082964
Kopeva K, Grakova E, Maltseva A, Mochula A, Gusakova A, Smorgon A, Zavadovsky K. Coronary Microvascular Dysfunction: Features and Prognostic Value. Journal of Clinical Medicine. 2023; 12(8):2964. https://doi.org/10.3390/jcm12082964
Chicago/Turabian StyleKopeva, Kristina, Elena Grakova, Alina Maltseva, Andrew Mochula, Anna Gusakova, Andrew Smorgon, and Konstantin Zavadovsky. 2023. "Coronary Microvascular Dysfunction: Features and Prognostic Value" Journal of Clinical Medicine 12, no. 8: 2964. https://doi.org/10.3390/jcm12082964