


Effect of Anthropometric Parameters on Achilles Tendon Stiffness of Professional Athletes Measured by Shear Wave Elastography
 , and
, and
Abstract
:1. Introduction
Objective
2. Methods
2.1. Study Population
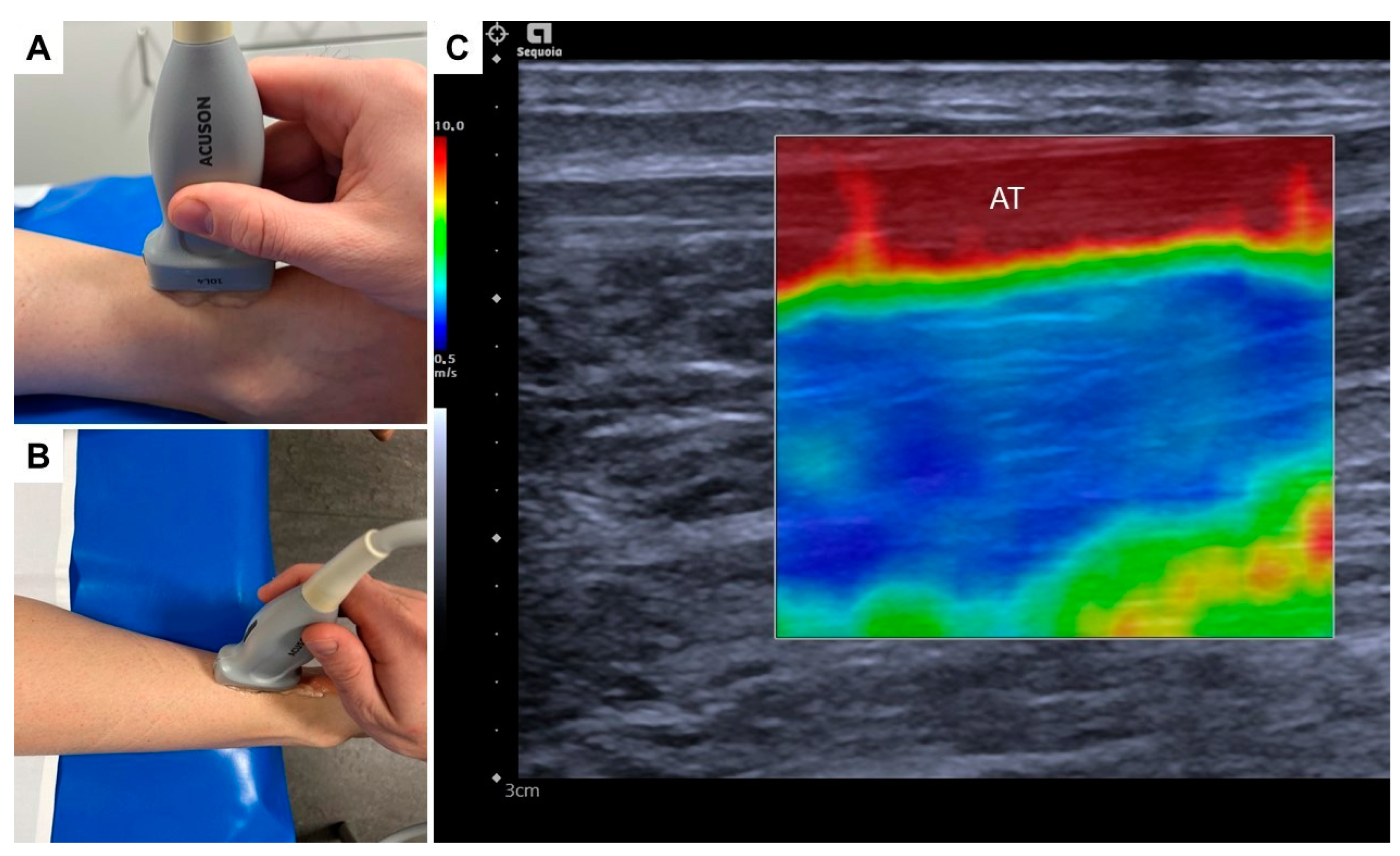
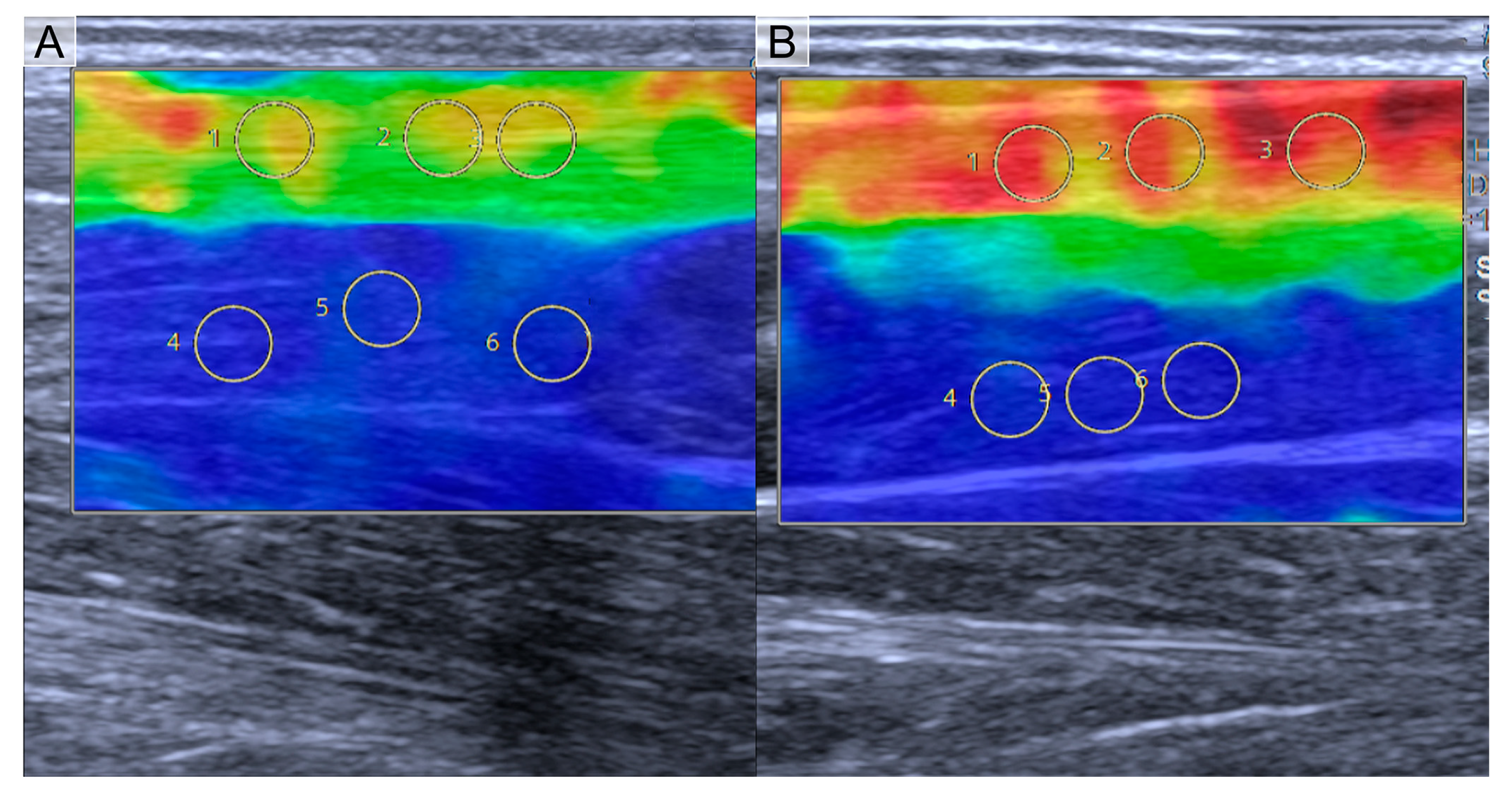
2.2. Shear Wave Elastography Examination
2.3. Statistical Analysis
3. Results
3.1. Athletes’ Characteristics
3.2. Results of US-SWE in Professional Athletes
4. Discussion
4.1. Influence of Anthropometric Parameters on Achilles Tendon Stiffness
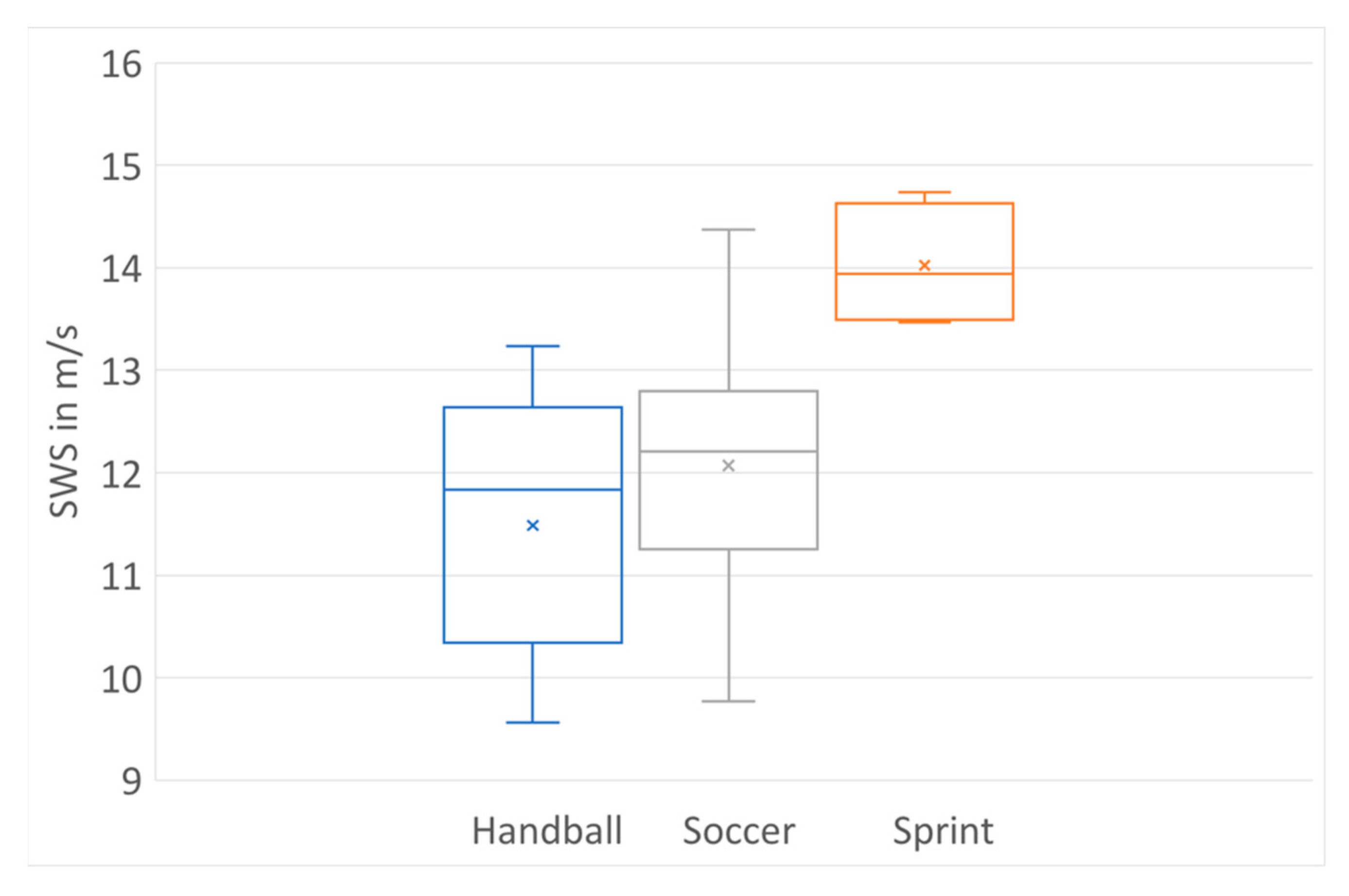
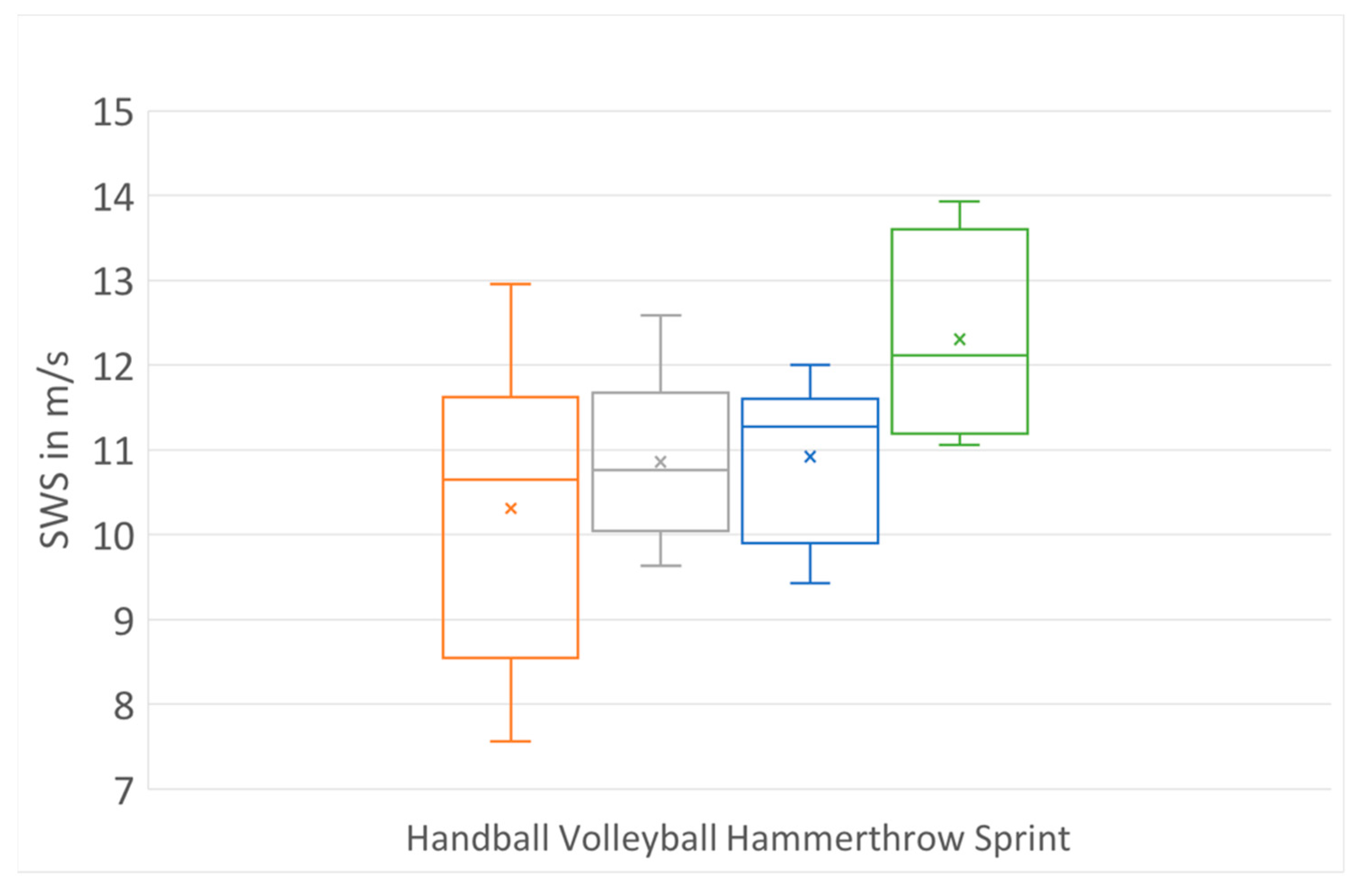
4.2. Achilles Tendon Stiffness in Different Sports
4.3. Role of SWE in Assessment of Achilles Tendon
4.4. Future Aspects in SWE
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AT | Achilles tendon |
| BMI | Body mass index |
| MSK | Musculoskeletal |
| ROI | Region of interest |
| SWE | Shear wave elastography |
| SWS | Shear wave speed |
| US | Ultrasound |
References
- Kannus, P.; Natri, A. Etiology and pathophysiology of tendon ruptures in sports. Scand. J. Med. Sci. Sport. 1997, 7, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Coombes, B.K.; Tucker, K.; Vicenzino, B.; Vuvan, V.; Mellor, R.; Heales, L.; Nordez, A.; Hug, F. Achilles and patellar tendinopathy display opposite changes in elastic properties: A shear wave elastography study. Scand. J. Med. Sci. Sport. 2018, 28, 1201–1208. [Google Scholar] [CrossRef]
- Zhang, L.N.; Wan, W.B.; Wang, Y.X.; Jiao, Z.Y.; Zhang, L.H.; Luo, Y.K.; Tang, P.F. Evaluation of Elastic Stiffness in Healing Achilles Tendon After Surgical Repair of a Tendon Rupture Using In Vivo Ultrasound Shear Wave Elastography. Med. Sci. Monit. 2016, 22, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Vleck, V.E.; Garbutt, G. Injury and training characteristics of male Elite, Development Squad, and Club triathletes. Int. J. Sports Med. 1998, 19, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Sun, Y.; Liu, L.; Wang, Z.; Wu, J.Y.; Qiu, L.; Wang, Y.X.; Yuan, Y.; Shen, S.F.; Chen, Q.; et al. A Multicenter Large-Sample Shear Wave Ultrasound Elastographic Study of the Achilles Tendon in Chinese Adults. J. Ultrasound Med. 2019, 38, 1191–1200. [Google Scholar] [CrossRef]
- Abate, M.; Silbernagel, K.G.; Siljeholm, C.; Di Iorio, A.; De Amicis, D.; Salini, V.; Werner, S.; Paganelli, R. Pathogenesis of tendinopathies: Inflammation or degeneration? Arthritis Res. Ther. 2009, 11, 235. [Google Scholar] [CrossRef]
- Breda, S.J.; van der Vlist, A.; de Vos, R.J.; Krestin, G.P.; Oei, E.H.G. The association between patellar tendon stiffness measured with shear-wave elastography and patellar tendinopathy-a case-control study. Eur. Radiol. 2020, 30, 5942–5951. [Google Scholar] [CrossRef]
- Ozcan, A.N.; Tan, S.; Tangal, N.G.; Ciraci, S.; Kudas, S.; Bektaser, S.B.; Arslan, H. Real-time sonoelastography of the patellar and quadriceps tendons: Pattern description in professional athletes and healthy volunteers. Med. Ultrason. 2016, 18, 299–304. [Google Scholar] [CrossRef]
- Dirrichs, T.; Quack, V.; Gatz, M.; Tingart, M.; Kuhl, C.K.; Schrading, S. Shear Wave Elastography (SWE) for the Evaluation of Patients with Tendinopathies. Acad Radiol. 2016, 23, 1204–1213. [Google Scholar] [CrossRef]
- Dirrichs, T.; Quack, V.; Gatz, M.; Tingart, M.; Rath, B.; Betsch, M.; Kuhl, C.K.; Schrading, S. Shear Wave Elastography (SWE) for Monitoring of Treatment of Tendinopathies: A Double-blinded, Longitudinal Clinical Study. Acad Radiol. 2018, 25, 265–272. [Google Scholar] [CrossRef]
- Taljanovic, M.S.; Gimber, L.H.; Becker, G.W.; Latt, L.D.; Klauser, A.S.; Melville, D.M.; Gao, L.; Witte, R.S. Shear-Wave Elastography: Basic Physics and Musculoskeletal Applications. Radiographics 2017, 37, 855–870. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, I.; Coombes, B.K.; Tucker, K.; Hug, F.; Dick, T.J.M. Age-related differences in gastrocnemii muscles and Achilles tendon mechanical properties in vivo. J. Biomech. 2020, 112, 110067. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yu, H.K.; Sheng, S.Y.; Liang, S.M.; Lu, H.; Chen, R.Y.; Pan, M.; Wen, Z.B. Quantitative evaluation of passive muscle stiffness by shear wave elastography in healthy individuals of different ages. Eur. Radiol. 2021, 31, 3187–3194. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Wu, M.; Liu, X.; Gao, K.; Liu, Y.; Zhang, Y.; Zhang, E.; Zhang, T. Age-Related Changes in Shear Wave Elastography Parameters of the Gastrocnemius Muscle in Association with Physical Performance in Healthy Adults. Gerontology 2021, 67, 306–313. [Google Scholar] [CrossRef]
- Turan, A.; Teber, M.A.; Yakut, Z.I.; Unlu, H.A.; Hekimoglu, B. Sonoelastographic assessment of the age-related changes of the Achilles tendon. Med. Ultrason 2015, 17, 58–61. [Google Scholar] [CrossRef]
- De Zordo, T.; Fink, C.; Feuchtner, G.M.; Smekal, V.; Reindl, M.; Klauser, A.S. Real-time sonoelastography findings in healthy Achilles tendons. AJR Am. J. Roentgenol. 2009, 193, W134–W138. [Google Scholar] [CrossRef] [PubMed]
- Slane, L.C.; Martin, J.; DeWall, R.; Thelen, D.; Lee, K. Quantitative ultrasound mapping of regional variations in shear wave speeds of the aging Achilles tendon. Eur. Radiol. 2017, 27, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Couppe, C.; Hansen, P.; Kongsgaard, M.; Kovanen, V.; Suetta, C.; Aagaard, P.; Kjaer, M.; Magnusson, S.P. Mechanical properties and collagen cross-linking of the patellar tendon in old and young men. J. Appl. Physiol. (1985) 2009, 107, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Sconfienza, L.M.; Albano, D.; Allen, G.; Bazzocchi, A.; Bignotti, B.; Chianca, V.; Facal de Castro, F.; Drakonaki, E.E.; Gallardo, E.; Gielen, J.; et al. Clinical indications for musculoskeletal ultrasound updated in 2017 by European Society of Musculoskeletal Radiology (ESSR) consensus. Eur. Radiol. 2018, 28, 5338–5351. [Google Scholar] [CrossRef]
- Tas, S.; Salkin, Y. An investigation of the sex-related differences in the stiffness of the Achilles tendon and gastrocnemius muscle: Inter-observer reliability and inter-day repeatability and the effect of ankle joint motion. Foot 2019, 41, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Arda, K.; Ciledag, N.; Aktas, E.; Aribas, B.K.; Kose, K. Quantitative assessment of normal soft-tissue elasticity using shear-wave ultrasound elastography. AJR Am. J. Roentgenol. 2011, 197, 532–536. [Google Scholar] [CrossRef]
- Fu, S.; Cui, L.; He, X.; Sun, Y. Elastic Characteristics of the Normal Achilles Tendon Assessed by Virtual Touch Imaging Quantification Shear Wave Elastography. J. Ultrasound Med. 2016, 35, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- Romer, C.; Czupajllo, J.; Zessin, E.; Fischer, T.; Wolfarth, B.; Lerchbaumer, M.H. Stiffness of Muscles and Tendons of the Lower Limb of Professional and Semiprofessional Athletes Using Shear Wave Elastography. J. Ultrasound Med. 2022, 41, 3061–3068. [Google Scholar] [CrossRef]
- Wiesinger, H.P.; Kosters, A.; Muller, E.; Seynnes, O.R. Effects of Increased Loading on In Vivo Tendon Properties: A Systematic Review. Med. Sci. Sport. Exerc. 2015, 47, 1885–1895. [Google Scholar] [CrossRef]
- Tas, S.; Onur, M.R.; Yilmaz, S.; Soylu, A.R.; Korkusuz, F. Shear Wave Elastography Is a Reliable and Repeatable Method for Measuring the Elastic Modulus of the Rectus Femoris Muscle and Patellar Tendon. J. Ultrasound Med. 2017, 36, 565–570. [Google Scholar] [CrossRef]
- Al-Qahtani, M.; Al-Tayyar, S.; Mirza, E.H.; Al-Musallam, A.; Al-Suwayyid, A.; Javed, R. Body Mass Index and Segmental Mass Correlation With Elastographic Strain Ratios of the Quadriceps Tendon. J. Ultrasound Med. 2019, 38, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Petrescu, P.H.; Izvernariu, D.A.; Iancu, C.; Dinu, G.O.; Crisan, D.; Popescu, S.A.; Sirli, R.L.; Nistor, B.M.; RauTia, I.C.; Lazureanu, D.C.; et al. Evaluation of normal and pathological Achilles tendon by real-time shear wave elastography. Rom. J. Morphol. Embryol. 2016, 57, 785–790. [Google Scholar]
- Romer, C.; Czupajllo, J.; Zessin, E.; Fischer, T.; Wolfarth, B.; Lerchbaumer, M.H. Muscle and Tendon Stiffness of the Lower Limb of Professional Adolescent Soccer Athletes Measured Using Shear Wave Elastography. Diagnostics 2022, 12, 2453. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Oliva, F.; Schiavone, C.; Salini, V. Achilles tendinopathy in amateur runners: Role of adiposity (Tendinopathies and obesity). Muscles Ligaments Tendons J. 2012, 2, 44–48. [Google Scholar]
- Esmaeili, A.; Stewart, A.M.; Hopkins, W.G.; Elias, G.P.; Aughey, R.J. Effects of Training Load and Leg Dominance on Achilles and Patellar Tendon Structure. Int. J. Sport. Physiol. Perform. 2017, 12, S2122–S2126. [Google Scholar] [CrossRef]
- Dirrichs, T.; Schrading, S.; Gatz, M.; Tingart, M.; Kuhl, C.K.; Quack, V. Shear Wave Elastography (SWE) of Asymptomatic Achilles Tendons: A Comparison Between Semiprofessional Athletes and the Nonathletic General Population. Acad Radiol. 2019, 26, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Wiesinger, H.P.; Rieder, F.; Kosters, A.; Muller, E.; Seynnes, O.R. Are Sport-Specific Profiles of Tendon Stiffness and Cross-Sectional Area Determined by Structural or Functional Integrity? PLoS ONE 2016, 11, e0158441. [Google Scholar] [CrossRef] [PubMed]
- Lorimer, A.V.; Hume, P.A. Stiffness as a Risk Factor for Achilles Tendon Injury in Running Athletes. Sport. Med. 2016, 46, 1921–1938. [Google Scholar] [CrossRef]
- Frankewycz, B.; Penz, A.; Weber, J.; da Silva, N.P.; Freimoser, F.; Bell, R.; Nerlich, M.; Jung, E.M.; Docheva, D.; Pfeifer, C.G. Achilles tendon elastic properties remain decreased in long term after rupture. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
- Tas, S.; Yilmaz, S.; Onur, M.R.; Soylu, A.R.; Altuntas, O.; Korkusuz, F. Patellar tendon mechanical properties change with gender, body mass index and quadriceps femoris muscle strength. Acta Orthop. Traumatol. Turc. 2017, 51, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Schimpchen, J.; Skorski, S.; Nopp, S.; Meyer, T. Are "classical" tests of repeated-sprint ability in football externally valid? A new approach to determine in-game sprinting behaviour in elite football players. J. Sport. Sci. 2016, 34, 519–526. [Google Scholar] [CrossRef]
- Lorimer, A.V.; Hume, P.A. Achilles tendon injury risk factors associated with running. Sport. Med. 2014, 44, 1459–1472. [Google Scholar] [CrossRef]
- Kinner, B.; Seemann, M.; Roll, C.; Schlumberger, A.; Englert, C.; Nerlich, M.; Prantl, L. Sports and activities after achilles tendon injury of the recreational athlete. Sportverletz. Sportschaden. 2009, 23, 210–216. [Google Scholar] [CrossRef]
- Caldwell, J.E.; Vosseller, J.T. Maximizing Return to Sports After Achilles Tendon Rupture in Athletes. Foot. Ankle Clin. 2019, 24, 439–445. [Google Scholar] [CrossRef]
- Cetti, R.; Christensen, S.E.; Ejsted, R.; Jensen, N.M.; Jorgensen, U. Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature. Am. J. Sport. Med. 1993, 21, 791–799. [Google Scholar] [CrossRef]
- Wise, P.M.; King, J.L.; Stauch, C.M.; Walley, K.C.; Aynardi, M.C.; Gallo, R.A. Outcomes of NCAA Defensive Football Players Following Achilles Tendon Repair. Foot Ankle Int. 2020, 41, 398–402. [Google Scholar] [CrossRef]
- Mansfield, K.; Dopke, K.; Koroneos, Z.; Bonaddio, V.; Adeyemo, A.; Aynardi, M. Achilles Tendon Ruptures and Repair in Athletes-a Review of Sports-Related Achilles Injuries and Return to Play. Curr. Rev. Musculoskelet. Med. 2022, 15, 353–361. [Google Scholar] [CrossRef]
- Knobloch, K.; Thermann, H.; Hufner, T. Achilles tendon rupture--early functional and surgical options with special emphasis on rehabilitation issues. Sportverletz. Sportschaden. 2007, 21, 34–40. [Google Scholar] [CrossRef]
- Majewski, M.; Schaeren, S.; Kohlhaas, U.; Ochsner, P.E. Postoperative rehabilitation after percutaneous Achilles tendon repair: Early functional therapy versus cast immobilization. Disabil. Rehabil. 2008, 30, 1726–1732. [Google Scholar] [CrossRef]
- Rettig, A.C.; Liotta, F.J.; Klootwyk, T.E.; Porter, D.A.; Mieling, P. Potential risk of rerupture in primary achilles tendon repair in athletes younger than 30 years of age. Am. J. Sport. Med. 2005, 33, 119–123. [Google Scholar] [CrossRef]
- Payne, C.; Watt, P.; Cercignani, M.; Webborn, N. Reproducibility of shear wave elastography measuresof the Achilles tendon. Skeletal. Radiol. 2018, 47, 779–784. [Google Scholar] [CrossRef]
- Prado-Costa, R.; Rebelo, J.; Monteiro-Barroso, J.; Preto, A.S. Ultrasound elastography: Compression elastography and shear-wave elastography in the assessment of tendon injury. Insights Imaging 2018, 9, 791–814. [Google Scholar] [CrossRef] [PubMed]
- Ivanac, G.; Lemac, D.; Kosovic, V.; Bojanic, K.; Cengic, T.; Dumic-Cule, I.; Pecina, M.; Brkljacic, B. Importance of shear-wave elastography in prediction of Achilles tendon rupture. Int. Orthop. 2021, 45, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.; Black, K. Choosing a combined oral contraceptive pill. Aust. Prescr. 2015, 38, 6–11. [Google Scholar] [CrossRef]
- Bennink, H.J. Reprint of Are all estrogens the same? Maturitas 2008, 61, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Romer, C.; Czupajllo, J.; Wolfarth, B.; Lerchbaumer, M.H.; Legerlotz, K. Effects of orally administered hormonal contraceptives on the musculoskeletal system of healthy premenopausal women-A systematic review. Health Sci. Rep. 2022, 5, e776. [Google Scholar] [CrossRef]
- Arendt, E.A.; Bershadsky, B.; Agel, J. Periodicity of noncontact anterior cruciate ligament injuries during the menstrual cycle. J. Gend Specif. Med. 2002, 5, 19–26. [Google Scholar] [PubMed]
- Legerlotz, K.; Nobis, T. Insights in the Effect of Fluctuating Female Hormones on Injury Risk-Challenge and Chance. Front. Physiol. 2022, 13, 827726. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.R.; Napier, C.; Willy, R.W.; Stellingwerff, T. Moving Beyond Weekly “Distance”: Optimizing Quantification of Training Load in Runners. J. Orthop. Sport. Phys. Ther. 2020, 50, 564–569. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 32) | Female (n = 33) | |||
|---|---|---|---|---|
| Mean & Range | Mean & Range | |||
| AT | 12.19 | 11.25–14.74 | 10.98 | 10.15–11.65 |
| Age | 19.83 | 18.00–21.00 | 20.76 | 18.00–24.50 |
| BMI | 23.52 | 22.40–24.43 | 23.34 | 21.30–24.38 |
| Coefficient | Standard Error | p Value | |
|---|---|---|---|
| Bias | 4.24 | 25.48 | 0.8686 |
| Gender (m = 1, f = 0) | −1.34 | 0.42 | 0.0021 |
| Age | 0.02 | 0.05 | 0.7060 |
| Height | 4.40 | 14.09 | 0.7561 |
| Weight | -0.05 | 0.16 | 0.7545 |
| BMI | 0.16 | 0.53 | 0.7697 |
| Coefficient | Standard Error | p Value | |
|---|---|---|---|
| Bias | 10.98 | 0.22 | <0.0001 |
| Gender (m = 1, f = 0) | 1.20 | 0.32 | 0.0003 |
| R² (adjusted) | 0.17 | ||
| Standard error | 1.29 m/s | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Römer, C.; Zessin, E.; Czupajllo, J.; Fischer, T.; Wolfarth, B.; Lerchbaumer, M.H. Effect of Anthropometric Parameters on Achilles Tendon Stiffness of Professional Athletes Measured by Shear Wave Elastography. J. Clin. Med. 2023, 12, 2963. https://doi.org/10.3390/jcm12082963
Römer C, Zessin E, Czupajllo J, Fischer T, Wolfarth B, Lerchbaumer MH. Effect of Anthropometric Parameters on Achilles Tendon Stiffness of Professional Athletes Measured by Shear Wave Elastography. Journal of Clinical Medicine. 2023; 12(8):2963. https://doi.org/10.3390/jcm12082963
Chicago/Turabian StyleRömer, Claudia, Enrico Zessin, Julia Czupajllo, Thomas Fischer, Bernd Wolfarth, and Markus Herbert Lerchbaumer. 2023. "Effect of Anthropometric Parameters on Achilles Tendon Stiffness of Professional Athletes Measured by Shear Wave Elastography" Journal of Clinical Medicine 12, no. 8: 2963. https://doi.org/10.3390/jcm12082963