
Association between Chronic Kidney Disease and Sudden Sensorineural Hearing Loss: A Longitudinal Follow-Up Studies Using ICD-10 Codes in a National Health Screening Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Data Collection
2.3. Exposure (Chronic Kidney Disease)
2.4. Outcome (Sudden Sensorineural Hearing Loss)
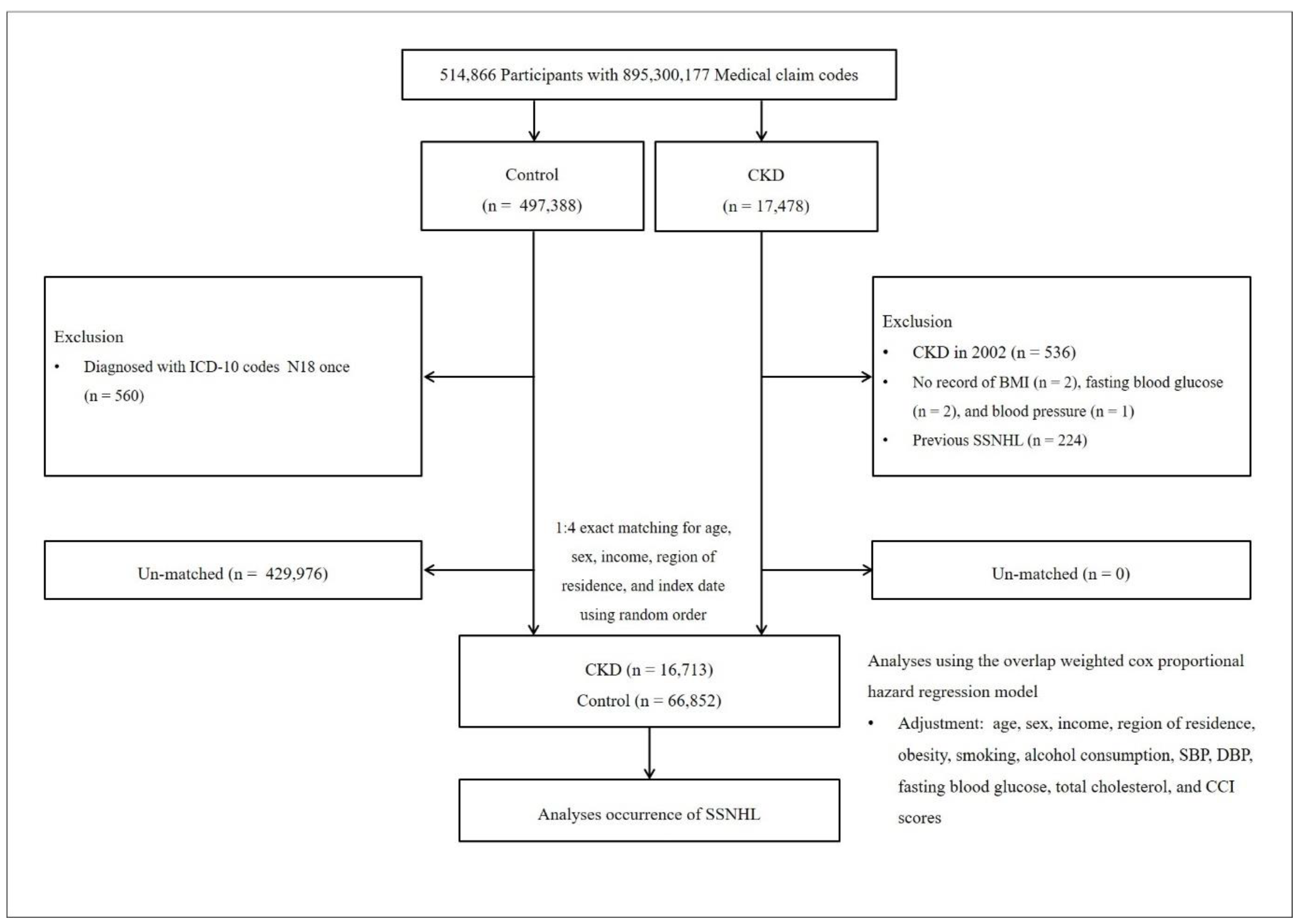
2.5. Participant Selection
2.6. Covariates
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [Green Version]
- Hanna, R.M.; Streja, E.; Kalantar-Zadeh, K. Burden of Anemia in Chronic Kidney Disease: Beyond Erythropoietin. Adv. Ther. 2021, 38, 52–75. [Google Scholar] [CrossRef]
- Hughes, G.B.; Freedman, M.A.; Haberkamp, T.J.; Guay, M.E. Sudden sensorineural hearing loss. Otolaryngol. Clin. N. Am. 1996, 29, 393–405. [Google Scholar] [CrossRef]
- Greco, A.; Fusconi, M.; Gallo, A.; Marinelli, C.; Macri, G.F.; De Vincentiis, M. Sudden sensorineural hearing loss: An autoimmune disease? Autoimmun. Rev. 2011, 10, 756–761. [Google Scholar] [CrossRef]
- Thodi, C.; Thodis, E.; Danielides, V.; Pasadakis, P.; Vargemezis, V. Hearing in renal failure. Nephrol. Dial. Transplant. 2006, 21, 3023–3030. [Google Scholar] [CrossRef] [Green Version]
- Jakic, M.; Mihaljevic, D.; Zibar, L.; Jakic, M.; Kotromanovic, Z.; Roguljic, H. Sensorineural hearing loss in hemodialysis patients. Coll. Antropol. 2010, 34, 165–171. [Google Scholar]
- Kim, J.Y.; Lee, S.; Cha, J.; Son, G.; Kim, D.K. Chronic kidney disease is associated with increased risk of sudden sensorineural hearing loss and Meniere’s disease: A nationwide cohort study. Sci. Rep. 2021, 11, 20194. [Google Scholar] [CrossRef]
- Lin, C.; Hsu, H.T.; Lin, Y.S.; Weng, S.F. Increased risk of getting sudden sensorineural hearing loss in patients with chronic kidney disease: A population-based cohort study. Laryngoscope 2013, 123, 767–773. [Google Scholar] [CrossRef]
- Wang, I.K.; Wang, C.Y.; Muo, C.H.; Yen, T.H.; Sung, F.C. Risk of sudden sensorineural hearing loss in patients with end-stage renal disease undergoing dialysis. Nephrology 2017, 22, 397–402. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, R.; Su, J. Sudden sensorineural hearing loss with end-stage renal disease: A report of 32 cases. Acta Otolaryngol. 2019, 139, 1004–1007. [Google Scholar] [CrossRef]
- Kang, S.M.; Lim, H.W.; Yu, H. Idiopathic sudden sensorineural hearing loss in dialysis patients. Ren. Fail 2018, 40, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional association between GERD and asthma: Two longitudinal follow-up studies using a national sample cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e1009. [Google Scholar] [CrossRef]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Li, F.; Morgan, K.L.; Zaslavsky, A.M. Balancing covariates via propensity score weighting. J. Am. Stat. Assoc. 2018, 113, 390–400. [Google Scholar] [CrossRef] [Green Version]
- Thomas, L.E.; Li, F.; Pencina, M.J. Overlap weighting: A propensity score method that mimics attributes of a randomized clinical trial. Jama 2020, 323, 2417–2418. [Google Scholar] [CrossRef]
- Li, F.; Thomas, L.E.; Li, F. Addressing extreme propensity scores via the overlap weights. Am. J. Epidemiol. 2019, 188, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Cuna, V.; Battaglino, G.; Capelli, I.; Sala, E.; Donati, G.; Cianciolo, G.; La Manna, G. Hypoacusia and chronic renal dysfunction: New etiopathogenetic prospective. Apher Dial 2015, 19, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Vaccaro, F.; Mulè, G.; Cottone, S.; Soresi, M.; Giannitrapani, L.; Vadalà, A.; Sparacino, V.; Calabrese, S.; Picone, F.P.; Montalto, G. Circulating levels of adhesion molecules in chronic kidney disease correlate with the stage of renal disease and with C-reactive protein. Arch. Med. Res. 2007, 38, 534–538. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Lindholm, B.; Heimbürger, M.; Heimbürger, O. Elevated serum levels of soluble adhesion molecules predict death in pre-dialysis patients: Association with malnutrition, inflammation, and cardiovascular disease. Nephrol. Dial. Transplant. 2000, 15, 1624–1630. [Google Scholar] [CrossRef]
- Kurkijärvi, R.; Jalkanen, S.; Isoniemi, H.; Salmi, M. Vascular adhesion protein-1 (VAP-1) mediates lymphocyte-endothelial interactions in chronic kidney rejection. Eur. J. Immunol. 2001, 31, 2876–2884. [Google Scholar] [CrossRef]
- Pertosa, G.; Grandaliano, G.; Gesualdo, L.; Schena, F.P. Clinical relevance of cytokine production in hemodialysis. Kidney Int. 2000, 58, S104–S111. [Google Scholar] [CrossRef] [Green Version]
- Krieglstein, C.F.; Granger, D.N. Adhesion molecules and their role in vascular disease. Am. J. Hypertens. 2001, 14, 44S–54S. [Google Scholar] [CrossRef] [Green Version]
- Quaranta, N.; Ramunni, A.; Brescia, P.; D’Elia, A.; Vacca, A.; Ria, R. Soluble intercellular adhesion molecule 1 and soluble vascular cell adhesion molecule 1 in sudden hearing loss. Otol. Neurotol. 2008, 29, 470–474. [Google Scholar] [CrossRef]
- Ramunni, A.; Quaranta, N.; Saliani, M.T.; Fallacara, R.A.; Ria, R.; Ranieri, G. Does a reduction of adhesion molecules by LDL-apheresis have a role in the treatment of sudden hearing loss? Ther. Apher. Dial. 2006, 10, 282–286. [Google Scholar] [CrossRef]
- Annuk, M.; Zilmer, M.; Fellström, B. Endothelium-dependent vasodilation and oxidative stress in chronic renal failure: Impact on cardiovascular disease. Kidney Int. 2003, 63, S50–S53. [Google Scholar] [CrossRef] [Green Version]
- Abdelwhab, S.; Lotfy, G.; Abdelmaksoud, S. Relation between asymmetric dimethylarginine (ADMA) and hearing loss in patients with renal impairment. Ren. Fail. 2008, 30, 877–883. [Google Scholar] [CrossRef]
- Gusbeth-Tatomir, P.; Covic, A. Causes and consequences of increased arterial stiffness in chronic kidney disease patients. Kidney Blood Press. Res. 2007, 30, 97–107. [Google Scholar] [CrossRef]
- Drueke, T.B.; Massy, Z.A. Atherosclerosis in CKD: Differences from the general population. Nat. Rev. Nephrol. 2010, 6, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.R.S.; Schoueri, J.H.M.; Alves, B.; Veiga, G.; Fonseca, F.L.A.; Bacci, M.R. Uremic neuropathy: An overview of the current literature. Rev. Assoc. Med. Bras. 2019, 65, 469–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R.; Gautam, P.; Gaur, S.; Kumar, S.; Taneja, V. Evaluation of central neuropathy in patients of chronic renal failure with normal hearing. Indian J. Otol. 2012, 18, 76. [Google Scholar] [CrossRef]
- Shvili, Y.; Gafter, U.; Zohar, Y.; Talmi, Y.P.; Levi, J. Brainstem auditory evoked responses in rats with experimental chronic renal failure. Clin. Sci. 1989, 76, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.R.; Bonfioli, F.; Garrubba, V.; Ghisellini, M.; Lamoretti, M.P.; Nicolai, P.; Camerini, C.; Maiorca, R. Audiological findings in elderly patients with chronic renal failure. Acta Otolaryngol. Suppl. 1990, 476, 54–68. [Google Scholar] [CrossRef]
- Rossini, P.M.; Di Stefano, E.; Febbo, A.; Di Paolo, B.; Basciani, M. Brain-stem auditory evoked responses (BAERs) in patients with chronic renal failure. Electroencephalogr. Clin. Neurophysiol. 1984, 57, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Aspris, A.K.; Thodi, C.D.; Balatsouras, D.G.; Thodis, E.D.; Vargemezis, V.; Danielides, V. Auditory brainstem responses in patients under treatment of hemodialysis. Ren. Fail. 2008, 30, 383–390. [Google Scholar] [CrossRef]
- Lin, R.J.; Krall, R.; Westerberg, B.D.; Chadha, N.K.; Chau, J.K. Systematic review and meta-analysis of the risk factors for sudden sensorineural hearing loss in adults. Laryngoscope 2012, 122, 624–635. [Google Scholar] [CrossRef]
- Lee, H.; Sohn, S.I.; Jung, D.K.; Cho, Y.W.; Lim, J.G.; Yi, S.D.; Lee, S.R.; Sohn, C.H.; Baloh, R.W. Sudden deafness and anterior inferior cerebellar artery infarction. Stroke 2002, 33, 2807–2812. [Google Scholar] [CrossRef]
- Lin, H.C.; Chao, P.Z.; Lee, H.C. Sudden sensorineural hearing loss increases the risk of stroke: A 5-year follow-up study. Stroke 2008, 39, 2744–2748. [Google Scholar] [CrossRef] [Green Version]
- Kobiyama, K.; Ley, K. Atherosclerosis. Circ. Res. 2018, 123, 1118–1120. [Google Scholar] [CrossRef] [PubMed]
- Balakumar, P.; Maung, U.K.; Jagadeesh, G. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharm. Res. 2016, 113, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, S.M.; Di Berardino, F.; Bucciarelli, P.; Berto, V.; Artoni, A.; Gianniello, F.; Ambrosetti, U.; Cesarani, A.; Pappalardo, E.; Martinelli, I. Risk factors for idiopathic sudden sensorineural hearing loss and their association with clinical outcome. Thromb. Res. 2015, 135, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Fasano, T.; Pertinhez, T.A.; Tribi, L.; Lasagni, D.; Pilia, A.; Vecchia, L.; Baricchi, R.; Bianchin, G. Laboratory assessment of sudden sensorineural hearing loss: A case-control study. Laryngoscope 2017, 127, 2375–2381. [Google Scholar] [CrossRef]
- Fusconi, M.; Chistolini, A.; de Virgilio, A.; Greco, A.; Massaro, F.; Turchetta, R.; Benincasa, A.T.; Tombolini, M.; de Vincentiis, M. Sudden sensorineural hearing loss: A vascular cause? Analysis of prothrombotic risk factors in head and neck. Int. J. Audiol. 2012, 51, 800–805. [Google Scholar] [CrossRef]
- Choi, H.G.; Kang, H.S.; Lim, H.; Kim, J.H.; Kim, J.H.; Cho, S.J.; Nam, E.S.; Min, K.W.; Park, H.Y.; Kim, N.Y.; et al. Potential Cancer Risk in Patients with Rheumatoid Arthritis: A Longitudinal Korean Population-Based Analysis. J. Pers. Med. 2022, 12, 965. [Google Scholar] [CrossRef]
- Kim, S.Y.; Chung, J.; Park, D.S.; Yoo, D.M.; Bang, W.J.; Choi, H.G. The Reciprocal Relationship between Osteoporosis and Renal Stones. J. Clin. Med. 2022, 11, 6614. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Before Overlap Weighting Adjustment | After Overlap Weighting Adjustment | ||||
|---|---|---|---|---|---|---|
| CKD | Control | Standardized Difference | CKD | Control | Standardized Difference | |
| Age (n, %) | 0.00 | 0.00 | ||||
| 40–44 | 98 (0.59) | 392 (0.59) | 75 (0.60) | 75 (0.60) | ||
| 45–49 | 359 (2.15) | 1436 (2.15) | 260 (2.10) | 260 (2.10) | ||
| 50–54 | 943 (5.64) | 3772 (5.64) | 685 (5.53) | 685 (5.53) | ||
| 55–59 | 1846 (11.05) | 7384 (11.05) | 1353 (10.91) | 1353 (10.91) | ||
| 60–64 | 2272 (13.59) | 9088 (13.59) | 1659 (13.38) | 1659 (13.38) | ||
| 65–69 | 2565 (15.35) | 10,260 (15.35) | 1886 (15.21) | 1886 (15.21) | ||
| 70–74 | 2939 (17.59) | 11,756 (17.59) | 2190 (17.66) | 2190 (17.66) | ||
| 75–79 | 2861 (17.12) | 11,444 (17.12) | 2149 (17.32) | 2149 (17.33) | ||
| 80–84 | 1903 (11.39) | 7612 (11.39) | 1434 (11.57) | 1434 (11.57) | ||
| 85+ | 927 (5.55) | 3708 (5.55) | 711 (5.73) | 711 (5.73) | ||
| Sex (n, %) | 0.00 | |||||
| Male | 10,981 (65.70) | 43,924 (65.70) | 8158 (65.78) | 8158 (65.78) | ||
| Female | 5732 (34.30) | 22,928 (34.30) | 4244 (34.22) | 4244 (34.22) | ||
| Income (n, %) | 0.00 | 0.00 | ||||
| 1 (lowest) | 2928 (17.52) | 11,712 (17.52) | 2162 (17.43) | 2162 (17.43) | ||
| 2 | 1924 (11.51) | 7696 (11.51) | 1429 (11.52) | 1429 (11.52) | ||
| 3 | 2384 (14.26) | 9536 (14.26) | 1763 (14.22) | 1763 (14.22) | ||
| 4 | 3308 (19.79) | 13,232 (19.79) | 2445 (19.72) | 2445 (19.72) | ||
| 5 (highest) | 6169 (36.91) | 24,676 (36.91) | 4603 (37.11) | 4603 (37.11) | ||
| Region of residence (n, %) | 0.00 | 0.00 | ||||
| Urban | 7157 (42.82) | 28,628 (42.82) | 5310 (42.82) | 5310 (42.82) | ||
| Rural | 9556 (57.18) | 38,224 (57.18) | 7092 (57.18) | 7092 (57.18) | ||
| Obesity † (n, %) | 0.15 | 0.00 | ||||
| Underweight | 443 (2.65) | 2220 (3.32) | 347 (2.79) | 347 (2.79) | ||
| Normal | 5129 (30.69) | 23,822 (35.63) | 3926 (31.66) | 3926 (31.66) | ||
| Overweight | 4379 (26.20) | 18,037 (26.98) | 3280 (26.45) | 3280 (26.45) | ||
| Obese I | 6000 (35.90) | 20,871 (31.22) | 4345 (35.04) | 4345 (35.04) | ||
| Obese II | 762 (4.56) | 1902 (2.85) | 503 (4.06) | 503 (4.06) | ||
| Smoking status (n, %) | 0.02 | 0.00 | ||||
| Nonsmoker | 10,688 (63.95) | 43,275 (64.73) | 7960 (64.18) | 7960 (64.18) | ||
| Past smoker | 1748 (10.46) | 6965 (10.42) | 1304 (10.51) | 1304 (10.51) | ||
| Current smoker | 4277 (25.59) | 16,612 (24.85) | 3138 (25.31) | 3138 (25.31) | ||
| Alcohol consumption (n, %) | 0.07 | 0.00 | ||||
| <1 time a week | 12,152 (72.71) | 46,344 (69.32) | 8910 (71.85) | 8911 (71.85) | ||
| ≥1 time a week | 4561 (27.29) | 20,508 (30.68) | 3491 (28.15) | 3491 (28.15) | ||
| SBP (Mean, SD) | 131.85 (18.38) | 128.66 (16.25) | 0.18 | 130.87 (15.41) | 130.87 (7.29) | 0.00 |
| DBP (Mean, SD) | 78.74 (11.53) | 78.10 (10.33) | 0.06 | 78.52 (9.82) | 78.52 (4.55) | 0.00 |
| Fasting blood glucose (Mean, SD) | 115.61 (49.21) | 103.74 (29.28) | 0.29 | 110.20 (33.15) | 110.20 (18.33) | 0.00 |
| Total cholesterol (Mean, SD) | 190.26 (45.68) | 193.11 (38.84) | 0.07 | 190.61 (39.05) | 190.61 (16.87) | 0.00 |
| CCI score (Mean, SD) | 2.19 (2.20) | 1.13 (1.73) | 0.53 | 1.84 (1.68) | 1.84 (0.99) | 0.00 |
| SSNHL (n, %) | 153 (0.92) | 603 (0.90) | 0.00 | 110 (0.89) | 109 (0.88) | 0.00 |
| N of Event/ N of Total (%) | Follow-Up Duration (PY) | IR per 1000 (PY) | IRD (95% CI) | Hazard Ratios for SSNHL | ||||
|---|---|---|---|---|---|---|---|---|
| Crude | p-Value | Overlap Weighted Model † | p-Value | |||||
| Total participants | ||||||||
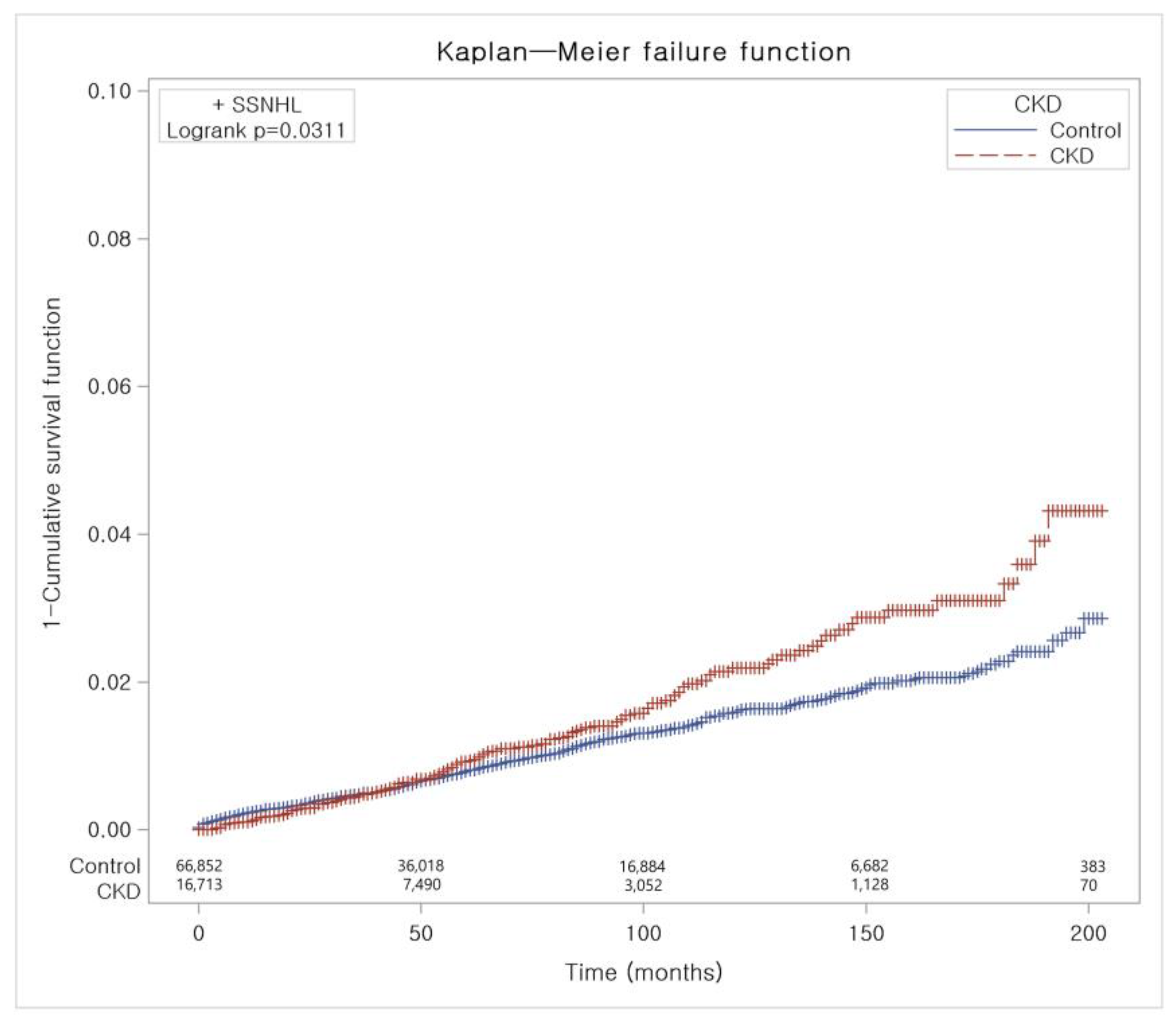
| CKD | 153/16,713 (0.92) | 70,780 | 2.16 | 0.42 (0.07 to 0.76) | 1.22 (1.02 to 1.45) | 0.031 * | 1.21 (1.04 to 1.39) | 0.011 * |
| Control | 603/66,852 (0.90) | 346,022 | 1.74 | 1 | 1 | |||
| Age < 70 years old | ||||||||
| CKD | 118/8,083 (1.46) | 45,337 | 2.60 | 0.67 (0.21 to 1.13) | 1.33 (1.09 to 1.63) | 0.006 * | 1.30 (1.10 to 1.54) | 0.002 * |
| Control | 414/32,332 (1.28) | 214,572 | 1.93 | 1 | 1 | |||
| Age ≥ 70 years old | ||||||||
| CKD | 35/8630 (0.41) | 25,443 | 1.38 | −0.06 (−0.57 to 0.45) | 0.90 (0.63 to 1.30) | 0.580 | 0.95 (0.72 to 1.25) | 0.724 |
| Control | 189/34,520 (0.55) | 131,450 | 1.44 | 1 | 1 | |||
| Male | ||||||||
| CKD | 98/10,981 (0.89) | 45,558 | 2.15 | 0.31 (−0.12 to 0.75) | 1.15 (0.92 to 1.44) | 0.212 | 1.18 (0.99 to 1.41) | 0.070 |
| Control | 408/43,924 (0.93) | 222,167 | 1.84 | 1 | 1 | |||
| Female | ||||||||
| CKD | 55/5732 (0.96) | 25,222 | 2.18 | 0.61 (0.05 to 1.16) | 1.35 (1.00 to 1.82) | 0.048 * | 1.26 (0.98 to 1.62) | 0.069 |
| Control | 195/22,928 (0.85) | 123,855 | 1.57 | 1 | 1 | |||
| Low-income group | ||||||||
| CKD | 60/7236 (0.83) | 30,267 | 1.98 | 0.25 (−0.26 to 0.78) | 1.12 (0.85 to 1.49) | 0.421 | 1.07 (0.85 to 1.34) | 0.579 |
| Control | 260/28,944 (0.90) | 150,599 | 1.73 | 1 | 1 | |||
| High-income group | ||||||||
| CKD | 93/9477 (0.98) | 40,513 | 2.30 | 0.54 (0.08 to 1.00) | 1.28 (1.02 to 1.61) | 0.033 * | 1.31 (1.09 to 1.58) | 0.005 * |
| Control | 343/37,908 (0.90) | 195,423 | 1.76 | 1 | 1 | |||
| Urban resident | ||||||||
| CKD | 83/7157 (1.16) | 32,171 | 2.58 | 0.77 (0.24 to 1.30) | 1.41 (1.10 to 1.80) | 0.006 * | 1.39 (1.13 to 1.70) | 0.002 * |
| Control | 279/28,628 (0.97) | 154,461 | 1.81 | 1 | 1 | |||
| Rural resident | ||||||||
| CKD | 70/9556 (0.73) | 38,609 | 1.81 | 0.12 (−0.33 to 0.57) | 1.05 (0.81 to 1.36) | 0.728 | 1.05 (0.85 to 1.29) | 0.647 |
| Control | 324/38,224 (0.85) | 191,561 | 1.69 | 1 | 1 | |||
| Underweight | ||||||||
| CKD | 2/443 (0.45) | 1359 | 1.47 | 0.11 (−2.00 to 2.22) | 1.06 (0.24 to 4.70) | 0.940 | 1.05 (0.34 to 3.19) | 0.937 |
| Control | 13/2220 (0.59) | 9526 | 1.36 | 1 | 1 | |||
| Normal weight | ||||||||
| CKD | 47/5129 (0.92) | 20,969 | 2.24 | 0.65 (0.05 to 1.26) | 1.38 (1.00 to 1.89) | 0.049 * | 1.29 (1.00 to 1.67) | 0.049 * |
| Control | 195/23,822 (0.82) | 122,872 | 1.59 | 1 | 1 | |||
| Overweight | ||||||||
| CKD | 52/4379 (1.19) | 19,568 | 2.66 | 0.74 (0.04 to 1.43) | 1.36 (1.00 to 1.85) | 0.052 | 1.30 (1.01 to 1.68) | 0.043 * |
| Control | 183/18,037 (1.01) | 95,092 | 1.92 | 1 | 1 | |||
| Obese | ||||||||
| CKD | 52/6762 (0.77) | 28,884 | 1.80 | 0.01 (−0.53 to 0.56) | 0.99 (0.73 to 1.34) | 0.948 | 1.05 (0.82 to 1.35) | 0.686 |
| Control | 212/22,773 (0.93) | 118,532 | 1.79 | 1 | 1 | |||
| Nonsmoker | ||||||||
| CKD | 112/10,688 (1.05) | 46,836 | 2.39 | 0.63 (0.20 to 1.06) | 1.33 (1.08 to 1.65) | 0.007 * | 1.29 (1.09 to 1.54) | 0.004 * |
| Control | 399/43,275 (0.92) | 226,976 | 1.76 | 1 | 1 | |||
| Past and current smoker | ||||||||
| CKD | 41/6025 (0.68) | 23,944 | 1.71 | 0.00 (−0.58 to 0.57) | 0.98 (0.70 to 1.37) | 0.888 | 1.00 (0.77 to 1.29) | 0.990 |
| Control | 204/23,577 (0.87) | 119,046 | 1.71 | 1 | 1 | |||
| Alcohol consumption < 1 time a week | ||||||||
| CKD | 116/12,152 (0.95) | 52,397 | 2.21 | 0.44 (0.04 to 0.85) | 1.22 (1.00 to 1.50) | 0.053 | 1.20 (1.01 to 1.42) | 0.037 * |
| Control | 428/46,344 (0.92) | 241,865 | 1.77 | 1 | 1 | |||
| Alcohol consumption ≥ 1 time a week | ||||||||
| CKD | 37/4561 (0.81) | 18,383 | 2.01 | 0.33 (−0.32 to 0.98) | 1.18 (0.83 to 1.68) | 0.360 | 1.21 (0.92 to 1.59) | 0.167 |
| Control | 175/20,508 (0.85) | 104,157 | 1.68 | 1 | 1 | |||
| SBP < 140 mmHg and DBP < 90 mmHg | ||||||||
| CKD | 102/10,953 (0.93) | 44,649 | 2.28 | 0.45 (0.01 to 0.89) | 1.22 (0.98 to 1.51) | 0.073 | 1.23 (1.04 to 1.46) | 0.015 * |
| Control | 451/48,853 (0.92) | 246,199 | 1.83 | 1 | 1 | |||
| SBP ≥ 140 mmHg or DBP ≥ 90 mmHg | ||||||||
| CKD | 51/5760 (0.89) | 26,131 | 1.95 | 0.43 (−0.12 to 0.98) | 1.27 (0.92 to 1.74) | 0.145 | 1.11 (0.84 to 1.47) | 0.460 |
| Control | 152/17,999 (0.84) | 99,823 | 1.52 | 1 | 1 | |||
| Fasting blood glucose < 100 mg/dL | ||||||||
| CKD | 69/7801 (0.88) | 35,843 | 1.93 | 0.19 (−0.29 to 0.65) | 1.08 (0.84 to 1.40) | 0.552 | 1.10 (0.91 to 1.34) | 0.313 |
| Control | 363/37,239 (0.97) | 208,139 | 1.74 | 1 | 1 | |||
| Fasting blood glucose ≥ 100 mg/dL | ||||||||
| CKD | 84/8912 (0.94) | 34,937 | 2.40 | 0.66 (0.16 to 1.17) | 1.36 (1.06 to 1.74) | 0.016 * | 1.31 (1.05 to 1.63) | 0.015 * |
| Control | 240/29,613 (0.81) | 137,883 | 1.74 | 1 | 1 | |||
| Total cholesterol < 200 mg/dL | ||||||||
| CKD | 86/10,354 (0.83) | 40,676 | 2.11 | 0.41 (−0.04 to 0.86) | 1.22 (0.96 to 1.55) | 0.100 | 1.22 (1.01 to 1.49) | 0.040 * |
| Control | 330/39,341 (0.84) | 193,809 | 1.70 | 1 | 1 | |||
| Total cholesterol ≥ 200 mg/dL | ||||||||
| CKD | 67/6359 (1.05) | 30,104 | 2.23 | 0.44 (−0.10 to 0.97) | 1.22 (0.93 to 1.59) | 0.151 | 1.20 (0.96 to 1.49) | 0.104 |
| Control | 273/27,511 (0.99) | 152,213 | 1.79 | 1 | 1 | |||
| CCI scores = 0 | ||||||||
| CKD | 52/4877 (1.07) | 22,865 | 2.27 | 0.45 (−0.14 to 1.05) | 1.23 (0.92 to 1.64) | 0.165 | 1.23 (1.01 to 1.49) | 0.039 * |
| Control | 348/35,944 (0.97) | 191,409 | 1.82 | 1 | 1 | |||
| CCI scores = 1 | ||||||||
| CKD | 23/2844 (0.81) | 11,499 | 2.00 | 0.12 (−0.75 to 0.98) | 1.04 (0.66 to 1.62) | 0.872 | 0.98 (0.70 to 1.37) | 0.918 |
| Control | 120/12,306 (0.98) | 63,790 | 1.88 | 1 | 1 | |||
| CCI scores ≥ 2 | ||||||||
| CKD | 78/8992 (0.87) | 36,416 | 2.14 | 0.65 (0.16 to 1.15) | 1.42 (1.08 to 1.88) | 0.013 * | 1.24 (0.94 to 1.64) | 0.129 |
| Control | 135/18,602 (0.73) | 90,823 | 1.49 | 1 | 1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, Y.J.; Choi, H.G.; Wee, J.H. Association between Chronic Kidney Disease and Sudden Sensorineural Hearing Loss: A Longitudinal Follow-Up Studies Using ICD-10 Codes in a National Health Screening Cohort. J. Clin. Med. 2023, 12, 2861. https://doi.org/10.3390/jcm12082861
Shim YJ, Choi HG, Wee JH. Association between Chronic Kidney Disease and Sudden Sensorineural Hearing Loss: A Longitudinal Follow-Up Studies Using ICD-10 Codes in a National Health Screening Cohort. Journal of Clinical Medicine. 2023; 12(8):2861. https://doi.org/10.3390/jcm12082861
Chicago/Turabian StyleShim, Ye Ji, Hyo Geun Choi, and Jee Hye Wee. 2023. "Association between Chronic Kidney Disease and Sudden Sensorineural Hearing Loss: A Longitudinal Follow-Up Studies Using ICD-10 Codes in a National Health Screening Cohort" Journal of Clinical Medicine 12, no. 8: 2861. https://doi.org/10.3390/jcm12082861