
Endometriosis and the Temporomandibular Joint—Preliminary Observations

Abstract
:1. Introduction
2. Study Aim
- Is there a correlation between the presence of pain on the right and left sides of the pelvis and pain on the right and left sides of the mandible (temporomandibular joint)?
- Is there a correlation between the presence of pain in the pelvis (right, left, middle, and back) and headaches on the right and left sides (temples), middle (forehead), and back (occipital)?
- Is teeth clenching related to headaches?
- Is teeth clenching related to pain in the temporomandibular joint?
- Is there a correlation between the occurrence of pain in the temporomandibular joint (TMJ) and the treatment of endometriosis?
- Is there a correlation between the occurrence of pain in the pelvis and the treatment of endometriosis?
- Is there a correlation between the occurrence of pain outside the pelvis (in other parts of the body) and the treatment of endometriosis?
3. Materials and Methods
4. Results
- There was a correlation between the presence of pain on the right and left sides of the pelvis and pain on the right and left sides of the temporomandibular joint, p-value = 0.0397, V = 0.2350 (Table 1).
- There was no relationship between the presence of pelvic pain on the right, left, middle, and back and headaches on the right and left sides (temples), middle (forehead), and back (occipital), p-value = 0.0647, V = 0.3469 (Table 1).
- There was no relationship between teeth clenching and headache, p-value = 0.4715, V = 0.2886 (Table 1).
- There was a highly significant relationship between teeth clenching and temporomandibular joint pain, p-value = 0.0005, V = 0.3695 (Table 1).
- There was no relationship between the occurrence of temporomandibular joint pain and the treatment of endometriosis, p-value = 0.5214, V = 0.3274 (Table 1).
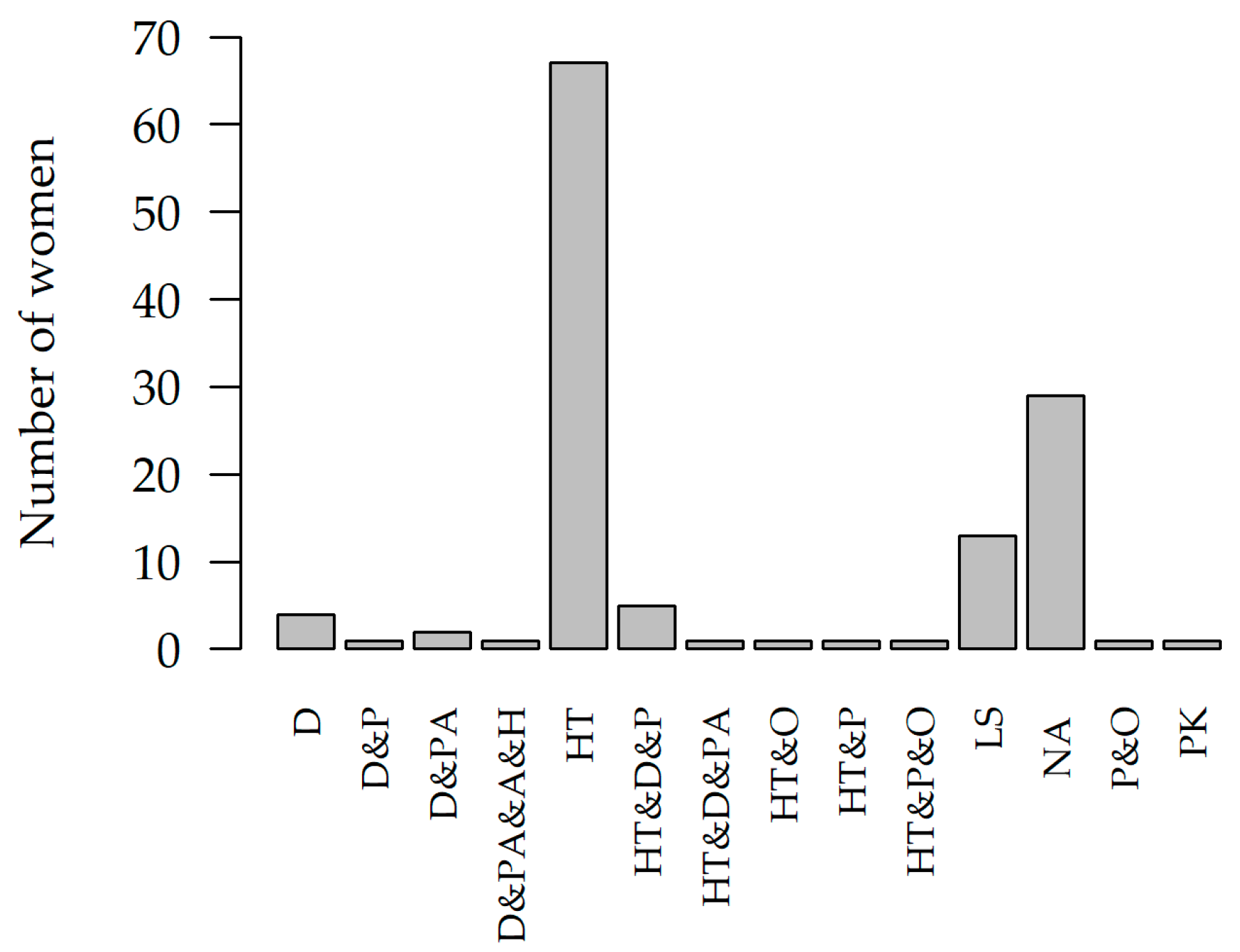
- There was a relationship between the presence of pain outside the pelvis (in other parts of the body) and the treatment modality for endometriosis, p-value = 0.0311, V = 0.4549 (Table 1, Figure 1). All subjects reported that they clench their teeth; we did not assess anxiety/stress levels in this study.
5. Discussion
6. Conclusions
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hudson, N. The missed disease? Endometriosis as an example of undone science. Reprod. Biomed. Soc. Online 2021, 14, 20–27. [Google Scholar] [CrossRef]
- Arafah, M.; Rashid, W.; Akhtar, M. Endometriosis: A Comprehensive Review. Adv. Anat. Pathol. 2021, 28, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.S.; Kotlyar, A.M.; Flores, V.A. Endometriosis is a chronic systemic disease: Clinical challenges and novel innovations. Lancet 2021, 397, 839–852. [Google Scholar] [CrossRef]
- Wójcik, M.; Szczepaniak, R.; Placek, K. Physiotherapy Management in Endometriosis. Int. J. Environ. Res. Public Health 2022, 19, 16148. [Google Scholar] [CrossRef]
- Guerriero, S.; Saba, L.; Pascual, M.A.; Ajossa, S.; Rodriguez, I.; Mais, V.; Alcazar, J.L. Transvaginal ultrasound vs magnetic resonance imaging for diagnosing deep infiltrating endometriosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2018, 51, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Bhyan, S.B.; Zhao, L.; Wee, Y.K.; Liu, Y.; Zhao, M. Genetic links between endometriosis and cancers in women. PeerJ 2019, 7, e8135. [Google Scholar] [CrossRef]
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Viganò, P. Endometriosis. Nat. Rev. Dis. Prim. 2018, 4, 9. [Google Scholar] [CrossRef]
- DiVasta, A.D.; Vitonis, A.F.; Laufer, M.R.; Missmer, S.A. Spectrum of symptoms in women diagnosed with endometriosis during adolescence vs adulthood. Am. J. Obstet. Gynecol. 2018, 218, 324.e1–324.e11. [Google Scholar] [CrossRef] [PubMed]
- Stefansson, H.; Geirsson, R.T.; Steinthorsdottir, V.; Jonsson, H.; Manolescu, A.; Kong, A.; Ingadottir, G.; Gulcher, J.; Stefansson, K. Genetic Factors Contribute to the Risk of Developing Endometriosis. Hum. Reprod. 2002, 17, 555–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannuccini, S.; Lazzeri, L.; Orlandini, C.; Tosti, C.; Clifton, V.L.; Petraglia, F. Potential Influence of in Utero and Early Neonatal Exposures on the Later Development of Endometriosis. Fertil. Steril. 2016, 105, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Borghese, B.; Sibiude, J.; Santulli, P.; Pillet, M.C.L.; Marcellin, L.; Brosens, I.; Chapron, C. Low Birth Weight Is Strongly Associated with the Risk of Deep Infiltrating Endometriosis: Results of a 743 Case-Control Study. PLoS ONE 2015, 10, e0117387. [Google Scholar] [CrossRef] [Green Version]
- Vitonis, A.F.; Vincent, K.; Rahmioglu, N.; Fassbender, A.; Buck Louis, G.M.; Hummelshoj, L.; Giudice, L.C.; Stratton, P.; Adamson, G.D.; Becker, C.M.; et al. World Endometriosis Research Foundation Endometriosis Phenome and Biobanking Harmonization Project: II. Clinical and Covariate Phenotype Data Collection in Endometriosis Research. Fertil. Steril. 2014, 102, 1223. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.A.; Missmer, S.A.; Vitonis, A.F.; Sarda, V.; Laufer, M.R.; DiVasta, A.D. Prevalence of Migraines in Adolescents with Endometriosis. Fertil. Steril. 2018, 109, 685–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viganò, P.; Somigliana, E.; Panina, P.; Rabellotti, E.; Vercellini, P.; Candiani, M. Principles of Phenomics in Endometriosis. Hum. Reprod. Update 2012, 18, 248–259. [Google Scholar] [CrossRef]
- Vannuccini, S.; Clifton, V.L.; Fraser, I.S.; Taylor, H.S.; Critchley, H.; Giudice, L.C.; Petraglia, F. Infertility and Reproductive Disorders: Impact of Hormonal and Inflammatory Mechanisms on Pregnancy Outcome. Hum. Reprod. Update 2016, 22, 104–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zullo, F.; Spagnolo, E.; Saccone, G.; Acunzo, M.; Xodo, S.; Ceccaroni, M.; Berghella, V. Endometriosis and Obstetrics Complications: A Systematic Review and Meta-Analysis. Fertil. Steril. 2017, 108, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Shigesi, N.; Kvaskoff, M.; Kirtley, S.; Feng, Q.; Fang, H.; Knight, J.C.; Missmer, S.A.; Rahmioglu, N.; Zondervan, K.T.; Becker, C.M. The Association between Endometriosis and Autoimmune Diseases: A Systematic Review and Meta-Analysis. Hum. Reprod. Update 2019, 25, 486–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brotskyi, N.; Tatarchuk, T.; Plaksiieva, K.; Fetsych, A.; Ostrianko, V. Temporal Bone Endometriosis—A Multidisciplinary Approach. A Clinical Case. J. Int. Dent. Med. Res. 2022, 15, 1305–1310. [Google Scholar]
- Bonato, L.L.; Quinelato, V.; De Felipe Cordeiro, P.C.; De Sousa, E.B.; Tesch, R.; Casado, P.L. Association between temporomandibular disorders and pain in other regions of the body. J. Oral Rehabil. 2017, 44, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Rocha, P.; Croci, C.S.; Caria, P.H.F. Is there relationship between temporomandibular disorders and head and cervical posture? A systematic review. J. Oral Rehabil. 2013, 40, 875–881. [Google Scholar] [CrossRef]
- Kusdra, P.M.; Stechman-Neto, J.; Leão, B.L.C.; Martins, P.F.A.; Lacerda, A.B.M.; Zeigelboim, B.S. Relationship between otological symptoms and TMD. Int. Tinnitus J. 2018, 22, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Garstka, A.A.; Brzózka, M.; Bitenc-Jasiejko, A.; Ardan, R.; Gronwald, H.; Skomro, P.; Lietz-Kijak, D. Cause-Effect Relationships between Painful TMD and Postural and Functional Changes in the Musculoskeletal System: A Preliminary Report. Pain Res. Manag. 2022, 2022, 1429932. [Google Scholar] [CrossRef]
- Robinson, J.L.; Soria, P.; Xu, M.; Vrana, M.; Luchetti, J.; Lu, H.H.; Chen, J.; Wadhwa, S. Estrogen Promotes Mandibular Condylar Fibrocartilage Chondrogenesis and Inhibits Degeneration via Estrogen Receptor Alpha in Female Mice. Sci. Rep. 2018, 8, 8527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, L.E.; Doetzer, A.; Beck, M.L. Immunohistochemical Markers of Temporomandibular Disorders: A Review of the Literature. J. Clin. Med. 2023, 12, 789. [Google Scholar] [CrossRef] [PubMed]
- Camejo Fde, A.; Almeida, L.E.; Doetzer, A.D.; Caporal, K.S.; Ambros, V.; Azevedo, M.; Alanis, L.R.; Olandoski, M.; Noronha, L.; Trevilatto, P.C. FasL expression in articular discs of human temporomandibular joint and association with osteoarthrosis. J. Oral Pathol. Med. 2014, 43, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Brichant, G.; Laraki, I.; Henry, L.; Munaut, C.; Nisolle, M. New Therapeutics in Endometriosis: A Review of Hormonal, Non-Hormonal, and Non-Coding RNA Treatments. Int. J. Mol. Sci. 2021, 22, 10498. [Google Scholar] [CrossRef]
- Capezzuoli, T.; Rossi, M.; La Torre, F.; Vannuccini, S.; Petraglia, F. Hormonal drugs for the treatment of endometriosis. Curr. Opin. Pharmacol. 2022, 67, 102311. [Google Scholar] [CrossRef] [PubMed]
- do Vale Braido, G.V.; Svensson, P.; dos Santos Proença, J.; Gruninger Mercante, F.; Fernandes, G.; de Godoi Gonçalves, D.A. Are central sensitization symptoms and psychosocial alterations interfering in the association between painful TMD, migraine, and headache attributed to TMD? Clin. Oral Investig. 2022, 27, 681–690. [Google Scholar] [CrossRef]
- Jenabi, E.; Khazaei, S. Endometriosis and migraine headache risk: A meta-analysis. Women Health 2020, 60, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Goldfinger, C.; Pukall, C.F.; Thibault-Gagnon, S.; McLean, L.; Chamberlain, S. Effectiveness of cognitive-behavioral therapy and physical therapy for provoked vestibulodynia: A randomized pilot study. J. Sex Med. 2016, 13, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Parada, H.A.; Calderon-Ospina, C.-A.; Chen, J.; Emril, D.R.; Fernandez-Villacorta, F.J.; Franco, H.; Ho, K.-Y.; Lara-Solares, A.; Li, C.C.-F.; et al. Current understanding of the mixed pain concept: A brief narrative review. Curr. Med Res. Opin. 2019, 35, 1011–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunselman, G.A.J.; Vermeulen, N.; Becker, C.; Calhaz-Jorge, C.; D’Hooghe, T.; De Bie, B.; Heikinheimo, O.; Horne, A.W.; Kiesel, L.; Nap, A.; et al. ESHRE guideline: Management of women with endometriosis. Hum. Reprod. 2014, 29, 400–412. [Google Scholar] [CrossRef]
- Schleedoorn, M.J.; Nelen, W.L.D.M.; Dunselman, G.A.J.; Vermeulen, N.; EndoKey Group. Selection of key recommendations for the management of women with endometriosis by an international panel of patients and professionals. Hum. Reprod. 2016, 31, 1208–1218. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE guideline: Endometriosis. Hum. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.eshre.eu/2022 (accessed on 27 March 2023).
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2022. Available online: https://www.r-project.org/ (accessed on 10 February 2023).
- Cramer, H. Mathematical Methods of Statistics; Princeton University Press: Princeton, NJ, USA, 1946. [Google Scholar]
- Boujenah, J.; Cedrin-Durnerin, I.; Herbemont, C.; Bricou, A.; Sifer, C.; Poncelet, C. Use of the endometriosis fertility index in daily practice: A prospective evaluation. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 219, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Haas, D.; Oppelt, P.; Shebl, O.; Shamiyeh, A.; Schimetta, W.; Mayer, R. Enzian classification: Does it correlate with clinical symptoms and the rASRM score? Acta Obstet. Gynecol. Scand. 2013, 92, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, N.; Abrao, M.S.; Einarsson, J.I.; Horne, A.W.; Johnson, N.P.; Lee, T.T.M.; Missmer, S.; Petrozza, J.; Tomassetti, C.; Zondervan, K.T.; et al. Endometriosis classification, staging and reporting systems: A review on the road to a universally accepted endometriosis classification. Facts Views Vis. Obgyn. 2021, 13, 305–330. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Hummelshoj, L.; Adamson, G.D.; Keckstein, J.; Taylor, H.S.; Abrao, M.S.; Bush, D.; Kiesel, L.; Tamimi, R.; Sharpe-Timms, K.L.; et al. World Endometriosis Society consensus on the classification of endometriosis. Hum. Reprod. 2017, 32, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Brawn, J.; Morotti, M.; Zondervan, K.T.; Becker, C.M.; Vincent, K. Central changes associated with chronic pelvic pain and endometriosis. Hum. Reprod. Update 2014, 20, 737–747. [Google Scholar] [CrossRef] [Green Version]
- Häuser, W. Endometriosis and chronic overlapping pain conditions. Schmerz 2021, 35, 179–182. [Google Scholar] [CrossRef]
- Szymańska, J.; Dąbrowska-Galas, M. An assessment of Polish women’s level of knowledge about endometriosis: A pilot study. BMC Women’s Health 2021, 21, 404. [Google Scholar] [CrossRef]
- Buggio, L.; Dridi, D.; Barbara, G.; Merli, C.E.M.; Cetera, G.E.; Vercellini, P. Novel pharmacological therapies for the treatment of endometriosis. Expert Rev. Clin. Pharmacol. 2022, 15, 1039–1052. [Google Scholar] [CrossRef] [PubMed]
- Gruber, T.M.; Mechsner, S. Pathogenesis of Endometriosis: The Origin of Pain and Subfertility. Cells 2021, 10, 1381. [Google Scholar] [CrossRef]
- Sims, O.T.; Gupta, J.; Missmer, S.A.; Aninye, I.O. Stigma and Endometriosis: A Brief Overview and Recommendations to Improve Psychosocial Well-Being and Diagnostic Delay. Int. J. Environ. Res. Public Health 2021, 18, 8210. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Singh, V.; Tayade, C. Fertil Steril Biomarkers in endometriosis: Challenges and opportunities. Fertil. Steril. 2017, 107, 523–532. [Google Scholar] [CrossRef] [Green Version]
- Coutinho, L.M.; Ferreira, M.C.; Rocha, A.L.L.; Carneiro, M.M.; Reis, F.M. New biomarkers in endometriosis. Adv. Clin. Chem. 2019, 89, 59–77. [Google Scholar]
- Saunders, P.T.K.; Horne, A.W. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell 2021, 184, 2807–2824. [Google Scholar] [CrossRef] [PubMed]
- Kho, R.M.; Andres, M.P.; Borrelli, G.M.; Neto, J.S.; Zanluchi, A.; Abrão, M.S. Surgical treatment of different types of endometriosis: Comparison of major society guidelines and preferred clinical algorithms. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 51, 102–110. [Google Scholar] [CrossRef]
- Bourdel, N.; Chauvet, P.; Billone, V.; Douridas, G.; Fauconnier, A.; Gerbaud, L.; Canis, M. Systematic review of quality of life measures in patients with endometriosis. PLoS ONE 2019, 14, e0208464. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, H.; Chen, S.; Lin, Y.; Xie, X.; Zhong, G.; Zhang, Q. Migraine Is More Prevalent in Advanced-Stage Endometriosis, Especially When Co-Occuring with Adenomoysis. Front. Endocrinol. 2022, 12, 814474. [Google Scholar] [CrossRef] [PubMed]
- Pavlović, J.M. Headache in Women. Contin. (Minneap. Minn.) 2021, 27, 686–702. [Google Scholar] [CrossRef]
- Dydyk, A.M.; Gupta, N. Chronic Pelvic Pain; StatPearls Publishing: Treasure, Island, 2022. [Google Scholar]
- Engeler, D.S.; Baranowski, A.P.; Dinis-Oliveira, P.; Elneil, S.; Hughes, J.; Messelink, E.J.; van Ophoven, A.; Williams, A.C.; European Association of Urology. The 2013 EAU guidelines on chronic pelvic pain: Is management of chronic pelvic pain a habit, a philosophy, or a science? 10 years of development. Eur. Urol. 2013, 64, 431–439. [Google Scholar] [CrossRef]
- Smolarz, B.; Szyłło, K.; Romanowicz, H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). Int. J. Mol. Sci. 2021, 22, 10554. [Google Scholar] [CrossRef]
- Weller, J.L.; Comeau, D.; Otis, J.A.D. Myofascial Pain. Semin. Neurol. 2018, 38, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Kawamura, A. Disc displacement and changes in condylar position. Dentomaxillofac. Radiol. 2013, 42, 84227642. [Google Scholar] [CrossRef]
- Blanco Aguilera, A.; Gonzalez Lopez, L.; Blanco Aguilera, E.; De la Hoz Aizpurua, J.L.; Rodriguez Torronteras, A.; Segura Saint-Gerons, R.; Blanco Hungría, A. Relationship between self-reported sleep bruxism and pain in patients with temporomandibular disorders. J. Oral Rehabil. 2014, 415, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Firmani, M.; Reyes, M.; Becerra, N.; Flores, G.; Weitzman, M.; Espinosa, P. Bruxismo de sueño en niños y adolescentes. Rev. Chil. Pediatr. 2015, 86, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castrillon, E.E.; Exposto, F.G. Sleep Bruxism and Pain. Dent. Clin. N. Am. 2018, 62, 657–663. [Google Scholar] [CrossRef]
- Demjah, G.; Kapusevska, B.; Pejkovska-Shahpaska, B. Bruxism Unconscious Oral Habit in Everyday Life. Open Access Maced. J. Med. Sci. 2019, 7, 876–881. [Google Scholar] [CrossRef] [Green Version]
- Matheus, R.A.; de Moraes Ramos-Perez, F.M.; Menezes, A.V.; Bovi Ambrosano, G.M.; Haiter-Neto, F.; Bóscolo, F.N.; de Almeida, S.M. The relationship between temporomandibular dysfunction and head and cervical posturę. J. Appl. Oral Sci. 2009, 17, 204–208. [Google Scholar] [CrossRef] [Green Version]
- Clower, L.; Fleshman, T.; Geldenhuys, W.J.; Santanam, N. Targeting Oxidative Stress Involved in Endometriosis and Its Pain. Biomolecules 2022, 12, 1055. [Google Scholar] [CrossRef]
- Amini, L.; Chekini, R.; Nateghi, M.R.; Haghani, H.; Jamialahmadi, T.; Sathyapalan, T.; Sahebkar, A. The Effect of Combined Vitamin C and Vitamin E Supplementation on Oxidative Stress Markers in Women with Endometriosis: A Randomized, Triple-Blind Placebo-Controlled Clinical Trial. Pain Res. Manag. 2021, 2021, 5529741. [Google Scholar] [CrossRef]
- Gardella, B.; Dominoni, M.; Gritti, A.; Arrigo, A.; Antonucci, S.; Carletti, G.V.; Musacchi, V.; Pietrocola, G. Endometriosis pain and epithelial neutrophil activating peptide-78 levels. Sci. Rep. 2022, 12, 3227. [Google Scholar] [CrossRef]
- Kitaya, K.; Yasuo, T. Commonalities and Disparities between Endometriosis and Chronic Endometritis: Therapeutic Potential of Novel Antibiotic Treatment Strategy against Ectopic Endometrium. Int. J. Mol. Sci. 2023, 24, 2059. [Google Scholar] [CrossRef] [PubMed]
- McNamara, H.C.; Frawley, H.C.; Donoghue, J.F.; Readman, E.; Healey, M.; Ellett, L.; Reddington, C.; Hicks, L.J.; Harlow, K.; Rogers, P.A.W.; et al. Peripheral, Central, and Cross Sensitization in Endometriosis-Associated Pain and Comorbid Pain Syndromes. Front. Reprod. Health 2021, 3, 729642. [Google Scholar] [CrossRef]
- Cho, S.; Mutlu, L.; Zhou, Y.; Taylor, H.S. Aromatase inhibitor regulates let-7 expression and let-7f-induced cell migration in endometrial cells from women with endometriosis. Fertil. Steril. 2016, 106, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Saare, M.; Rekker, K.; Laisk-Podar, T.; Rahmioglu, N.; Zondervan, K.; Salumets, A.; Götte, M.; Peters, M. Challenges in endometriosis miRNA studies—From tissue heterogeneity to disease specific miRNAs. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 2282–2292. [Google Scholar] [CrossRef] [PubMed]
- Samani, E.N.; Mamillapalli, R.; Li, F.; Mutlu, L.; Hufnagel, D.; Krikun, G.; Taylor, H.S. Micrometastasis of endometriosis to distant organs in a murine model. Oncotarget 2017, 10, 2282–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardiner, J. Cytoskeletal Tensegrity in Microgravity. Life 2021, 11, 1091. [Google Scholar] [CrossRef]
- Meng, F.; Terentjevm, E.M. Theory of Semiflexible Filaments and Networks. Polymers 2017, 9, 52. [Google Scholar] [CrossRef]
- Leicht, B.T.; Kennedy, C.; Richardson, C. Inflammatory Biochemical Mediators and Their Role in Myofascial Pain and Osteopathic Manipulative Treatment: A Literature Review. Cureus 2022, 14, e22252. [Google Scholar] [CrossRef] [PubMed]
- Bonder, J.H.; Chi, M.; Rispoli, L. Myofascial Pelvic Pain and Related Disorders. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 501–515. [Google Scholar] [CrossRef]
- Galasso, A.; Urits, I.; An, D.; Nguyen, D.; Borchart, M.; Yazdi, C.; Manchikanti, L.; Kaye, R.J.; Kaye, A.D.; Mancuso, K.F.; et al. A Comprehensive Review of the Treatment and Management of Myofascial Pain Syndrome. Curr. Pain Headache Rep. 2020, 24, 43. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D. Central and peripheral pain generators in women with chronic pelvic pain: Patient centered assessment and treatment. Curr. Rheumatol. Rev. 2015, 11, 146–166. [Google Scholar] [CrossRef]
- Marquardt, R.M.; Kim, T.H.; Shin, J.H.; Jeong, J.W. Progesterone and Estrogen Signaling in the Endometrium: What Goes Wrong in Endometriosis? Int. J. Mol. Sci. 2019, 20, 3822. [Google Scholar] [CrossRef] [Green Version]
- Mardon, A.K.; Leake, H.B.; Szeto, I.K.; Astill, T.; Hilton, S.; Moseley, G.L.; Chalmers, K.J. Treatment recommendations for the management of persistent pelvic pain: A systematic review of international clinical practice guidelines. BJOG: Int. J. Obstet. Gynaecol. 2022, 129, 1248–1260. [Google Scholar] [CrossRef]
- Anthonissen, M.; Daly, D.; Janssens, T.; Van den Kerckhove, E. The effects of conservative treatments on burn scars: A systematic review. Burns 2016, 42, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Jeon, J.H.; Hong, A.; Yang, H.T.; Yim, H.; Cho, Y.S.; Kim, D.H.; Hur, J.; Kim, J.H.; Chun, W.; et al. The effect of burn rehabilitation massage therapy on hypertrophic scar after burn: A randomized controlled trial. Burns 2014, 40, 1513–1520. [Google Scholar] [CrossRef]
- Boden, I.; Sullivan, K.; Hackett, C.; Winzer, B.; Lane, R.; McKinnon, M.; Robertson, I. ICEAGE (Incidence of Complications following Emergency Abdominal surgery: Get Exercising): Study protocol of a pragmatic, multicentre, randomised controlled trial testing physiotherapy for the prevention of complications and improved physical recovery after emergency abdominal surgery. World J. Emerg. Surg. 2018, 13, 29. [Google Scholar] [CrossRef]
- Morotti, M.; Vincent, K.; Becker, C.M. Mechanisms of pain in endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 209, 8–13. [Google Scholar] [CrossRef]
- Rolla, E. Endometriosis: Advances and controversies in classification, pathogenesis, diagnosis, and treatment. F1000Research 2019, 8, F1000. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, M.; Gibbons, T.; Armour, M.; Wang, R.; Glanville, E.; Hodgson, R.; Cave, A.E.; Ong, J.; Tong, Y.Y.F.; Jacobson, T.Z.; et al. When to Do Surgery and When Not to Do Surgery for Endometriosis: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2020, 27, 390–407. [Google Scholar] [CrossRef]
- Sverrisdóttir, U.Á.; Hansen, S.; Rudnicki, M. Impact of diet on pain perception in women with endometriosis: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 271, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhao, W.; Li, T.; Zhao, Y.; Bu, H.; Song, S. Effects of acupuncture for the treatment of endometriosis-related pain: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186616. [Google Scholar] [CrossRef]
- Meresman, G.F.; Götte, M.; Laschke, M.W. Plants as source of new therapies for endometriosis: A review of preclinical and clinical studies. Hum. Reprod. Update 2021, 27, 367–392. [Google Scholar] [CrossRef]
- Mira, T.A.A.; Yela, D.A.; Podgaec, S.; Baracat, E.C.; Benetti-Pinto, C.L. Hormonal treatment isolated versus hormonal treatment associated with electrotherapy for pelvic pain control in deep endometriosis: Randomized clinical trial. Eur. J. Obstet. Gyneacol. Reprod. Biol. 2020, 255, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Del Mar Salinas-Asensio, M.; Ocón-Hernández, O.; Mundo-López, A.; Fernández-Lao, C.; Peinado, F.M.; Padilla-Vinuesa, C.; Álvarez-Salvago, F.; Postigo-Martín, P.; Lozano-Lozano, M.; Lara-Ramos, A.; et al. ‘Physio-EndEA’ Study: A Randomized, Parallel-Group Controlled Trial to Evaluate the Effect of a Supervised and Adapted Therapeutic Exercise Program to Improve Quality of Life in Symptomatic Women Diagnosed with Endometriosis. Int. J. Environ. Res. Public Health 2022, 19, 1738. [Google Scholar] [CrossRef]
- Brown, J.; Crawford, T.J.; Allen, C.; Hopewell, S.; Prentice, A. Nonsteroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst. Rev. 2017, 23, CD004753. [Google Scholar] [CrossRef] [PubMed]
- Anastasiu, C.V.; Moga, M.A.; Neculau, A.E.; Bălan, A.; Scârneciu, I.; Dragomir, R.M.; Dull, A.M.; Chicea, L.M. Biomarkers for the Noninvasive Diagnosis of Endometriosis: State of the Art and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 1750. [Google Scholar] [CrossRef] [Green Version]
- Maulitz, L.; Stickeler, E.; Stickel, S.; Habel, U.; Tchaikovski, S.N.; Chechko, N. Endometriosis, psychiatric comorbidities and neuroimaging: Estimating the odds of an endometriosis brain. Front. Neuroendocrinol. 2022, 65, 100988. [Google Scholar] [CrossRef]
- Evans, S.; Fernandez, S.; Olive, L.; Payne, L.A.; Mikocka-Walus, A. Psychological and mind-body interventions for endometriosis: A systematic review. J. Psychosom. Res. 2019, 124, 109756. [Google Scholar] [CrossRef] [PubMed]
- Tennfjord, M.K.; Gabrielsen, R.; Tellum, T. Effect of physical activity and exercise on endometriosis-associated symptoms: A systematic review. BMC Womens Health 2021, 21, 355. [Google Scholar] [CrossRef]
- Sillem, M.; Juhasz-Böss, I.; Klausmeier, I.; Mechsner, S.; Siedentopf, F.; Solomayer, E. Osteopathy for Endometriosis and Chronic Pelvic Pain—A Pilot Study. Geburtshilfe Frauenheilkd 2016, 76, 960–963. [Google Scholar] [CrossRef] [Green Version]
- Ouanounou, A.; Goldberg, M.; Haas, D.A. Pharmacotherapy in Temporomandibular Disorders: A Review. J. Can. Dent. Assoc. 2017, 83, h7. [Google Scholar] [PubMed]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 7, 29. [Google Scholar] [CrossRef] [Green Version]
- Kubala, E.; Lietz-Kijak, D.; Strzelecka, P.; Wieczorek, A.; Skomro, P.; Gronwald, H. Multidisciplinary and Nonpharmacological Management of Pain in Temporomandibular Disorders (TMDs). Pain Res. Manag. 2022, 2022, 3604386. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.A.; Pasinato, F.; Correa, E.; da Silva, A.M. Global body posture and plantar pressure distribution in individuals with and without temporomandibular disorder: A preliminary study. J. Manip. Physiol. Ther. 2014, 37, 407–414. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho França, P.R.; Pereira Lontra, A.C.; Dias Fernandes, P. Endometriosis: A Disease with Few Direct Treatment Options. Molecules 2022, 27, 4034. [Google Scholar] [CrossRef] [PubMed]
- Volker, C.; Mills, J. Endometriosis and body image: Comparing people with and without endometriosis and exploring the relationship with pelvic pain. Body Image 2022, 43, 518–522. [Google Scholar] [CrossRef]
- Kabani, Z.; Ramos-Nino, M.E.; Ramdass, P.V.A.K. Endometriosis and COVID-19: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 12951. [Google Scholar] [CrossRef]
- Khoja, O.; Silva Passadouro, B.; Mulvey, M.; Delis, I.; Astill, S.; Tan, A.L.; Sivan, M.J. Clinical Characteristics and Mechanisms of Musculoskeletal Pain in Long COVID. Pain Res. 2022, 15, 1729–1748. [Google Scholar] [CrossRef] [PubMed]
- Emodi-Perlman, A.; Eli, I. One year into the COVID-19 pandemic—Temporomandibular disorders and bruxism: What we have learned and what we can do to improve our manner of treatment. Dent. Med. Probl. 2021, 58, 215–218. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of Research Question | p = Value | Cramer V |
|---|---|---|
| 1. | 0.0397 | 0.2350 |
| 2. | 0.0647 | 0.3469 |
| 3. | 0.4715 | 0.2886 |
| 4. | 0.0005 | 0.3695 |
| 5. | 0.5214 | 0.3274 |
| 6. | 0.0104 | 0.3709 |
| 7. | 0.0311 | 0.4549 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wójcik, M.; Goździewicz, T.; Hudáková, Z.; Siatkowski, I. Endometriosis and the Temporomandibular Joint—Preliminary Observations. J. Clin. Med. 2023, 12, 2862. https://doi.org/10.3390/jcm12082862
Wójcik M, Goździewicz T, Hudáková Z, Siatkowski I. Endometriosis and the Temporomandibular Joint—Preliminary Observations. Journal of Clinical Medicine. 2023; 12(8):2862. https://doi.org/10.3390/jcm12082862
Chicago/Turabian StyleWójcik, Małgorzata, Tomasz Goździewicz, Zuzana Hudáková, and Idzi Siatkowski. 2023. "Endometriosis and the Temporomandibular Joint—Preliminary Observations" Journal of Clinical Medicine 12, no. 8: 2862. https://doi.org/10.3390/jcm12082862