
Vitamin D, Albumin, and D-Dimer as Significant Prognostic Markers in Early Hospitalization in Patients with COVID-19
 ,
,
Abstract
:1. Introduction
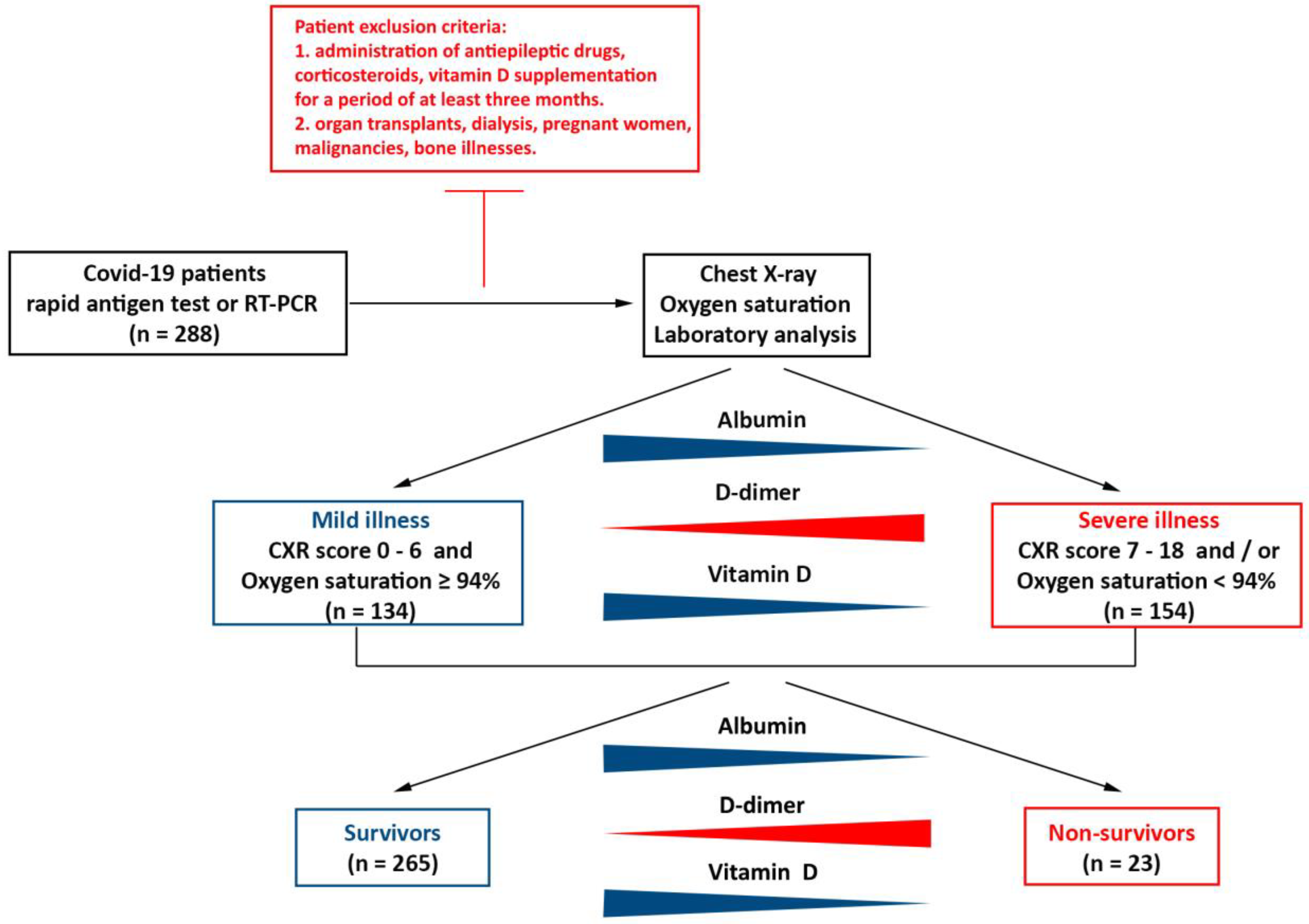
2. Materials and Methods
3. Statistical Analysis
4. Results
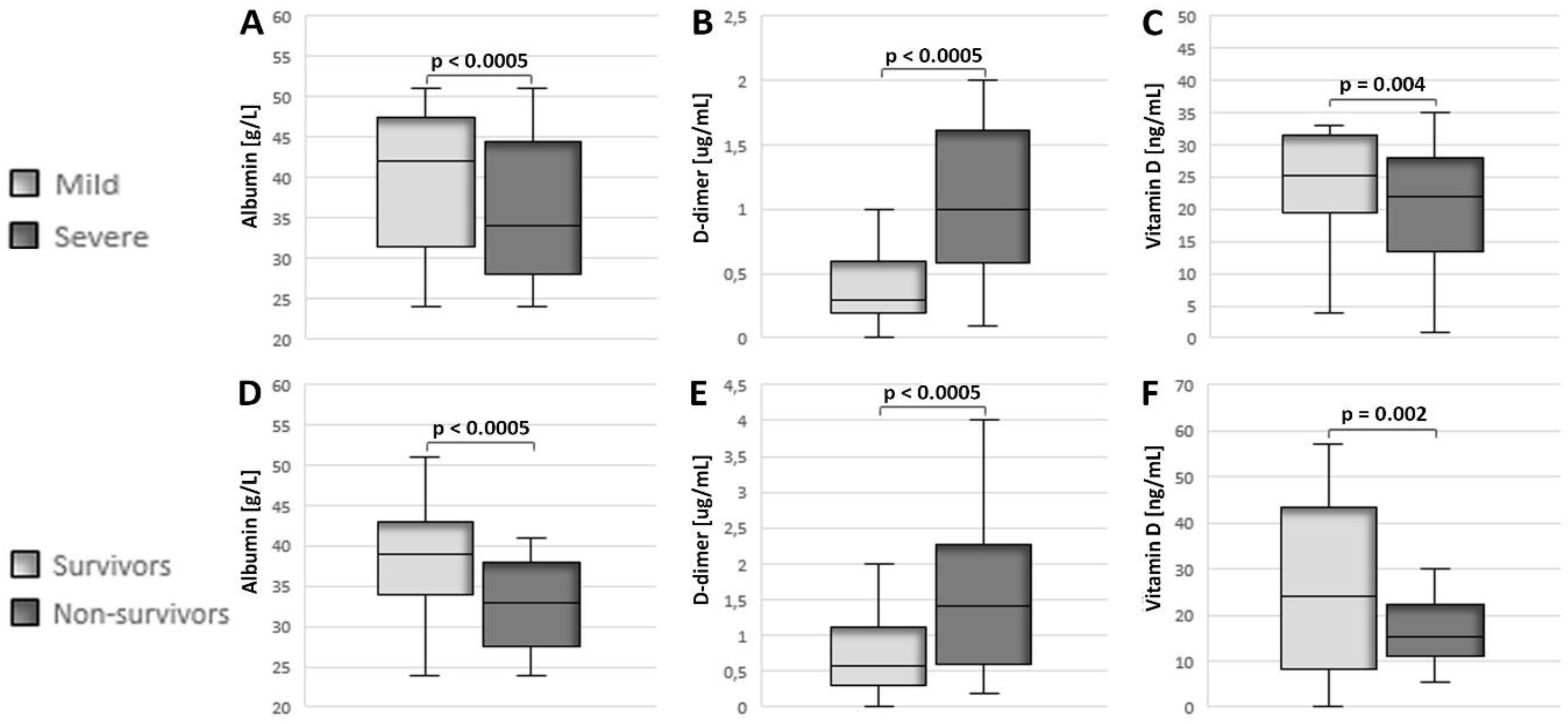
4.1. Decreased Levels of Vitamin D and Albumin, in Combination with Elevated Levels of D-Dimer, Indicate a More Severe Clinical Picture and a Fatal Outcome for Patients with COVID-19
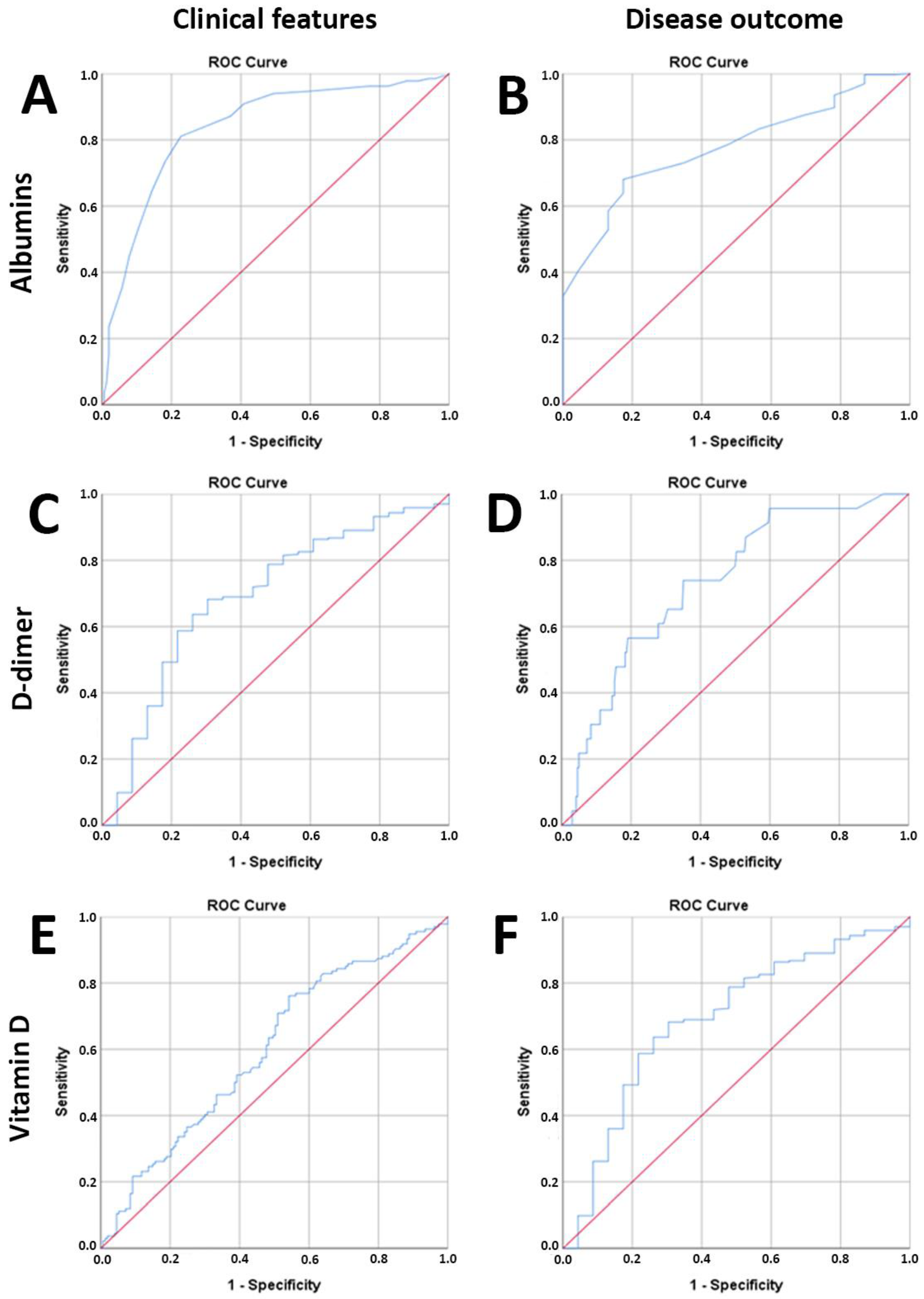
4.2. Serum Concentrations of Vitamin D, D-Dimer, and Albumin Are Significant Prognostic Factors for the Severity of the Clinical Picture and the Outcome of the Disease
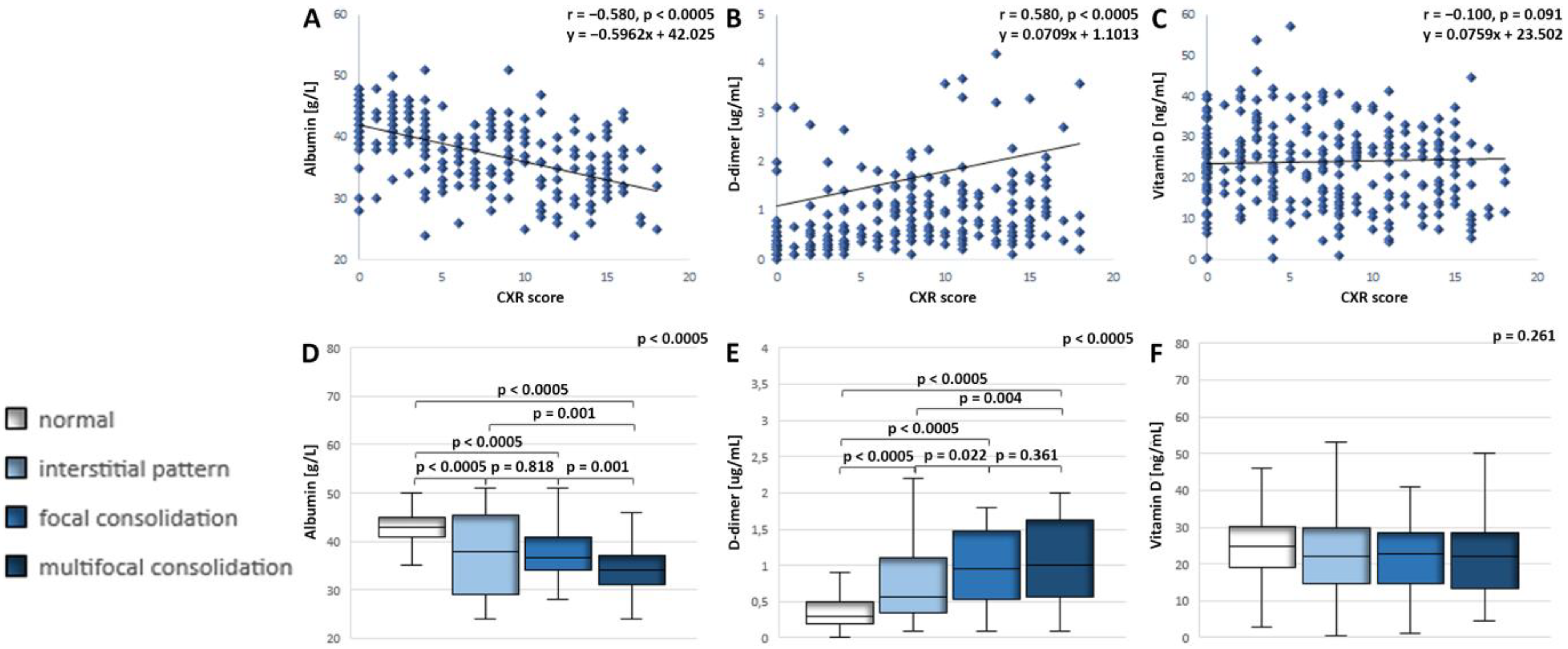
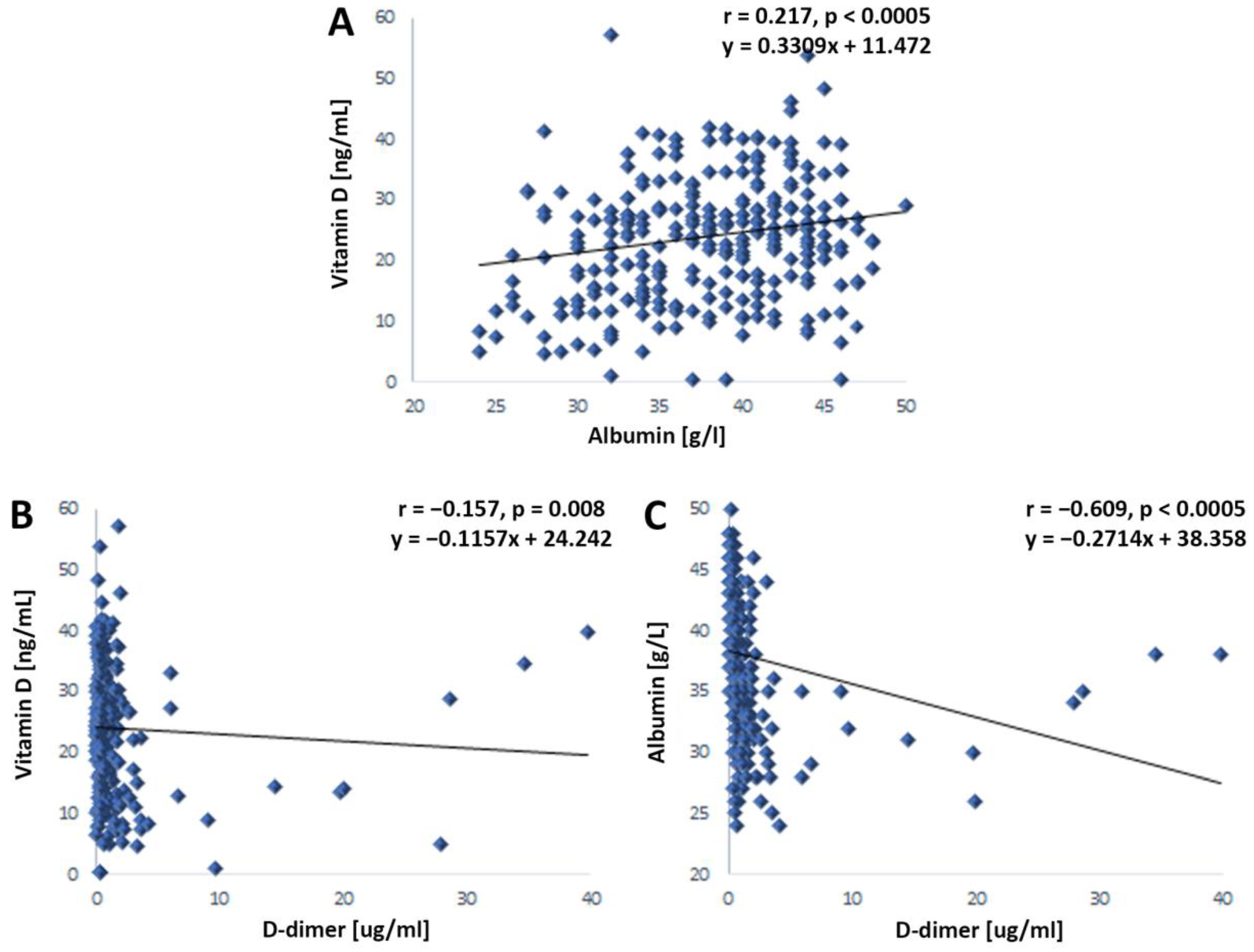
4.3. Interrelation of Serum Levels of Vitamin D, Albumin, and D-Dimer in Patients with COVID-19
4.4. Associations of Vitamin D, Albumin, and D-Dimer with Other Laboratory Parameters in Patients with COVID-19
4.5. The Influence of the Examined Set of Predictors (Albumin, D-Dimer, and Vitamin D) on the Development of a Severe Clinical Picture and a Fatal Disease Outcome in Patients with COVID-19
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zumla, A.; Chan, J.F.; Azhar, E.I.; Hui, D.S.; Yuen, K.Y. Coronaviruses—Drug discovery and therapeutic options. Nat. Rev. Drug Discov. 2016, 15, 327–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamsi, A.; Mohammad, T.; Anwar, S.; AlAjmi, M.F.; Hussain, A.; Rehman, M.T.; Islam, A.; Hassan, M.I. Glecaprevir and Maraviroc are high-affinity inhibitors of SARS-CoV-2 main protease: Possible implication in COVID-19 therapy. Biosci. Rep. 2020, 40, BSR20201256. [Google Scholar] [CrossRef]
- Mohammad, T.; Shamsi, A.; Anwar, S.; Umair, M.; Hussain, A.; Rehman, M.T.; AlAjmi, M.F.; Islam, A.; Hassan, M.I. Identification of high-affinity inhibitors of SARS-CoV-2 main protease: Towards the development of effective COVID-19 therapy. Virus Res. 2020, 288, 198102. [Google Scholar] [CrossRef]
- Shamsi, A.; Mohammad, T.; Anwar, S.; Amani, S.; Khan, M.S.; Husain, F.M.; Rehman, M.T.; Islam, A.; Hassan, M.I. Potential drug targets of SARS-CoV-2: From genomics to therapeutics. Int. J. Biol. Macromol. 2021, 177, 1–9. [Google Scholar] [CrossRef]
- Mann, R.; Perisetti, A.; Gajendran, M.; Gandhi, Z.; Umapathy, C.; Goyal, H. Clinical Characteristics, Diagnosis, and Treatment of Major Coronavirus Outbreaks. Front. Med. 2020, 7, 581521. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.A.; Martineau, A.R.; Hooper, R.L. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Alsegai, O.; Sridharan, K.; Hammad, M.; Hammad, M.M. Evaluation of serum vitamin D levels in COVID-19 positive critically ill adults. Pharmacia 2021, 68, 347–351. [Google Scholar] [CrossRef]
- Biesalski, H.K. Obesity, vitamin D deficiency and old age a serious combination with respect to coronavirus disease-2019 severity and outcome. Curr. Opin. Clin. Nutr. Metab. Care. 2021, 24, 18–24. [Google Scholar] [CrossRef]
- Bae, M.; Kim, H. Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules 2020, 25, 5346. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Slominski, R.M.; Goepfert, P.A.; Kim, T.-K.; Holick, M.F.; Jetten, A.M.; Raman, C. Reply to Jakovac and to Rocha et al.: Can vitamin D prevent or manage COVID-19 illness? Am. J. Physiol. Metab. 2020, 319, E455–E457. [Google Scholar] [CrossRef] [PubMed]
- Weir, E.K.; Thenappan, T.; Bhargava, M.; Chen, Y. Does vitamin D deficiency increase the severity of COVID-19? Clin. Med. 2020, 20, e107–e108. [Google Scholar] [CrossRef] [PubMed]
- Arboleda, J.F.; Urcuqui-Inchima, S. Vitamin D Supplementation: A Potential Approach for Coronavirus/COVID-19 Therapeutics? Front Immunol. 2020, 11, 1523. [Google Scholar] [CrossRef]
- Viana-Llamas, M.C.; Arroyo-Espliguero, R.; Silva-Obregón, J.A.; Uribe-Heredia, G.; Núñez-Gil, I.; García-Magallón, B.; Torán-Martínez, C.G.; Castillo-Sandoval, A.; Díaz-Caraballo, E.; Rodríguez-Guinea, I.; et al. Hypoalbuminemia on admission in COVID-19 infection: An early predictor of mortality and adverse events. A retrospective observational study. Med. Clin. 2021, 156, 428–436. [Google Scholar] [CrossRef]
- Turcato, G.; Zaboli, A.; Kostic, I.; Melchioretto, B.; Ciccariello, L.; Zaccaria, E.; Olivato, A.; Maccagnani, A.; Pfeifer, N.; Bonora, A. Severity of SARS-CoV-2 infection and albumin levels recorded at the first emergency department evaluation: A multicentre retrospective observational study. Emerg. Med. J. 2022, 39, 63–69. [Google Scholar] [CrossRef]
- Huang, J.; Cheng, A.; Kumar, R.; Fang, Y.; Chen, G.; Zhu, Y.; Lin, S. Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity. J. Med. Virol. 2020, 92, 2152–2158. [Google Scholar] [CrossRef]
- Soetedjo, N.N.M.; Iryaningrum, M.R.; Damara, F.A.; Permadhi, I.; Sutanto, L.B.; Hartono, H.; Rasyid, H. Prognostic properties of hypoalbuminemia in COVID-19 patients: A systematic review and diagnostic meta-analysis. Clin. Nutr. ESPEN 2021, 45, 120–126. [Google Scholar] [CrossRef]
- Rostami, M.; Mansouritorghabeh, H. D-dimer level in COVID-19 infection: A systematic review. Expert Rev. Hematol. 2020, 13, 1265–1275. [Google Scholar] [CrossRef]
- Shah, S.; Shah, K.; Patel, S.B.; Patel, F.S.; Osman, M.; Velagapudi, P.; Turagam, M.K.; Lakkireddy, D.; Garg, J. Elevated D-Dimer Levels Are Associated With Increased Risk of Mortality in Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Cardiol. Rev. 2020, 28, 295–302. [Google Scholar] [CrossRef]
- Poudel, A.; Poudel, Y.; Adhikari, A.; Aryal, B.B.; Dangol, D.; Bajracharya, T.; Maharjan, A.; Gautam, R. D-dimer as a biomarker for assessment of COVID-19 prognosis: D-dimer levels on admission and its role in predicting disease outcome in hospitalized patients with COVID-19. PLoS ONE 2021, 16, e0256744. [Google Scholar] [CrossRef]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. La Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2020. BMI Classification Percentile and Cut off Points. Available online: http://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 14 December 2020).
- Laird, E.; Rhodes, J.; Kenny, R.A. Vitamin D and inflammation: Potential implications for severity of COVID-19. Ir. Med. J. 2020, 113, 81. [Google Scholar]
- Albergamo, A.; Apprato, G.; Silvagno, F. The Role of Vitamin D in Supporting Health in the COVID-19 Era. Int. J. Mol. Sci. 2022, 23, 3621. [Google Scholar] [CrossRef] [PubMed]
- Soltani-Zangbar, M.S.; Mahmoodpoor, A.; Dolati, S.; Shamekh, A.; Valizadeh, S.; Yousefi, M.; Sanaie, S. Serum levels of vitamin D and immune system function in patients with COVID-19 admitted to intensive care unit. Gene Rep. 2022, 26, 101509. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Sandoval, J.C.; Castillos-Ávalos, V.J.; Paz-Cortés, A.; Santillan-Ceron, A.; Hernandez-Jimenez, S.; Mehta, R.; Correa-Rotter, R. Very Low Vitamin D Levels are a Strong Independent Predictor of Mortality in Hospitalized Patients with Severe COVID-19. Arch. Med. Res. 2021, 53, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Roizen, J.D.; Long, C.; Casella, A.; O’Lear, L.; Caplan, I.; Lai, M.; Sasson, I.; Singh, R.; Makowski, A.J.; Simmons, R.; et al. Obesity Decreases Hepatic 25-Hydroxylase Activity Causing Low Serum 25-Hydroxyvitamin D. J. Bone Miner. Res. 2019, 34, 1068–1073. [Google Scholar] [CrossRef]
- Singh, S.; Jain, R. Vitamin D deficiency in patients with diabetes and COVID-19 infection. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1033–1035. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2022, 62, 1308–1316. [Google Scholar] [CrossRef]
- Rivera-Paredez, B.; Hidalgo-Bravo, A.; León-Reyes, G.; León-Maldonado, L.S.; Aquino-Gálvez, A.; Castillejos-López, M.; Denova-Gutiérrez, E.; Flores, Y.N.; Salmerón, J.; Velázquez-Cruz, R. Total, Bioavailable, and Free 25-Hydroxyvitamin D Equally Associate with Adiposity Markers and Metabolic Traits in Mexican Adults. Nutrients 2021, 13, 3320. [Google Scholar] [CrossRef]
- Li, C.; Chen, P.; Duan, X.; Wang, J.; Shu, B.; Li, X.; Ba, Q.; Li, J.; Wang, Y.; Wang, H. Bioavailable 25(OH)D but Not Total 25(OH)D Is an Independent Determinant for Bone Mineral Density in Chinese Postmenopausal Women. Ebiomedicine 2016, 15, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matin, S.; Fouladi, N.; Pahlevan, Y.; Asghariazar, V.; Molaei, S.; Khiavi, H.A.; Negaresh, M.; Safarzadeh, E. The sufficient vitamin D and albumin level have a protective effect on COVID-19 infection. Arch. Microbiol. 2021, 203, 5153–5162. [Google Scholar] [CrossRef]
- Mehta, P.; Fajgenbaum, D.C. Is severe COVID-19 a cytokine storm syndrome: A hyperinflammatory debate. Curr. Opin. Rheumatol. 2021, 33, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Gungor, B.; Atici, A.; Baycan, O.F.; Alici, G.; Ozturk, F.; Tugrul, S.; Asoglu, R.; Cevik, E.; Sahin, I.; Barman, H.A. Elevated D-dimer levels on admission are associated with severity and increased risk of mortality in COVID-19: A systematic review and meta-analysis. Am. J. Emerg. Med. 2020, 39, 173–179. [Google Scholar] [CrossRef]
- Sengupta, T.; Majumder, R.; Majumder, S. Role of vitamin D in treating COVID-19-associated coagulopathy: Problems and perspectives. Mol. Cell. Biochem. 2021, 476, 2421–2427. [Google Scholar] [CrossRef]
- Bruinstroop, E.; van de Ree, M.; Huisman, M. The use of D-dimer in specific clinical conditions: A narrative review. Eur. J. Intern. Med. 2009, 20, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Ahmad Malik, J.; Ahmed, S.; Shinde, M.; Almermesh, M.H.S.; Alghamdi, S.; Hussain, A.; Anwar, S. The Impact of COVID-19 On Comorbidities: A Review Of Recent Updates For Combating It. Saudi J. Biol. Sci. 2022, 29, 3586–3599. [Google Scholar] [CrossRef]
- Teymoori-Rad, M.; Shokri, F.; Salimi, V.; Marashi, S.M. The interplay between vitamin D and viral infections. Rev. Med. Virol. 2019, 29, e2032. [Google Scholar] [CrossRef]
- Mohammad, S.; Mishra, A.; Ashraf, M.Z. Emerging Role of Vitamin D and its Associated Molecules in Pathways Related to Pathogenesis of Thrombosis. Biomolecules 2019, 9, 649. [Google Scholar] [CrossRef] [Green Version]
- Jovicic, B.P.; Rakovic, I.; Pavkovic, A.; Markovic, V.; Petrovic, S.; Gavrilovic, J.; Canovic, P.; Marjanovic, R.R.; Folic, M. Significance of initial clinical laboratoryparameters as prognostic factors in patients with COVID-19. Vojnosanit. Pregl. 2022, 79, 849–856. [Google Scholar] [CrossRef]
- Milan Manani, S.; Virzì, G.M.; Clementi, A.; Brocca, A.; De Cal, M.; Tantillo, I.; Ferrando, L.; Crepaldi, C.; Ronco, C. Pro-inflammatory cytokines: A possible relationship with dialytic adequacy and serum albumin in peritoneal dialysis patients. Clin. Kidney J. 2016, 9, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Milenkovic, M.; Hadzibegovic, A.; Kovac, M.; Jovanovic, B.; Stanisavljevic, J.; Djikic, M.; Sijan, D.; Ladjevic, N.; Palibrk, I.; Djukanovic, M.; et al. D-dimer, CRP, PCT, and IL-6 Levels at Admission to ICU Can Predict In-Hospital Mortality in Patients with COVID-19 Pneumonia. Oxidative Med. Cell. Longev. 2022, 2022, 8997709. [Google Scholar] [CrossRef] [PubMed]
- Senol, A. The ability of D-dimer, albumin, and D-Dimer/albumin ratio to predict in-hospital mortality and intensive care unit admission in COVID-19 patients admitted to the emergency department. Bratisl. Med. J. 2022, 123, 908–912. [Google Scholar] [CrossRef]
- Violi, F.; Ceccarelli, G.; Loffredo, L.; Alessandri, F.; Cipollone, F.; D’Ardes, D.; D’Ettorre, G.; Pignatelli, P.; Venditti, M.; Mastroianni, C.M.; et al. Albumin Supplementation Dampens Hypercoagulability in COVID-19: A Preliminary Report. Thromb. Haemost. 2020, 121, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Aloisio, E.; Serafini, L.; Chibireva, M.; Dolci, A.; Panteghini, M. Hypoalbuminemia and elevated D-dimer in COVID-19 patients: A call for result harmonization. Clin. Chem. Lab. Med. 2020, 58, e255–e256. [Google Scholar] [CrossRef] [PubMed]
- Küçükceran, K.; Ayranci, M.K.; Girişgin, A.S.; Koçak, S. Predictive value of D-dimer/albumin ratio and fibrinogen/albumin ratio for in-hospital mortality in patients with COVID-19. Int. J. Clin. Pract. 2021, 75, e14263. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yang, H.; Wang, J.; Li, X.; Xue, C.; Niu, C.; Liao, P. Serum Albumin Levels are a Predictor of COVID-19 Patient Prognosis: Evidence from a Single Cohort in Chongqing, China. Int. J. Gen. Med. 2021, 14, 2785–2797. [Google Scholar] [CrossRef] [PubMed]
- Zerbato, V.; Sanson, G.; De Luca, M.; Di Bella, S.; di Masi, A.; Caironi, P.; Marini, B.; Ippodrino, R.; Luzzati, R. The Impact of Serum Albumin Levels on COVID-19 Mortality. Infect. Dis. Rep. 2022, 14, 278–286. [Google Scholar] [CrossRef]
- Vanegas-Cedillo, P.E.; Bello-Chavolla, O.Y.; Ramírez-Pedraza, N.; Rodríguez Encinas, B.; Pérez Carrión, C.I.; Jasso-Ávila, M.I.; Valladares-García, J.C.; Hernández-Juárez, D.; Vargas-Vázquez, A.; Antonio-Villa, N.E.; et al. Serum Vitamin D Levels Are Associated With Increased COVID-19 Severity and Mortality Independent of Whole-Body and Visceral Adiposity. Front. Nutr. 2022, 9, 813485. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Clinical Features | Disease Outcome | |||||
|---|---|---|---|---|---|---|---|
| Mild | Severe | p Value | Survivors | Non-Survivors | p Value | ||
| Patients | 134 (46.5%) | 154 (53.5%) | NA | 265 (92.0%) | 23 (8.0%) | NA | |
| Gender | Male | 77 (40.3%) | 114 (59.7%) | 0.004 * | 175 (91.6%) | 16 (8.4%) | 0.821 * |
| Female | 57 (58.8%) | 40 (41.2%) | 90 (92.8%) | 7 (7.2%) | |||
| Age Mdn (1Q, 3Q) | 45.5 (37.8, 59.3) | 65.5 (55.0, 71.0) | <0.0005 ** | 57 (42.0, 67.0) | 70 (67.0, 77.0) | <0.0005 ** | |
| BMI Mdn (1Q, 3Q) | 24.8 (22.1, 26.8) | 27.8 (26.0, 30.8) | <0.0005 ** | 26.3 (24.0, 29.1) | 27.8 (25.8, 29.8) | 0.076 ** | |
| Diabetes mellitus | No | 124 (69.7%) | 103 (30.3%) | <0.0005 * | 214 (94.3%) | 13 (5.7%) | 0.012 * |
| Yes | 8 (26.0%) | 51 (74.0%) | 49 (83.1%) | 10 (16.9%) | |||
| Arterial hypertension | No | 105 (62.9%) | 62 (37.1%) | <0.0005 * | 160 (95.8%) | 7 (4.2%) | 0.007 * |
| Yes | 27 (22.7%) | 92 (77.3%) | 103 (86.6%) | 16 (13.4%) | |||
| Obstructive lung disease | No | 125 (46.5%) | 144 (53.5%) | 0.777 * | 247 (91.8%) | 22 (8.2%) | NA |
| Yes | 5 (38.5%) | 8 (61.5%) | 12 (92.3%) | 1 (7.7%) | |||
| Clinical Features | Variables | Albumin (g/L) | D-dimer (ug/mL) | Vitamin D (ng/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Spearman’s Rho | p Value | N | Spearman’s Rho | p Value | N | Spearman’s Rho | p Value | N | ||
| Mild | Albumin (g/L) | 1.000 | . | 132 | −0.512 | <0.0005 | 131 | −0.022 | 0.799 | 132 |
| D-dimer (ug/mL) | −0.512 | <0.0005 | 131 | 1.000 | . | 132 | 0.054 | 0.540 | 132 | |
| Vitamin D (ng/mL) | −0.022 | 0.799 | 132 | 0.054 | 0.540 | 132 | 1.000 | . | 134 | |
| Severe | Albumin (g/L) | 1.000 | . | 154 | −0.368 | <0.0005 | 153 | 0.288 | <0.0005 | 153 |
| D-dimer (ug/mL) | −0.368 | <0.0005 | 153 | 1.000 | . | 153 | −0.239 | 0.003 | 152 | |
| Vitamin D (ng/mL) | 0.288 | <0.0005 | 153 | −0.239 | 0.003 | 152 | 1.000 | . | 153 | |
| Variables | Albumin (g/L) | D-dimer (ug/mL) | Vitamin D (ng/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Spearman’s Rho | p Value | N | Spearman’s Rho | p Value | N | Spearman’s Rho | p Value | N | |
| WBC (109/L) | −0.332 | <0.0005 | 285 | 0.261 | <0.0005 | 284 | −0.151 | 0.011 | 285 |
| Lym (109/L) | 0.432 | <0.0005 | 285 | −0.418 | <0.0005 | 284 | 0.034 | 0.562 | 285 |
| PLT (109/L) | −0.134 | 0.024 | 285 | 0.119 | 0.045 | 284 | −0.110 | 0.063 | 285 |
| BG (mmol/L) | −0.345 | <0.0005 | 285 | 0.332 | <0.0005 | 284 | −0.134 | 0.024 | 285 |
| K (mmol/L) | 0.091 | 0.126 | 281 | −0.045 | 0.454 | 280 | −0.016 | 0.787 | 281 |
| CRP (mg/L) | −0.651 | <0.0005 | 286 | 0.626 | <0.0005 | 285 | −0.071 | 0.229 | 286 |
| PCT (ng/mL) | −0.466 | <0.0005 | 285 | 0.488 | <0.0005 | 284 | −0.087 | 0.141 | 285 |
| AST (IU/L) | −0.341 | <0.0005 | 286 | 0.429 | <0.0005 | 285 | −0.027 | 0.655 | 286 |
| ALT (IU/L) | −0.139 | 0.018 | 286 | 0.232 | <0.0005 | 285 | −0.018 | 0.765 | 286 |
| CKMB (U/L) | −0.247 | <0.0005 | 284 | 0.241 | <0.0005 | 283 | −0.174 | 0.003 | 284 |
| LDH (U/L) | −0.491 | <0.0005 | 286 | 0.595 | <0.0005 | 285 | −0.096 | 0.107 | 286 |
| pro-BNP (pg/mL) | −0.658 | <0.0005 | 283 | 0.589 | <0.0005 | 282 | −0.248 | <0.0005 | 283 |
| Fibrinogen (g/L) | −0.488 | <0.0005 | 264 | 0.501 | <0.0005 | 265 | 0.067 | 0.276 | 265 |
| PT (s) | −0.377 | <0.0005 | 253 | 0.331 | <0.0005 | 254 | −0.103 | 0.100 | 255 |
| INR | −0.342 | <0.0005 | 257 | 0.206 | 0.001 | 258 | −0.136 | 0.029 | 259 |
| hsTnI (ng/mL) | −0.272 | <0.0005 | 283 | 0.251 | <0.0005 | 282 | −0.107 | 0.072 | 283 |
| Ferritin (ug/L) | −0.462 | <0.0005 | 285 | 0.478 | <0.0005 | 284 | 0.024 | 0.682 | 285 |
| B | S.E. | Wald | df | p Value | Exp(B) | 95% C.I. for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Albumin (g/L) | −0.276 | 0.034 | 64.833 | 1 | <0.0005 | 0.759 | 0.710 | 0.812 |
| D-dimer (ug/mL) | −0.011 | 0.031 | 0.114 | 1 | 0.736 | 0.989 | 0.931 | 1.052 |
| Vitamin D (ng/mL) | 0.000 | 0.007 | 0.005 | 1 | 0.946 | 1.000 | 0.985 | 1.014 |
| Constant | 10.759 | 1.350 | 63.483 | 1 | <0.0005 | 47,048.223 | ||
| B | S.E. | Wald | df | p Value | Exp(B) | 95% C.I. for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Albumin (g/L) | −0.194 | 0.046 | 18.144 | 1 | <0.0005 | 0.823 | 0.753 | 0.900 |
| D-dimer (ug/mL) | −0.026 | 0.062 | 0.179 | 1 | 0.672 | 0.974 | 0.863 | 1.099 |
| Vitamin D (ng/mL) | 0.010 | 0.007 | 1.965 | 1 | 0.161 | 1.010 | 0.996 | 1.025 |
| Constant | 4.261 | 1.552 | 7.541 | 1 | 0.006 | 70.910 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popovska Jovičić, B.; Raković, I.; Gavrilović, J.; Sekulić Marković, S.; Petrović, S.; Marković, V.; Pavković, A.; Čanović, P.; Radojević Marjanović, R.; Irić-Čupić, V.; et al. Vitamin D, Albumin, and D-Dimer as Significant Prognostic Markers in Early Hospitalization in Patients with COVID-19. J. Clin. Med. 2023, 12, 2825. https://doi.org/10.3390/jcm12082825
Popovska Jovičić B, Raković I, Gavrilović J, Sekulić Marković S, Petrović S, Marković V, Pavković A, Čanović P, Radojević Marjanović R, Irić-Čupić V, et al. Vitamin D, Albumin, and D-Dimer as Significant Prognostic Markers in Early Hospitalization in Patients with COVID-19. Journal of Clinical Medicine. 2023; 12(8):2825. https://doi.org/10.3390/jcm12082825
Chicago/Turabian StylePopovska Jovičić, Biljana, Ivana Raković, Jagoda Gavrilović, Sofija Sekulić Marković, Sara Petrović, Vladan Marković, Aleksandar Pavković, Predrag Čanović, Ružica Radojević Marjanović, Violeta Irić-Čupić, and et al. 2023. "Vitamin D, Albumin, and D-Dimer as Significant Prognostic Markers in Early Hospitalization in Patients with COVID-19" Journal of Clinical Medicine 12, no. 8: 2825. https://doi.org/10.3390/jcm12082825