Determinants of Lipid Parameters in Patients without Diagnosed Cardiovascular Disease—Results of the Polish Arm of the EUROASPIRE V Survey

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of Lipid Parameters
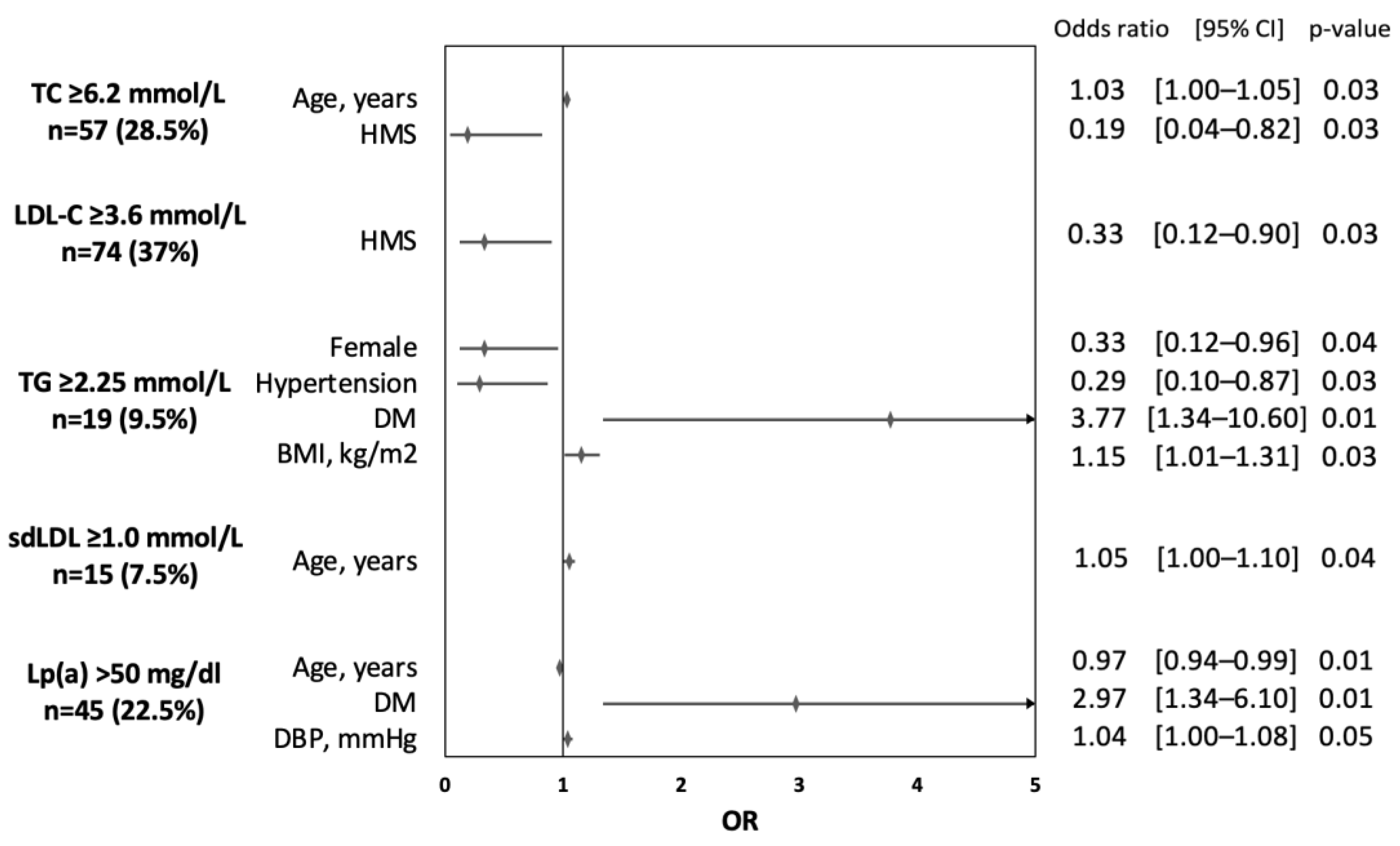
3.2. Determinants of Elevated Lipid Parameters
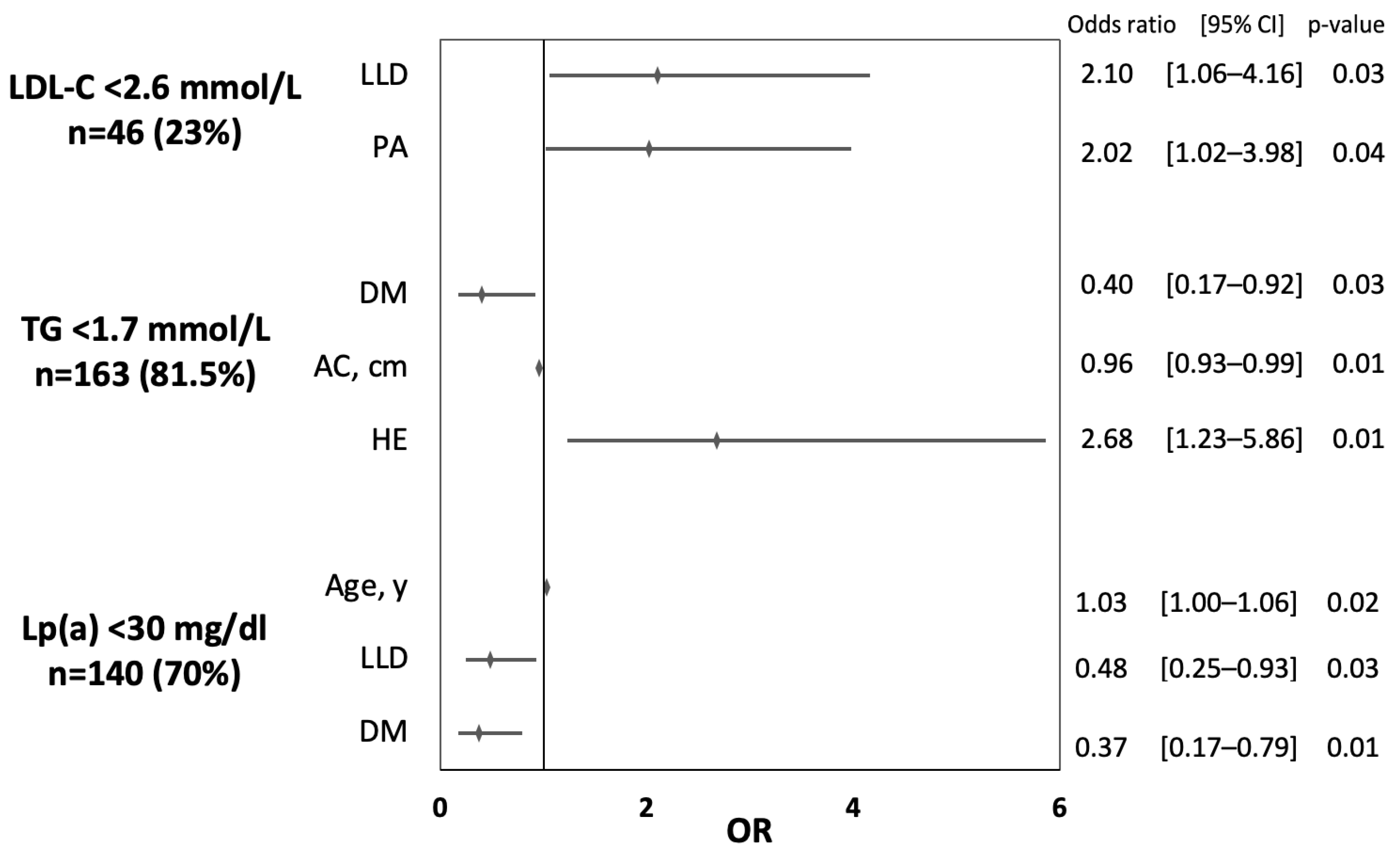
3.3. Determinants of Adequate Control of Lipid Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Borén, J.; Williams, K.J. The Central Role of Arterial Retention of Cholesterol-Rich Apolipoprotein-B-Containing Lipoproteins in the Pathogenesis of Atherosclerosis: A Triumph of Simplicity. Curr. Opin. Lipidol. 2016, 27, 473–483. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Primary Prevention Efforts Are Poorly Developed in People at High Cardiovascular Risk: A Report from the European Society of Cardiology EURObservational Research Programme EUROASPIRE V Survey in 16 European Countries. Eur. J. Prev. Cardiol. 2021, 28, 370–379. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The Effects of Lowering LDL Cholesterol with Statin Therapy in People at Low Risk of Vascular Disease: Meta-Analysis of Individual Data from 27 Randomised Trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.H.; Lee, J.B.; Kim, S.H.; Jo, M.-W.; Hwang, J.Y.; Bae, S.J.; Jung, C.H.; Lee, W.J.; Park, J.-Y.; Park, G.-M.; et al. Serum Triglyceride Levels and Cardiovascular Disease Events in Koreans. Cardiology 2015, 131, 228–235. [Google Scholar] [CrossRef]
- Nordestgaard, B.G. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and Biology. Circ. Res. 2016, 118, 547–563. [Google Scholar] [CrossRef]
- Sarwar, N.; Danesh, J.; Eiriksdottir, G.; Sigurdsson, G.; Wareham, N.; Bingham, S.; Boekholdt, S.M.; Khaw, K.-T.; Gudnason, V. Triglycerides and the Risk of Coronary Heart Disease: 10,158 Incident Cases among 262,525 Participants in 29 Western Prospective Studies. Circulation 2007, 115, 450–458. [Google Scholar] [CrossRef]
- Burgess, S.; Ference, B.A.; Staley, J.R.; Freitag, D.F.; Mason, A.M.; Nielsen, S.F.; Willeit, P.; Young, R.; Surendran, P.; Karthikeyan, S.; et al. Association of LPA Variants with Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol. 2018, 3, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Szczepaniak-Chicheł, L.; Mastej, M.; Piwowarska, W.; Jóźwiak, J.; Konduracka, E.; Tykarski, A. Metabolic Factors of Cardiovascular Risk in LIPIDOGRAM 2004 Study. Arter. Hypertens. 2006, 10, 377–392. [Google Scholar]
- Zdrojewski, T.; Solnica, B.; Cybulska, B.; Bandosz, P.; Rutkowski, M.; Stokwiszewski, J.; Gaciong, Z.; Banach, M.; Wojtyniak, B.; Pencina, M.; et al. Prevalence of Lipid Abnormalities in Poland. The NATPOL 2011 Survey. Kardiol. Pol. 2016, 74, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Pająk, A.; Szafraniec, K.; Polak, M.; Polakowska, M.; Kozela, M.; Piotrowski, W.; Kwaśniewska, M.; Podolecka, E.; Kozakiewicz, K.; Tykarski, A.; et al. Changes in the Prevalence, Treatment, and Control of Hypercholesterolemia and Other Dyslipidemias over 10 Years in Poland: The WOBASZ Study. Pol. Arch. Intern. Med. 2016, 126, 642–652. [Google Scholar] [CrossRef] [Green Version]
- Scheidt-Nave, C.; Du, Y.; Knopf, H.; Schienkiewitz, A.; Ziese, T.; Nowossadeck, E.; Gößwald, A.; Busch, M.A. Prevalence of dyslipidemia among adults in Germany: Results of the German Health Interview and Examination Survey for Adults (DEGS 1). Bundesgesundheitsbl. Gesundh. Gesundh. 2013, 56, 661–667. [Google Scholar] [CrossRef] [Green Version]
- Tóth, P.P.; Potter, D.; Ming, E.E. Prevalence of Lipid Abnormalities in the United States: The National Health and Nutrition Examination Survey 2003–2006. J. Clin. Lipidol. 2012, 6, 325–330. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Santos, H.O.; Earnest, C.P.; Tinsley, G.M.; Izidoro, L.F.M.; Macedo, R.C.O. Small Dense Low-Density Lipoprotein-Cholesterol (SdLDL-C): Analysis, Effects on Cardiovascular Endpoints and Dietary Strategies. Prog. Cardiovasc. Dis. 2020, 63, 503–509. [Google Scholar] [CrossRef]
- Laskowska, E.; Michalski, P.; Pietrzykowski, Ł.; Kasprzak, M.; Kosobucka, A.; Grzelakowska, K.; Buczkowski, K.; Jankowski, P.; Gąsior, Z.; Kosior, D.; et al. Implementation of Therapeutic Recommendations in High Cardiovascular-Risk Patients. The Polish Population of EUROASPIRE V Survey. Med. Res. J. 2021, 6, 230–236. [Google Scholar] [CrossRef]
- Michalski, P.; Kasprzak, M.; Pietrzykowski, Ł.; Grzelakowska, K.; Buczkowski, K.; Gąsior, Z.; Kosior, D.; Kamiński, K.; Jankowski, P.; Kubica, A. Ambulatory Assessment of Medication Adherence in High Cardiovascular-Risk Patients. The Polish Population of the EUROASPIRE V Survey. Med. Res. J. 2021, 6, 316–321. [Google Scholar] [CrossRef]
- Kubica, A.; Pietrzykowski, Ł.; Michalski, P.; Kasprzak, M.; Ratajczak, J.; Siódmiak, J.; Fabiszak, T.; Buczkowski, K.; Krintus, M.; Jankowski, P. The Occurrence of Cardiovascular Risk Factors and Functioning in Chronic Illness in the Polish Population of EUROASPIRE V. Cardiol. J. 2022. [Google Scholar] [CrossRef]
- Jankowski, P.; Kosior, D.; Sowa, P.; Szóstak-Janiak, K.; Kozieł, P.; Krzykwa, A.; Sawicka, E.; Haberka, M.; Setny, M.; Kamiński, K.; et al. Secondary Prevention of Coronary Artery Disease in Poland. Results from the POLASPIRE Survey. Cardiol. J. 2020, 27, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.A.; Santos Ferreira, D.L.; Fraser, A.; Soares, A.L.G.; Howe, L.D.; Lawlor, D.A.; Carslake, D.; Davey Smith, G.; O’Keeffe, L.M. Sex Differences in Systemic Metabolites at Four Life Stages: Cohort Study with Repeated Metabolomics. BMC Med. 2021, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Al-Shali, K.Z.; Hegele, R.A. Hypertriglyceridemia: Its Etiology, Effects and Treatment. CMAJ 2007, 176, 1113–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubica, A.; Gruchała, M.; Jaguszewski, M.; Jankowski, P.; Świeczkowski, D.; Merks, P.; Uchmanowicz, I. Adherence to Treatment—A Pivotal Issue in Long-Term Treatment of Patients with Cardiovascular Diseases. An Expert Standpoint. Med. Res. J. 2017, 2, 123–127. [Google Scholar] [CrossRef] [Green Version]
- De Backer, G.; Jankowski, P.; Kotseva, K.; Mirrakhimov, E.; Reiner, Ž.; Rydén, L.; Tokgözoğlu, L.; Wood, D.; De Bacquer, D.; EUROASPIRE V Collaborators; et al. Management of Dyslipidaemia in Patients with Coronary Heart Disease: Results from the ESC-EORP EUROASPIRE V Survey in 27 Countries. Atherosclerosis 2019, 285, 135–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankowski, P.; Kozieł, P.; Setny, M.; Paniczko, M.; Haberka, M.; Banach, M.; Bacquer, D.D.; Backer, G.D.; Kotseva, K.; Wood, D.; et al. Dyslipidemia Management in Patients with Coronary Artery Disease. Data from the POLASPIRE Survey. J. Clin. Med. 2021, 10, 3711. [Google Scholar] [CrossRef]
- Sygnowska, E.; Piwońska, A.; Waśkiewicz, A.; Broda, G. Socioeconomic Factors and the Risk of Metabolic Syndrome in the Adult Polish Population: The WOBASZ Study. Kardiol. Pol. 2012, 70, 718–727. [Google Scholar]
- Ai, M.; Otokozawa, S.; Asztalos, B.F.; Ito, Y.; Nakajima, K.; White, C.C.; Cupples, L.A.; Wilson, P.W.; Schaefer, E.J. Small Dense LDL Cholesterol and Coronary Heart Disease: Results from the Framingham Offspring Study. Clin. Chem. 2010, 56, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Hoogeveen, R.C.; Gaubatz, J.W.; Sun, W.; Dodge, R.C.; Crosby, J.R.; Jiang, J.; Couper, D.; Virani, S.S.; Kathiresan, S.; Boerwinkle, E.; et al. Small Dense Low-Density Lipoprotein-Cholesterol Concentrations Predict Risk for Coronary Heart Disease: The Atherosclerosis Risk In Communities (ARIC) Study. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Płaczkowska, S.; Sołkiewicz, K.; Bednarz-Misa, I.; Kratz, E.M. Atherogenic Plasma Index or Non-High-Density Lipoproteins as Markers Best Reflecting Age-Related High Concentrations of Small Dense Low-Density Lipoproteins. Int. J. Mol. Sci. 2022, 23, 5089. [Google Scholar] [CrossRef]
- Izumida, T.; Nakamura, Y.; Sato, Y.; Ishikawa, S. Association among Age, Gender, Menopausal Status and Small Dense Low-Density Lipoprotein Cholesterol: A Cross-Sectional Study. BMJ Open 2021, 11, e041613. [Google Scholar] [CrossRef] [PubMed]
- Tsimikas, S.; Gordts, P.L.S.M.; Nora, C.; Yeang, C.; Witztum, J.L. Statin Therapy Increases Lipoprotein(a) Levels. Eur. Heart J. 2020, 41, 2275–2284. [Google Scholar] [CrossRef] [PubMed]
- Gudbjartsson, D.F.; Thorgeirsson, G.; Sulem, P.; Helgadottir, A.; Gylfason, A.; Saemundsdottir, J.; Bjornsson, E.; Norddahl, G.L.; Jonasdottir, A.; Jonasdottir, A.; et al. Lipoprotein(a) Concentration and Risks of Cardiovascular Disease and Diabetes. J. Am. Coll. Cardiol. 2019, 74, 2982–2994. [Google Scholar] [CrossRef] [PubMed]
- Lamina, C.; Ward, N.C. Lipoprotein (a) and Diabetes Mellitus. Atherosclerosis 2022, 349, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, L.C.; Arauz-Pacheco, C.; Lackner, C.; Albright, G.; Adams, B.V.; Raskin, P. Lipoprotein (a) Levels in Diabetes Mellitus: Relationship to Metabolic Control. Ann. Intern. Med. 1992, 117, 42–47. [Google Scholar] [CrossRef]
- Simony, S.B.; Mortensen, M.B.; Langsted, A.; Afzal, S.; Kamstrup, P.R.; Nordestgaard, B.G. Sex Differences of Lipoprotein(a) Levels and Associated Risk of Morbidity and Mortality by Age: The Copenhagen General Population Study. Atherosclerosis 2022, 355, 76–82. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Analyzed Parameter | Value | |
|---|---|---|
| Age, median (IQR) | 52.0 (43.0–60.0) | |
| Years of education, median (IQR) | 15.0 (13.0–17.0) | |
| Higher education, n (%) | 117 (58.5) | |
| Female gender, n (%) | 133 (66.5) | |
| Material status, n (%) | Low | 30 (15.0) |
| Average | 141(70.5) | |
| High | 29 (14.5) | |
| History of hyperlipidemia, n (%) | 105 (52.5) | |
| Lipid-lowering drugs, n (%) | 92 (46.0) | |
| History of hypertension, n (%) | 140 (70.0) | |
| BP-lowering drugs, n (%) | 126 (63.0) | |
| SBP [mmHg], median (IQR) | 125.0 (118.0–135.0) | |
| DBP [mmHg], median (IQR) | 77.0 (70.0–82.0) | |
| SBP/DBP < 140/90 mmHg, n (%) | 155 (77.5) | |
| History of DM, n (%) | 41 (20.5) | |
| Insulin and/or oral medications, n (%) | 17 (8.5) | |
| FPG [mmol/L], median (IQR) | 5.42 (5.04–5.88) | |
| FPG < 5.56 mmol/L (<100 mg/dL), n (%) | 117 (58.5) | |
| AC [cm], median (IQR) | 87.0 (80.0–95.5) | |
| AC, n (%) | Normal | 74 (37.0) |
| Overweight [F ≥ 80 cm and <88 cm, M ≥ 94 cm and <102 cm] | 57 (28.5) | |
| Obesity [F ≥ 88 cm, M ≥ 102 cm] | 69 (34.5) | |
| BMI [kg/m2], median (IQR) | 26.0 (24.0–28.7) | |
| BMI category, n (%) | Underweight < 18.5 kg/m2 | 6 (3.0) |
| Normal 18.5–24.9 kg/m2 | 77 (38.5) | |
| Overweight 25.0–29.9 kg/m2 | 84 (42.0) | |
| Obesity > 30.0 kg/m2 | 33 (16.5) | |
| Non-smoker status, n (%) | 170 (85.0) | |
| Adequate physical activity, n (%) | 81 (40.5) | |
| hsTnI [ng/L], median (IQR) | 2.3 (1.6–3.2) | |
| CRP [mg/L], median (IQR) | 0.9 (0.6–1.7) | |
| Serum creatinine [mg/dL], median (IQR) | 0.8 (0.7–0.9) |
| Subgroups | TC [mmol/L] | LDL-C [mmol/L] | HDL-C [mmol/L] | TG [mmol/L] | sdLDL-C [mmol/L] | Lp(a) [mg/dL] | |
|---|---|---|---|---|---|---|---|
| Total population | 5.56 (4.91–6.26) | 3.29 (2.68–4.0) | 1.50 (1.25–1.81) | 1.21 (0.90–1.55) | 0.64 (0.53–0.78) | 9.19 (3.54–42.07) | |
| Gender | Female | 5.64 (5.02–6.43) | 3.30 (2.69–4.17) | 1.60 (1.37–1.90) | 1.13 (0.88–1.44) | 0.63 (0.52–0.79) | 8.20 (3.45–40.6) |
| Male | 5.45 (4.77–6.08) | 3.13 (2.6–3.89) | 1.33 (1.18–1.54) | 1.33 (0.96–1.75) | 0.65 (0.53–0.79) | 11.12 (3.77–42.2) | |
| p-value | 0.055 | 0.19 | < 0.001 | 0.03 | 0.96 | 0.62 | |
| Age | < 60 years | 5.51 (4.89–6.19) | 3.15 (2.66–3.87) | 1.47 (1.27–1.78) | 1.15 (0.88–1.51) | 0.63 (0.53–0.75) | 10.55 (3.48–61.01) |
| ≥ 60 years | 5.72 (5.07–6.95) | 3.45 (2.72–4.51) | 1.59 (1.26–1.87) | 1.30 (0.96–1.64) | 0.66 (0.53–0.90) | 6.60 (3.64–14.21) | |
| p-value | 0.045 | 0.057 | 0.287 | 0.125 | 0.084 | 0.171 | |
| DM | No | 5.55 (4.94–6.23) | 3.30 (2.70–4.03) | 1.53 (1.28–1.84) | 1.14 (0.88–1.50) | 0.63 (0.52–0.77) | 8.30 (3.48–35.59) |
| Yes | 5.57 (5.07–6.42) | 3.28 (2.58–3.83) | 1.38 (1.18–1.76) | 1.39 (0.97–2.14) | 0.66 (0.54–0.80) | 13.30 (3.98–78.80) | |
| p-value | 0.906 | 0.721 | 0.036 | 0.012 | 0.429 | 0.094 | |
| HT | No | 5.65 (5.15–6.61) | 3.29 (2.69–4.17) | 1.54 (1.23–1.77) | 1.30 (0.97–1.78) | 0.69 (0.54–0.86) | 14.21 (4.05–52.86) |
| Yes | 5.51 (4.82–6.21) | 3.29 (2.68–3.92) | 1.48 (1.27–1.83) | 1.15 (0.88–1.51) | 0.60 (0.52–0.75) | 6.81 (3.46–37.4) | |
| p-value | 0.080 | 0.596 | 0.670 | 0.105 | 0.061 | 0.078 | |
| BMI categories | Normal | 5.62 (5.0–6.27) | 3.3 (2.71–3.93) | 1.59 (1.35–1.89) | 1.09 (0.85–1.35) | 0.61 (0.51–0.73) | 11.12 (3.74–64.58) |
| Overweight | 5.54 (4.85–6.34) | 3.28 (2.66–4.08) | 1.44 (1.24–1.76) | 1.3 (0.93–1.61) | 0.66 (0.55–0.81) | 10.55 (3.61–33.33) | |
| Obesity | 5.4 (4.75–6.18) | 3.17 (2.62–3.93) | 1.4 (1.19–1.65) | 1.35 (0.96–2.15) | 0.64 (0.53–0.81) | 5.68 (3.0–23.48) | |
| p-value | 0.409 | 0.850 | 0.043 | 0.012 | 0.173 | 0.162 | |
| AC categories | Normal | 5.46 (4.65–6.12) | 3.14 (2.61–3.7) | 1.5 (1.24–1.81) | 1.07 (0.88–1.36) | 0.58 (0.51–0.72) | 11.96 (4.06–64.0) |
| Overweight | 5.68 (5.11–6.27) | 3.42 (2.82–4.07) | 1.59 (1.36–1.81) | 1.24 (0.89–1.52) | 0.66 (0.53–0.77) | 10.4 (3.57–49.6) | |
| Obesity | 5.59 (4.87–6.52) | 3.17 (2.6–4.24) | 1.44 (1.24–1.89) | 1.35 (0.96–1.8) | 0.66 (0.54–0. 091) | 6.9 (3.0–24.37) | |
| p-value | 0.258 | 0.259 | 0.418 | 0.023 | 0.038 | 0.228 | |
| Education | Primary/ Secondary | 5.54 (5.02–6.27) | 3.27 (2.71–4.16) | 1.44 (1.24–1.71) | 1.39 (1.09–1.76) | 0.66 (0.53–0.81) | 8.36 (3.0–40.6) |
| Higher | 5.58 (4.88–6.22) | 3.29 (2.63–3.89) | 1.52 (1.29–1.89) | 1.06 (0.83–1.37) | 0.60 (0.52–0.76) | 10.02 (3.74–41.6) | |
| p-value | 0.810 | 0.332 | 0.123 | < 0.001 | 0.241 | 0.393 | |
| Material status | Very low/Low | 5.58 (5.07–6.68) | 3.38 (2.72–4.19) | 1.43 (1.21–1.88) | 1.34 (1.03–2.08) | 0.67 (0.56–0.87) | 5.82 (3.22–51.72) |
| Average | 5.69 (4.97–6.36) | 3.35 (2.63–4.06) | 1.55 (1.29–1.81) | 1.23 (0.92–1.56) | 0.64 (0.52–0.78) | 10.02 (3.6–42.25) | |
| High | 5.35 (4.8–5.61) | 3.09 (2.74–3.41) | 1.42 (1.27–1.58) | 0.96 (0.79–1.35) | 0.57 (0.53–0.73) | 11.12 (3.86–24.42) | |
| p-value | 0.078 | 0.239 | 0.302 | 0.017 | 0.407 | 0.846 | |
| Physical activity | No | 5.68 (5.09–6.31) | 3.40 (2.79–4.04) | 1.53 (1.27–1.87) | 1.24 (0.93–1.56) | 0.65 (0.53–0.80) | 8.42 (3.55–44.70) |
| Yes | 5.42 (4.68–6.22) | 3.09 (2.46–3.94) | 1.43 (1.23–1.76) | 1.10 (0.88–1.51) | 0.58 (0.53–0.76) | 9.57 (3.66–39.13) | |
| p-value | 0.165 | 0.120 | 0.082 | 0.374 | 0.242 | 0.995 | |
| Smoking status | Non-smoker | 5.51 (4.88–6.26) | 3.16 (2.65–3.93) | 1.50 (1.26–1.82) | 1.20 (0.87–1.53) | 0.63 (0.52–0.78) | 9.80 (3.60–41.60) |
| Active smoker | 6.03 (5.28–6.22) | 3.50 (2.75–4.19) | 1.51 (1.24–1.81) | 1.28 (1.04–1.69) | 0.67 (0.58–0.78) | 7.03 (3.26–47.15) | |
| p-value | 0.151 | 0.234 | 0.855 | 0.083 | 0.256 | 0.825 | |
| Lipid-lowering treatment | No | 5.57 (4.98–6.22) | 3.30 (2.75–3.90) | 1.50 (1.31–1.83) | 1.12 (0.85–1.51) | 0.63 (0.51–0.75) | 6.24 (3.12–33.21) |
| Yes | 5.54 (4.84–6.41) | 3.14 (2.38–4.19) | 1.46 (1.21–1.77) | 1.30 (0.96–1.60) | 0.66 (0.53–0.81) | 14.04 (4.31–50.67) | |
| p-value | 0.758 | 0.613 | 0.162 | 0.073 | 0.247 | 0.007 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratajczak, J.; Kubica, A.; Michalski, P.; Pietrzykowski, Ł.; Białczyk, A.; Kosobucka-Ozdoba, A.; Bergmann, K.; Buczkowski, K.; Krintus, M.; Jankowski, P.; et al. Determinants of Lipid Parameters in Patients without Diagnosed Cardiovascular Disease—Results of the Polish Arm of the EUROASPIRE V Survey. J. Clin. Med. 2023, 12, 2738. https://doi.org/10.3390/jcm12072738
Ratajczak J, Kubica A, Michalski P, Pietrzykowski Ł, Białczyk A, Kosobucka-Ozdoba A, Bergmann K, Buczkowski K, Krintus M, Jankowski P, et al. Determinants of Lipid Parameters in Patients without Diagnosed Cardiovascular Disease—Results of the Polish Arm of the EUROASPIRE V Survey. Journal of Clinical Medicine. 2023; 12(7):2738. https://doi.org/10.3390/jcm12072738
Chicago/Turabian StyleRatajczak, Jakub, Aldona Kubica, Piotr Michalski, Łukasz Pietrzykowski, Aleksandra Białczyk, Agata Kosobucka-Ozdoba, Katarzyna Bergmann, Krzysztof Buczkowski, Magdalena Krintus, Piotr Jankowski, and et al. 2023. "Determinants of Lipid Parameters in Patients without Diagnosed Cardiovascular Disease—Results of the Polish Arm of the EUROASPIRE V Survey" Journal of Clinical Medicine 12, no. 7: 2738. https://doi.org/10.3390/jcm12072738