
Guided Growth for the Treatment of Cubitus Varus in Children: Medium- to Long-Term Results
 ,
,
Abstract
:1. Introduction
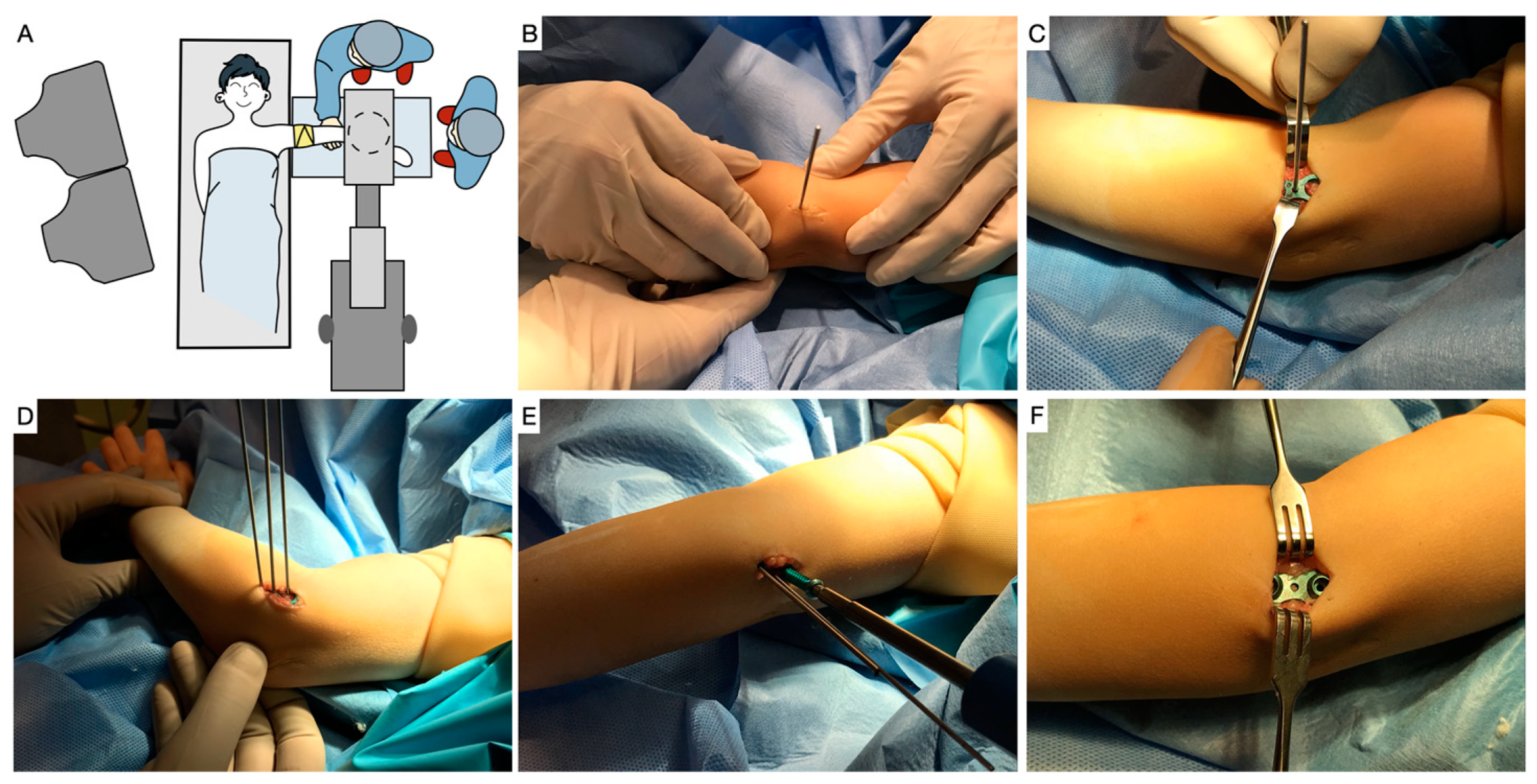
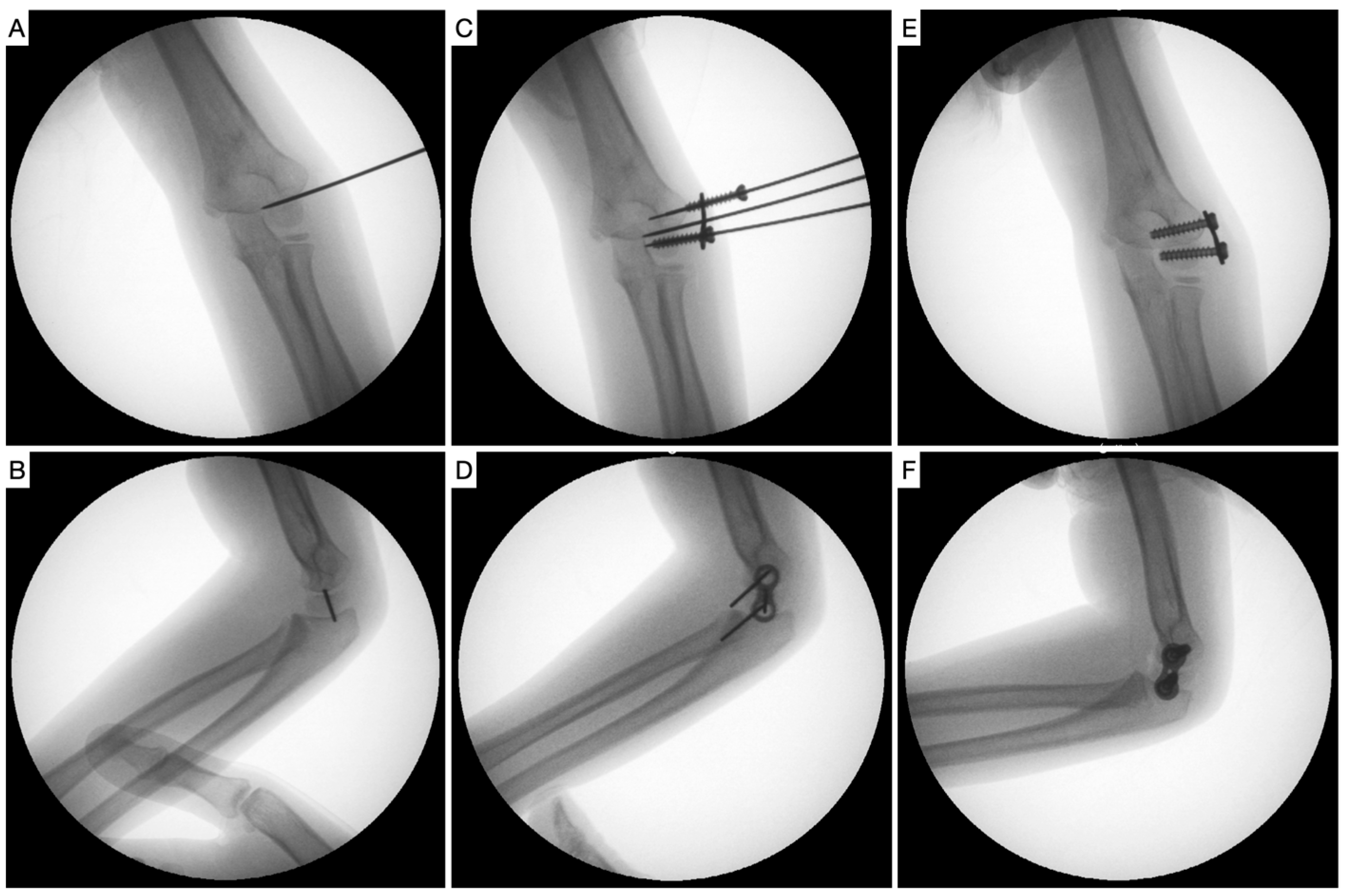
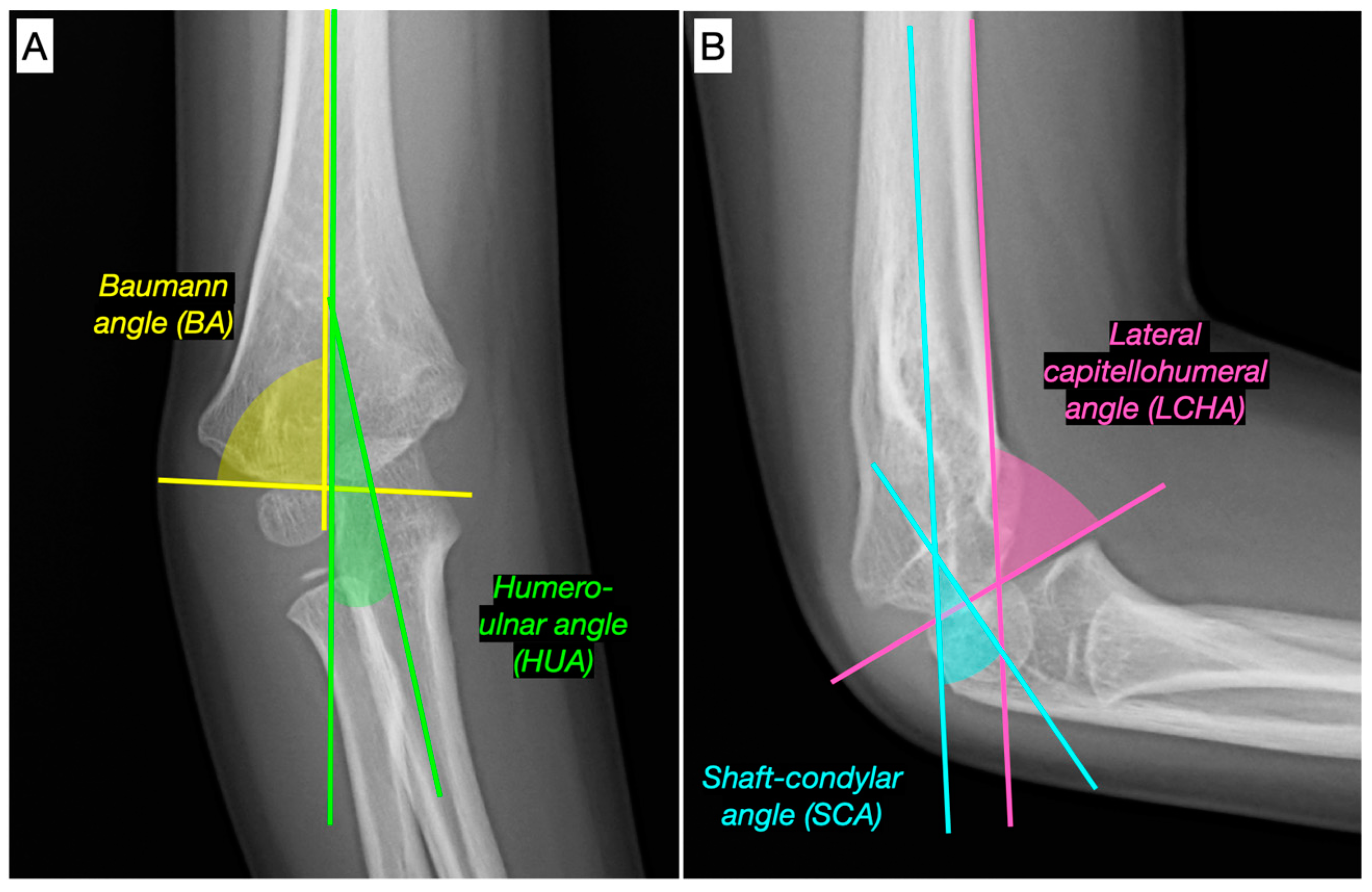
2. Materials and Methods
3. Results
3.1. Descriptive Analysis
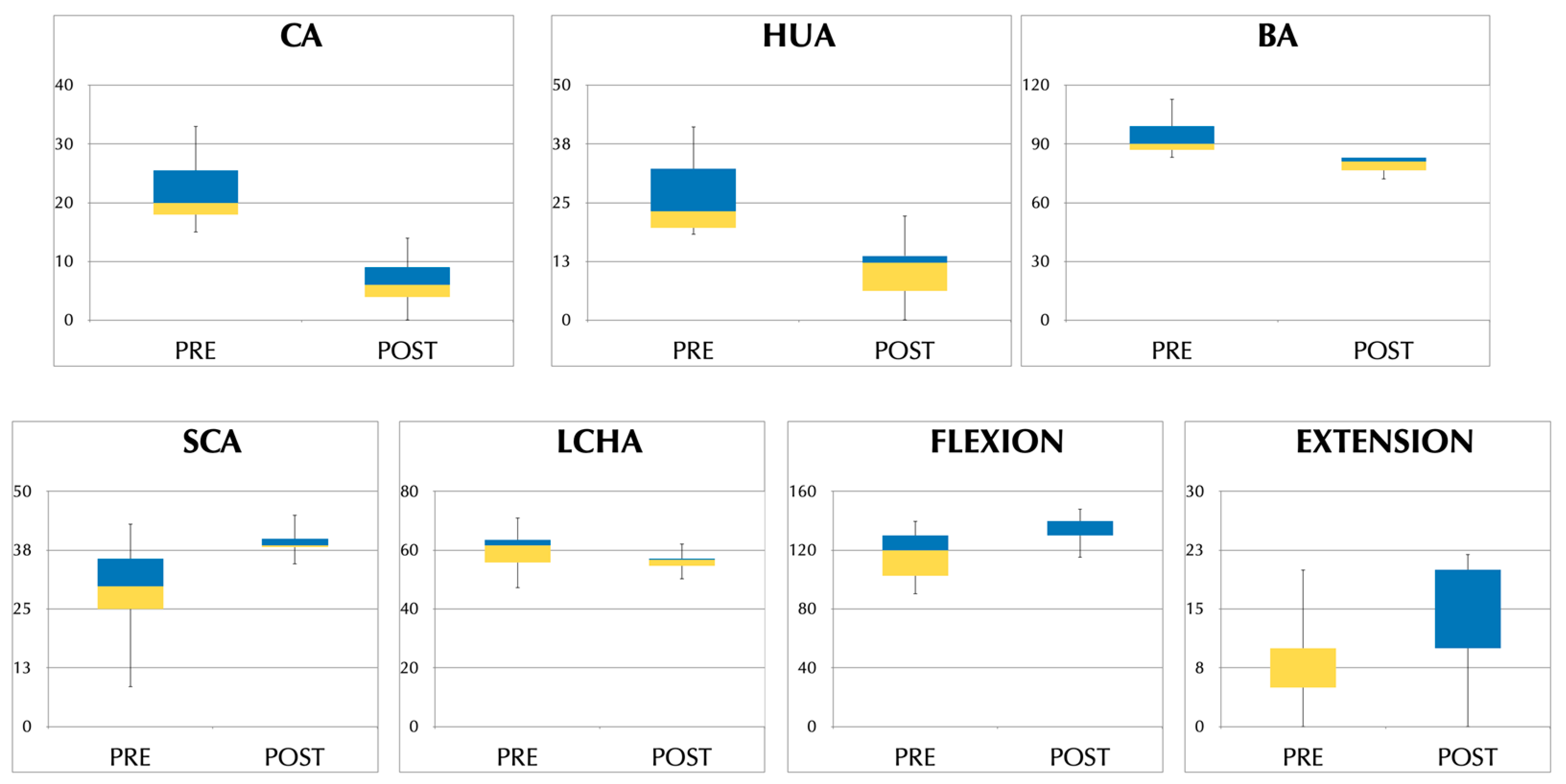
3.2. Comparative Pre- vs. Post-Analysis
3.3. Correlation Analysis
3.4. Complications
3.5. Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miyamura, S.; Oka, K.; Abe, S.; Shigi, A.; Tanaka, H.; Sugamoto, K.; Yoshikawa, H.; Murase, T. Altered bone density and stress distribution patterns in long-standing cubitus varus deformity and their effect during early osteoarthritis of the elbow. Osteoarthr. Cartil. 2018, 26, 72–83. [Google Scholar] [CrossRef] [Green Version]
- Fujioka, H.; Nakabayashi, Y.; Hirata, S.; Go, G.; Nish, S.; Mizuno, K. Analysis of Tardy Ulnar Nerve Palsy Associated with Cubitus Varus Deformity After a Supracondylar Fracture of the Humerus: A report of four cases. J. Orthop. Trauma 1995, 9, 435–440. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Spinner, R.J.; McKee, M.D.; Ben Kibler, W.; Hastings, H.; Morrey, B.F.; Kato, H.; Takayama, S.; Imatani, J.; Toh, S.; et al. Tardy Posterolateral Rotatory Instability of the Elbow due to Cubitus Varus. J. Bone Jt. Surg. 2001, 83, 1358–1369. [Google Scholar] [CrossRef] [PubMed]
- Spinner, R.J.; O’Driscoll, S.; Davids, J.R.; Goldner, R.D. Cubitus Varus Associated with Dislocation of Both the Medial Portion of the Triceps and the Ulnar Nerve. J. Hand Surg. 1999, 24, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.A. Cubitus Varus—It’s More Than Just a Crooked Arm! J. Pediatr. Orthop. 2017, 37 (Suppl. S2), S37–S41. [Google Scholar] [CrossRef]
- Solfelt, D.A.; Hill, B.W.; Anderson, C.P.; Cole, P.A. Supracondylar osteotomy for the treatment of cubitus varus in children: A systematic review. Bone Jt. J. 2014, 96-B, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.S.; Pham, B.; Lattanza, L.L. Surgical Correction of Cubitus Varus. J. Hand Surg. AM. 2016, 41, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Liddell, T.R.; Hennrikus, W.L.; Bresnahan, J.J. A Simple Dual-Planar Osteotomy to Correct Cubitus Varus Deformity in Children. J. Orthop. Trauma 2016, 30, e340–e345. [Google Scholar] [CrossRef]
- Kumar, R.; Rangasamy, K.; Gopinathan, N.R.; Sudesh, P.; Goni, V.G. Is modified reverse step-cut osteotomy better than Yun’s reverse V osteotomy in paediatric cubitus varus deformity correction? A prospective, double-blinded, randomized controlled trial. Int. Orthop. 2022, 46, 2041–2053. [Google Scholar] [CrossRef]
- Raney, E.M.; Thielen, Z.; Gregory, S.; Sobralske, M. Complications of Supracondylar Osteotomies for Cubitus Varus. J. Pediatr. Orthop. 2012, 32, 232–240. [Google Scholar] [CrossRef]
- Murase, T.; Takeyasu, Y.; Oka, K.; Kataoka, T.; Tanaka, H.; Yoshikawa, H. Three-Dimensional Corrective Osteotomy for Cubitus Varus Deformity with Use of Custom-Made Surgical Guides. JBJS Essent. Surg. Tech. 2014, 4, e6. [Google Scholar] [CrossRef]
- Omori, S.; Murase, T.; Oka, K.; Kawanishi, Y.; Oura, K.; Tanaka, H.; Yoshikawa, H. Postoperative accuracy analysis of three-dimensional corrective osteotomy for cubitus varus deformity with a custom-made surgical guide based on computer simulation. J. Shoulder Elb. Surg. 2014, 24, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Zhong, M.; Lou, Y.; Xu, P.; Jiang, B.; Mao, F.; Chen, D.; Zheng, P. Clinical application of individualized 3D-printed navigation template to children with cubitus varus deformity. J. Orthop. Surg. Res. 2020, 15, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Wang, J.; Rai, S.; Ze, R.; Hong, P.; Wang, S.; Tang, X. 3D-printed model and osteotomy template technique compared with conventional closing-wedge osteotomy in cubitus varus deformity. Sci. Rep. 2022, 12, 6762. [Google Scholar] [CrossRef] [PubMed]
- Burghardt, R.D.; Herzenberg, J.E. Temporary hemiepiphysiodesis with the eight-Plate for angular deformities: Mid-term results. J. Orthop. Sci. 2010, 15, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Almahmudi, A.; Alshehri, D.; Assaggaf, H. Lateral Condyle Hemiepiphysiodesis in Treatment of Cubits Varus Deformity Post Supracondylar Humours Fracture: A Case Report. Med. Case Rep. 2020, 6, 150. [Google Scholar] [CrossRef]
- Verka, P.S. A novel minimally invasive method in pediatric cubitus varus deformity, distal lateral humerus hemiepiphysiodesis: A case report. J. Pediatr. Neurol. Disord. 2021, 4, 1–2. [Google Scholar]
- Soldado, F.; Diaz-Gallardo, P.; Cherqaoui, A.; Nguyen, T.-Q.; Romero-Larrauri, P.; Knorr, J. Unsuccessful mid-term results for distal humeral hemiepiphysiodesis to treat cubitus varus deformity in young children. J. Pediatr. Orthop. B 2022, 31, 431–433. [Google Scholar] [CrossRef]
- Sink, E.L.; Leunig, M.; Zaltz, I.; Gilbert, J.C.; Clohisy, J.; Academic Network for Conservational Hip Outcomes Research Group. Reliability of a Complication Classification System for Orthopaedic Surgery. Clin. Orthop. Relat. Res. 2012, 470, 2220–2226. [Google Scholar] [CrossRef] [Green Version]
- Kumar, B.; Pai, S.; Ray, B.; Mishra, S.; Siddaraju, K.S.; Pandey, A.K.; Binu, S. Radiographic study of carrying angle and morphometry of skeletal elements of human elbow. Rom. J. Morphol. Embryol. 2010, 51, 521–526. [Google Scholar]
- Kang, S.; Park, S.-S. Predisposing Effect of Elbow Alignment on the Elbow Fracture Type in Children. J. Orthop. Trauma 2015, 29, e253–e258. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, C.A.; Patterson, J.M.M.; Sutter, M.; Krauss, M.; Steffen, J.A.; Galatz, L. Elbow radiographic anatomy: Measurement techniques and normative data. J. Shoulder Elb. Surg. 2012, 21, 1236–1246. [Google Scholar] [CrossRef] [Green Version]
- Beaty, J.H.; Kasser, J.R. Evaluation of pediatric distal humeral fractures. In Rockwood and Wilkins’ Fractures in Children, 8th ed.; Flynn, J.M., Skaggs, D.L., Waters, P.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015; pp. 565–579. [Google Scholar]
- Shank, C.F.; Wiater, B.P.; Pace, J.L.; Lee, J.; Thomas, J.; Schmale, G.; Bittner, G.; Bompadre, V.; Stults, J.; Krengel, W. The lateral capitellohumeral angle in normal children: Mean, variation, and reliability in comparison to Baumann’s angle. J. Pediatr. Orthop. 2011, 31, e266–e271. [Google Scholar] [CrossRef] [PubMed]
- Kasser, J.R.; Beaty, J.H. The Elbow Region: General Concepts in the Pediatric Patient. In Rockwood & Wilkins’ Fractures in Children; Beaty, J.H., Kasser, J.R., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 529–541. [Google Scholar]
- Métaizeau, J.-P.; Wong-Chung, J.; Bertrand, H.; Pasquier, P. Percutaneous Epiphysiodesis Using Transphyseal Screws (PETS). J. Pediatr. Orthop. 1998, 18, 363–369. [Google Scholar] [CrossRef]
- Stahl, E.J.; Karpman, R. Normal growth and growth predictions in the upper extremity. J. Hand Surg. 1986, 11, 593–596. [Google Scholar] [CrossRef]
- Pritchett, J.W. Growth plate activity in the upper extremity. Clin. Orthop. Relat. Res. 1991, 268, 235–242. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRE | POST | Difference | p Value | |
|---|---|---|---|---|
| CA | −20 (−18 to −26) | −6 (−4 to −9) | −16 (−18 to −9) | <0.001 |
| HUA | −19 (−15 to −29) | −8 (−1 to −10) | −16 (−19 to −12) | <0.001 |
| BA | 90 (87 to 100) | 81 (76 to 83) | −11 (−17 to −7) | <0.001 |
| SCA | 29.8 (24.3 to 36.2) | 38.5 (38.1 to 40) | 7.5 (3.3 to 13.8) | <0.001 |
| LCHA | 61.6 (54 to 64.1) | 56.7 (54.6 to 57.3) | −4.8 (−6.8 to 0.6) | 0.018 |
| Flexion | 120 (100 to 130) | 130 (130 to 140) | 10 (0 to 24) | 0.006 |
| Extension | 0 (−10 to 0) | 0 (o to 10) | 10 (0 to 10) | 0.013 |
| Satisfied | Unsatisfied | p Value | |
|---|---|---|---|
| Age | 4.93 (3.9 to 6.7) | 9.00 (7.9 to 10.1) | 0.037 |
| Implant duration | 72.17 (61.3 to 93.3) | 76.45 (63.5 to 89.4) | 0.466 |
| Initial clinical CA | 21 (17.5 to 28) | 19 (18 to 20) | 0.304 |
| Initial HUA | 19 (15 to 30) | 19 (18 to 20) | 0.5 |
| CA correction | −16 (−19 to −10) | −12 (−16 to −8) | 0.248 |
| HUA correction | −16 (−19.1 to −12) | −12 (−15 to −9) | 0.196 |
| Study | N | Mean Age (y) | Previous Fracture | Pre HUA | Technique | Post HUA | FU (m) |
|---|---|---|---|---|---|---|---|
| Almahmudi 2020 [16] | 1 | 10 | SHF | −3° | Eight-Plate and screws | +6° | 12 |
| Verka 2021 [17] | 1 | 5.67 | SHF | −22.4° | Eight-Plate and screws | NR | 18 |
| Soldado 2022 [18] | 5 | 3.58 (2.5 to 4.42) | NR | −22.5° (−15 to −30) * | Medial oblique cannulated screw | −21° (−15 to −30) * | 46 |
| Current study 2023 | 15 | 5.1 years (4 to 7.1) | 12 SHF, 1 CHF, 2 multiple | −19 (−15 to −29) | Eight-Plate and screws | −8 (−1 to −10) | 81 (64 to 103) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Álvarez, S.; Galán-Olleros, M.; Alonso-Hernández, J.; Vara-Patudo, I.; Miranda-Gorozarri, C.; Palazón-Quevedo, Á. Guided Growth for the Treatment of Cubitus Varus in Children: Medium- to Long-Term Results. J. Clin. Med. 2023, 12, 2632. https://doi.org/10.3390/jcm12072632
Martínez-Álvarez S, Galán-Olleros M, Alonso-Hernández J, Vara-Patudo I, Miranda-Gorozarri C, Palazón-Quevedo Á. Guided Growth for the Treatment of Cubitus Varus in Children: Medium- to Long-Term Results. Journal of Clinical Medicine. 2023; 12(7):2632. https://doi.org/10.3390/jcm12072632
Chicago/Turabian StyleMartínez-Álvarez, Sergio, María Galán-Olleros, Javier Alonso-Hernández, Isabel Vara-Patudo, Carlos Miranda-Gorozarri, and Ángel Palazón-Quevedo. 2023. "Guided Growth for the Treatment of Cubitus Varus in Children: Medium- to Long-Term Results" Journal of Clinical Medicine 12, no. 7: 2632. https://doi.org/10.3390/jcm12072632