
Conservative and Surgical Treatment of Osteochondromas in Children, Particularly with or without Surgical Lengthening of the Ulna
 and
and
Abstract
:1. Introduction
2. Materials and Methods
- (C) Conservative therapy,
- (E) Simple excision procedure,
- (L) Excision and lengthening.
3. Results
3.1. Demographics
3.2. Functional and Cosmetic Outcome
3.3. Radiographic Evaluation
3.3.1. Relative Shortening
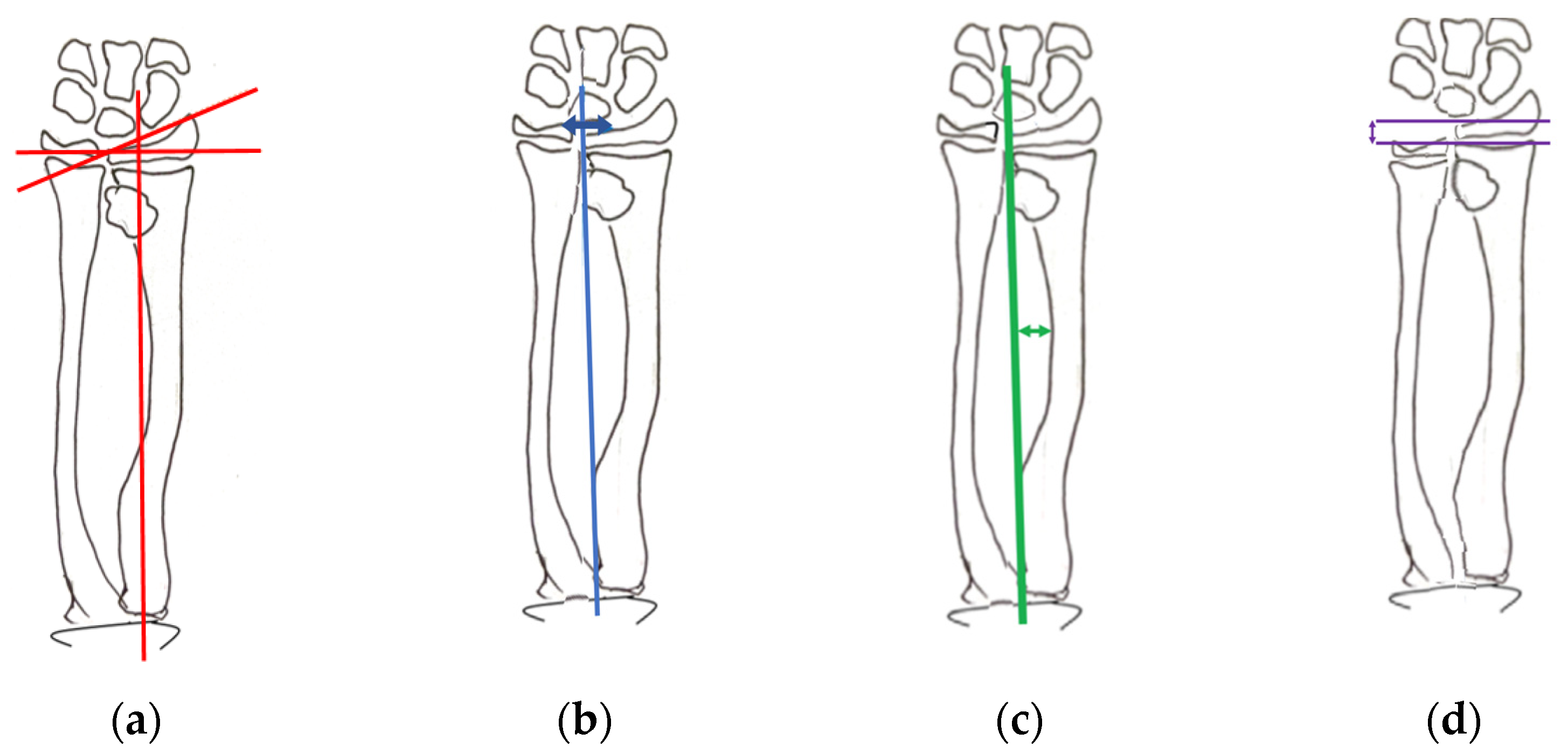
3.3.2. Radial Articular Angle
3.3.3. Carpal Slip
3.3.4. Radial Bowing
3.3.5. Lengthening
3.4. Complications of the Excision with Bone Lengthening Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, E.K.; Jones, N.F.; Lawrence, J.F. Treatment of multiple hereditary osteochondromas of the forearm in children: A study of surgical procedures. J. Bone Jt. Surg. Br. Vol. 2006, 88, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Masada, K.; Tsuyuguchi, Y.; Kawai, H.; Kawabata, H.; Noguchi, K.; Ono, K. Operations for forearm deformity caused by multiple osteochondromas. J. Bone Jt. Surg. Br. Vol. 1989, 71, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Vogt, B.; Tretow, H.L.; Daniilidis, K.; Wacker, S.; Buller, T.C.; Henrichs, M.P.; Roedl, R.W.; Schiedel, F. Reconstruction of forearm deformity by distraction osteogenesis in children with relative shortening of the ulna due to multiple cartilaginous exostosis. J. Pediatr. Orthop. 2011, 31, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Bilen, F.E.; Eralp, L.; Balci, H.I.; Kocaoglu, M.; Ozger, H. Correction of forearm deformities in children with multiple osteochondroma, by corrective radial osteotomy and ulnar lengthening by distraction osteogenesis. Acta Orthop. Belg. 2009, 75, 743–747. [Google Scholar] [PubMed]
- Matsubara, H.; Tsuchiya, H.; Sakurakichi, K.; Yamashiro, T.; Watanabe, K.; Tomita, K. Correction and lengthening for deformities of the forearm in multiple cartilaginous exostoses. J. Orthop. Sci. 2006, 11, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akita, S.; Murase, T.; Yonenobu, K.; Shimada, K.; Masada, K.; Yoshikawa, H. Long-Term Results of Surgery for Forearm Deformities in Patients with Multiple Cartilaginous Exostoses. J. Bone Jt. Surg. Am. 2007, 89, 1993–1999. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, S.; van der Zwan, A.L.; Kommol, E.; EPOS Upper Limb Study Group and Collaborators. Reliability of the Masada and Jo classifications for multiple hereditary exostoses in the forearm. J. Hand Surg. Eur. Vol. 2021, 46, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Peterson, H.A. Deformities and problems of the forearm in children with multiple hereditary osteochondromata. J. Pediatr. Orthop. 1994, 14, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.; Pejin, Z.; Salon, A.; Finidori, G.; Glorion, C.; Pannier, S. Radial osteotomy for the correction of forearm deformities in hereditary multiple osteochondroma. Hand Surg. Rehabil. 2020, 39, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Fogel, G.R.; McElfresh, E.C.; Peterson, H.A.; Wicklund, P.T. Management of deformities of the forearm in multiple hereditary osteochondromas. J. Bone Jt. Surg. Am. 1984, 66, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Ip, D.; Li, Y.H.; Chow, W.; Leong, J.C. Reconstruction of forearm deformities in multiple cartilaginous exostoses. J. Pediatr. Orthop. B 2003, 12, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Komura, S.; Matsumoto, K.; Hirakawa, A.; Akiyama, H. Natural History and Characteristics of Hand Exostoses in Multiple Hereditary Exostoses. J. Hand Surg. Am. 2021, 46, 815.e1–815.e12. [Google Scholar] [CrossRef] [PubMed]
- Noonan, K.J.; Levenda, A.; Snead, J.; Feinberg, J.R.; Mih, A. Evaluation of the forearm in untreated adult subjects with multiple hereditary osteochondromatosis. J. Bone Jt. Surg. Am. 2002, 84, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Bader, B.; Grill, F. Ulnar lengthening in osteochondroma (multiple cartilagenous exostoses) of the forearm. Handchir. Mikrochir. Plast. Chir. 2000, 32, 321–327. [Google Scholar] [CrossRef]
- Dahl, M.T. The gradual correction of forearm deformities in multiple hereditary exostoses. Hand Clin. 1993, 9, 707–718. [Google Scholar] [CrossRef]
- Pritchett, J.W. Lengthening the ulna in patients with hereditary multiple exostoses. J. Bone Jt. Surg. Br. Vol. 1986, 68, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, J.I.; Kato, H.; Fujioka, F.; Iwasaki, N.; Suenaga, N.; Minami, A. Tumor location affects the results of simple excision for multiple osteochondromas in the forearm. J. Bone Jt. Surg. Am. 2007, 89, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
- Jo, A.R.; Jung, S.T.; Kim, M.S.; Oh, C.S.; Min, B.J. An Evaluation of Forearm Deformities in Hereditary Multiple Exostoses: Factors Associated with Radial Head Dislocation and Comprehensive Classification. J. Hand Surg. 2017, 42, 292-e1. [Google Scholar] [CrossRef] [PubMed]
- Belyea, C.; Pulos, N.; Ezaki, M.; Wall, L.; Mills, J.; Beckwith, T.; Oishi, S.N. Effect of Distal Ulna Osteochondroma Excision and Distal Ulnar Tether Release on Forearm Deformity in Preadolescent Patients with Multiple Hereditary Exostosis. J. Pediatr. Orthop. 2020, 40, e222–e226. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 15 Patients (17 Forearms) | |||
|---|---|---|---|
| Conservative Therapy | 3 Patients (4 Forearms) | ||
| Surgery | 12 patients (13 forearms) | Simple excision | 4 patients (4 forearms) |
| Excision with lengthening of the ulna | 8 patients (9 forearms) | ||
| Additional corrective osteotomy of radius or ulna | 7 forearms | ||
| Relative Shortening (mm) | Bone Lengthening (mm) | ||
|---|---|---|---|
| Excision with lengthening | 10 | 6 | |
| 13 | 8 | ||
| 2 | 11 | ||
| 13 | 31 | ||
| 15 | 6 | ||
| 10 | 16 | ||
| 14 | 15 | ||
| Mean | 11.6 | 13.3 | |
| Median | 13 | 11 | |
| SD | 4.3 | 8.8 | |
| Therapy/Measurements | Radial Articular Angle (°) | Carpal Slip (%) | Radial Bowing (mm) | ||||
|---|---|---|---|---|---|---|---|
| Conservative | beginning | end | beginning | end | beginning | end | |
| 27 | 37 | 49.1 | 50.9 | 13.5 | 15.6 | ||
| 33 | 38 | 50.8 | 51.3 | 13.4 | 14.8 | ||
| 40 | 44 | 34 | 37 | 13.7 | 14 | ||
| 48 | 44 | 53.6 | 69.3 | 18.7 | 16.7 | ||
| Mean | 37 | 41 | 46.9 | 52.1 | 14.9 | 15.3 | |
| Median | 36.5 | 41 | 50 | 51 | 14 | 15.5 | |
| SD | 8.9 | 4 | 8.8 | 13.2 | 2.6 | 1.2 | |
| Simple exostoses excision | preoperative | postoperative | preoperative | postoperative | preoperative | postoperative | |
| 17 | 18 | 43.7 | 39.7 | 16.3 | 17.7 | ||
| * | 32 | * | 26.1 | * | 12.2 | ||
| * | 30 | * | 57.6 | * | 9.4 | ||
| 53 | 51 | * | * | 24.7 | 25.8 | ||
| * | 37 | 39.8 | 51.7 | * | 20.4 | ||
| 45 | 36 | 49.9 | 41.2 | 11.2 | 14.1 | ||
| 41 | 36 | 56.6 | 23 | 12.3 | 14.2 | ||
| 38 | 36 | 54.7 | 32 | 15.2 | 18.9 | ||
| Mean | 34 | 33 | 45.1 | 41.1 | 14 | 16.3 | |
| Median | 33.5 | 31 | 44 | 40 | 12 | 15 | |
| SD | 14.5 | 13.8 | 15.3 | 15.8 | 8.3 | 7.2 | |
| Excision with lengthening | 38 | 35 | 38 | 50.5 | 8.1 | 8.7 | |
| 44 | 49 | 38.5 | 32.6 | 14 | 19.2 | ||
| 39 | 35 | * | 30.3 | 12.1 | * | ||
| * | 31 | * | 42.8 | * | * | ||
| * | 32 | * | 51.7 | * | * | ||
| Mean | 39 | 35 | 47.7 | 38 | 6.8 | 7 | |
| Median | 38.5 | 35.5 | 48 | 35 | 7 | 7 | |
| SD | 5.3 | 6.4 | 11.9 | 10.2 | 1.3 | 1.7 | |
| Clavien/Dindo Classification | Complications | Number of Forearms |
|---|---|---|
| Grade I | Pin tract infections | 3 |
| Grade IIIb | Incongruence of the elbow joint due to radial head dislocation | 1 |
| Grade IIIb | Radial bowing due to ulna lengthening | 1 |
| Grade IIIb | Angulation in the osteotomy region | 1 |
| Grade IIIb | Dislocation of the external fixator caused by a fall on the forearm, resulting in ulna bowing | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercier, J.; Bernasconi, R.; Steiger, C.; Kaempfen, A.; Krieg, A.H. Conservative and Surgical Treatment of Osteochondromas in Children, Particularly with or without Surgical Lengthening of the Ulna. J. Clin. Med. 2023, 12, 4273. https://doi.org/10.3390/jcm12134273
Mercier J, Bernasconi R, Steiger C, Kaempfen A, Krieg AH. Conservative and Surgical Treatment of Osteochondromas in Children, Particularly with or without Surgical Lengthening of the Ulna. Journal of Clinical Medicine. 2023; 12(13):4273. https://doi.org/10.3390/jcm12134273
Chicago/Turabian StyleMercier, Julie, Reto Bernasconi, Christina Steiger, Alexandre Kaempfen, and Andreas H. Krieg. 2023. "Conservative and Surgical Treatment of Osteochondromas in Children, Particularly with or without Surgical Lengthening of the Ulna" Journal of Clinical Medicine 12, no. 13: 4273. https://doi.org/10.3390/jcm12134273