
EASIX Is an Accurate and Easily Available Prognostic Score in Critically Ill Patients with Advanced Liver Disease


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Evaluation of Clinical Scores
2.3. Analyses Regarding Presence of Infection
2.4. Collection of Data
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
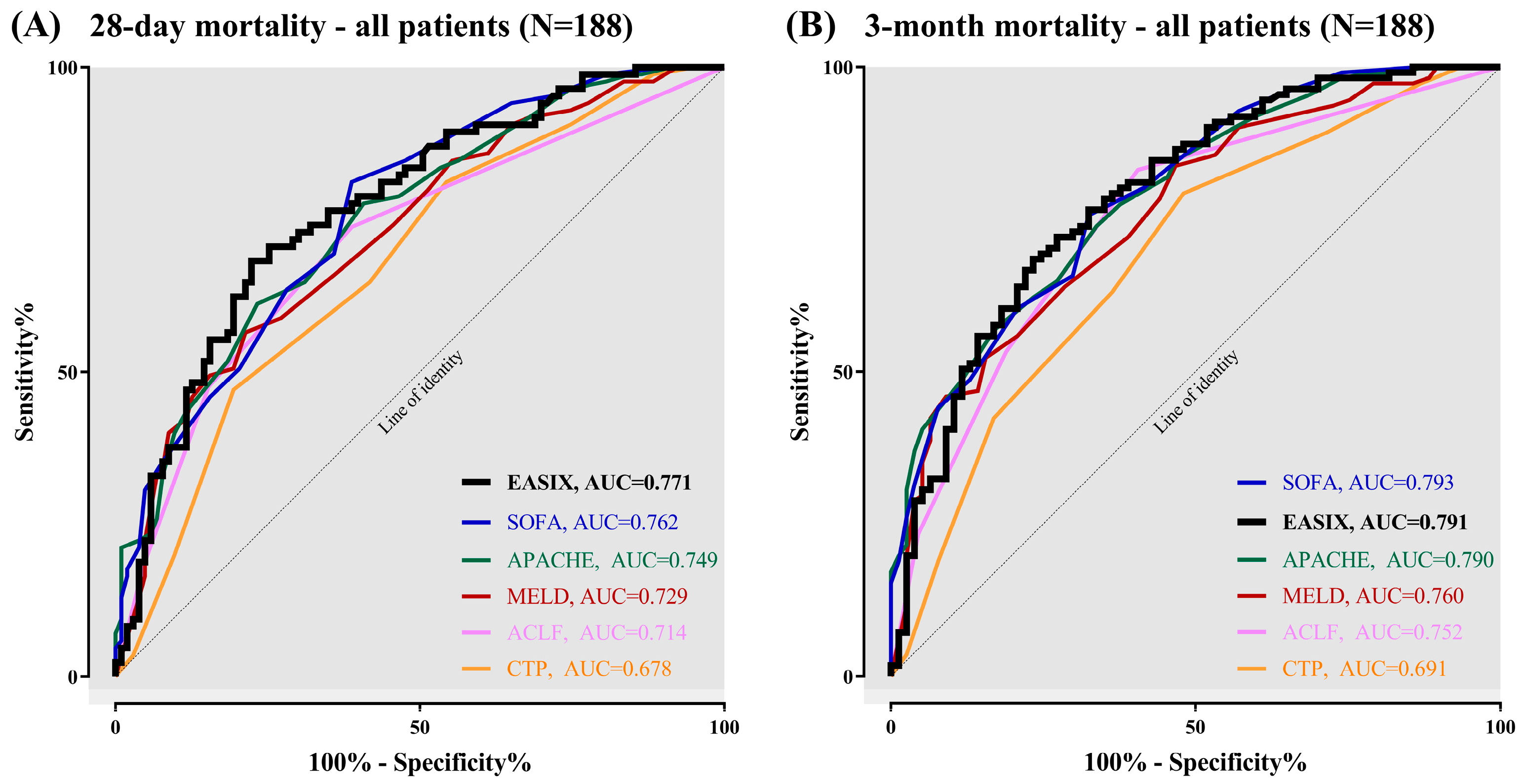
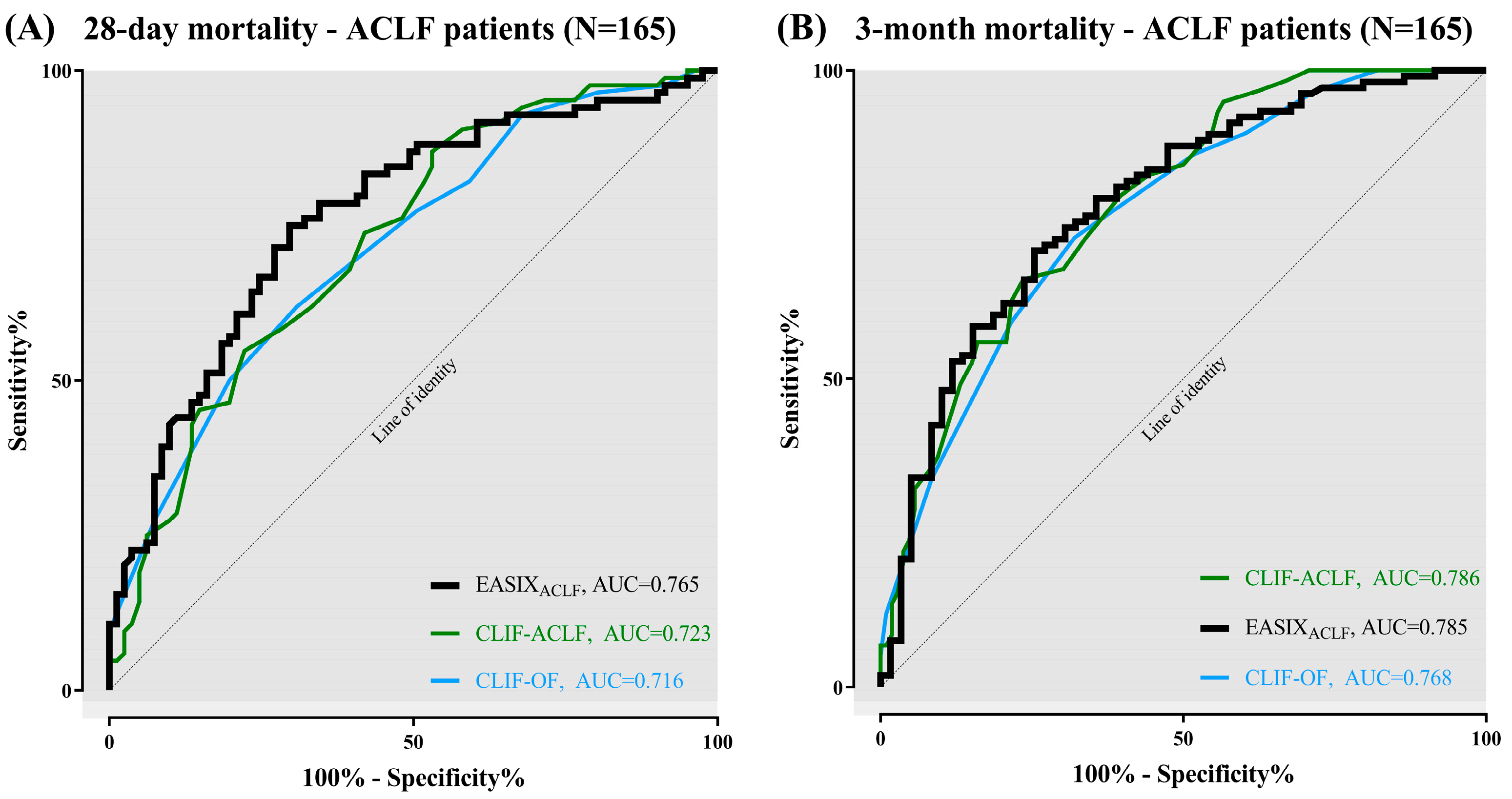
3.2. Prognostic Ability of EASIX
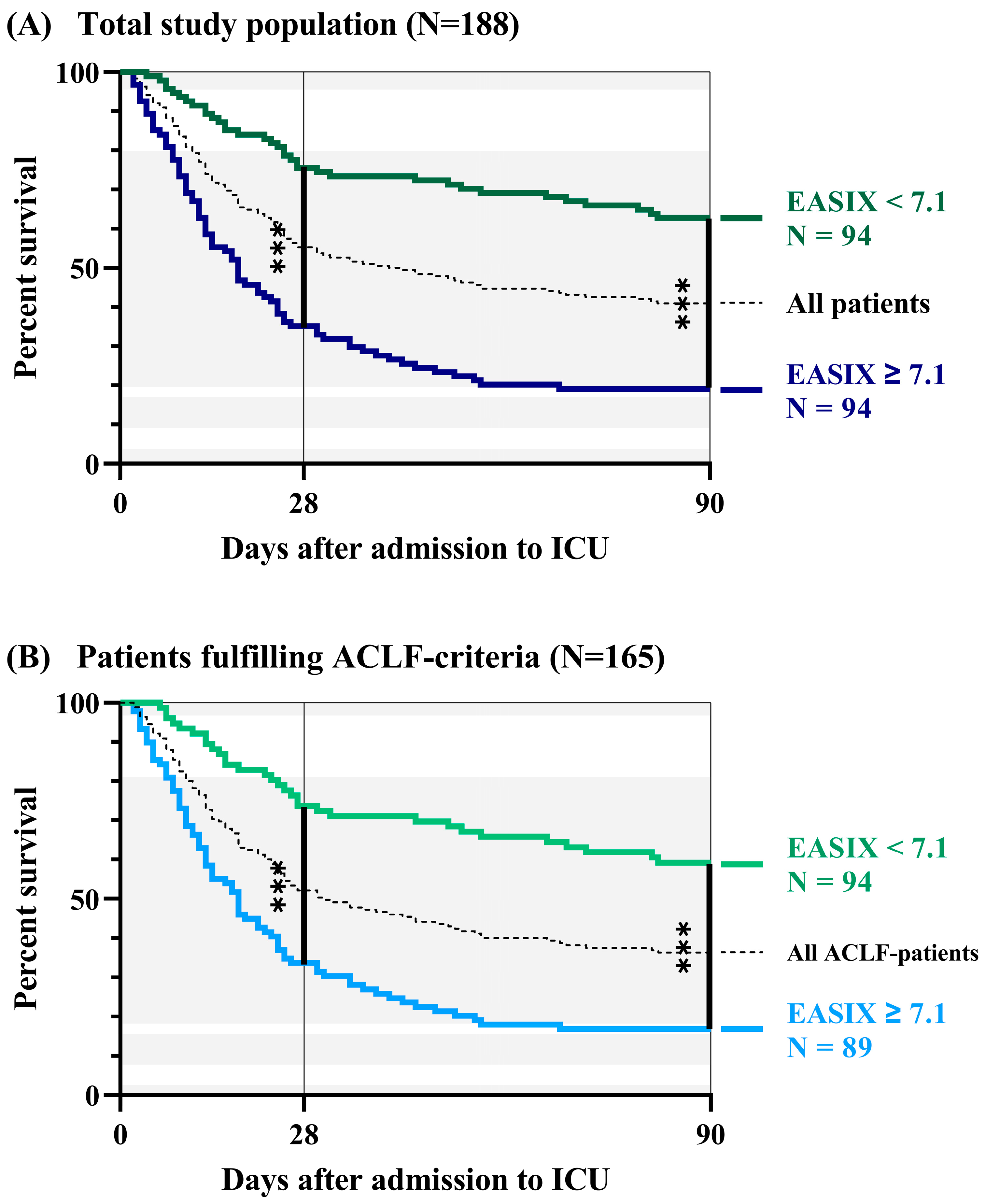
3.3. Survival Analyses Based on Baseline EASIX
3.4. Diagnostic Potential of EASIX
3.5. Correlation Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACLF | Acute-on-chronic liver failure |
| AlloTPL | Allogeneic stem cell transplantation |
| AUC | Area under curve |
| AKI | Acute kidney injury |
| APACHE-II | Acute and physiology chronic health evaluation II |
| BAL | Broncho-alveolar lavage |
| CRP | C-reactive protein |
| CTP | Child-Turcotte-Pugh |
| CT | Computed tomography |
| CLIF | Chronic liver failure |
| CLIF-OF | CLIF organ failure score |
| CLIF-ACLF | CLIF Acute-on-chronic liver failure score |
| COVID-19 | Coronavirus disease 2019 |
| ED | Endothelial dysfunction |
| EASL | European association for the study of the liver |
| EASIX | Endothelial activation and stress index |
| FiO2 | Fraction of inspired oxygen |
| GvHD | Graft-versus-host disease |
| HE | Hepatic encephalopathy |
| HR | Hazard ratio |
| HRS | Hepatorenal syndrome |
| INR | International normalised ratio |
| IQR | Interquartile range |
| LC | Liver cirrhosis |
| MAP | Mean arterial pressure |
| MELD | Model of end-stage liver disease |
| N | Number of patients |
| NASH | Non-alcoholic fatty liver disease |
| NPV | Negative predictive value |
| NO | Nitric oxide |
| PPV | Positive predictive value |
| PMN | Polymorphonuclear neutrophils |
| PaO2 | Arterial partial pressure of oxygen |
| PCT | Procalcitonin |
| R2 | Linear regression coefficient |
| rs | Spearman’s coefficient |
| ROC | Receiver-operating-characteristic curves |
| SBP | Spontaneous bacterial peritonitis |
| SOFA | Sequential organ failure assessment |
| SEC | Sinusoidal endothelial cells |
| WBC | White blood cell count (per microlitre) |
References
- Levesque, E.; Saliba, F.; Ichai, P.; Samuel, D. Outcome of patients with cirrhosis requiring mechanical ventilation in ICU. J. Hepatol. 2014, 60, 570–578. [Google Scholar] [CrossRef]
- Bernardi, M.; Moreau, R.; Angeli, P.; Schnabl, B.; Arroyo, V. Mechanisms of decompensation and organ failure in cirrhosis: From peripheral arterial vasodilation to systemic inflammation hypothesis. J. Hepatol. 2015, 63, 1272–1284. [Google Scholar] [CrossRef]
- Malbrain, M.L.; Chiumello, D.; Pelosi, P.; Bihari, D.; Innes, R.; Ranieri, V.M.; Del Turco, M.; Wilmer, A.; Brienza, N.; Malcangi, V.; et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: A multiple-center epidemiological study. Crit. Care Med. 2005, 33, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Dong, V.; Karvellas, C.J. Acute-on-chronic liver failure: Objective admission and support criteria in the intensive care unit. JHEP Rep. 2019, 1, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Fernandez, M.; Semela, D.; Bruix, J.; Colle, I.; Pinzani, M.; Bosch, J. Angiogenesis in liver disease. J. Hepatol. 2009, 50, 604–620. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Fernandez, J.; Papp, M.; Caraceni, P.; Laleman, W.; Gambino, C.; Giovo, I.; Uschner, F.E.; Jimenez, C.; Mookerjee, R.; et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J. Hepatol. 2020, 73, 842–854. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, A.L.; Qurashi, M.; Shetty, S. The Role of Sinusoidal Endothelial Cells in the Axis of Inflammation and Cancer within the Liver. Front. Physiol. 2020, 11, 990. [Google Scholar] [CrossRef]
- Shubham, S.; Kumar, D.; Rooge, S.; Maras, J.S.; Maheshwari, D.; Nautiyal, N.; Kumari, R.; Bhat, A.; Kumar, G.; Rastogi, A.; et al. Cellular and functional loss of liver endothelial cells correlates with poor hepatocyte regeneration in acute-on-chronic liver failure. Hepatol. Int. 2019, 13, 777–787. [Google Scholar] [CrossRef]
- Iwakiri, Y.; Groszmann, R.J. Vascular endothelial dysfunction in cirrhosis. J. Hepatol. 2007, 46, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Karaa, A.; Kamoun, W.S.; Xu, H.; Zhang, J.; Clemens, M.G. Differential effects of oxidative stress on hepatic endothelial and Kupffer cell eicosanoid release in response to endothelin-1. Microcirculation 2006, 13, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Morales-Ruiz, M.; Cejudo-Martin, P.; Fernandez-Varo, G.; Tugues, S.; Ros, J.; Angeli, P.; Rivera, F.; Arroyo, V.; Rodes, J.; Sessa, W.C.; et al. Transduction of the liver with activated Akt normalizes portal pressure in cirrhotic rats. Gastroenterology 2003, 125, 522–531. [Google Scholar] [CrossRef]
- Kamoun, W.S.; Karaa, A.; Kresge, N.; Merkel, S.M.; Korneszczuk, K.; Clemens, M.G. LPS inhibits endothelin-1-induced endothelial NOS activation in hepatic sinusoidal cells through a negative feedback involving caveolin-1. Hepatology 2006, 43, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Bolognesi, M.; Di Pascoli, M.; Verardo, A.; Gatta, A. Splanchnic vasodilation and hyperdynamic circulatory syndrome in cirrhosis. World J. Gastroenterol. 2014, 20, 2555–2563. [Google Scholar] [CrossRef] [PubMed]
- Braet, F.; Wisse, E. Structural and functional aspects of liver sinusoidal endothelial cell fenestrae: A review. Comp. Hepatol. 2002, 1, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, H.; Penack, O.; Radujkovic, A.; Schult, D.; Majer-Lauterbach, J.; Blau, I.W.; Bullinger, L.; Jiang, S.; Muller-Tidow, C.; Dreger, P.; et al. Early bilirubinemia after allogeneic stem cell transplantation-an endothelial complication. Bone Marrow Transpl. 2021. [Google Scholar] [CrossRef]
- Luft, T.; Benner, A.; Terzer, T.; Jodele, S.; Dandoy, C.E.; Storb, R.; Kordelas, L.; Beelen, D.; Gooley, T.; Sandmaier, B.M.; et al. EASIX and mortality after allogeneic stem cell transplantation. Bone Marrow Transpl. 2020, 55, 553–561. [Google Scholar] [CrossRef]
- Luft, T.; Benner, A.; Jodele, S.; Dandoy, C.E.; Storb, R.; Gooley, T.; Sandmaier, B.M.; Becker, N.; Radujkovic, A.; Dreger, P.; et al. EASIX in patients with acute graft-versus-host disease: A retrospective cohort analysis. Lancet Haematol. 2017, 4, e414–e423. [Google Scholar] [CrossRef]
- Jiang, S.; Penack, O.; Terzer, T.; Schult, D.; Majer-Lauterbach, J.; Radujkovic, A.; Blau, I.W.; Bullinger, L.; Muller-Tidow, C.; Dreger, P.; et al. Predicting sinusoidal obstruction syndrome after allogeneic stem cell transplantation with the EASIX biomarker panel. Haematologica 2021, 106, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Mayr, U.; Lukas, M.; Elnegouly, M.; Vogt, C.; Bauer, U.; Ulrich, J.; Schmid, R.M.; Huber, W.; Lahmer, T. Ascitic Interleukin 6 Is Associated with Poor Outcome and Spontaneous Bacterial Peritonitis: A Validation in Critically Ill Patients with Decompensated Cirrhosis. J. Clin. Med. 2020, 9, 2865. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; Saliba, F.; Pavesi, M.; Amoros, A.; Moreau, R.; Gines, P.; Levesque, E.; Durand, F.; Angeli, P.; Caraceni, P.; et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. J. Hepatol. 2014, 61, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- American Association for the Study of Liver Diseases; European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merz, A.; Germing, U.; Kobbe, G.; Kaivers, J.; Jauch, A.; Radujkovic, A.; Hummel, M.; Benner, A.; Merz, M.; Dreger, P.; et al. EASIX for prediction of survival in lower-risk myelodysplastic syndromes. Blood Cancer J. 2019, 9, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luft, T.; Wendtner, C.M.; Kosely, F.; Radujkovic, A.; Benner, A.; Korell, F.; Kihm, L.; Bauer, M.F.; Dreger, P.; Merle, U. EASIX for Prediction of Outcome in Hospitalized SARS-CoV-2 Infected Patients. Front. Immunol. 2021, 12, 634416. [Google Scholar] [CrossRef]
- Park, S.; Go, S.I.; Lee, G.W. The Endothelial Activation and Stress Index (EASIX) score is an independent prognostic factor in patients with diffuse large B-cell lymphoma. BMC Cancer 2022, 22, 816. [Google Scholar] [CrossRef]
- Afdhal, N.; McHutchison, J.; Brown, R.; Jacobson, I.; Manns, M.; Poordad, F.; Weksler, B.; Esteban, R. Thrombocytopenia associated with chronic liver disease. J. Hepatol. 2008, 48, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Realdi, G.; Fattovich, G.; Hadziyannis, S.; Schalm, S.W.; Almasio, P.; Sanchez-Tapias, J.; Christensen, E.; Giustina, G.; Noventa, F. Survival and prognostic factors in 366 patients with compensated cirrhosis type B: A multicenter study. The Investigators of the European Concerted Action on Viral Hepatitis (EUROHEP). J. Hepatol. 1994, 21, 656–666. [Google Scholar] [CrossRef]
- Qamar, A.A.; Grace, N.D.; Groszmann, R.J.; Garcia-Tsao, G.; Bosch, J.; Burroughs, A.K.; Ripoll, C.; Maurer, R.; Planas, R.; Escorsell, A.; et al. Incidence, prevalence, and clinical significance of abnormal hematologic indices in compensated cirrhosis. Clin. Gastroenterol. Hepatol. 2009, 7, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Arroyo, V.; Moreau, R.; Kamath, P.S.; Jalan, R.; Gines, P.; Nevens, F.; Fernandez, J.; To, U.; Garcia-Tsao, G.; Schnabl, B. Acute-on-chronic liver failure in cirrhosis. Nat. Rev. Dis. Prim. 2016, 2, 16041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, J.; Xiong, J.; Zhang, Y.; Peng, T.; Huang, M.; Lin, Y.; Guo, Y.; Wu, H.; Wang, C. Serum lactate dehydrogenase is predictive of persistent organ failure in acute pancreatitis. J. Crit. Care 2017, 41, 161–165. [Google Scholar] [CrossRef]
- Lu, J.; Wei, Z.; Jiang, H.; Cheng, L.; Chen, Q.; Chen, M.; Yan, J.; Sun, Z. Lactate dehydrogenase is associated with 28-day mortality in patients with sepsis: A retrospective observational study. J. Surg. Res. 2018, 228, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Ferriero, R.; Nusco, E.; De Cegli, R.; Carissimo, A.; Manco, G.; Brunetti-Pierri, N. Pyruvate dehydrogenase complex and lactate dehydrogenase are targets for therapy of acute liver failure. J. Hepatol. 2018, 69, 325–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duman, A.; Akoz, A.; Kapci, M.; Ture, M.; Orun, S.; Karaman, K.; Turkdogan, K.A. Prognostic value of neglected biomarker in sepsis patients with the old and new criteria: Predictive role of lactate dehydrogenase. Am. J. Emerg. Med. 2016, 34, 2167–2171. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Lu, C.; Pan, N.; Zhang, M.; An, Y.; Xu, M.; Zhang, L.; Guo, Y.; Tan, L. Serum lactate dehydrogenase activities as systems biomarkers for 48 types of human diseases. Sci. Rep. 2021, 11, 12997. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Prado, V.; Trebicka, J.; Amoros, A.; Gustot, T.; Wiest, R.; Deulofeu, C.; Garcia, E.; Acevedo, J.; Fuhrmann, V.; et al. Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe. J. Hepatol. 2019, 70, 398–411. [Google Scholar] [CrossRef] [Green Version]
- Cervoni, J.P.; Thevenot, T.; Weil, D.; Muel, E.; Barbot, O.; Sheppard, F.; Monnet, E.; Di Martino, V. C-reactive protein predicts short-term mortality in patients with cirrhosis. J. Hepatol. 2012, 56, 1299–1304. [Google Scholar] [CrossRef]
- Papp, M.; Vitalis, Z.; Altorjay, I.; Tornai, I.; Udvardy, M.; Harsfalvi, J.; Vida, A.; Kappelmayer, J.; Lakatos, P.L.; Antal-Szalmas, P. Acute phase proteins in the diagnosis and prediction of cirrhosis associated bacterial infections. Liver Int. 2012, 32, 603–611. [Google Scholar] [CrossRef]
- Le Moine, O.; Deviere, J.; Devaster, J.M.; Crusiaux, A.; Durand, F.; Bernuau, J.; Goldman, M.; Benhamou, J.P. Interleukin-6: An early marker of bacterial infection in decompensated cirrhosis. J. Hepatol. 1994, 20, 819–824. [Google Scholar] [CrossRef]
- Pieri, G.; Agarwal, B.; Burroughs, A.K. C-reactive protein and bacterial infection in cirrhosis. Ann. Gastroenterol. 2014, 27, 113–120. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics of the Study Population | |
|---|---|
| Female sex, N/total (%) | 69/188 (37%) |
| Age, years | 59 (51–67) |
| Body weight, kg | 75 (66–85) |
| Body height, cm | 175 (168–180) |
| Body mass index, kg/m2 | 25 (22–27) |
| SOFA | 11 (8–14) |
| APACHE II | 22 (17–27) |
| MELD | 26 (22–32) |
| CTP | 12 (10–13) |
| CTP C, N/total (%) | 154/188 (82%) |
| No ACLF—Grade 0, N/total (%) | 23/188 (22%) |
| ACLF, N/total (%) | 165/188 (88%) |
| ACLF Grade I, N/total (%) | 39/165 (24%) |
| ACLF Grade II, N/total (%) | 47/165 (28%) |
| ACLF Grade III, N/total (%) | 79/165 (48%) |
| CLIF-C OF, N = 188 | 11 (9–14) |
| CLIF-C ACLF, N = 165 | 58 (50–65) |
| CLIF-C AD, N = 23 | 53 (47–59) |
| Etiology of cirrhosis, N/total (%) | Alcoholic 135/188 (72%) |
| Viral 15/188 (8%) | |
| Autoimmune 9/188 (5%) | |
| Cryptogenic/NASH 29/188 (15%) | |
| Diagnoses at admission, N/total (%) | Sepsis/Pneumonia 77/188 (41%) |
| AKI/HRS 41/188 (22%) | |
| Gastrointestinal bleeding 38/188 (20%) | |
| Hepatic encephalopathy 32/188 (17%) | |
| Length of ICU stay, days | 11 (5–19) |
| 28-day mortality, N/total (%) | 85/188 (45%) |
| 3-month mortality, N/total (%) | 111/188 (59%) |
| Clinical cause of death, N/total (%) | Sepsis, Pneumonia 86/111 (77%) |
| Gastrointestinal bleeding 13/111 (12%) | |
| Cardiocirculatory failure 12/111 (11%) | |
| Dialysis during ICU, N/total (%) | 105/188 (56%) |
| LDH, IU/mL | 269 (209–366) |
| Thrombocytes, 109 cells/L | 73 (45–115) |
| Creatinine, mg/dL | 1.9 (1.2–2.9) |
| Bilirubin, mg/dL | 5.2 (2.2–12.6) |
| INR | 1.8 (1.5–2.4) |
| MAP, mmHg | 68 (62–75) |
| Use of vasopressors, N/total (%) | 117/188 (62%) |
| PaO2, mmHg | 86 (74–99) |
| FiO2, % | 30 (30–40) |
| Mechanical ventilation, N/total (%) | 84/188 (45%) |
| HE, N/total (%) | 120/188 (64%) |
| Spearman’s Coefficient rs | Linear Regression R2 | p-Value | |
|---|---|---|---|
| APACHE-II | 0.592 | 0.262 | <0.001 |
| SOFA | 0.625 | 0.262 | <0.001 |
| MELD | 0.593 | 0.200 | <0.001 |
| CTP | 0.438 | 0.093 | <0.001 |
| ACLF Grade I–III | 0.477 | 0.109 | <0.001 |
| CLIF-OF (N = 165) | 0.458 | 0.136 | <0.001 |
| CLIF-ACLF (N = 165) | 0.380 | 0.083 | <0.001 |
| CRP, mg/dL | 0.261 | 0.006 | <0.001 |
| PCT, ng/mL | 0.456 | 0.054 | <0.001 |
| WBC, 109 cells/L | 0.084 | 0.022 | 0.250 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schult, D.; Rasch, S.; Schmid, R.M.; Lahmer, T.; Mayr, U. EASIX Is an Accurate and Easily Available Prognostic Score in Critically Ill Patients with Advanced Liver Disease. J. Clin. Med. 2023, 12, 2553. https://doi.org/10.3390/jcm12072553
Schult D, Rasch S, Schmid RM, Lahmer T, Mayr U. EASIX Is an Accurate and Easily Available Prognostic Score in Critically Ill Patients with Advanced Liver Disease. Journal of Clinical Medicine. 2023; 12(7):2553. https://doi.org/10.3390/jcm12072553
Chicago/Turabian StyleSchult, David, Sebastian Rasch, Roland M. Schmid, Tobias Lahmer, and Ulrich Mayr. 2023. "EASIX Is an Accurate and Easily Available Prognostic Score in Critically Ill Patients with Advanced Liver Disease" Journal of Clinical Medicine 12, no. 7: 2553. https://doi.org/10.3390/jcm12072553