
Dealing with the Persistent Pathogenic Issues of Dry Eye Disease: The Importance of External and Internal Stimuli and Tissue Responses

{kind=link}
Abstract
:1. Introduction
2. Hormesis and Para-Inflammation—An Adaptive Means of Reacting to Stimuli
3. Dry Eye Disease as a Response to Tissue Stress
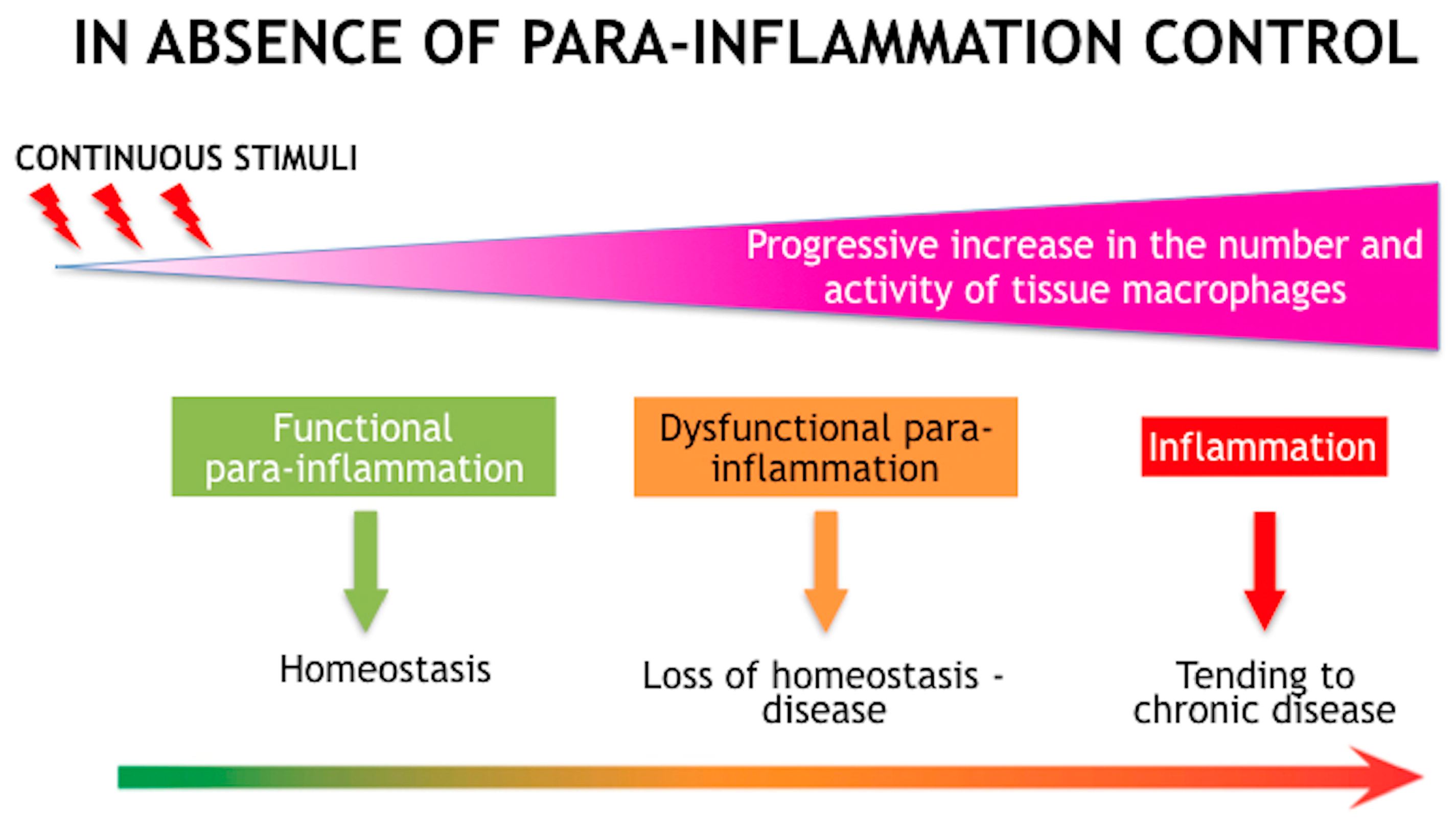
4. Para-Inflammation as an Adaptive Response to Tissue Stress
5. Principles of Treatment
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dogru, M.; Wakamatsu, T.; Kojima, T.; Matsumoto, Y.; Tsubota, K. The role of oxidative stress and inflammation in dry eye disease. Cornea 2009, 28, S70–S74. [Google Scholar] [CrossRef]
- Rolando, M.; Refojo, M.F. Tear evaporimeter for measuring water evaporation rate from the tear film under controlled conditions in humans. Exp. Eye Res. 1983, 36, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Refojo, M.F.; Kenyon, K.R. Increased tear evaporation in eyes with keratoconjunctivitis sicca. Arch. Ophthalmol. 1983, 101, 557–558. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Solomon, A.; Dursun, D.; Li, D.-Q. 2 Dry eye and delayed tear clearance: A call to arms. Adv. Exp. Med. Biol. 2002, 506, 74739–74744. [Google Scholar]
- Rolando, M.; Barabino, S.; Mingari, C.; Moretti, S.; Giuffrida, S.; Calabria, G. Distribution of conjunctival HLA-DR expression and the pathogenesis of damage in early dry eyes. Cornea 2005, 24, 951–954. [Google Scholar] [CrossRef]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 2008, 454, 428–435. [Google Scholar] [CrossRef]
- Chen, M.; Xu, X. Parainflammation, chronic inflammation and age-related macular degeneration. J. Leukoc. Biol. 2015, 98, 713–725. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.H.C.; Ma, J.Y.W.; Jobling, A.I.; Brandli, A.; Greferath, U.; Fletcher, E.L.; Vessey, K.A. Exploring the pathogenesis of age-related macular degeneration: A review of the interplay between retinal pigment epithelium dysfunction and the innate immune system. Front. Neurosci. 2022, 16, 1009599. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Kolko, M.; Melik-Parsadaniantz, S.; Messmer, E.M. Inflammation in Glaucoma: From the back to the front of the eye, and beyond. Prog. Retin. Eye Res. 2021, 83, 100916. [Google Scholar] [CrossRef]
- Martin, O.A.; Redon, C.E.; Dickey, J.S.; Nakamura, A.J.; Bonner, W.M. Para-inflammation mediates systemic DNA damage in response to tumor growth. Commun. Integr. Biol. 2011, 4, 78–81. [Google Scholar] [CrossRef]
- Rolando, M.; Barabino, S. The Subtle Role of Para-inflammation in Modulating the Progression of Dry Eye Disease. Ocul. Immunol. Inflamm. 2021, 18, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Bonini, S.; Labetoulle, M.; Messmer, E.; Aragona, P.; Castillo, J.M.B.; Ciprandi, G.; Damiani, V.; Irkec, M.; Baudouin, C.; Rolando, M. Association of Dry Eye with Laryngopharyngeal Reflux in Clinical Practice. Curr. Eye Res. 2021, 47, 214–219. [Google Scholar] [CrossRef]
- Medzhitov, R. Inflammation 2010: New adventures of an old flame. Cell 2010, 140, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabrese, V.; Giordano, J.; Ruggieri, M.; Berritta, D.; Trovato, A.; Ontario, M.; Bianchini, R.; Calabrese, E. Hormesis, cellular stress response, and redox homeostasis in autism spectrum disorders. J. Neurosci. Res. 2016, 94, 1488–1498. [Google Scholar] [CrossRef]
- Liu, Z.; Chen, D.; Chen, X.; Bian, F.; Gao, N.; Li, J.; Pflugfelder, S.C.; Li, D.-Q. Autophagy Activation Protects Ocular Surface from Inflammation in a Dry Eye Model In Vitro. Int. J. Mol. Sci. 2020, 21, 8966. [Google Scholar] [CrossRef] [PubMed]
- Terman, A.; Gustafsson, B.; Brunk, U.T. Autophagy, organelles and ageing. J. Pathol. 2007, 211, 134–143. [Google Scholar] [CrossRef]
- Johnson, J.D.; Fleshner, M. Releasing signals, secretory pathways, and immune function of endogenous extracellular heat shock protein 72. J. Leukoc. Biol. 2006, 79, 425. [Google Scholar] [CrossRef] [Green Version]
- Salminen, A.; Kaarniranta, K. Regulation of the aging process by autophagy. Trends Mol. Med. 2009, 15, 217–224. [Google Scholar] [CrossRef]
- Xu, H.; Chen, M.; Forrester, J.V. Para-inflammation in the aging retina. Prog. Retin. Eye Res. 2009, 28, 348–368. [Google Scholar] [CrossRef]
- Simonsen, A.; Cumming, R.C.; Brech, A.; Isakson, P.; Schubert, D.R.; Finley, K.D. Promoting basal levels of autophagy in the nervous system enhances longevity and oxidant resistance in adult Drosophila. Autophagy 2008, 4, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Chambery, A. Insulin-like growth factor binding proteins 4 and 7 released by senescent cells promote premature senescence in mesenchymal stem cells. Cell. Death Dis. 2013, 4, e911. [Google Scholar]
- Davalos, A.R.; Coppe, J.P.; Campisi, J.; Desprez, P.Y. Senescent cells as a source of inflammatory factors for tumor progression. Cancer Metastasis Rev. 2010, 29, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Fumagalli, M.; d’Adda di Fagagna, F. SASPense and DDRama in cancer and ageing. Nat. Cell Biol. 2009, 11, 921–923. [Google Scholar] [CrossRef]
- Forrester, J.V. Bowman lecture on the role of inflammation in degenerative diseases of the eye. Eye 2013, 27, 340–352. [Google Scholar] [CrossRef] [Green Version]
- Terao, M.; Katayama, I. Local cortisol hydocorticosterone activation in skin physiology and pathology. J. Dermatol. Sci. 2016, 84, 11–16. [Google Scholar] [CrossRef]
- Susarla, R.; Liu, L.; Walker, E.A.; Bujalska, I.J.; Alsalem, J.; Williams, G.P.; Sreekantam, S.; Taylor, A.E.; Tallouzi, M.; Southworth, H.S.; et al. Cortisol biosynthesis in the human ocular surface innate immune response. PLoS ONE 2014, 9, e94913. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.C.; Grosso, R.A.; Fader, C.M. Hallmarks of Aging: An Autophagic Perspective. Front. Endocrinol. 2019, 9, 790. [Google Scholar] [CrossRef]
- Kallab, M.; Szegedi, S.; Hommer, N.; Stegmann, H.; Kaya, S.; Werkmeister, R.M.; Schmidl, D.; Schmetterer, L.; Garhöfer, G. Topical Low Dose Preservative-Free Hydrocortisone Reduces Signs and Symptoms in Patients with Chronic Dry Eye: A Randomized Clinical Trial. Adv. Ther. 2020, 37, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Perez, V.L.; Stern, M.E.; Pflugfelder, S.C. Inflammatory basis for dry eye disease flares. Exp. Eye Res. 2020, 201, 108294. [Google Scholar] [CrossRef]
- van Setten, G.; Labetoulle, M.; Baudouin, C.; Rolando, M. Evidence of seasonality and effects of psychrometry in dry eye disease. Acta Ophthalmol. 2016, 94, 499–506. [Google Scholar] [CrossRef] [Green Version]
- Aragona, P.; Baudouin, C.; Benitez Del Castillo, J.M.; Messmer, E.; Barabino, S.; Merayo-Lloves, J.; Brignole-Baudouin, F.; Inferrera, L.; Rolando, M.; Mencucci, R.; et al. The ocular microbiome and microbiota and their effects on ocular surface pathophysiology and disorders. Surv. Ophthalmol. 2021, 66, 907–925. [Google Scholar] [CrossRef]
- Aragona, P.; Rolando, M. Towards a dynamic customised therapy for ocular surface dysfunctions. Br. J. Ophthalmol. 2013, 97, 955–960. [Google Scholar] [CrossRef]
- Rolando, M.; Vagge, A. Safety and Efficacy of Cortisol Phosphate in the Treatment of Dry Eye in Sjogren Syndrome. J. Ocul. Pharmacol. Ther. 2017, 33, 383–390. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Maskin, S.L.; Anderson, B.; Chodosh, J.; Holland, E.J.; De Paiva, C.S.; Bartels, S.P.; Micuda, T.; Proskin, H.M.; Vogel, R. A randomized, double-masked, placebo-controlled, multicenter comparison of loteprednol etabonate ophthalmic suspension, 0.5%, and placebo for treatment of keratoconjunctivitis sicca in patients with delayed tear clearance. Am. J. Ophthalmol. 2004, 138, 444–457. [Google Scholar] [CrossRef]
- Shin, D.; Min, S. Comparison of treatment effects between 4.9% Nacetylaspartyl glutamic acid and 0.05% cyclosporine A eye drops in dry eye patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 3285–3291. [Google Scholar] [CrossRef]
- Wang, Y.J.; Monteagudo, A.; Downey, M.A.; Ashton-Rickardt, P.; Elmaleh, D. Cromolyn inhibits the secretion of inflammatory cytokines by human microglia (HMC3). Sci. Rep. 2021, 11, 8054. [Google Scholar] [CrossRef]
- Enríquez-de-Salamanca, A.; Castellanos, E.; Stern, M.E.; Fernández, I.; Carreño, E.; García-Vázquez, C.; Herreras, J.M.; Calonge, M. Tear cytokine and chemokine analysis and clinical correlations in evaporative-type dry eye disease. Mol. Vis. 2010, 16, 862–873. [Google Scholar]
- Labetoulle, M.; Benitez-del-Castillo, J.M.; Barabino, S.; Herrero Vanrell, R.; Daull, P.; Garrigue, J.-S.; Rolando, M. Artificial Tears: Biological Role of Their Ingredients in the Management of Dry Eye Disease. Int. J. Mol. Sci. 2022, 23, 2434. [Google Scholar] [CrossRef]
- Shimazaki, J.; Seika, D.; Saga, M.; Fukagawa, K.; Sakata, M.; Iwasaki, M.; Okano, T. A prospective, randomize trial of two mucin secretagogues for the treatment of dry eye syndrome in office workers. Sci. Rep. 2017, 7, 15210. [Google Scholar] [CrossRef] [Green Version]
- Sall, K.; Stevenson, O.D.; Mundorf, T.K.; Reis, B.L. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmology 2000, 107, 631–639. [Google Scholar] [CrossRef]
- Messmer, E.M.; Ahmad, S.; Benitez Del Castillo, J.M.; Mrukwa-Kominek, E.; Rolando, M.; Vitovska, O.; Baudouin, C.; A panel of European dry eye disease expert. Management of inflammation in dry eye disease: Recommendations from a European panel of experts. Eur. J. Ophthalmol. 2022, in press. [Google Scholar] [CrossRef]
- Qazi, Y.; Kheirkhah, A.; Blackie, C.; Trinidad, M.; Williams, C.; Cruzat, A.; Korb, D.R.; Hamrah, P. Clinically relevant immune-cellular metrics of inflammation in meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2018, 59, 6111–6123. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rolando, M.; Barabino, S.; Giannaccare, G.; Aragona, P. Dealing with the Persistent Pathogenic Issues of Dry Eye Disease: The Importance of External and Internal Stimuli and Tissue Responses. J. Clin. Med. 2023, 12, 2205. https://doi.org/10.3390/jcm12062205
Rolando M, Barabino S, Giannaccare G, Aragona P. Dealing with the Persistent Pathogenic Issues of Dry Eye Disease: The Importance of External and Internal Stimuli and Tissue Responses. Journal of Clinical Medicine. 2023; 12(6):2205. https://doi.org/10.3390/jcm12062205
Chicago/Turabian StyleRolando, Maurizio, Stefano Barabino, Giuseppe Giannaccare, and Pasquale Aragona. 2023. "Dealing with the Persistent Pathogenic Issues of Dry Eye Disease: The Importance of External and Internal Stimuli and Tissue Responses" Journal of Clinical Medicine 12, no. 6: 2205. https://doi.org/10.3390/jcm12062205