
The Imprint of Exposome on the Development of Atopic Dermatitis across the Lifespan: A Narrative Review
 , , ,
, , , {kind=link}
Abstract
:1. Introduction
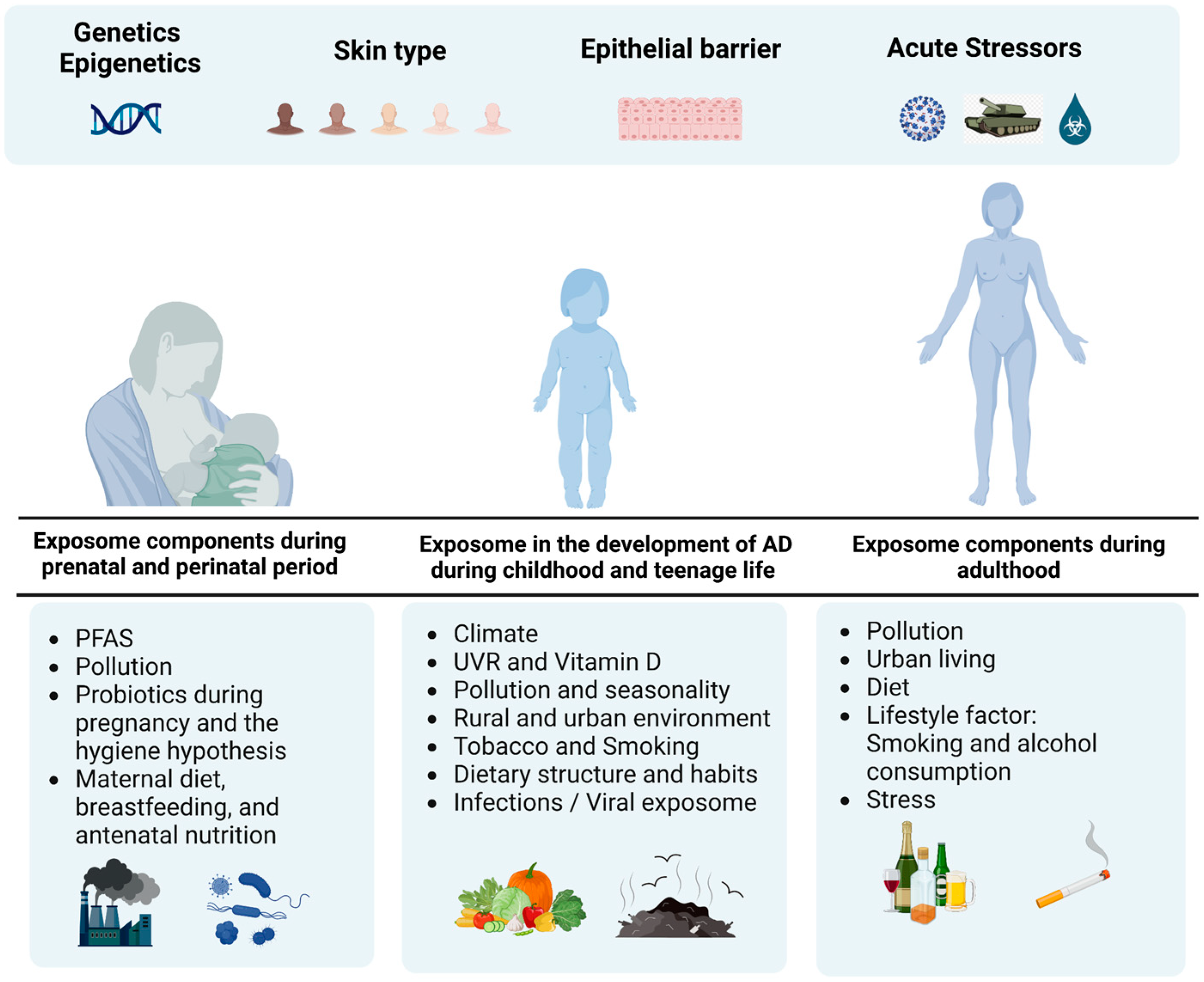
2. The Role of Exposome Components during Prenatal and Perinatal Period
2.1. Perfluoroalkyl and Polyfluoroalkyl Substances (PFASs)
2.2. Pollution
2.3. Probiotics during Pregnancy and the Hygiene Hypothesis
2.4. Maternal Diet and Antenatal Nutrition
3. Exposome in the Development of AD during Childhood and Teenage Life
3.1. Climate, UVR and Vitamin D
3.2. Pollution and Seasonality
3.3. Rural and Urban Environment
3.4. Tobacco and Smoking
3.5. Dietary Structure and Habits
3.6. Infections/Viral Exposome
4. The Exposome Effect on AD of Adulthood
4.1. Pollution
4.2. Urban Living
4.3. Diet
4.4. Lifestyle Factors—Smoking and Alcohol Consumption
4.5. Stress
5. Acute Stress Challenges: COVID-19 Pandemic and Russo–Ukrainian War
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic Dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Moltrasio, C.; Romagnuolo, M.; Marzano, A.V. Epigenetic Mechanisms of Epidermal Differentiation. Int. J. Mol. Sci. 2022, 23, 4874. [Google Scholar] [CrossRef]
- Smieszek, S.P.; Welsh, S.; Xiao, C.; Wang, J.; Polymeropoulos, C.; Birznieks, G.; Polymeropoulos, M.H. Correlation of Age-of-Onset of Atopic Dermatitis with Filaggrin Loss-of-Function Variant Status. Sci. Rep. 2020, 10, 2721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irvine, A.D.; Mina-Osorio, P. Disease Trajectories in Childhood Atopic Dermatitis: An Update and Practitioner’s Guide. Br. J. Dermatol. 2019, 181, 895–906. [Google Scholar] [CrossRef] [Green Version]
- Stefanovic, N.; Irvine, A.D.; Flohr, C. The Role of the Environment and Exposome in Atopic Dermatitis. Curr. Treat. Options Allergy 2021, 8, 222–241. [Google Scholar] [CrossRef] [PubMed]
- Ben-Gashir, M.A.; Seed, P.T.; Hay, R.J. Reliance on Erythema Scores May Mask Severe Atopic Dermatitis in Black Children Compared with Their White Counterparts. Br. J. Dermatol. 2002, 147, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Mei-Yen Yong, A.; Tay, Y.-K. Atopic Dermatitis. Dermatol. Clin. 2017, 35, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Chovatiya, R.; Begolka, W.S.; Thibau, I.J.; Silverberg, J.I. Financial Burden and Impact of Atopic Dermatitis Out-of-Pocket Healthcare Expenses among Black Individuals in the United States. Arch. Dermatol. Res. 2021, 314, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Lusignan, S.; Alexander, H.; Broderick, C.; Dennis, J.; McGovern, A.; Feeney, C.; Flohr, C. The Epidemiology of Eczema in Children and Adults in England: A Population-based Study Using Primary Care Data. Clin. Exp. Allergy 2021, 51, 471–482. [Google Scholar] [CrossRef]
- West, C.E.; Jenmalm, M.C.; Prescott, S.L. The Gut Microbiota and Its Role in the Development of Allergic Disease: A Wider Perspective. Clin. Exp. Allergy 2015, 45, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.; Law, B.; Liu, Y.-H.; Ambrocio, A.; Au, N.; Jiang, M.; Chow, K. The Association between Maternal Stress and Childhood Eczema: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker-Lalomio, M.; McCann, K.; Piorkowski, J.; Freels, S.; Persky, V.W. Prenatal Exposure to Polychlorinated Biphenyls and Asthma, Eczema/Hay Fever, and Frequent Ear Infections. J. Asthma 2018, 55, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, U.B.; Grandjean, P.; Nielsen, F.; Weihe, P.; Budtz-Jørgensen, E. Breastfeeding as an Exposure Pathway for Perfluorinated Alkylates. Environ. Sci. Technol. 2015, 49, 10466–10473. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Zartarian, V.; Moya, J.; Freeman, N.; Beamer, P.; Black, K.; Tulve, N.; Shalat, S. A Meta-Analysis of Children’s Hand-to-Mouth Frequency Data for Estimating Nondietary Ingestion Exposure. Risk Anal. 2007, 27, 411–420. [Google Scholar] [CrossRef] [PubMed]
- von Holst, H.; Nayak, P.; Dembek, Z.; Buehler, S.; Echeverria, D.; Fallacara, D.; John, L. Perfluoroalkyl Substances Exposure and Immunity, Allergic Response, Infection, and Asthma in Children: Review of Epidemiologic Studies. Heliyon 2021, 7, e08160. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Huang, R.; Hua, L.; Guo, Y.; Huang, L.; Zhao, Y.; Wang, X.; Zhang, J. Prenatal Exposure to Perfluoroalkyl and Polyfluoroalkyl Substances and Childhood Atopic Dermatitis: A Prospective Birth Cohort Study. Environ. Health 2018, 17, 8. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.-L.; Wang, S.-L.; Hsieh, C.-J.; Wen, H.-J.; Kuo, C.-C.; Liu, H.-J.; Sun, C.-W.; Chen, M.-L.; Wu, M.-T.; TMICS Study Group. Association between Prenatal Exposure to Metals and Atopic Dermatitis Among Children Aged 4 Years in Taiwan. JAMA Netw. Open 2021, 4, e2131327. [Google Scholar] [CrossRef] [PubMed]
- Just, A.C.; Whyatt, R.M.; Perzanowski, M.S.; Calafat, A.M.; Perera, F.P.; Goldstein, I.F.; Chen, Q.; Rundle, A.G.; Miller, R.L. Prenatal Exposure to Butylbenzyl Phthalate and Early Eczema in an Urban Cohort. Environ. Health Perspect. 2012, 120, 1475–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Park, S.K.; Park, H.; Lee, W.; Lee, J.H.; Hong, Y.-C.; Ha, M.; Kim, Y.; Lee, B.-E.; Ha, E. Joint Association of Prenatal Bisphenol-A and Phthalates Exposure with Risk of Atopic Dermatitis in 6-Month-Old Infants. Sci. Total Environ. 2021, 789, 147953. [Google Scholar] [CrossRef] [PubMed]
- Shaw, T.E.; Currie, G.P.; Koudelka, C.W.; Simpson, E.L. Eczema Prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J. Investig. Dermatol. 2011, 131, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.-I.; Lee, S.-H.; Lee, S.-Y.; Kim, H.-C.; Kim, H.-B.; Kim, J.-H.; Lim, H.; Park, M.J.; Cho, H.-J.; Yoon, J.; et al. Prenatal PM2.5 Exposure and Vitamin D–Associated Early Persistent Atopic Dermatitis via Placental Methylation. Ann. Allergy Asthma Immunol. 2020, 125, 665–673.e1. [Google Scholar] [CrossRef]
- Foolad, N.; Armstrong, A.W. Prebiotics and Probiotics: The Prevention and Reduction in Severity of Atopic Dermatitis in Children. Benef. Microbes 2014, 5, 151–160. [Google Scholar] [CrossRef]
- Makrgeorgou, A.; Leonardi-Bee, J.; Bath-Hextall, F.J.; Murrell, D.F.; Tang, M.L.; Roberts, A.; Boyle, R.J. Probiotics for Treating Eczema. Cochrane Database Syst. Rev. 2018, 2018, CD006135. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Zhai, S.; Tang, X.; Liu, C.; Li, W. Gut Microbiota and Atopic Dermatitis in Children: A Scoping Review. BMC Pediatr. 2022, 22, 323. [Google Scholar] [CrossRef]
- Prescott, S.L.; Calder, P.C. N-3 Polyunsaturated Fatty Acids and Allergic Disease. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 123–129. [Google Scholar] [CrossRef]
- Bloomfield, S.F.; Rook, G.A.; Scott, E.A.; Shanahan, F.; Stanwell-Smith, R.; Turner, P. Time to Abandon the Hygiene Hypothesis: New Perspectives on Allergic Disease, the Human Microbiome, Infectious Disease Prevention and the Role of Targeted Hygiene. Perspect. Public Health 2016, 136, 213–224. [Google Scholar] [CrossRef]
- Amalia, N.; Orchard, D.; Francis, K.L.; King, E. Systematic Review and Meta-analysis on the Use of Probiotic Supplementation in Pregnant Mother, Breastfeeding Mother and Infant for the Prevention of Atopic Dermatitis in Children. Australas. J. Derm. 2020, 61, 628–643. [Google Scholar] [CrossRef] [PubMed]
- Nicolaou, N.; Pancheva, R.; Karaglani, E.; Sekkidou, M.; Marinova-Achkar, M.; Popova, S.; Tzaki, M.; Kapetanaki, A.; Iacovidou, N.; Boutsikou, T.; et al. The Risk Reduction Effect of a Nutritional Intervention With a Partially Hydrolyzed Whey-Based Formula on Cow’s Milk Protein Allergy and Atopic Dermatitis in High-Risk Infants Within the First 6 Months of Life: The Allergy Reduction Trial (A.R.T.), a Multicenter Double-Blinded Randomized Controlled Study. Front. Nutr. 2022, 9, 863599. [Google Scholar] [CrossRef]
- LISA Study Group; Sausenthaler, S.; Koletzko, S.; Schaaf, B.; Lehmann, I.; Borte, M.; Herbarth, O.; von Berg, A.; Wichmann, H.-E.; Heinrich, J. Maternal Diet during Pregnancy in Relation to Eczema and Allergic Sensitization in the Offspring at 2 y of Age. Am. J. Clin. Nutr. 2007, 85, 530–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, K.G.; Gebretsadik, T.; Hartman, T.J.; Rosa, M.J.; Tylavsky, F.A.; Adgent, M.A.; Moore, P.E.; Kocak, M.; Bush, N.R.; Davis, R.L.; et al. Prenatal Omega-3 and Omega-6 Polyunsaturated Fatty Acids and Childhood Atopic Dermatitis. J. Allergy Clin. Immunol. Pract. 2020, 8, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Brzozowska, A.; Podlecka, D.; Jankowska, A.; Król, A.; Kaleta, D.; Trafalska, E.; Nowakowska-Świrta, E.; Kałużny, P.; Hanke, W.; Bal-Gierańczyk, K.; et al. Maternal Diet during Pregnancy and Risk of Allergic Diseases in Children up to 7–9 Years Old from Polish Mother and Child Cohort Study. Environ. Res. 2022, 208, 112682. [Google Scholar] [CrossRef]
- Mubanga, M.; Lundholm, C.; D’Onofrio, B.M.; Stratmann, M.; Hedman, A.; Almqvist, C. Association of Early Life Exposure to Antibiotics With Risk of Atopic Dermatitis in Sweden. JAMA Netw. Open 2021, 4, e215245. [Google Scholar] [CrossRef]
- Cui, H.; Mu, Z. Prenatal Maternal Risk Factors Contributing to Atopic Dermatitis: A Systematic Review and Meta-Analysis of Cohort Studies. Ann. Derm. 2023, 35, 11. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Hanifin, J.; Simpson, E.L. Climatic Factors Are Associated with Childhood Eczema Prevalence in the United States. J. Investig. Dermatol. 2013, 133, 1752–1759. [Google Scholar] [CrossRef] [Green Version]
- Rueter, K.; Jones, A.P.; Siafarikas, A.; Chivers, P.; Prescott, S.L.; Palmer, D.J. The Influence of Sunlight Exposure and Sun Protecting Behaviours on Allergic Outcomes in Early Childhood. Int. J. Environ. Res. Public Health 2021, 18, 5429. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.A.; Ganmaa, D.; Sidbury, R.; Erdenedelger, K.; Radnaakhand, N.; Khandsuren, B. Randomized Trial of Vitamin D Supplementation for Winter-Related Atopic Dermatitis in Children. J. Allergy Clin. Immunol. 2014, 134, 831–835.e1. [Google Scholar] [CrossRef] [PubMed]
- Thyssen, J.P.; Zirwas, M.J.; Elias, P.M. Potential Role of Reduced Environmental UV Exposure as a Driver of the Current Epidemic of Atopic Dermatitis. J. Allergy Clin. Immunol. 2015, 136, 1163–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, C.; Silverberg, J.I. The Prevalence and Persistence of Atopic Dermatitis in Urban United States Children. Ann. Allergy Asthma Immunol. 2019, 123, 173–178.e1. [Google Scholar] [CrossRef]
- Wan, J.; Oganisian, A.; Spieker, A.J.; Hoffstad, O.J.; Mitra, N.; Margolis, D.J.; Takeshita, J. Racial/Ethnic Variation in Use of Ambulatory and Emergency Care for Atopic Dermatitis among US Children. J. Investig. Dermatol. 2019, 139, 1906–1913.e1. [Google Scholar] [CrossRef] [PubMed]
- Tackett, K.J.; Jenkins, F.; Morrell, D.S.; McShane, D.B.; Burkhart, C.N. Structural Racism and Its Influence on the Severity of Atopic Dermatitis in African American Children. Pediatr. Derm. 2020, 37, 142–146. [Google Scholar] [CrossRef]
- Botha, M.; Basera, W.; Facey-Thomas, H.E.; Gaunt, B.; Genuneit, J.; Gray, C.L.; Kiragu, W.; Ramjith, J.; Watkins, A.; Levin, M.E. Nutrition and Allergic Diseases in Urban and Rural Communities from the South African Food Allergy Cohort. Pediatr. Allergy Immunol. 2019, 30, 511–521. [Google Scholar] [CrossRef]
- Lee, J.-T.; Cho, Y.-S.; Son, J.-Y. Relationship between Ambient Ozone Concentrations and Daily Hospital Admissions for Childhood Asthma/Atopic Dermatitis in Two Cities of Korea during 2004–2005. Int. J. Environ. Health Res. 2010, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yi, O.; Kwon, H.-J.; Kim, H.; Ha, M.; Hong, S.-J.; Hong, Y.-C.; Leem, J.-H.; Sakong, J.; Lee, C.G.; Kim, S.-Y.; et al. Effect of Environmental Tobacco Smoke on Atopic Dermatitis among Children in Korea. Environ. Res. 2012, 113, 40–45. [Google Scholar] [CrossRef]
- Krämer, U.; Weidinger, S.; Darsow, U.; Möhrenschlager, M.; Ring, J.; Behrendt, H. Seasonality in Symptom Severity Influenced by Temperature or Grass Pollen: Results of a Panel Study in Children with Eczema. J. Investig. Dermatol. 2005, 124, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kathuria, P.; Silverberg, J.I. Association of Pollution and Climate with Atopic Eczema in US Children. Pediatr. Allergy Immunol. 2016, 27, 478–485. [Google Scholar] [CrossRef]
- Patra, V.; Byrne, S.N.; Wolf, P. The Skin Microbiome: Is It Affected by UV-Induced Immune Suppression? Front. Microbiol. 2016, 7, 1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero-Fernandez, M.; Montero-Vilchez, T.; Diaz-Calvillo, P.; Romera-Vilchez, M.; Buendia-Eisman, A.; Arias-Santiago, S. Impact of Water Exposure and Temperature Changes on Skin Barrier Function. J. Clin. Med. 2022, 11, 298. [Google Scholar] [CrossRef]
- Tamagawa-Mineoka, R.; Katoh, N. Atopic Dermatitis: Identification and Management of Complicating Factors. Int. J. Mol. Sci. 2020, 21, 2671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arafune, J.; Tsujiguchi, H.; Hara, A.; Shimizu, Y.; Hori, D.; Nguyen, T.T.T.; Suzuki, F.; Hamagishi, T.; Yamada, Y.; Nakamura, H.; et al. Increased Prevalence of Atopic Dermatitis in Children Aged 0–3 Years Highly Exposed to Parabens. Int. J. Environ. Res. Public Health 2021, 18, 11657. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Silcocks, P.; Williams, H.C. What Causes Flares of Eczema in Children? Br. J. Dermatol. 2009, 161, 640–646. [Google Scholar] [CrossRef]
- Haarala, A.K.; Sinikumpu, S.-P.; Vaaramo, E.; Jokelainen, J.; Timonen, M.; Auvinen, J.; Pekkanen, J.; Huilaja, L. A Childhood Farm Environment Protects from Allergic Sensitization until Middle Age but Not from New-Onset Sensitization in Adulthood: A 15 Year Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 7078. [Google Scholar] [CrossRef]
- Penders, J.; Gerhold, K.; Thijs, C.; Zimmermann, K.; Wahn, U.; Lau, S.; Hamelmann, E. New Insights into the Hygiene Hypothesis in Allergic Diseases: Mediation of Sibling and Birth Mode Effects by the Gut Microbiota. Gut Microbes 2014, 5, 239–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akdis, C.A.; Akdis, M.; Boyd, S.D.; Sampath, V.; Galli, S.J.; Nadeau, K.C. Allergy: Mechanistic Insights into New Methods of Prevention and Therapy. Sci. Transl. Med. 2023, 15, eadd2563. [Google Scholar] [CrossRef]
- Herrant, M.; Loucoubar, C.; Boufkhed, S.; Bassène, H.; Sarr, F.D.; Baril, L.; Mercereau-Puijalon, O.; Mécheri, S.; Sakuntabhai, A.; Paul, R. Risk Factors Associated with Asthma, Atopic Dermatitis and Rhinoconjunctivitis in a Rural Senegalese Cohort. Allergy Asthma Clin. Immunol. 2015, 11, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thyssen, J.P.; Ahluwalia, T.S.; Paternoster, L.; Ballardini, N.; Bergström, A.; Melén, E.; Chawes, B.L.; Stokholm, J.; Hourihane, J.O.; O’Sullivan, D.M.; et al. Interaction between Filaggrin Mutations and Neonatal Cat Exposure in Atopic Dermatitis. Allergy 2020, 75, 1481–1485. [Google Scholar] [CrossRef]
- Langan, S.M.; Flohr, C.; Williams, H.C. The Role of Furry Pets in Eczema: A Systematic Review. Arch. Derm. 2007, 143, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Galeone, C.; Bach, J.-F.; La Vecchia, C.; Chatenoud, L. Pet Exposure and Risk of Atopic Dermatitis at the Pediatric Age: A Meta-Analysis of Birth Cohort Studies. J. Allergy Clin. Immunol. 2013, 132, 616–622.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruokolainen, L.; Paalanen, L.; Karkman, A.; Laatikainen, T.; von Hertzen, L.; Vlasoff, T.; Markelova, O.; Masyuk, V.; Auvinen, P.; Paulin, L.; et al. Significant Disparities in Allergy Prevalence and Microbiota between the Young People in Finnish and Russian Karelia. Clin. Exp. Allergy 2017, 47, 665–674. [Google Scholar] [CrossRef]
- Haahtela, T.; Laatikainen, T.; Alenius, H.; Auvinen, P.; Fyhrquist, N.; Hanski, I.; von Hertzen, L.; Jousilahti, P.; Kosunen, T.U.; Markelova, O.; et al. Hunt for the Origin of Allergy—Comparing the Finnish and Russian Karelia. Clin. Exp. Allergy 2015, 45, 891–901. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Janson, C.; Malinovschi, A.; Holm, M.; Franklin, K.A.; Modig, L.; Johannessen, A.; Schlünssen, V.; Gislason, T.; Jogi, N.O.; et al. Asthma, Allergic Rhinitis and Atopic Dermatitis in Association with Home Environment—The RHINE Study. Sci. Total Environ. 2022, 853, 158609. [Google Scholar] [CrossRef]
- Mahdavinia, M.; Greenfield, L.R.; Moore, D.; Botha, M.; Engen, P.; Gray, C.; Lunjani, N.; Hlela, C.; Basera, W.; Hobane, L.; et al. House Dust Microbiota and Atopic Dermatitis; Effect of Urbanization. Pediatr. Allergy Immunol. 2021, 32, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.E.; Botha, M.; Basera, W.; Facey-Thomas, H.E.; Gaunt, B.; Gray, C.L.; Kiragu, W.; Ramjith, J.; Watkins, A.; Genuneit, J. Environmental Factors Associated with Allergy in Urban and Rural Children from the South African Food Allergy (SAFFA) Cohort. J. Allergy Clin. Immunol. 2020, 145, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Lunjani, N.; Tan, G.; Dreher, A.; Sokolowska, M.; Groeger, D.; Warwyzniak, M.; Altunbulakli, C.; Westermann, P.; Basera, W.; Hobane, L.; et al. Environment-dependent Alterations of Immune Mediators in Urban and Rural South African Children with Atopic Dermatitis. Allergy 2022, 77, 569–581. [Google Scholar] [CrossRef]
- Thacher, J.D.; Gruzieva, O.; Pershagen, G.; Neuman, Å.; Wickman, M.; Kull, I.; Melén, E.; Bergström, A. Pre- and Postnatal Exposure to Parental Smoking and Allergic Disease Through Adolescence. Pediatrics 2014, 134, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Biagini Myers, J.M.; Khurana Hershey, G.K. Eczema in Early Life: Genetics, the Skin Barrier, and Lessons Learned from Birth Cohort Studies. J. Pediatr. 2010, 157, 704–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantor, R.; Kim, A.; Thyssen, J.P.; Silverberg, J.I. Association of Atopic Dermatitis with Smoking: A Systematic Review and Meta-Analysis. J. Am. Acad. Dermatol. 2016, 75, 1119–1125.e1. [Google Scholar] [CrossRef] [Green Version]
- Morales, E.; Strachan, D.; Asher, I.; Ellwood, P.; Pearce, N.; Garcia-Marcos, L. Combined Impact of Healthy Lifestyle Factors on Risk of Asthma, Rhinoconjunctivitis and Eczema in School Children: ISAAC Phase III. Thorax 2019, 74, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Jaffary, F.; Faghihi, G.; Mokhtarian, A.; Hosseini, S. Effects of Oral Vitamin E on Treatment of Atopic Dermatitis: A Randomized Controlled Trial. J. Res. Med. Sci. 2015, 20, 1053. [Google Scholar] [CrossRef]
- Shin, J.; Kim, Y.J.; Kwon, O.; Kim, N.-I.; Cho, Y. Associations among Plasma Vitamin C, Epidermal Ceramide and Clinical Severity of Atopic Dermatitis. Nutr. Res. Pract. 2016, 10, 398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.-Y.; Chung, J.; Kim, M.-K.; Kwon, S.O.; Cho, B.-H. Antioxidant Nutrient Intakes and Corresponding Biomarkers Associated with the Risk of Atopic Dermatitis in Young Children. Eur. J. Clin. Nutr. 2010, 64, 245–252. [Google Scholar] [CrossRef]
- Cho, S.I.; Lee, H.; Lee, D.H.; Kim, K.-H. Association of Frequent Intake of Fast Foods, Energy Drinks, or Convenience Food with Atopic Dermatitis in Adolescents. Eur. J. Nutr. 2020, 59, 3171–3182. [Google Scholar] [CrossRef]
- Kong, H.H.; Oh, J.; Deming, C.; Conlan, S.; Grice, E.A.; Beatson, M.A.; Nomicos, E.; Polley, E.C.; Komarow, H.D.; NISC Comparative Sequence Program; et al. Temporal Shifts in the Skin Microbiome Associated with Disease Flares and Treatment in Children with Atopic Dermatitis. Genome Res. 2012, 22, 850–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grice, E.A.; Kong, H.H.; Conlan, S.; Deming, C.B.; Davis, J.; Young, A.C.; NISC Comparative Sequencing Program; Bouffard, G.G.; Blakesley, R.W.; Murray, P.R.; et al. Topographical and Temporal Diversity of the Human Skin Microbiome. Science 2009, 324, 1190–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerre, R.D.; Holm, J.B.; Palleja, A.; Sølberg, J.; Skov, L.; Johansen, J.D. Skin Dysbiosis in the Microbiome in Atopic Dermatitis Is Site-Specific and Involves Bacteria, Fungus and Virus. BMC Microbiol. 2021, 21, 256. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, H.; Li, N.; Bonnelykke, K.; Chawes, B.L.K.; Skov, T.; Paludan-Müller, G.; Stokholm, J.; Smith, B.; Krogfelt, K.A. Reduced Diversity of the Intestinal Microbiota during Infancy Is Associated with Increased Risk of Allergic Disease at School Age. J. Allergy Clin. Immunol. 2011, 128, 646–652.e5. [Google Scholar] [CrossRef] [PubMed]
- Namara, B.; Nash, S.; Lule, S.A.; Akurut, H.; Mpairwe, H.; Akello, F.; Tumusiime, J.; Kizza, M.; Kabagenyi, J.; Nkurunungi, G.; et al. Effects of Treating Helminths during Pregnancy and Early Childhood on Risk of Allergy-Related Outcomes: Follow-up of a Randomized Controlled Trial. Pediatr. Allergy Immunol. 2017, 28, 784–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.H.; Patel, K.R.; Singam, V.; Rastogi, S.; Silverberg, J.I. A Systematic Review and Meta-Analysis of the Prevalence and Phenotype of Adult-Onset Atopic Dermatitis. J. Am. Acad. Dermatol. 2019, 80, 1526–1532.e7. [Google Scholar] [CrossRef]
- Niwa, Y.; Sumi, H.; Kawahira, K.; Terashima, T.; Nakamura, T.; Akamatsu, H. Protein Oxidative Damage in the Stratum Corneum: Evidence for a Link between Environmental Oxidants and the Changing Prevalence and Nature of Atopic Dermatitis in Japan. Br. J. Derm. 2003, 149, 248–254. [Google Scholar] [CrossRef]
- Folster-Holst, R.; Pape, M.; Buss, Y.L.; Christophers, E.; Weichenthal, M. Low Prevalence of the Intrinsic Form of Atopic Dermatitis among Adult Patients. Allergy 2006, 61, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.-T.; Ku, K.-C.; Chen, D.-Y.; Lin, C.-H.; Tsuang, B.-J.; Chen, Y.-H. Adult Atopic Dermatitis and Exposure to Air Pollutants—A Nationwide Population-Based Study. Ann. Allergy Asthma Immunol. 2017, 118, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Kantor, R.; Silverberg, J.I. Environmental Risk Factors and Their Role in the Management of Atopic Dermatitis. Expert Rev. Clin. Immunol. 2017, 13, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothenberg, M.E. The Climate Change Hypothesis for the Allergy Epidemic. J. Allergy Clin. Immunol. 2022, 149, 1522–1524. [Google Scholar] [CrossRef] [PubMed]
- Kim, K. Influences of Environmental Chemicals on Atopic Dermatitis. Toxicol. Res. 2015, 31, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Tang, K.-T.; Chen, P.-A.; Lee, M.-R.; Lee, M.-F.; Chen, Y.-H. The Relationship between Exposure to Polycyclic Aromatic Hydrocarbons and Adult Atopic Dermatitis. Asian Pac. J. Allergy Immunol. 2020. [Google Scholar] [CrossRef]
- Hidaka, T.; Ogawa, E.; Kobayashi, E.H.; Suzuki, T.; Funayama, R.; Nagashima, T.; Fujimura, T.; Aiba, S.; Nakayama, K.; Okuyama, R.; et al. The Aryl Hydrocarbon Receptor AhR Links Atopic Dermatitis and Air Pollution via Induction of the Neurotrophic Factor Artemin. Nat. Immunol. 2017, 18, 64–73. [Google Scholar] [CrossRef]
- Hendricks, A.J.; Eichenfield, L.F.; Shi, V.Y. The Impact of Airborne Pollution on Atopic Dermatitis: A Literature Review. Br. J. Derm. 2020, 183, 16–23. [Google Scholar] [CrossRef]
- Kabashima, K.; Otsuka, A.; Nomura, T. Linking Air Pollution to Atopic Dermatitis. Nat. Immunol. 2017, 18, 5–6. [Google Scholar] [CrossRef]
- Wesley, N.O.; Maibach, H.I. Racial (Ethnic) Differences in Skin Properties: The Objective Data. Am. J. Clin. Dermatol. 2003, 4, 843–860. [Google Scholar] [CrossRef] [PubMed]
- Pesce, G.; Marcon, A.; Carosso, A.; Antonicelli, L.; Cazzoletti, L.; Ferrari, M.; Fois, A.G.; Marchetti, P.; Olivieri, M.; Pirina, P.; et al. Adult Eczema in Italy: Prevalence and Associations with Environmental Factors. J. Eur. Acad. Derm. Venereol. 2015, 29, 1180–1187. [Google Scholar] [CrossRef]
- Nnoruka, E.N. Current Epidemiology of Atopic Dermatitis in South-Eastern Nigeria. Int. J. Derm. 2004, 43, 739–744. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Hanifin, J.M. Adult Eczema Prevalence and Associations with Asthma and Other Health and Demographic Factors: A US Population–Based Study. J. Allergy Clin. Immunol. 2013, 132, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Balić, A.; Vlašić, D.; Žužul, K.; Marinović, B.; Bukvić Mokos, Z. Omega-3 Versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. Int. J. Mol. Sci. 2020, 21, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksen, B.B.; Kåre, D.L. Open Trial of Supplements of Omega 3 and 6 Fatty Acids, Vitamins and Minerals in Atopic Dermatitis. J. Dermatol. Treat. 2006, 17, 82–85. [Google Scholar] [CrossRef]
- Ito, M.; Morita, T.; Okazaki, S.; Koto, M.; Ichikawa, Y.; Takayama, R.; Hoashi, T.; Saeki, H.; Kanda, N. Dietary Habits in Adult Japanese Patients with Atopic Dermatitis. J. Derm. 2019, 46, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Goicolea, J.; Hernández, R.; Bañuelos, C.; Segovia, J.; Fernández-Ortiz, A.; Gonçalves, M.; Alonso, L.; Macaya, C. [Coronary angioscopy: Initial experience during coronary interventions]. Rev. Esp. Cardiol. 1995, 48, 798–806. [Google Scholar] [PubMed]
- Park, S.; Bae, J.-H. Fermented Food Intake Is Associated with a Reduced Likelihood of Atopic Dermatitis in an Adult Population (Korean National Health and Nutrition Examination Survey 2012-2013). Nutr. Res. 2016, 36, 125–133. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Greenland, P. Eczema and Cardiovascular Risk Factors in 2 US Adult Population Studies. J. Allergy Clin. Immunol. 2015, 135, 721–728.e6. [Google Scholar] [CrossRef]
- Lee, C.H.; Chuang, H.Y.; Hong, C.H.; Huang, S.K.; Chang, Y.C.; Ko, Y.C.; Yu, H.S. Lifetime Exposure to Cigarette Smoking and the Development of Adult-Onset Atopic Dermatitis: Smoking and Adult Atopic Dermatitis. Br. J. Dermatol. 2011, 164, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Pilz, A.C.; Schielein, M.C.; Schuster, B.; Heinrich, L.; Haufe, E.; Abraham, S.; Heratizadeh, A.; Harder, I.; Kleinheinz, A.; Wollenberg, A.; et al. Atopic Dermatitis: Disease Characteristics and Comorbidities in Smoking and Non-smoking Patients from the TREATgermany Registry. Acad. Derm. Venereol. 2022, 36, 413–421. [Google Scholar] [CrossRef]
- Morra, D.E.; Cho, E.; Li, T.; Camargo, C.A.; Qureshi, A.A.; Drucker, A.M. Smoking and Risk of Adult-Onset Atopic Dermatitis in US Women. J. Am. Acad. Dermatol. 2021, 84, 561–563. [Google Scholar] [CrossRef]
- Pilz, A.C.; Durner, V.; Schielein, M.C.; Schuster, B.; Beckmann, J.; Biedermann, T.; Eyerich, K.; Zink, A. Addictions in Patients with Atopic Dermatitis: A Cross-sectional Pilot Study in Germany. J. Eur. Acad. Derm. Venereol. 2022, 36, 84–90. [Google Scholar] [CrossRef]
- Pondeljak, N.; Lugović-Mihić, L. Stress-Induced Interaction of Skin Immune Cells, Hormones, and Neurotransmitters. Clin. Ther. 2020, 42, 757–770. [Google Scholar] [CrossRef]
- Seiffert, K.; Hilbert, E.; Schaechinger, H.; Zouboulis, C.C.; Deter, H.-C. Psychophysiological Reactivity under Mental Stress in Atopic Dermatitis. Dermatology 2005, 210, 286–293. [Google Scholar] [CrossRef]
- Kodama, A.; Horikawa, T.; Suzuki, T.; Ajiki, W.; Takashima, T.; Harada, S.; Ichihashi, M. Effect of Stress on Atopic Dermatitis: Investigation in Patients after the Great Hanshin Earthquake. J. Allergy Clin. Immunol. 1999, 104, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.M.; Akiyama, T. The Vicious Cycle of Itch and Anxiety. Neurosci. Biobehav. Rev. 2018, 87, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Garg, N.K.; Paller, A.S.; Fishbein, A.B.; Zee, P.C. Sleep Disturbances in Adults with Eczema Are Associated with Impaired Overall Health: A US Population-Based Study. J. Investig. Dermatol. 2015, 135, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinhoff, M.; Suárez, A.; Feramisco, J.; Koo, J. Psychoneuroimmunology of Psychological Stress and Atopic Dermatitis: Pathophysiologic and Therapeutic Updates. Acta Derm. Venerol. 2012, 92, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Yosipovitch, G.; Tran, B.; Papoiu, A.; Russoniello, C.; Wang, H.; Patel, T.; Chan, Y. Effect of Itch, Scratching and Mental Stress on Autonomic Nervous System Function in Atopic Dermatitis. Acta Derm. Venerol. 2010, 90, 354–361. [Google Scholar] [CrossRef]
- Hurley, S.; Franklin, R.; McCallion, N.; Byrne, A.M.; Fitzsimons, J.; Byrne, S.; White, M.; O’Mahony, L.; Hourihane, J.O. Allergy-related Outcomes at 12 Months in the CORAL Birth Cohort of Irish Children Born during the First COVID 19 Lockdown. Pediatr. Allergy Immunol. 2022, 33, e13766. [Google Scholar] [CrossRef]
- Singh, M.; Pawar, M.; Bothra, A.; Choudhary, N. Overzealous Hand Hygiene during the COVID 19 Pandemic Causing an Increased Incidence of Hand Eczema among General Population. J. Am. Acad. Dermatol. 2020, 83, e37–e41. [Google Scholar] [CrossRef]
- Pecoraro, L.; Chiaffoni, G.; Piacentini, G.; Pietrobelli, A. The Need of an Updated Culture of “Occupational” Atopic Hand Dermatitis in Children at the Time of COVID-19. Acta Biomed. 2022, 93, e2022324. [Google Scholar] [CrossRef] [PubMed]
- Rundle, C.W.; Presley, C.L.; Militello, M.; Barber, C.; Powell, D.L.; Jacob, S.E.; Atwater, A.R.; Watsky, K.L.; Yu, J.; Dunnick, C.A. Hand Hygiene during COVID-19: Recommendations from the American Contact Dermatitis Society. J. Am. Acad. Dermatol. 2020, 83, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.; Bašić, F.; Bogunovic, I.; Barcelo, D. Russian-Ukrainian War Impacts the Total Environment. Sci. Total Environ. 2022, 837, 155865. [Google Scholar] [CrossRef]
- Riegleman, K.L.; Farnsworth, G.S.; Wong, E.B. Atopic Dermatitis in the US Military. Cutis 2019, 104, 144–147. [Google Scholar] [PubMed]
- The Lancet Ukraine’s Humanitarian Disaster: Priorities for Health. Lancet 2022, 399, 1023. [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grafanaki, K.; Bania, A.; Kaliatsi, E.G.; Vryzaki, E.; Vasilopoulos, Y.; Georgiou, S. The Imprint of Exposome on the Development of Atopic Dermatitis across the Lifespan: A Narrative Review. J. Clin. Med. 2023, 12, 2180. https://doi.org/10.3390/jcm12062180
Grafanaki K, Bania A, Kaliatsi EG, Vryzaki E, Vasilopoulos Y, Georgiou S. The Imprint of Exposome on the Development of Atopic Dermatitis across the Lifespan: A Narrative Review. Journal of Clinical Medicine. 2023; 12(6):2180. https://doi.org/10.3390/jcm12062180
Chicago/Turabian StyleGrafanaki, Katerina, Angelina Bania, Eleni G. Kaliatsi, Eleftheria Vryzaki, Yiannis Vasilopoulos, and Sophia Georgiou. 2023. "The Imprint of Exposome on the Development of Atopic Dermatitis across the Lifespan: A Narrative Review" Journal of Clinical Medicine 12, no. 6: 2180. https://doi.org/10.3390/jcm12062180