
The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management

 , , and
, , and
Abstract
:1. Introduction
1.1. Global Burden of Valvular Heart Disease (VHD)
1.2. Factors Responsible for Changes in the Epidemiology of VHD
- -
- Population aging. Worldwide life-expectancy has improved over time [9]. As populations age, some VHD historically considered “age-related”, such as CAVD and degenerative mitral regurgitation (MR), have time to become symptomatic and, consequently, be detected. Furthermore, major advances in the treatment of VHD have allowed for the improvement of long-term survival, thus increasing global prevalence.
- -
- Availability of imaging techniques and accessibility to diagnosis and treatment. Some VHDs, such as RHD, are associated with poverty, inequality, overcrowding, and a lack of healthcare facilities, including access to treatment. Despite the worldwide rates of extreme poverty having fallen in the past 40–50 years, RHD prevalence continues to increase unabated. The continuing increase in prevalence cannot be attributed only to population aging but likely reflects the increased global awareness, the increasing availability of echocardiography for case definitions, the greater access to treatment, and the consequent improved survival in many low-income countries [8]. Similarly, in middle- and high-income countries, the advent of progressively advanced echocardiography machines, the improvement of operator skills, and the shift of healthcare systems towards prevention policies have meant that degenerative VHDs (for example, aortic stenosis—AS—and primary MR) are diagnosed more easily, even if mild and asymptomatic.
- -
- Migration flows. The spread of urbanization worldwide during the transition from agricultural to industrial activity and service economies is responsible for exposing increasing numbers of people to traditional and non-traditional cardiovascular risk factors, such as smoking, hypertension, obesity, diabetes, air pollution, and stress, which are strongly associated with VHD, as calcific AS [10]. As fertility rates fall below replacement levels in high-income countries and population aging increases, the need for young immigrant groups to supplement the workforce and provide support for the elderly becomes more pressing [10]. Socioeconomic deprivation is common in immigrant groups and is compounded by a range of health inequalities, many of which are indirect consequences of discrimination and racism [11]. Immigrants are more likely to have RHD, which is usually very rare among high-income country inhabitants, and are exposed to cardiovascular risk factors that make them more prone to develop early cardiovascular disease, including VHD.
- -
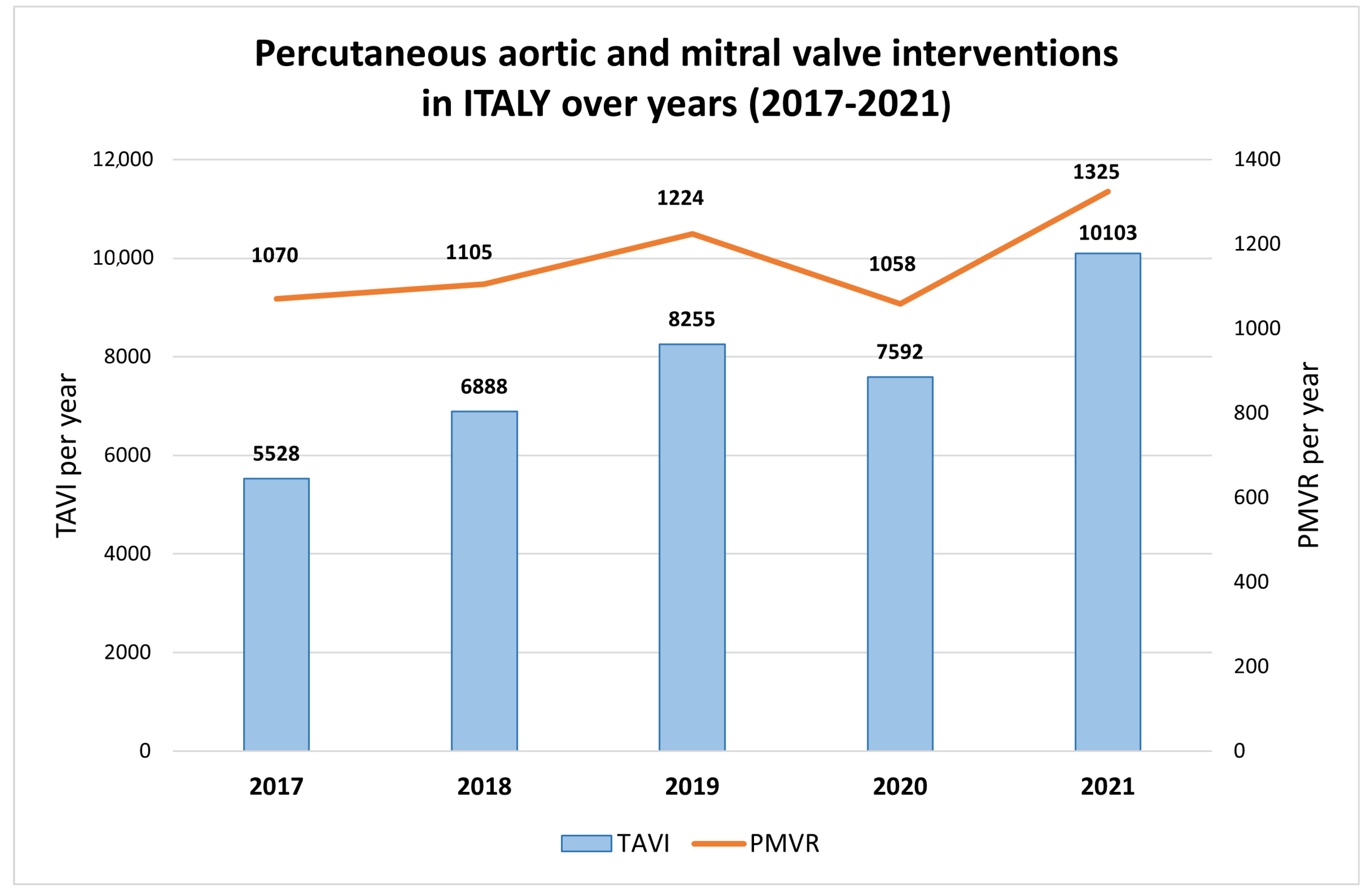
- The improvement in valve surgery and the advent of transcatheter procedures. Valve repair and replacement are now routine cardiac surgical procedures with increasing safety and durability, and they are responsible for the increased survival of patients with VHD. Even in low- and middle-income countries, the access to heart valve surgery is increasing day by day. Nonetheless, due to the combination of high device costs and available workforce capacity and expertise, large discrepancies still persist. Indeed, while in some West-African countries, just 1 cardiac surgeon per 10 million inhabitants is available [12], in some European Countries (e.g., Finland and Lithuania), this proportion goes up to 1 per 200 [7]. In the last decade, transcatheter interventions for VHD have had a rapid increase, allowing for the successful treatment of VHD in old, fragile, and high-surgical-risk patients, with procedural numbers growing exponentially [13]. Moreover, the intrinsic possibility of performing multiple sequential and “staged” transcatheter procedures sparks a real paradigm change for the management of patients with mixed valve disease, who are no longer strictly obliged to undergo cardiac surgery [14]. Confirming the popularity of transcatheter interventions for VHD, a median of 60.0 transcatheter aortic valve implantation procedures and 5.4 percutaneous mitral valve (MV) repairs (PMVR) per million inhabitants were performed in 2019 in European countries [7]. For example, as shown in Figure 1, a relevant increase in percutaneous aortic and MV interventions occurred in Italy in the last five years.
- -
- The increase in the predisposing factors of infective endocarditis. The last 20 years have witnessed an increase in all the main factors predisposing to infective endocarditis, such as an aging population, the increased use of intracardiac, vascular, and valvular devices (e.g., pacemakers, defibrillators, biological and mechanical valve prostheses), epidemic levels of opioid addiction, and associated injection drug use. Furthermore, the inadequate and unholy antibiotic use, with the consequent increase in antibiotic resistance, has led to the dangerous shift from Streptococcus to more virulent microorganisms, such as Staphylococcus and Enterococcus, as more common causative organisms of infective endocarditis [15].
2. Aortic Stenosis
3. Aortic Regurgitation
4. Mitral Stenosis
5. Mitral Regurgitation
6. Tricuspid Regurgitation
7. Multiple VHD
8. Heart Valve Centers
9. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AR | Aortic regurgitation |
| AS | Aortic stenosis |
| BAV | Bicuspid aortic valve |
| CAVD | Calcific aortic valve disease |
| CMR | Cardiac magnetic resonance |
| CIED | Cardiac implantable electronic device |
| ESC | European Society of Cardiology |
| FMR | Functional-mitral regurgitation |
| HF | Heart failure |
| HT | Heart team |
| LA | Left atrium |
| LV | Left ventricular |
| LVESD | Left ventricular end-systolic diameter |
| MAC | Mitral annulus calcification |
| MAD | Mitral annular disjunction |
| MHD | Multivalvular heart disease |
| MR | Mitral regurgitation |
| MS | Mitral stenosis |
| MV | Mitral valve |
| MVD | Mitral valve dysfunction |
| MVP | Mitral valve prolapse |
| OMT | Optimized medical therapy |
| PH | Pulmonary hypertension |
| PMR | Primary mitral regurgitation |
| RHD | Rheumatic heart disease |
| SAVR | Surgical aortic valve replacement |
| SCD | Sudden cardiac death |
| SMR | Secondary mitral regurgitation |
| TAVR | Transcatheter aortic valve replacement |
| TR | Tricuspid regurgitation |
| TV | Tricuspid valve |
| VHD | Valvular heart disease |
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Aluru, J.S.; Barsouk, A.; Saginala, K.; Rawla, P.; Barsouk, A. Valvular Heart Disease Epidemiology. Med. Sci. 2022, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Coffey, S.; Harper, A.R.; Cairns, B.J.; Roberts, I.S.; Prendergast, B. Clinical information has low sensitivity for postmortem diagnosis of heart valve disease. Heart 2017, 103, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Marangou, J.; Beaton, A.; Aliku, T.O.; Nunes, M.C.P.; Kangaharan, N.; Remenyi, B. Echocardiography in Indigenous Populations and Resource Poor Settings. Heart Lung Circ. 2019, 28, 1427–1435. [Google Scholar] [CrossRef] [Green Version]
- Yadgir, S.; Johnson, C.O.; Aboyans, V.; Adebayo, O.M.; Adedoyin, R.A.; Afarideh, M.; Alahdab, F.; Alashi, A.; Alipour, V.; Arabloo, J.; et al. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990–2017. Circulation 2020, 141, 1670–1680. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: Cardiovascular disease statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef]
- Meyer, A.C.; Drefahl, S.; Ahlbom, A.; Lambe, M.; Modig, K. Trends in life expectancy: Did the gap between the healthy and the ill widen or close? BMC Med. 2020, 18, 41. [Google Scholar] [CrossRef]
- Guyatt, G.H. The treatment of heart failure. A methodological review of the literature. Drugs 1986, 32, 538–568. [Google Scholar] [CrossRef]
- Cainzos-Achirica, M.; Fedeli, U.; Sattar, N.; Agyemang, C.; Jenum, A.K.; McEvoy, J.W.; Murphy, J.D.; Brotons, C.; Elosua, R.; Bilal, U.; et al. Epidemiology, risk factors, and opportunities for prevention of cardiovascular disease in individuals of South Asian ethnicity living in Europe. Atherosclerosis 2019, 286, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Edwin, F.; Zuhlke, L.; Farouk, H.; Mocumbi, A.O.; Entsua-Mensah, K.; Delsol-Gyan, D.; Bode-Thomas, F.; Brooks, A.; Cupido, B.; Tettey, M.; et al. Status and Challenges of Care in Africa for Adults with Congenital Heart Defects. World J. Pediatr. Congenit. Heart Surg. 2017, 8, 495–501. [Google Scholar] [CrossRef]
- Prendergast, B.D.; Baumgartner, H.; Delgado, V.; Gérard, O.; Haude, M.; Himmelmann, A.; Iung, B.; Leafstedt, M.; Lennartz, J.; Maisano, F.; et al. Transcatheter heart valve interventions: Where are we? Where are we going? Eur. Heart J. 2019, 40, 422–440. [Google Scholar] [CrossRef] [Green Version]
- Hahn, R.T.; Pibarot, P.; Otto, C.M. Transcatheter interventions spark a paradigm change for management of patients with mixed valve disease. Eur. Heart J. 2022, 43, 2767–2769. [Google Scholar] [CrossRef]
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zuhlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Barwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.L.; Vermeer, F.; Boersma, E.; et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef] [Green Version]
- Kearney, K.S.S.; Eiriksdottir, G.; O’Brien, K.D.; Gudnason, V.; Owens, D.S. Incidence and progression of aortic valve calcification among the elderly: A prospective analysis of the Age, Gene-Environment Susceptibility (AGES)-Reykjavik Study. Circulation 2012, 126, A17756. [Google Scholar]
- Messika-Zeitoun, D.; Bielak, L.F.; Peyser, P.A.; Sheedy, P.F.; Turner, S.T.; Nkomo, V.T.; Breen, J.F.; Maalouf, J.; Scott, C.; Tajik, A.J.; et al. Aortic valve calcification: Determinants and progression in the population. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Lyu, L.; Shen, J.; Pan, Y.; Jing, J.; Wang, Y.J.; Wei, T. Epidemiological study of calcified aortic valve stenosis in a Chinese community population. Postgrad. Med. J. 2022. [Google Scholar] [CrossRef]
- Rapezzi, C.; Giannini, F.; Campo, G. Aortic stenosis, transcatheter aortic valve replacement and transthyretin cardiac amyloidosis: Are we progressively unraveling the tangle? Eur. J. Heart Fail. 2021, 23, 259–263. [Google Scholar] [CrossRef]
- Xu, S.; Donnellan, E.; Desai, M.Y. Radiation-Associated Valvular Disease. Curr. Cardiol. Rep. 2020, 22, 167. [Google Scholar] [CrossRef] [PubMed]
- Osnabrugge, R.L.; Mylotte, D.; Head, S.J.; Van Mieghem, N.M.; Nkomo, V.T.; LeReun, C.M.; Bogers, A.J.; Piazza, N.; Kappetein, A.P. Aortic stenosis in the elderly: Disease prevalence and number of candidates for transcatheter aortic valve replacement: A meta-analysis and modeling study. J. Am. Coll. Cardiol. 2013, 62, 1002–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delesalle, G.; Bohbot, Y.; Rusinaru, D.; Delpierre, Q.; Marechaux, S.; Tribouilloy, C. Characteristics and Prognosis of Patients with Moderate Aortic Stenosis and Preserved Left Ventricular Ejection Fraction. J. Am. Heart Assoc. 2019, 8, e011036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontogeorgos, S.; Thunstrom, E.; Basic, C.; Hansson, P.O.; Zhong, Y.; Ergatoudes, C.; Morales, D.; Mandalenakis, Z.; Rosengren, A.; Caidahl, K.; et al. Prevalence and risk factors of aortic stenosis and aortic sclerosis: A 21-year follow-up of middle-aged men. Scand. Cardiovasc. J. 2020, 54, 115–123. [Google Scholar] [CrossRef]
- Yan, A.T.; Koh, M.; Chan, K.K.; Guo, H.; Alter, D.A.; Austin, P.C.; Tu, J.V.; Wijeysundera, H.C.; Ko, D.T. Association between Cardiovascular Risk Factors and Aortic Stenosis: The Canheart Aortic Stenosis Study. J. Am. Coll. Cardiol. 2017, 69, 1523–1532. [Google Scholar] [CrossRef]
- Banovic, M.; Athithan, L.; McCann, G.P. Aortic stenosis and diabetes mellitus: An ominous combination. Diabetes Vasc. Dis. Res. 2019, 16, 310–323. [Google Scholar] [CrossRef]
- Samad, Z.; Sivak, J.A.; Phelan, M.; Schulte, P.J.; Patel, U.; Velazquez, E.J. Prevalence and Outcomes of Left-Sided Valvular Heart Disease Associated with Chronic Kidney Disease. J. Am. Heart Assoc. 2017, 6, e006044. [Google Scholar] [CrossRef] [Green Version]
- Zentner, D.; Hunt, D.; Chan, W.; Barzi, F.; Grigg, L.; Perkovic, V. Prospective evaluation of aortic stenosis in end-stage kidney disease: A more fulminant process? Nephrol. Dial. Transpl. 2011, 26, 1651–1655. [Google Scholar] [CrossRef] [Green Version]
- Candellier, A.H.L.; Morelle, J.; Choukroun, G.; Jadoul, M.; Brazier, M.; Goffin, É. Aortic stenosis in patients with kidney failure: Is there an advantage for a PD-first policy? Perit. Dial. Int. 2021, 41, 158–167. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar]
- Kang, D.H.; Park, S.J.; Lee, S.A.; Lee, S.; Kim, D.H.; Kim, H.K.; Yun, S.C.; Hong, G.R.; Song, J.M.; Chung, C.H.; et al. Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis. N. Engl. J. Med. 2020, 382, 111–119. [Google Scholar] [CrossRef]
- Banovic, M.; Putnik, S.; Penicka, M.; Doros, G.; Deja, M.A.; Kockova, R.; Kotrc, M.; Glaveckaite, S.; Gasparovic, H.; Pavlovic, N.; et al. Aortic Valve ReplAcemenT versus Conservative Treatment in Asymptomatic SeveRe Aortic Stenosis: The Avatar Trial. Circulation 2021, 145, 648–658. [Google Scholar] [CrossRef]
- Alkhouli, M.; Zack, C.J.; Sarraf, M.; Bashir, R.; Nishimura, R.A.; Eleid, M.F.; Nkomo, V.T.; Sandhu, G.S.; Gulati, R.; Greason, K.L.; et al. Morbidity and Mortality Associated with Balloon Aortic Valvuloplasty: A National Perspective. Circ. Cardiovasc. Interv. 2017, 10, e004481. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risks: A Compass for Global Action. J. Am. Coll. Cardiol. 2020, 76, 2980–2981. [Google Scholar] [CrossRef]
- Andell, P.; Li, X.; Martinsson, A.; Andersson, C.; Stagmo, M.; Zoller, B.; Sundquist, K.; Smith, J.G. Epidemiology of valvular heart disease in a Swedish nationwide hospital-based register study. Heart 2017, 103, 1696–1703. [Google Scholar] [CrossRef] [Green Version]
- D’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [Green Version]
- Akinseye, O.A.P.A.; Ibebuogu, U.N. Aortic Valve Regurgitation: A Comprehensive Review. Curr. Probl. Cardiol. 2018, 43, 315–334. [Google Scholar] [CrossRef]
- Griffin, B. Valvular heart disease. In Manual of Cardiovascular Medicine, 4th ed.; Griffin, B., Callahan, T.D., Menon, V., Wu, W.M., Cauthen, C.A., Dunn, J.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Volume 1, pp. 238–355. [Google Scholar]
- Enriquez-Sarano, M.T.A.J. Aortic Regurgitation. N. Engl. J. Med. 2004, 351, 1539–1546. [Google Scholar] [CrossRef]
- Maurer, M.S.; Bokhari, S.; Damy, T.; Dorbala, S.; Drachman, B.M.; Fontana, M.; Grogan, M.; Kristen, A.V.; Lousada, I.; Nativi-Nicolau, J.; et al. Expert Consensus Recommendations for the Suspicion and Diagnosis of Transthyretin Cardiac Amyloidosis. Circ. Heart Fail. 2019, 12, e006075. [Google Scholar] [CrossRef]
- Canciello, G.; Mancusi, C.; Izzo, R.; Morisco, C.; Strisciuglio, T.; Barbato, E.; Trimarco, B.; Luca, N.; de Simone, G.; Losi, M.A. Determinants of aortic root dilatation over time in patients with essential hypertension: The Campania Salute Network. Eur. J. Prev. Cardiol. 2020, 28, 1508–1514. [Google Scholar] [CrossRef]
- Yang, L.T.; Enriquez-Sarano, M.; Michelena, H.I.; Nkomo, V.T.; Scott, C.G.; Bailey, K.R.; Oguz, D.; Ullah, M.W.; Pellikka, P.A. Predictors of Progression in Patients with Stage B Aortic Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 2480–2492. [Google Scholar] [CrossRef] [PubMed]
- Groner, A.; Qadir, A. Aortic root dilation in a child with Marfan syndrome and mosaic Turner syndrome. Cardiol. Young 2020, 30, 1976–1977. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, V.; Matura, L.A.; Sidenko, S.; Ho, V.B.; Arai, A.E.; Rosing, D.R.; Bondy, C.A. Aortic valve disease in Turner syndrome. J. Am. Coll. Cardiol. 2008, 51, 1904–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flyer, J.N.; Sleeper, L.A.; Colan, S.D.; Singh, M.N.; Lacro, R.V. Effect of Losartan or Atenolol on Children and Young Adults with Bicuspid Aortic Valve and Dilated Aorta. Am. J. Cardiol. 2021, 144, 111–117. [Google Scholar] [CrossRef]
- Groenink, M.; den Hartog, A.W.; Franken, R.; Radonic, T.; de Waard, V.; Timmermans, J.; Scholte, A.J.; van den Berg, M.P.; Spijkerboer, A.M.; Marquering, H.A.; et al. Losartan reduces aortic dilatation rate in adults with Marfan syndrome: A randomized controlled trial. Eur. Heart J. 2013, 34, 3491–3500. [Google Scholar] [CrossRef] [Green Version]
- Antunes, M.J. The Global Burden of Rheumatic Heart Disease: Population-Related Differences (It is Not All the Same!). Braz. J. Cardiovasc. Surg. 2020, 35, 958–963. [Google Scholar] [CrossRef]
- Liu, F.Z.; Xue, Y.M.; Liao, H.T.; Zhan, X.Z.; Guo, H.M.; Huang, H.L.; Fang, X.H.; Wei, W.; Rao, F.; Deng, H.; et al. Five-year epidemiological survey of valvular heart disease: Changes in morbidity, etiological spectrum and management in a cardiovascular center of Southern China. J. Thorac. Dis. 2014, 6, 1724–1730. [Google Scholar]
- Meenakshisundaram, R.; Thirumalaikolundusubramanian, P. Valvular heart disease in Indian subcontinent: Social issues. Indian J. Community Med. 2009, 34, 57–58. [Google Scholar] [CrossRef]
- Carapetis, J.R.; Steer, A.C.; Mulholland, E.K.; Weber, M. The global burden of group A streptococcal diseases. Lancet Infect. Dis. 2005, 5, 685–694. [Google Scholar] [CrossRef]
- Hull, M.C.; Morris, C.G.; Pepine, C.J.; Mendenhall, N.P. Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy. JAMA 2003, 290, 2831–2837. [Google Scholar] [CrossRef] [Green Version]
- Nestico, P.F.; Depace, N.L.; Morganroth, J.; Kotler, M.N.; Ross, J. Mitral annular calcification: Clinical, pathophysiology, and echocardiographic review. Am. Heart J. 1984, 107 Pt 1, 989–996. [Google Scholar] [CrossRef]
- Kanjanauthai, S.; Nasir, K.; Katz, R.; Rivera, J.J.; Takasu, J.; Blumenthal, R.S.; Eng, J.; Budoff, M.J. Relationships of mitral annular calcification to cardiovascular risk factors: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2010, 213, 558–562. [Google Scholar] [CrossRef] [Green Version]
- Fox, C.S.; Vasan, R.S.; Parise, H.; Levy, D.; O’Donnell, C.J.; D’Agostino, R.B.; Benjamin, E.J.; Framingham Heart, S. Mitral annular calcification predicts cardiovascular morbidity and mortality: The Framingham Heart Study. Circulation 2003, 107, 1492–1496. [Google Scholar] [CrossRef]
- Mohlenkamp, S.; Lehmann, N.; Moebus, S.; Schmermund, A.; Dragano, N.; Stang, A.; Siegrist, J.; Mann, K.; Jockel, K.H.; Erbel, R.; et al. Quantification of coronary atherosclerosis and inflammation to predict coronary events and all-cause mortality. J. Am. Coll. Cardiol. 2011, 57, 1455–1464. [Google Scholar] [CrossRef] [Green Version]
- Fox, P.; Hudson, M.; Brown, C.; Lord, S.; Gebski, V.; De Souza, P.; Lee, C.K. Markers of systemic inflammation predict survival in patients with advanced renal cell cancer. Br. J. Cancer 2013, 109, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Kato, N.; Guerrero, M.; Padang, R.; Amadio, J.M.; Eleid, M.F.; Scott, C.G.; Lee, A.T.; Pislaru, S.V.; Nkomo, V.T.; Pellikka, P.A. Prevalence and Natural History of Mitral Annulus Calcification and Related Valve Dysfunction. Mayo Clin. Proc. 2022, 97, 1094–1107. [Google Scholar] [CrossRef]
- Ezzati, M.V.H.S.; Lawes, C.M.; Leach, R.; James, W.P.; Lopez, A.D.; Rodgers, A.; Murray, C.J. Rethinking the “diseases of affluence” paradigm: Global patterns of nutritional risks in relation to economic development. PLoS Med. 2005, 2, e133. [Google Scholar] [CrossRef] [Green Version]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef]
- Martínez-Sellés, M.; García-Fernández, M.A.; Moreno, M.; Larios, E.; García-Robles, J.A.; Pinto, A. Influencia del sexo en la etiología de la insuficiencia mitral [Influence of gender on the etiology of mitral regurgitation]. Rev. Esp. Cardiol. 2006, 59, 1335–1338. [Google Scholar] [CrossRef]
- Essop, M.R. NVRanvhde, management, and prevention in Africa. Circulation 2005, 112, 3584–3591. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.Y.; Tsai, K.Z.; Lin, Y.P.; Lin, C.S.; Zeng, H.C.; Takimoto, E.; Lin, G.M. Prevalence and characteristics of mitral valve prolapse in military young adults in Taiwan of the CHIEF Heart Study. Sci. Rep. 2021, 11, 2719. [Google Scholar] [CrossRef] [PubMed]
- Dziadzko, V.; Dziadzko, M.; Medina-Inojosa, J.R.; Benfari, G.; Michelena, H.I.; Crestanello, J.A.; Maalouf, J.; Thapa, P.; Enriquez-Sarano, M. Causes and mechanisms of isolated mitral regurgitation in the community: Clinical context and outcome. Eur. Heart J. 2019, 40, 2194–2202. [Google Scholar] [CrossRef] [PubMed]
- Bakkestrøm, R.; Banke, A.; Christensen, N.L.; Pecini, R.; Irmukhamedov, A.; Andersen, M.; Borlaug, B.A.; Møller, J.E. Hemodynamic Characteristics in Significant Symptomatic and Asymptomatic Primary Mitral Valve Regurgitation at Rest and During Exercise. Circ. Cardiovasc. Imaging 2018, 11, e007171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utsunomiya, H.; Hidaka, T.; Susawa, H.; Izumi, K.; Harada, Y.; Kinoshita, M.; Itakura, K.; Masada, K.; Kihara, Y. Exercise-Stress Echocardiography and Effort Intolerance in Asymptomatic/Minimally Symptomatic Patients with Degenerative Mitral Regurgitation Combined Invasive-Noninvasive Hemodynamic Monitoring. Circ. Cardiovasc. Imaging 2018, 11, e007282. [Google Scholar] [CrossRef] [Green Version]
- Avierinos, J.-F.; Tribouilloy, C.; Grigioni, F.; Suri, R.; Barbieri, A.; Michelena, H.I.; Ionico, T.; Rusinaru, D.; Ansaldi, S.; Habib, G.; et al. Impact of ageing on presentation and outcome of mitral regurgitation due to flail leaflet: A multicentre international study. Eur. Heart J. 2013, 34, 2600–2609. [Google Scholar] [CrossRef] [Green Version]
- Grigioni, F.; Clavel, M.A.; Vanoverschelde, J.L.; Tribouilloy, C.; Pizarro, R.; Huebner, M.; Avierinos, J.F.; Barbieri, A.; Suri, R.; Pasquet, A.; et al. The MIDA Mortality Risk Score: Development and external validation of a prognostic model for early and late death in degenerative mitral regurgitation. Eur. Heart J. 2018, 39, 1281–1291. [Google Scholar] [CrossRef] [Green Version]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [Green Version]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [Green Version]
- Buzzatti, N.; Van Hemelrijck, M.; Denti, P.; Ruggeri, S.; Schiavi, D.; Scarfo, I.S.; Reser, D.; Taramasso, M.; Weber, A.; La Canna, G.; et al. Transcatheter or surgical repair for degenerative mitral regurgitation in elderly patients: A propensity-weighted analysis. J. Thorac. Cardiovasc. Surg. 2019, 158, 86–94.e1. [Google Scholar] [CrossRef]
- Sorajja, P.; Vemulapalli, S.; Feldman, T.; Mack, M.; Holmes, D.R., Jr.; Stebbins, A.; Kar, S.; Thourani, V.; Ailawadi, G. Outcomes with Transcatheter Mitral Valve Repair in the United States: An STS/ACC TVT Registry Report. J. Am. Coll. Cardiol. 2017, 70, 2315–2327. [Google Scholar] [CrossRef]
- Dejgaard, L.A.; Lie, O.H.; Helle-Valle, T.M.; Edvardsen, T.; Haugaa, K.H. Reply: Arrhythmic Mitral Annulus Disjunction and Mitral Valve Prolapse: Components of the Same Clinical Spectrum? J. Am. Coll. Cardiol. 2019, 73, 739–740. [Google Scholar] [CrossRef]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Batista, R.; Yang, L.T.; Maalouf, J.; Thapa, P.; Asirvatham, S.; Michelena, H.I.; et al. The Mitral Annular Disjunction of Mitral Valve Prolapse: Presentation and Outcome. JACC Cardiovasc. Imaging 2021, 14, 2073–2087. [Google Scholar] [CrossRef]
- Bennett, S.; Thamman, R.; Griffiths, T.; Oxley, C.; Khan, J.N.; Phan, T.; Patwala, A.; Heatlie, G.; Kwok, C.S. Mitral annular disjunction: A systematic review of the literature. Echocardiography 2019, 36, 1549–1558. [Google Scholar] [CrossRef]
- Toh, H.; Mori, S.; Izawa, Y.; Fujita, H.; Miwa, K.; Suzuki, M.; Takahashi, Y.; Toba, T.; Watanabe, Y.; Kono, A.K.; et al. Prevalence and extent of mitral annular disjunction in structurally normal hearts: Comprehensive 3D analysis using cardiac computed tomography. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 614–622. [Google Scholar] [CrossRef]
- Bharati, S.; Granston, A.S.; Liebson, P.R.; Loeb, H.S.; Rosen, K.M.; Lev, M. The conduction system in mitral valve prolapse syndrome with sudden death. Am. Heart J. 1981, 101, 667–670. [Google Scholar] [CrossRef]
- Chehab, O.; Roberts-Thomson, R.; Ling, C.N.Y.; Marber, M.; Prendergast, B.D.; Rajani, R.; Redwood, S.R. Secondary mitral regurgitation: Pathophysiology, proportionality and prognosis. Heart 2020, 106, 716–723. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Topilsky, Y.; Maltais, S.; Medina Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef]
- Wang, T.K.M.; Akyuz, K.; Mentias, A.; Kirincich, J.; Crane, A.D.; Xu, S.; Popovic, Z.B.; Xu, B.; Gillinov, A.M.; Pettersson, G.B.; et al. Contemporary Etiologies, Outcomes, and Novel Risk Score for Isolated Tricuspid Regurgitation. JACC Cardiovasc. Imaging 2022, 15, 731–744. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Bohbot, Y.; Chadha, G.; Delabre, J.; Landemaine, T.; Beyls, C.; Tribouilloy, C. Characteristics and prog- nosis of patients with significant tricuspid regur- gitation. Arch. Cardiovasc. Dis. 2019, 112, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Muraru, D.; Addetia, K.; Guta, A.C.; Ochoa-Jimenez, R.C.; Genovese, D.; Veronesi, F.; Basso, C.; Iliceto, S.; Badano, L.; Lang, R. Right atrial volume is a major determinant of tricuspid annulus area in func- tional tricuspid regurgitation: A three-dimensional echocardiographic study. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Addetia, K.; Harb, S.C.; Hahn, R.T.; Kapadia, S.; Lang, R.M. Cardiac Implantable Electronic Device Lead-Induced Tricuspid Regurgitation. JACC Cardiovasc. Imaging 2019, 12, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Maisano, F. Transcatheter tricuspid valve intervention: State of the art. EuroIntervention 2017, 13, AA40–AA50. [Google Scholar] [CrossRef] [PubMed]
- Rodés-Cabau, J.; Hahn, R.T.; Latib, A.; Laule, M.; Lauten, A.; Maisano, F.; Schofer, J.; Campelo-Parada, F.; Puri, R.; Vahanian, A. Transcatheter Therapies for Treating Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2016, 67, 1829–1845. [Google Scholar] [CrossRef]
- Nickenig, G.; Weber, M.; Schuler, R.; Hausleiter, J.; Nabauer, M.; von Bardeleben, R.S.; Sotiriou, E.; Schafer, U.; Deuschl, F.; Alessandrini, H.; et al. Tricuspid valve repair with the Cardioband system: Two-year outcomes of the multicentre, prospective TRI-REPAIR study. EuroIntervention 2021, 16, e1264–e1271. [Google Scholar] [CrossRef]
- Praz, F.; Muraru, D.; Kreidel, F.; Lurz, P.; Hahn, R.T.; Delgado, V.; Senni, M.; von Bardeleben, R.S.; Nickenig, G.; Hausleiter, J.; et al. Transcatheter treatment for tricuspid valve disease. EuroIntervention 2021, 17, 791–808. [Google Scholar] [CrossRef]
- Iung, B.; Baron, G.; Tornos, P.; Gohlke-Barwolf, C.; Butchart, E.G.; Vahanian, A. Valvular heart disease in the community: A European experience. Curr. Probl. Cardiol. 2007, 32, 609–661. [Google Scholar] [CrossRef]
- Tribouilloy, C.; Bohbot, Y.; Kubala, M.; Ruschitzka, F.; Popescu, B.; Wendler, O.; Laroche, C.; Bartha, E.; Ince, H.; Simkova, I.; et al. Characteristics, management, and outcomes of patients with multiple native valvular heart disease: A substudy of the EURObservational Research Programme Valvular Heart Disease II Survey. Eur. Heart J. 2022, 43, 2756–2766. [Google Scholar] [CrossRef]
- Unger, P.; Tribouilloy, C. Aortic Stenosis with Other Concomitant Valvular Disease: Aortic Regurgitation, Mitral Regurgitation, Mitral Stenosis, or Tricuspid Regurgitation. Cardiol. Clin. 2020, 38, 33–46. [Google Scholar] [CrossRef]
- Goncalves, A.; Marcos-Alberca, P.; Almeria, C.; Feltes, G.; Rodriguez, E.; Hernandez-Antolin, R.A.; Garcia, E.; Maroto, L.; Perez, C.F.; Cardoso, J.C.S.; et al. Acute left ventricle diastolic function improvement after transcatheter aortic valve implantation. Eur. J. Echocardiogr. 2011, 12, 790–797. [Google Scholar] [CrossRef] [Green Version]
- Tamargo, M.; Obokata, M.; Reddy, Y.N.V.; Pislaru, S.V.; Lin, G.; Egbe, A.C.; Nishimura, R.A.; Borlaug, B.A. Functional mitral regurgitation and left atrial myopathy in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2020, 22, 489–498. [Google Scholar] [CrossRef]
- Quesada, R. The Treatment of Severe Aortic Stenosis in the Presence of Mitral Regurgitation: There Is Much to Be Learned. Revasc. Med. 2021, 32, 41–42. [Google Scholar] [CrossRef]
- Benfari, G.; Setti, M.; Nistri, S.; Fanti, D.; Maffeis, C.; Tafciu, E.; Pighi, M.; Cicoira, M.; Ribichini, F.L.; Rossi, A. Relevance of Functional Mitral Regurgitation in Aortic Valve Stenosis. Am. J. Cardiol. 2020, 136, 115–121. [Google Scholar] [CrossRef]
- Arshad, H.B.; Minhas, A.M.K.; Khan, S.U.; Nasir, K.; Rao, N.; Thacker, S.; Butt, S.A.; Faza, N.; Little, S.H.; von Ballmoos, M.W.; et al. National Trends and Outcomes of Surgical Aortic Valve Replacement with Concomitant Mitral Valve Surgery. Cardiovasc. Revasc. Med. 2022, 40, 13–19. [Google Scholar] [CrossRef]
- Barbanti, M.; Webb, J.; Hahn, R.T.; Feldman, T.; Boone, R.H.; Smith, C.R.; Kodali, S.; Zajarias, A.; Thompson, C.; Green, P.; et al. Impact of preoperative moderate/severe mitral regurgitation on 2-year outcome after trans- catheter and surgical aortic valve replacement: Insight from the Placement of Aortic Transcatheter Valve (PARTNER) Trial Cohort A. Circulation 2013, 128, 2776–2784. [Google Scholar] [CrossRef] [Green Version]
- Lindman, B.R.; Dweck, M.R.; Lancellotti, P.; Genereux, P.; Pierard, L.A.; O’Gara, P.T.; Bonow, R.O. Management of Asymptomatic Severe Aortic Stenosis: Evolving Concepts in Timing of Valve Replacement. JACC Cardiovasc. Imaging 2020, 13, 481–493. [Google Scholar] [CrossRef]
- Agricola, E.; Ancona, F.; Brochet, E.; Donal, E.; Dweck, M.; Faletra, F.; Lancellotti, P.; Mahmoud-Elsayed, H.; Marsan, N.A.; Maurovich-Hovart, P.; et al. The structural heart disease interventional imager rationale, skills and training: A position paper of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 471–479. [Google Scholar] [CrossRef]
- Chambers, J.B.; Lancellotti, P. Heart Valve Clinics, Centers, and Networks. Cardiol. Clin. 2020, 38, 65–74. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef]
- Badheka, A.O.; Patel, N.J.; Panaich, S.S.; Patel, S.V.; Jhamnani, S.; Singh, V.; Pant, S.; Patel, N.; Patel, N.; Arora, S.; et al. Effect of Hospital Volume on Outcomes of Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2015, 116, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Magne, J.; Dulgheru, R.; Clavel, M.A.; Donal, E.; Vannan, M.A.; Chambers, J.; Rosenhek, R.; Habib, G.; Lloyd, G.; et al. Outcomes of patients with asymptomatic aortic stenosis followed up in Heart valve clinics. JAMA Cardiol. 2018, 3, 1060–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, J.B.; Prendergast, B.; Iung, B.; Rosenhek, R.; Zamorano, J.L.; Pierard, L.A.; Modine, T.; Falk, V.; Kappetein, A.P.; Pibarot, P.; et al. Standards defining a ‘Heart Valve Centre’: ESC Working Group on Valvular Heart Disease and European Association for Cardiothoracic Surgery Viewpoint. Eur. Heart J. 2017, 38, 2177–2183. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, R.A.; O’Gara, P.T.; Bavaria, J.E.; Brindis, R.G.; Carroll, J.D.; Kavinsky, C.J.; Lindman, B.R.; Linderbaum, J.A.; Little, S.H.; Mack, M.J.; et al. 2019 AATS/ACC/ASE/SCAI/STS Expert Consensus Systems of Care Document: A Proposal to Optimize Care for Patients with Valvular Heart Disease: A Joint Report of the American Association for Thoracic Surgery, American College of Cardiology, American Society of Echocardiography, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2019, 73, 2609–2635. [Google Scholar] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Valvulopathy | Etiology | Anatomy | Prevalence | Risk Factors |
|---|---|---|---|---|
| Aortic Stenosis | Degenerative (81.9%), rheumatic (11.2%), Congenital (5.6%), post-endocarditis (1.3%) | CAVD: Aspecific Bicuspid valve: fusion between right and left leaflets is the most common Rheumatic: commissural fusion | 3.4% in the elderly | Aging, hypertension, diabetes, chronic kidney disease |
| Aortic regurgitation | Congenital bicuspid AV, calcific degeneration, rheumatic disease (in developing countries), myxomatous degeneration | Type I: aortic root dilatation + coaptation defect Type II: leaflet prolapse Type III: leaflets degeneration and retraction | 1.6% in UK elders aged >65 years old; 4.9% of participants in the US Framingham study | Hypertension, aging, Marfan syndrome, Turner’s syndrome |
| Mitral Regurgitation | Primary: endocarditis, degenerative, papillary muscle rupture. Secondary: ischemic, dilated cardiomyopathy, atrial enlargement caused by AF | Type I: normal leaflet motion Type II: excessive leaflet motion Type III: restricted leaflet motion IIIa: leaflet motion restricted in both systole and diastole. IIIb: leaflet motion restricted in diastole | up to 10% of the general population; mitral valve prolapse: 3% of the general population. | Myxomatous degeneration (in the younger population), fibroelastic deficiency disease (in the elderly), LV dysfunction, LA dilatation |
| Tricuspid Regurgitation | Primary: endocarditis, degenerative, prosthetic valve failure, implantable device-related Secondary: left heart disease, atrial functional, pulmonary disease, right heart disease. | -annular dilatation -leaflet tethering, leaflet restriction | 4% | Aging, atrial arrythmias, pulmonary hypertension, RV dysfunction, lead in the right ventricle. |
| Valve Disease | Follow-Up | Medical Therapy | Intervention |
|---|---|---|---|
| Aortic Stenosis | Mild: every 3–5 y Moderate: every 1–2 y Severe: every 6–12 mo | N.A. | Severe AS in symptomatic patients or asymptomatic patients with LV systolic dysfunction or a positive stress test
|
| Aortic Regurgitation | Mild: every 3–5 y Moderate: every 1–2 y Severe: every 6–12 mo |
|
|
| Mitral Regurgitation | Mild: every 3–5 y Moderate: every 1–2 y Severe: every 6–12 mo |
|
|
| Tricuspid Regurgitation | Non-specific follow-up period. |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santangelo, G.; Bursi, F.; Faggiano, A.; Moscardelli, S.; Simeoli, P.S.; Guazzi, M.; Lorusso, R.; Carugo, S.; Faggiano, P. The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management. J. Clin. Med. 2023, 12, 2178. https://doi.org/10.3390/jcm12062178
Santangelo G, Bursi F, Faggiano A, Moscardelli S, Simeoli PS, Guazzi M, Lorusso R, Carugo S, Faggiano P. The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management. Journal of Clinical Medicine. 2023; 12(6):2178. https://doi.org/10.3390/jcm12062178
Chicago/Turabian StyleSantangelo, Gloria, Francesca Bursi, Andrea Faggiano, Silvia Moscardelli, Pasquale Simone Simeoli, Marco Guazzi, Roberto Lorusso, Stefano Carugo, and Pompilio Faggiano. 2023. "The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management" Journal of Clinical Medicine 12, no. 6: 2178. https://doi.org/10.3390/jcm12062178