
Clinical Outcomes of the Intraocular Lens Injector and Busin Glide for Descemet Stripping Automated Endothelial Keratoplasty in Patients with Iridocorneal Endothelial Syndrome
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alvarado, J.A.; Murphy, C.G.; Maglio, M.; Hetherington, J. Pathogenesis of Chandler’s syndrome, essential iris atrophy and the Cogan-Reese syndrome. I. Alterations of the corneal endothelium. Investig. Ophthalmol. Vis. Sci. 1986, 27, 853–872. [Google Scholar]
- Shields, M.B.; Campbell, D.G.; Simmons, R.J. The essential iris atrophies. Am. J. Ophthalmol. 1978, 85, 749–759. [Google Scholar] [CrossRef]
- Shields, M.B. Progressive essential iris atrophy, Chandler’s syndrome, and the iris nevus (Cogan-Reese) syndrome: A spectrum of disease. Surv. Ophthalmol. 1979, 24, 3–20. [Google Scholar] [CrossRef]
- Doe, E.A.; Budenz, D.L.; Gedde, S.J.; Imami, N.R. Long-term surgical outcomes of patients with glaucoma secondary to the iridocorneal endothelial syndrome. Ophthalmology 2001, 108, 1789–1795. [Google Scholar] [CrossRef]
- Silva, L.; Najafi, A.; Suwan, Y.; Teekhasaenee, C.; Ritch, R. The iridocorneal endothelial syndrome. Surv. Ophthalmol. 2018, 63, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Walkden, A.; Au, L. Iridocorneal endothelial syndrome: Clinical perspectives. Clin. Ophthalmol. 2018, 12, 657–664. [Google Scholar] [CrossRef] [Green Version]
- Sorkin, N.; Einan-Lifshitz, A.; Boutin, T.; Showail, M.; Borovik, A.; Chan, C.C.; Rootman, D.S. Descemet membrane endothelial keratoplasty in iridocorneal endothelial syndrome and posterior polymorphous corneal dystrophy. Can. J. Ophthalmol. 2019, 54, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, M.; Downward, L.; Curnow, E.; Larkin, D.F.; Tuft, S.J. Graft Survival After Penetrating and Endothelial Keratoplasty in Iridocorneal Endothelial Syndrome. Cornea 2020, 39, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, M.A.; Hollick, E.J. Descemet Stripping Endothelial Keratoplasty in Iridocorneal Endothelial Syndrome: Postoperative Complications and Long-Term Outcomes. Cornea 2015, 34, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Park, C.Y.; Lee, J.K.; Gore, P.K.; Lim, C.Y.; Chuck, R.S. Keratoplasty in the United States: A 10-Year Review from 2005 through 2014. Ophthalmology 2015, 122, 2432–2442. [Google Scholar] [CrossRef]
- Quek, D.T.; Wong, C.W.; Wong, T.T.; Han, S.B.; Htoon, H.M.; Ho, C.L.; Tan, D.T.; Price, F.W., Jr.; Price, M.O.; Mehta, J.S. Graft failure and intraocular pressure control after keratoplasty in iridocorneal endothelial syndrome. Am. J. Ophthalmol. 2015, 160, 422–429.e1. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Calhoun, P.; Kollman, C.; Price, F.W., Jr.; Lass, J.H. Descemet Stripping Endothelial Keratoplasty: Ten-Year Endothelial Cell Loss Compared with Penetrating Keratoplasty. Ophthalmology 2016, 123, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Ao, M.; Feng, Y.; Xiao, G.; Xu, Y.; Hong, J. Clinical outcome of Descemet stripping automated endothelial keratoplasty in 18 cases with iridocorneal endothelial syndrome. Eye 2018, 32, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Khor, W.B.; Teo, K.Y.; Mehta, J.S.; Tan, D.T. Descemet stripping automated endothelial keratoplasty in complex eyes: Results with a donor insertion device. Cornea 2013, 32, 1063–1068. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.S.; Chua, J.; Poh, R.; Beuerman, R.W.; Tan, D. Primary graft failure after Descemet-stripping automated endothelial keratoplasty: Clinico-pathological study. Cornea 2008, 27, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Tsatsos, M.; Athanasiadis, I.; Kopsachilis, N.; Krishnan, R.; Hossain, P.; Anderson, D. Comparison of the Endosaver with noninjector techniques in Descemet’s stripping endothelial keratoplasty. Indian J. Ophthalmol. 2017, 65, 1133–1137. [Google Scholar]
- Terry, M.A.; Straiko, M.D.; Goshe, J.M.; Shamie, N.; Shah, A.; Alqudah, A.A.; Davis-Boozer, D. Endothelial keratoplasty: Prospective, randomized, masked clinical trial comparing an injector with forceps for tissue insertion. Am. J. Ophthalmol. 2013, 156, 61–68.e3. [Google Scholar] [CrossRef] [PubMed]
- Gangwani, V.; Obi, A.; Hollick, E.J. A prospective study comparing EndoGlide and Busin glide insertion techniques in descemet stripping endothelial keratoplasty. Am. J. Ophthalmol. 2012, 153, 38–43.e1. [Google Scholar] [CrossRef] [PubMed]
- Soma, T.; Koh, S.; Oie, Y.; Maruyama, K.; Tsujikawa, M.; Kawasaki, S.; Maeda, N.; Nishida, K. Clinical evaluation of a newly developed graft inserter (NS Endo-Inserter) for Descemet stripping automated endothelial keratoplasty. Clin. Ophthalmol. 2019, 13, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Sacchetti, M.; Mantelli, F.; Marenco, M.; Macchi, I.; Ambrosio, O.; Rama, P. Diagnosis and Management of Iridocorneal Endothelial Syndrome. Biomed. Res. Int. 2015, 2015, 763093. [Google Scholar] [CrossRef] [Green Version]
- Akanda, Z.Z.; Naeem, A.; Russell, E.; Belrose, J.; Si, F.F.; Hodge, W.G. Graft rejection rate and graft failure rate of penetrating keratoplasty (PKP) vs. lamellar procedures: A systematic review. PLoS ONE 2015, 10, e0119934. [Google Scholar] [CrossRef] [PubMed]
- McCarey, B.E.; Edelhauser, H.F.; Lynn, M.J. Review of corneal endothelial specular microscopy for FDA clinical trials of refractive procedures, surgical devices, and new intraocular drugs and solutions. Cornea 2008, 27, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Calvo-de-Mora, M.; Quilendrino, R.; Ham, L.; Liarakos, V.S.; van Dijk, K.; Baydoun, L.; Dapena, I.; Oellerich, S.; Melles, G.R. Clinical outcome of 500 consecutive cases undergoing Descemet’s membrane endothelial keratoplasty. Ophthalmology 2015, 122, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Price, F.W., Jr. Descemet stripping with endothelial keratoplasty for treatment of iridocorneal endothelial syndrome. Cornea 2007, 26, 493–497. [Google Scholar] [CrossRef]
- Hong, Y.; Peng, R.M.; Wang, M.; Qu, H.Q.; Hong, J. Suture pull-through insertion techniques for Descemet stripping automated endothelial keratoplasty in Chinese phakic eyes: Outcomes and complications. PLoS ONE 2013, 8, e61929. [Google Scholar] [CrossRef]
- Groat, B.Y.M.; Vroman, D.T.; Fernandez dC, L.E. Descemet-Stripping Automated Endothelial Keratoplasty Technique in Patients with Anterior Chamber Intraocular Lenses. Br. J. Ophthalmol. 2007, 91, 714. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, Y.; Uno, T.; Shisida, K.; Xue, L.; Shiraishi, A.; Zheng, X.; Ohashi, Y. Demonstration of aqueous streaming through a laser iridotomy window against the corneal endothelium. Arch. Ophthalmol. 2006, 124, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, M.A.; Saad, H.A.; Shamie, N.; Chen, E.S.; Phillips, P.M.; Friend, D.J.; Holiman, J.D.; Stoeger, C. Endothelial keratoplasty: The influence of insertion techniques and incision size on donor endothelial survival. Cornea 2009, 28, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, J.S.; Por, Y.M.; Poh, R.; Beuerman, R.W.; Tan, D. Comparison of donor insertion techniques for descemet stripping automated endothelial keratoplasty. Arch. Ophthalmol. 2008, 126, 1383–1388. [Google Scholar] [CrossRef] [Green Version]
- Ang, M.; Mehta, J.S.; Anshu, A.; Wong, H.K.; Htoon, H.M.; Tan, D. Endothelial cell counts after Descemet’s stripping automated endothelial keratoplasty versus penetrating keratoplasty in Asian eyes. Clin. Ophthalmol. 2012, 6, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Chaurasia, S.; Ramappa, M.; Garg, P.; Murthy, S.I.; Senthil, S.; Sangwan, V.S. Endothelial keratoplasty in the management of irido-corneal endothelial syndrome. Eye 2013, 27, 564–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rooij, J.; Engel, A.; Remeijer, L.; van Cleijnenbreugel, H.; Wubbels, R. Long-Term Functional and Anatomical Outcome after Descemet Stripping Automated Endothelial Keratoplasty: A Prospective Single-Center Study. J. Ophthalmol. 2018, 2018, 7320816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.; Wang, Y.; Ji, J.; Gao, N.; Chen, J. Deep lamellar endothelial keratoplasty for iridocorneal endothelial syndrome in phakic eyes. Arch. Ophthalmol. 2009, 127, 33–36. [Google Scholar] [CrossRef] [Green Version]
- Nahum, Y.; Mimouni, M.; Busin, M. Risk Factors Predicting the Need for Graft Exchange After Descemet Stripping Automated Endothelial Keratoplasty. Cornea 2015, 34, 876–879. [Google Scholar] [CrossRef] [PubMed]
- Anshu, A.; Price, M.O.; Price, F.W. Descemet’s stripping endothelial keratoplasty: Long-term graft survival and risk factors for failure in eyes with preexisting glaucoma. Ophthalmology 2012, 119, 1982–1987. [Google Scholar] [CrossRef] [PubMed]
- Decroos, F.C.; Delmonte, D.W.; Chow, J.H.; Stinnett, S.S.; Kim, T.; Carlson, A.N.; Afshari, N.A. Increased Rates of Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK) Graft Failure and Dislocation in Glaucomatous Eyes with Aqueous Shunts. J. Ophthalmic Vis. Res. 2012, 7, 203–213. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Injector (n = 12) | Busin Glide (n = 12) | p Value | |
|---|---|---|---|
| Age (years) | 55.00 ± 10.55 | 52.84 ± 18.00 | 0.723 |
| Sex (male/female) | 5/7 | 6/6 | 0.682 |
| Preoperative BCVA (LogMAR) | 0.91 ± 0.68 | 1.08 ± 0.53 | 0.512 |
| History of glaucoma surgery | 2 (16.67%) | 1 (8.33%) | 0.537 |
| History of keratoplasty | 0 | 1 (8.33%) | 0.307 |
| Donor endothelial cell count (cells/mm2) | 3003 ± 398 | 3144 ± 291 | 0.334 |
| Type of surgery | |||
| DSAEK alone | 4 (33.33%) | 4 (33.33%) | 1.000 |
| DSAEK + cataract surgery + IOL | 8 (66.67%) | 8 (66.67%) | 1.000 |
| Injector (n = 12) | Busin Glide (n = 12) | p Value | |
|---|---|---|---|
| Donor ECD (cells/mm2) | 3003 ± 398 | 3144 ± 291 | 0.334 |
| ECD at 1 month (cells/mm2) | 2341 ± 519 | 2095 ± 393 | 0.203 |
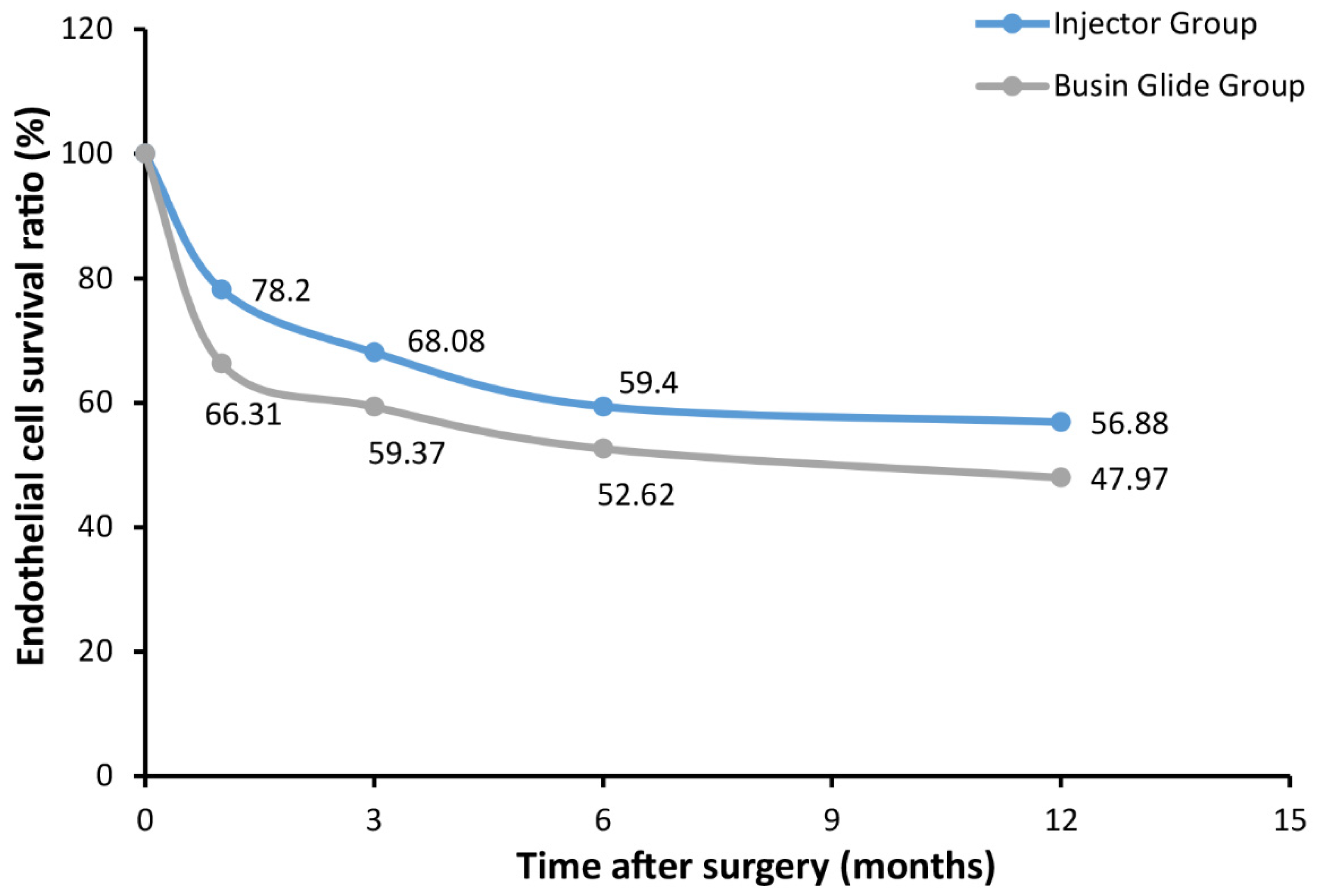
| ECL at 1 month (%) | 21.80 ± 15.01 | 33.69 ± 9.75 | 0.031 |
| ECD at 3 months (cells/mm2) | 2039 ± 487 | 1874 ± 374 | 0.364 |
| ECL at 3 months (%) | 31.92 ± 15.29 | 40.63 ± 10.23 | 0.115 |
| ECD at 6 months (cells/mm2) | 1787 ± 501 | 1669 ± 481 | 0.561 |
| ECL at 6 months (%) | 40.60 ± 14.29 | 47.38 ± 13.60 | 0.247 |
| ECD at 12 months (cells/mm2) | 1713 ± 557 | 1521 ± 471 | 0.370 |
| ECL at 12 months (%) | 43.12 ± 16.03 | 52.03 ± 13.34 | 0.153 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Liu, Z.; Sun, B.; Zhao, Z.; Wang, H.; Zheng, Q.; Chen, W. Clinical Outcomes of the Intraocular Lens Injector and Busin Glide for Descemet Stripping Automated Endothelial Keratoplasty in Patients with Iridocorneal Endothelial Syndrome. J. Clin. Med. 2023, 12, 1856. https://doi.org/10.3390/jcm12051856
Li S, Liu Z, Sun B, Zhao Z, Wang H, Zheng Q, Chen W. Clinical Outcomes of the Intraocular Lens Injector and Busin Glide for Descemet Stripping Automated Endothelial Keratoplasty in Patients with Iridocorneal Endothelial Syndrome. Journal of Clinical Medicine. 2023; 12(5):1856. https://doi.org/10.3390/jcm12051856
Chicago/Turabian StyleLi, Saiqing, Zihao Liu, Binjia Sun, Zelin Zhao, Haiou Wang, Qinxiang Zheng, and Wei Chen. 2023. "Clinical Outcomes of the Intraocular Lens Injector and Busin Glide for Descemet Stripping Automated Endothelial Keratoplasty in Patients with Iridocorneal Endothelial Syndrome" Journal of Clinical Medicine 12, no. 5: 1856. https://doi.org/10.3390/jcm12051856