
Comparison of Microbial Sampling Sites and Donor-Related Factors on Corneal Graft Contamination

Abstract
:1. Introduction
2. Materials and Methods
2.1. History and Contamination Rate Analysis
2.2. Donor-Associated Factor Collection
2.3. Donation Surgery and Microbial Sampling
2.4. Microbiological Identification
2.5. Statistical Analysis
3. Results
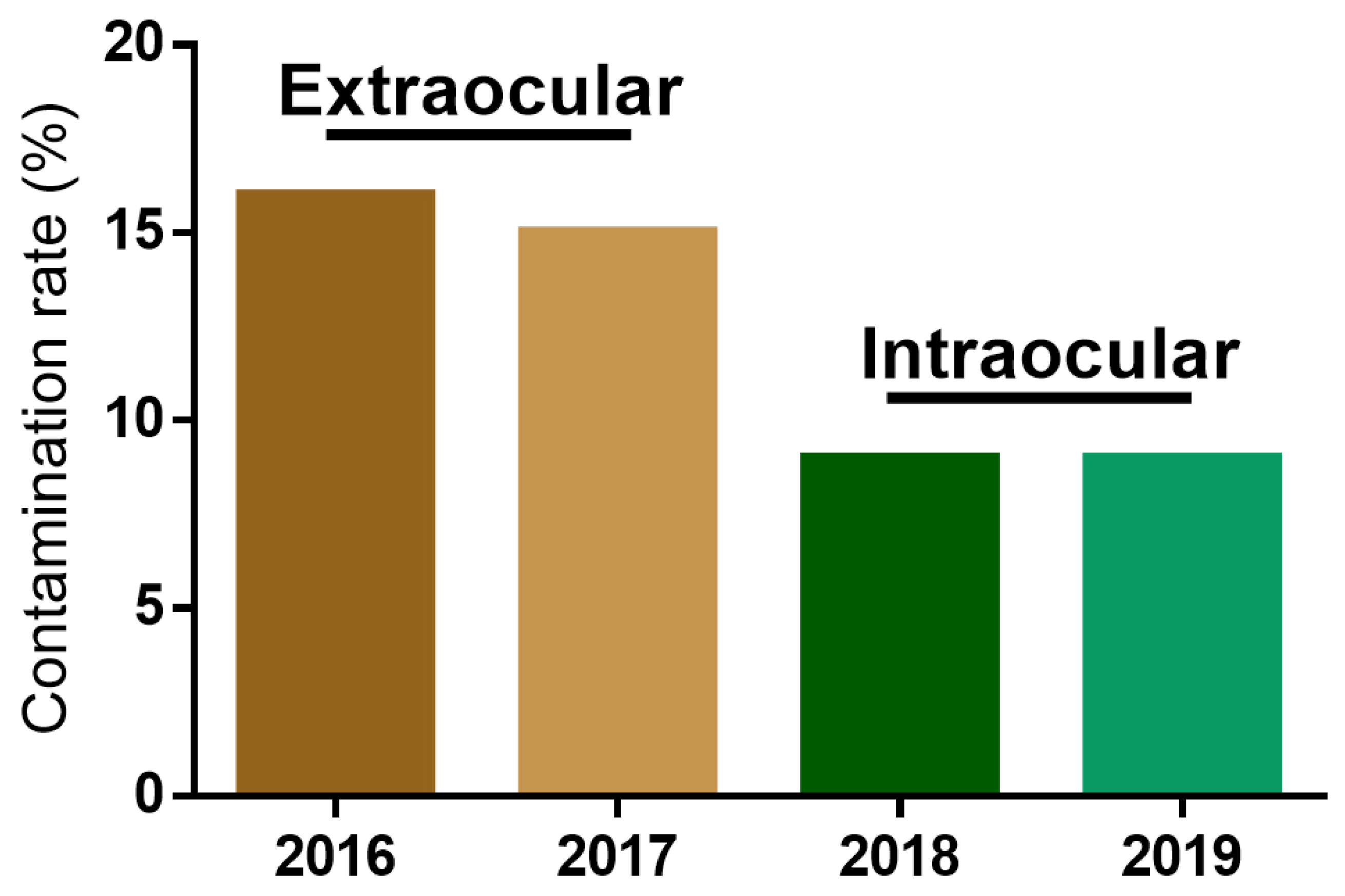
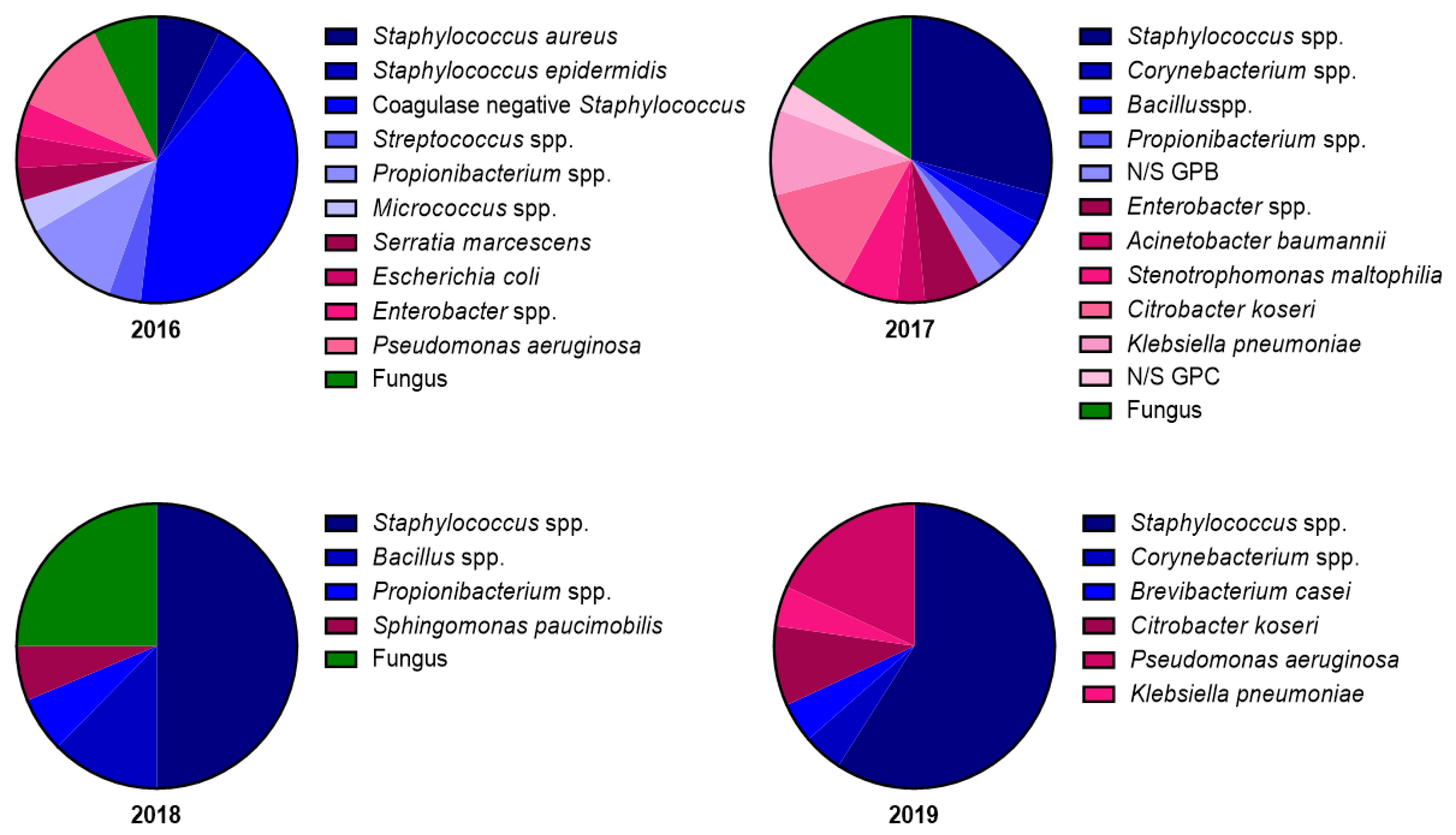
3.1. Changes in Contamination Rate and Microbial Strain Composition after Modification of the Microbial Sampling Site
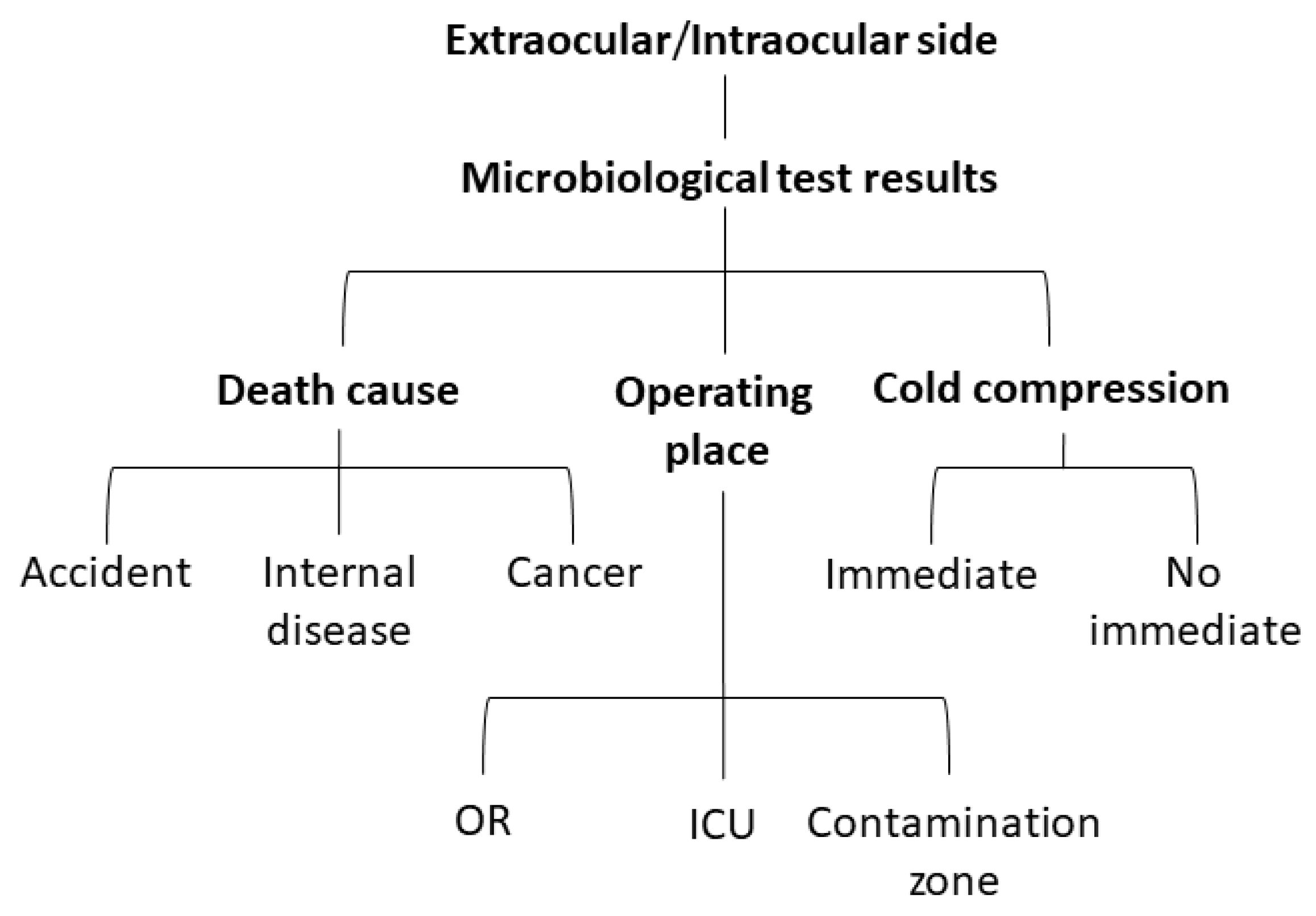
3.2. Comparison of Microbial Sampling Site and Classification of Donor-Associated Factors
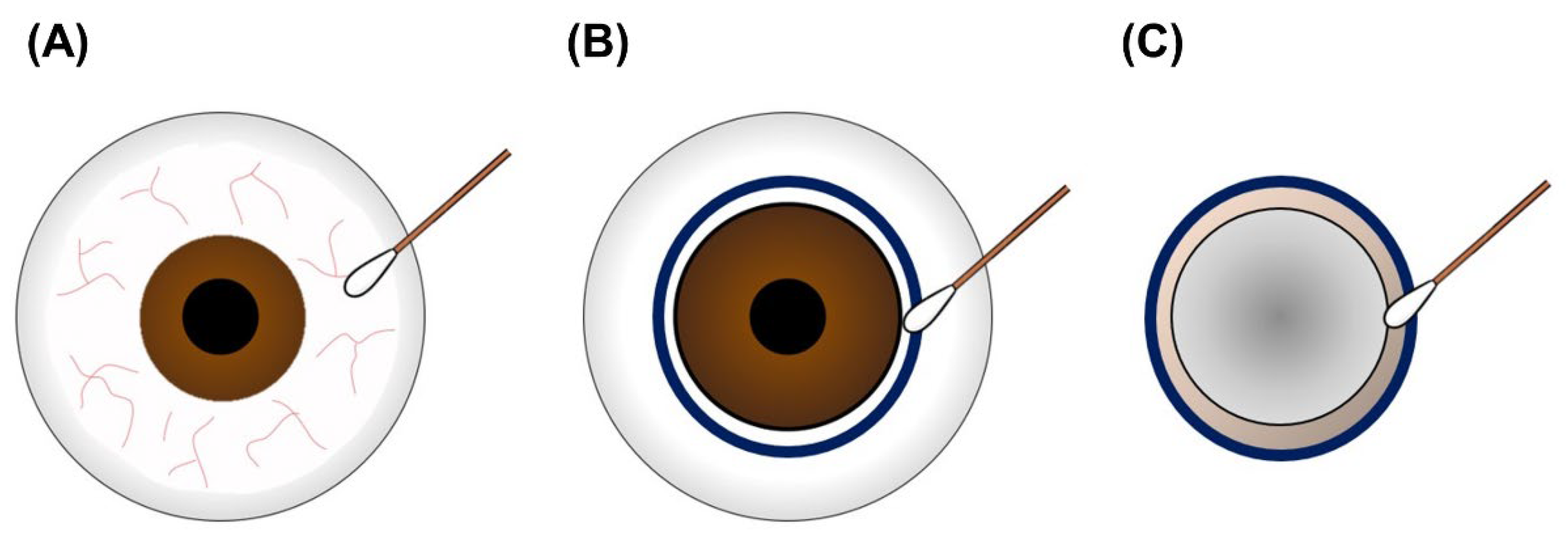
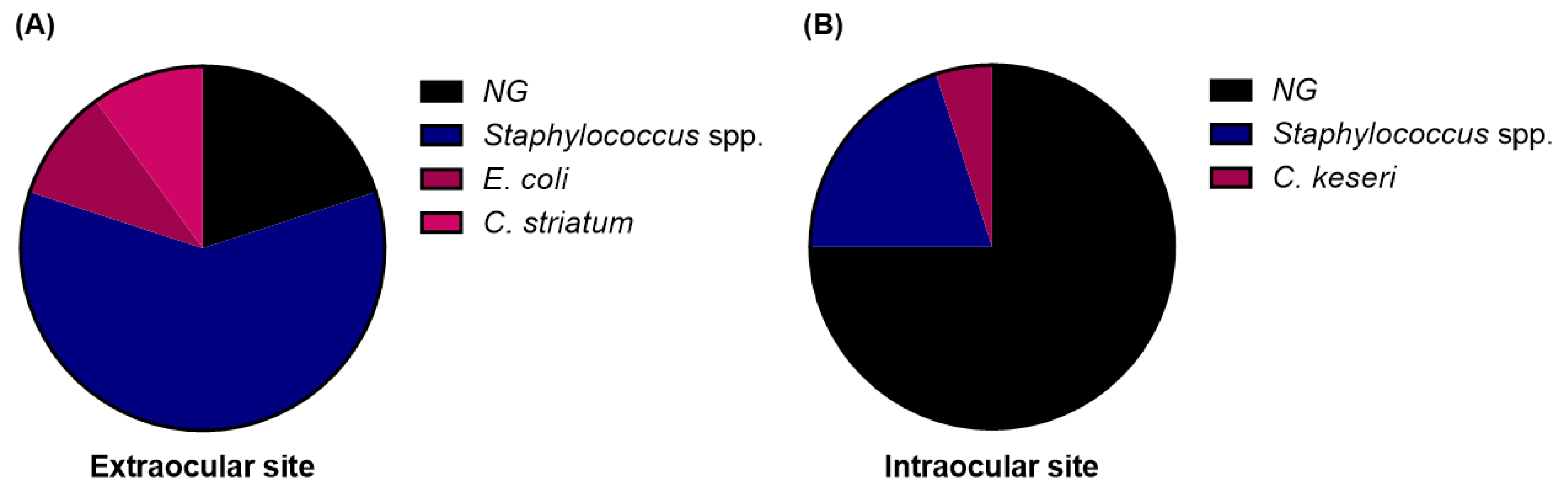
3.3. Sampling at the Extraocular Side of the Corneoscleral Rim Revealed Higher Sensitivity than That at the Intraocular Side
3.4. Difference in Sampling Results Is Not Caused by Donor-Associated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keyhani, K.; Seedor, J.A.; Shah, M.K.; Terraciano, A.J.; Ritterband, D.C. The incidence of fungal keratitis and endophthalmitis following penetrating keratoplasty. Cornea 2005, 24, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Jones, M.N.; Srinivasan, S.; Neal, T.J.; Armitage, W.J.; Kaye, S.B.; Group, N.O.T.A. Endophthalmitis after penetrating keratoplasty. Ophthalmology 2015, 122, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Gruenert, A.K.; Rosenbaum, K.; Geerling, G.; Fuchsluger, T.A. The influence of donor factors on corneal organ culture contamination. Acta Ophthalmol. 2017, 95, 733–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, L.; Errani, P.G.; Zerbinati, A.; Musacchi, Y.; Di Pede, B.; Tassinari, G. Frequency of positive donor rim cultures after penetrating keratoplasty using hypothermic and organ-cultured donor corneas. Cornea 2007, 26, 552–556. [Google Scholar] [CrossRef]
- Borowsky, C.M.; Wallau, A.D.; Reetz, A.; Kwitko, S.; Rymer, S.; Locatelli, C.I. Positive corneoscleral rim culture in penetrating keratoplasty at the Porto Alegre Clinical Hospital. Arq. Bras. Oftalmol. 2008, 71, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Schroeter, J.; Wilkemeyer, I.; Herrlinger, F.; Pruss, A. Comparison of in situ corneoscleral disc excision versus whole globe enucleation in cornea donors regarding microbial contamination in organ culture medium—A prospective monocentric study over 9 years. Transfus. Med. Hemother. 2012, 39, 391–394. [Google Scholar] [CrossRef]
- Spelsberg, H.; Reinhard, T.; Sengler, U.; Daeubener, W.; Sundmacher, R. Organ-cultured corneal grafts from septic donors: A retrospective study. Eye 2002, 16, 622–627. [Google Scholar] [CrossRef]
- Hassan, S.S.; Wilhelmus, K.R.; Dahl, P.; Davis, G.C.; Roberts, R.T.; Ross, K.W.; Varnum, B.H.; Medical Review Subcommittee of the Eye Bank Association of America. Infectious disease risk factors of corneal graft donors. Arch. Ophthalmol. 2008, 126, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Linke, S.J.; Fricke, O.H.; Eddy, M.-T.; Bednarz, J.; Druchkiv, V.; Kaulfers, P.-M.; Wulff, B.; Püschel, K.; Richard, G.; Hellwinkel, O.J. Risk factors for donor cornea contamination: Retrospective analysis of 4546 procured corneas in a single eye bank. Cornea 2013, 32, 141–148. [Google Scholar] [CrossRef]
- EBAA. Procedures Manual; EBAA: Washington, DC, USA, 1992. [Google Scholar]
- Gupta, N.; Vashist, P.; Ganger, A.; Tandon, R.; Gupta, S.K. Eye donation and eye banking in India. Natl. Med. J. India 2018, 31, 283–286. [Google Scholar] [CrossRef]
- Wang, Y.-J.; Li, S.-C.; Lin, W.-C.; Huang, F.-C. Intracellular Microbiome Profiling of the Acanthamoeba Clinical Isolates from Lens Associated Keratitis. Pathogens 2021, 10, 266. [Google Scholar] [CrossRef]
- Wilhelmus, K.R.; Hassan, S.S. The prognostic role of donor corneoscleral rim cultures in corneal transplantation. Ophthalmology 2007, 114, 440–445. [Google Scholar] [CrossRef]
- Khouani, M.; Debellemanière, G.; Malugani, C.; Gauthier, A.S.; Pouthier, F.; Delbosc, B.; Saleh, M. Evaluation of microbial contamination of corneal transplants: One-year report from a French regional eye bank. Cornea 2014, 33, 899–904. [Google Scholar] [CrossRef]
- Hermel, M.; Salla, S.; Hamsley, N.; Steinfeld, A.; Walter, P. Detection of contamination during organ culture of the human cornea. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 248, 117–126. [Google Scholar] [CrossRef]
- Röck, T.; Landenberger, J.; Buhl, M.; Yoeruek, E.; Bartz-Schmidt, K.U.; Bramkamp, M.; Blumenstock, G.; Röck, D. Factors influencing the contamination rates of the conjunctival swabs and organ culture media of human donor eyes. Medicine 2018, 97, e11879. [Google Scholar] [CrossRef]
- Robert, P.-Y.; Camezind, P.; Drouet, M.; Ploy, M.-C.; Adenis, J.-P. Internal and external contamination of donor corneas before in situ excision: Bacterial risk factors in 93 donors. Graefe’s Arch. Clin. Exp. Ophthalmol. 2002, 240, 265–270. [Google Scholar] [CrossRef]
- Parekh, M.; Borroni, D.; Romano, V.; Kaye, S.B.; Camposampiero, D.; Ponzin, D.; Ferrari, S. Next-generation sequencing for the detection of microorganisms present in human donor corneal preservation medium. BMJ Open Ophthalmol. 2019, 4, e000246. [Google Scholar] [CrossRef] [Green Version]
- Graham, J.; Moore, J.; Xu, J.; Goodall, E.; Dooley, J.; Dartt, D.; Downes, S.; Moore, T. Pathogen or commensal: A PCR based study of ocular surface bacteria in normal and dry eyes. Acta Ophthalmol. Scand. 2007, 85, 5616–5623. [Google Scholar] [CrossRef]
- Bonar, E.; Bukowski, M.; Chlebicka, K.; Madry, A.; Bereznicka, A.; Kosecka-Strojek, M.; Dubin, G.; Miedzobrodzki, J.; Mak, P.; Wladyka, B. Human skin microbiota-friendly lysostaphin. Int. J. Biol. Macromol. 2021, 31, 852–860. [Google Scholar] [CrossRef]
- Dulon, M.; Haamann, F.; Peters, C.; Schablon, A.; Nienhaus, A. MRSA prevalence in European healthcare settings: A review. BMC Infect. Dis. 2011, 11, 1–13. [Google Scholar] [CrossRef]
- Goscinski, G.; Lundholm, M.; Odenholt, I.; Sjölin, J. Variation in the propensity to release endotoxin after cefuroxime exposure in different gram-negative bacteria: Uniform and dose-dependent reduction by the addition of tobramycin. Scand. J. Infect. Dis. 2003, 35, 40–46. [Google Scholar] [CrossRef]
- Hurley, J. Antibiotic-induced release of endotoxin. Drug Saf. 1995, 12, 183–195. [Google Scholar] [CrossRef]
- Dofferhoff, A.S.; Nijland, J.H.; de Vries-Hospers, H.G.; Mulder, P.O.; Weits, J.; Bom, V.J. Effects of different types and combinations of antimicrobial agents on endotoxin release from gram-negative bacteria: An in-vitro and in-vivo study. Scand. J. Infect. Dis. 1991, 23, 745–754. [Google Scholar] [CrossRef]
- Young, M.P.J.; Carter, D.H.; Worthington, H.; Korachi, M.; Drucker, D.B. Microbial analysis of bone collected during implant surgery: A clinical and laboratory study. Clin. Oral Implant. Res. 2001, 12, 95–103. [Google Scholar] [CrossRef]
- Parvizi, J.; Barnes, S.; Shohat, N.; Edmiston Jr, C.E. Environment of care: Is it time to reassess microbial contamination of the operating room air as a risk factor for surgical site infection in total joint arthroplasty? Am. J. Infect. Control 2017, 45, 1267–1272. [Google Scholar] [CrossRef]
- de Souza Evangelista, S.; dos Santos, S.G.; de Resende Stoianoff, M.A.; de Oliveira, A.C. Analysis of microbial load on surgical instruments after clinical use and following manual and automated cleaning. Am. J. Infect. Control 2015, 43, 522–527. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraocular Site | ||||
|---|---|---|---|---|
| − | + | p-Value | ||
| Extraocular site | − | 10 (33.33) | 4 (13.33) | 0.019 * |
| + | 15 (50.00) | 1 (3.33) | ||
| Extraocular Site | |||
| Pre-surgery sampling | |||
| (+) | (−) | ||
| Post-surgery sampling | (+) | 14 (70) | 2 (10) |
| (−) | 3 (15) | 1 (5) | |
| Sensitivity: 82.35% Specificity: 33.33% | |||
| Intraocular site | |||
| Pre-surgery sampling | |||
| (+) | (−) | ||
| Post-surgery sampling | (+) | 3 (15) | 2 (10) |
| (−) | 14 (70) | 1 (5) | |
| Sensitivity: 17.65% Specificity: 33.33% | |||
| Extraocular Site | |||
| − | + | p-Value | |
| (n = 14) | (n = 16) | ||
| n (%) | n (%) | ||
| Death cause | |||
| Accident | 6 (42.86) | 4 (25.00) | 0.251 |
| Cancer | 6 (42.86) | 5 (31.25) | |
| Internal disease | 2 (14.29) | 7 (43.75) | |
| Operating place | |||
| Contamination zone | 3 (21.43) | 4 (25.0) | 0.892 |
| ICU | 3 (21.43) | 5 (31.25) | |
| OR | 8 (57.14) | 7 (43.75) | |
| Cold compression | |||
| No immediate | 3 (21.43) | 8 (50.00) | 0.215 |
| Immediate | 11 (78.57) | 8 (50.00) | |
| Intraocular Site | |||
| − | + | p-Value | |
| (n = 25) | (n = 5) | ||
| n (%) | n (%) | ||
| Death cause | |||
| Accident | 9 (36.00) | 1 (20.00) | 0.392 |
| Cancer | 10 (40.00) | 1 (20.00) | |
| Internal disease | 6 (24.00) | 3 (60.00) | |
| Operating place | |||
| Contamination zone | 5 (20.00) | 2 (40.00) | 0.387 |
| ICU | 8 (32.00) | 0 (0.00) | |
| OR | 12 (48.00) | 3 (60.00) | |
| Cold compression | |||
| No immediate | 9 (36.00) | 2 (40.00) | 1.000 |
| Immediate | 16 (64.00) | 3 (60.00) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-J.; Sung, K.-C.; Lin, W.-C.; Huang, F.-C. Comparison of Microbial Sampling Sites and Donor-Related Factors on Corneal Graft Contamination. J. Clin. Med. 2022, 11, 6236. https://doi.org/10.3390/jcm11216236
Wang Y-J, Sung K-C, Lin W-C, Huang F-C. Comparison of Microbial Sampling Sites and Donor-Related Factors on Corneal Graft Contamination. Journal of Clinical Medicine. 2022; 11(21):6236. https://doi.org/10.3390/jcm11216236
Chicago/Turabian StyleWang, Yu-Jen, Ko-Chiang Sung, Wei-Chen Lin, and Fu-Chin Huang. 2022. "Comparison of Microbial Sampling Sites and Donor-Related Factors on Corneal Graft Contamination" Journal of Clinical Medicine 11, no. 21: 6236. https://doi.org/10.3390/jcm11216236