
No Long-Term Mucosal Lesions in the Esophagus but More Gastric Mucosal Lesions after Sleeve Gastrectomy in Obese Rats

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Animal Surgery and Post-Surgery Procedures
2.3. Luminal Bile Acid Concentrations
2.4. Histological Analyses
2.5. Statistical Analyses
3. Results
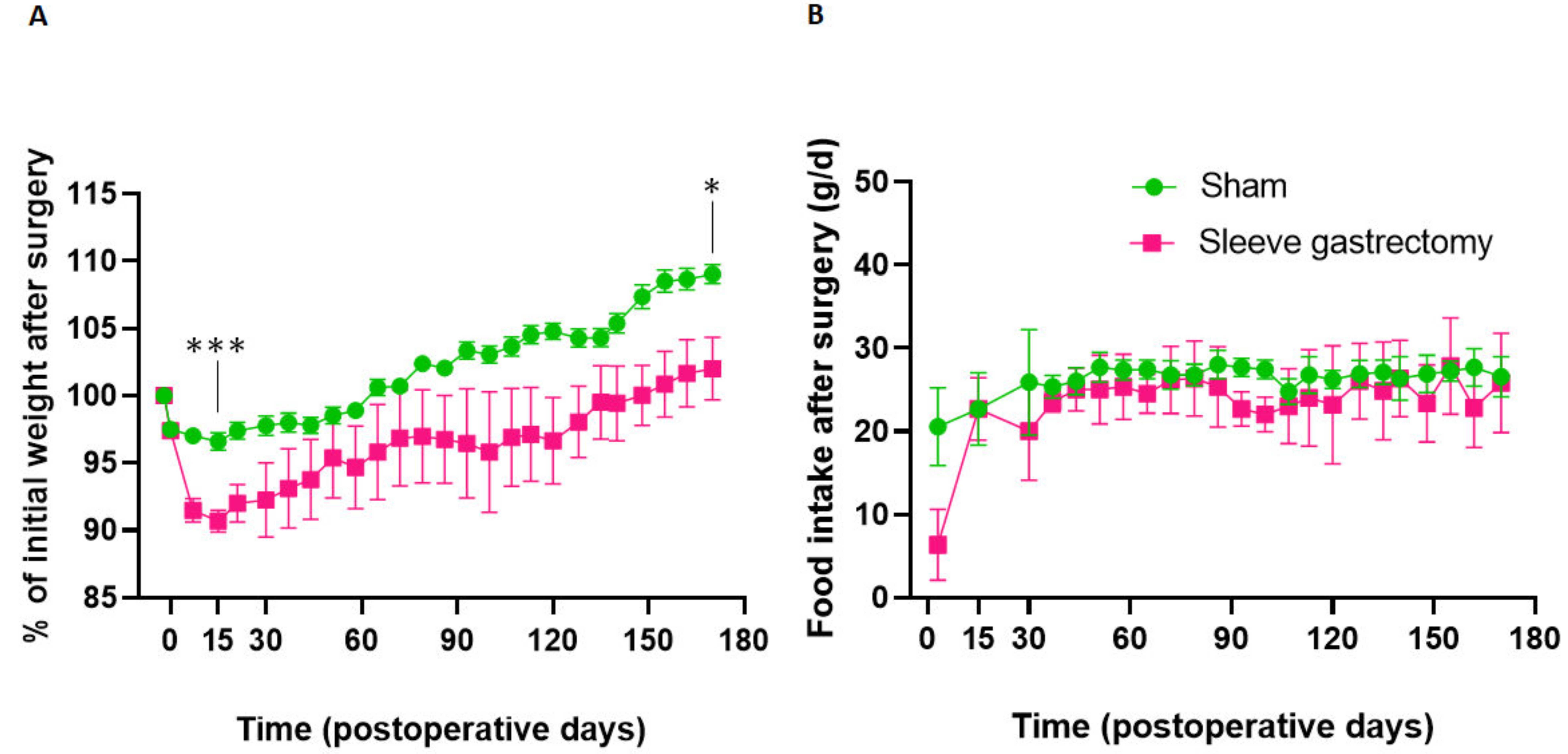
3.1. Evolution of Body Weight and Food Intake at 24 Weeks Postoperatively
3.2. Luminal Esogastric Bile Acid Content at 24 Weeks Postoperatively
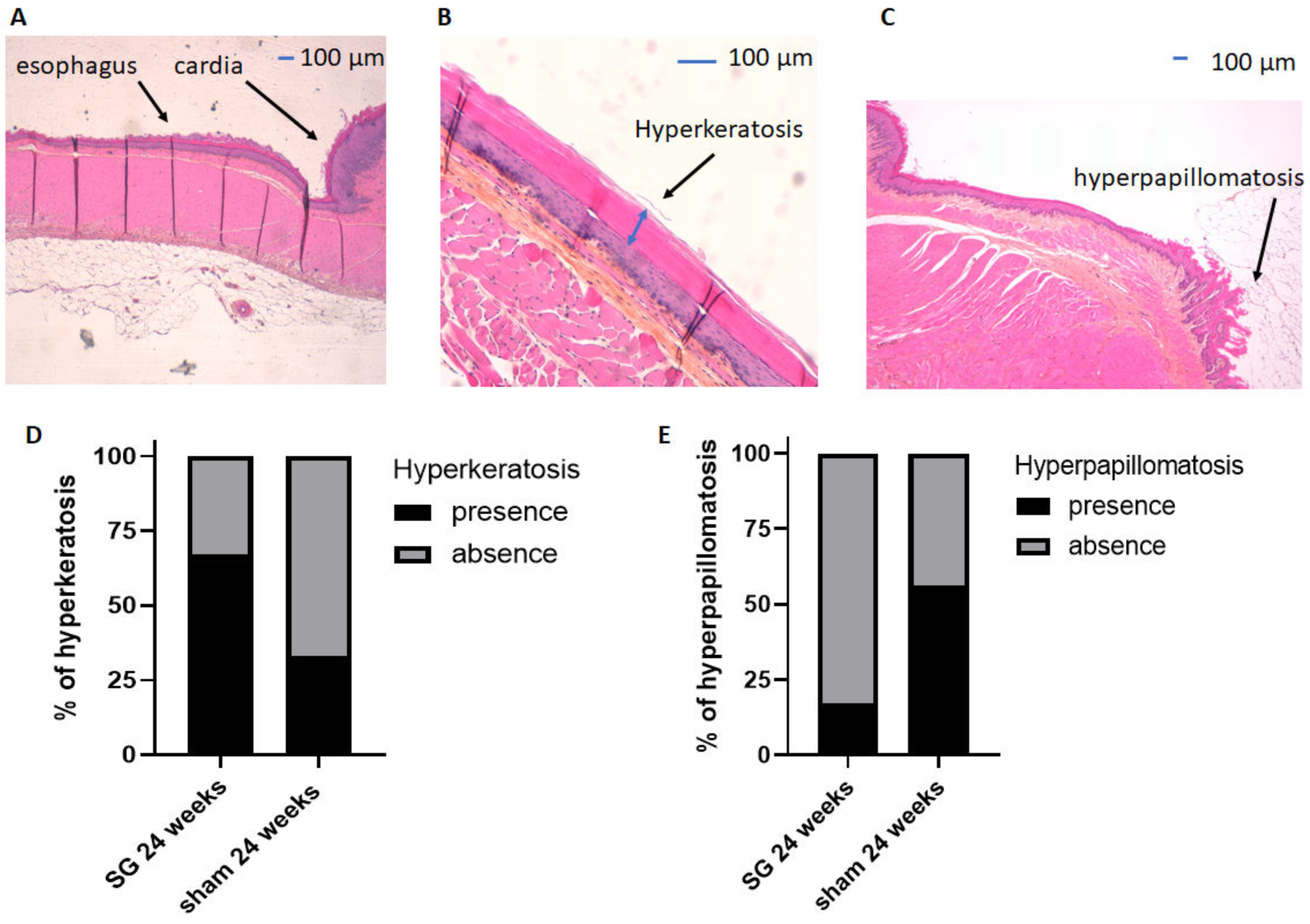
3.3. Histological Analyses of the Esophageal Mucosa at 24 Weeks Postoperatively
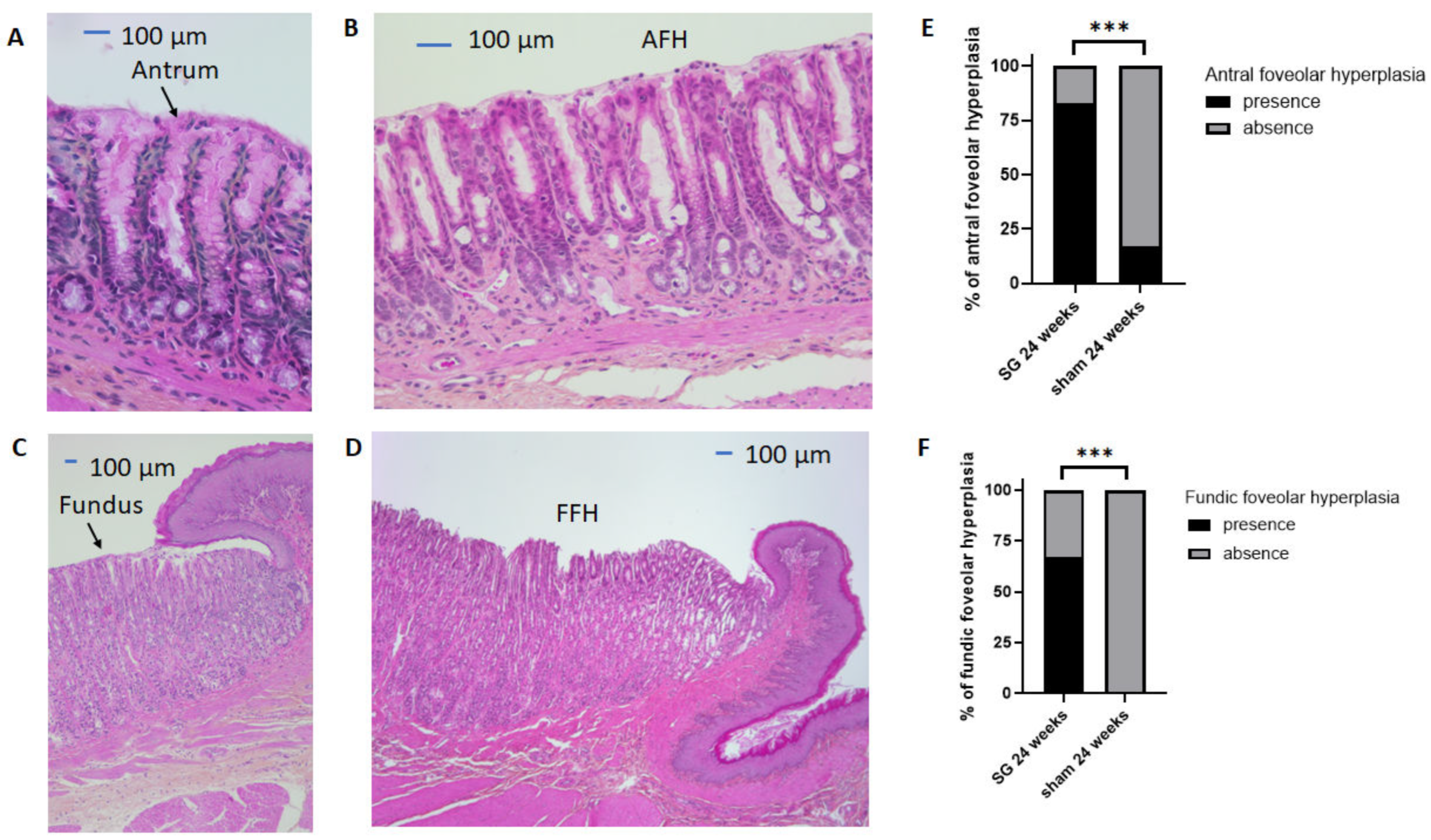
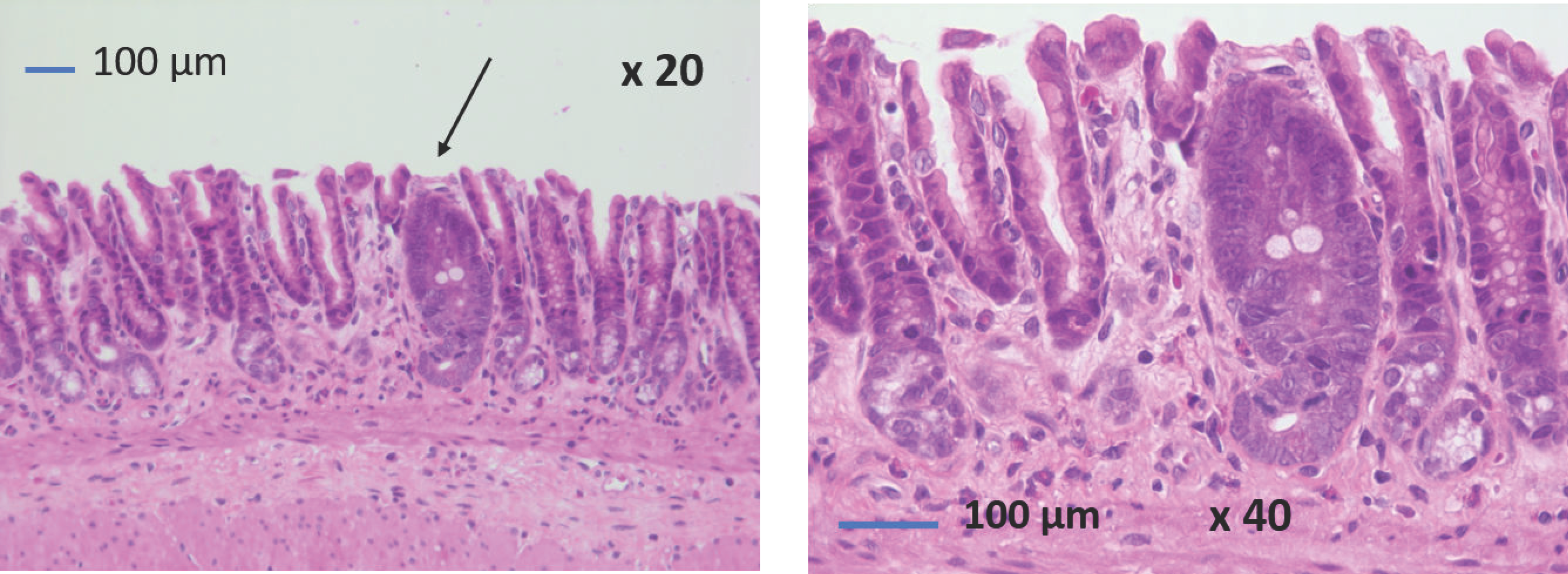
3.4. Histological Analyses of the Gastric Mucosa at 24 Weeks Postoperatively
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlsson, L.M.S.; Sjöholm, K.; Jacobson, P.; Andersson-Assarsson, J.C.; Svensson, P.A.; Taube, M.; Carlsson, B.; Peltonen, M. Life Expectancy after Bariatric Surgery in the Swedish Obese Subjects Study. N. Engl. J. Med. 2020, 383, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Ramos, A.; Shikora, S.; Kow, L. Bariatric Surgery Survey 2018: Similarities and Disparities Among the 5 IFSO Chapters. Obes. Surg. 2021, 31, 1937–1948. [Google Scholar] [CrossRef]
- Coupaye, M.; Rivière, P.; Breuil, M.C.; Castel, B.; Bogard, C.; Dupré, T.; Flamant, M.; Msika, S.; LeDoux, S. Comparison of nutritional status during the first year after sleeve gastrectomy and Roux-en-Y gastric bypass. Obes. Surg. 2014, 24, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Márquez, M.; Belda-Lozano, R.; Ferrer-Ayza, M. Technical controversies in laparoscopic sleeve gastrectomy. Obes. Surg. 2012, 22, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Coupaye, M.; Gorbatchef, C.; Calabrese, D.; Sami, O.; Msika, S.; Coffin, B.; Ledoux, S. Gastroesophageal Reflux After Sleeve Gastrectomy: A Prospective Mechanistic Study. Obes. Surg. 2018, 28, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Spechler, S.J.; Souza, R.F. Barrett’s esophagus. N. Engl. J. Med. 2014, 371, 836–845. [Google Scholar] [CrossRef]
- Hvid-Jensen, F.; Pedersen, L.; Drewes, A.M.; Sørensen, H.T.; Funch-Jensen, P. Incidence of Adenocarcinoma among Patients with Barrett’s Esophagus. N. Engl. J. Med. 2011, 365, 1375–1383. [Google Scholar] [CrossRef] [Green Version]
- Brown, W.A.; Johari Halim Shah, Y.; Balalis, G.; Bashir, A.; Ramos, A.; Kow, L.; Herrera, M.; Shikora, S.; Campos, G.M.; Himpens, J.; et al. IFSO Position Statement on the Role of Esophago-Gastro-Duodenal Endoscopy Prior to and after Bariatric and Metabolic Surgery Procedures. Obes. Surg. 2020, 30, 3135–3153. [Google Scholar] [CrossRef]
- Campos, G.M.; Mazzini, G.S.; Altieri, M.S.; Docimo, S., Jr.; DeMaria, E.J.; Rogers, A.M.; Clinical Issues Committee of the American Society for Metabolic and Bariatric Surgery. ASMBS position statement on the rationale for performance of upper gastrointestinal endoscopy before and after metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2021, 17, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Lallemand, L.; Duchalais, E.; Musquer, N.; Jacobi, D.; Coron, E.; des Varannes, S.B.; Mirallié, E.; Blanchard, C. Does Sleeve Gastrectomy Increase the Risk of Barret’s Esophagus? Obes. Surg. 2021, 31, 101–110. [Google Scholar] [CrossRef]
- Benvenga, R.; Roussel, J.; Cohen, R.; Bouchoucha, M.; Bendacha, Y.; Catheline, J.M. Long-term endoscopic follow-up after sleeve gastrectomy. J. Visc. Surg. 2020, 159, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Genco, A.; Soricelli, E.; Casella, G.; Maselli, R.; Castagneto-Gissey, L.; Di Lorenzo, N.; Basso, N. Gastroesophageal reflux disease and Barrett’s esophagus after laparoscopic sleeve gastrectomy: A possible, underestimated long-term complication. Surg. Obes. Relat. Dis. 2017, 13, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Sebastianelli, L.; Benois, M.; Vanbiervliet, G.; Bailly, L.; Robert, M.; Turrin, N.; Gizard, E.; Foletto, M.; Bisello, M.; Albanese, A.; et al. Systematic Endoscopy 5 Years After Sleeve Gastrectomy Results in a High Rate of Barrett’s Esophagus: Results of a Multicenter Study. Obes. Surg. 2019, 29, 1462–1469. [Google Scholar] [CrossRef] [PubMed]
- Felsenreich, D.M.; Ladinig, L.M.; Beckerhinn, P.; Sperker, C.; Schwameis, K.; Krebs, M.; Jedamzik, J.; Eilenberg, M.; Bichler, C.; Prager, G.; et al. Update: 10 Years of Sleeve Gastrectomy-the First 103 Patients. Obes. Surg. 2018, 28, 3586–3594. [Google Scholar] [CrossRef]
- Csendes, A.; Orellana, O.; Martínez, G.; Burgos, A.M.; Figueroa, M.; Lanzarini, E. Clinical, Endoscopic, and Histologic Findings at the Distal Esophagus and Stomach Before and Late (10.5 Years) after Laparoscopic Sleeve Gastrectomy: Results of a Prospective Study with 93% Follow-Up. Obes. Surg. 2019, 29, 3809–3817. [Google Scholar] [CrossRef]
- Salminen, P.; Grönroos, S.; Helmiö, M.; Hurme, S.; Juuti, A.; Juusela, R.; Peromaa-Haavisto, P.; Leivonen, M.; Nuutila, P.; Ovaska, J. Effect of Laparoscopic Sleeve Gastrectomy vs Roux-en-Y Gastric Bypass on Weight Loss, Comorbidities, and Reflux at 10 Years in Adult Patients with Obesity: The SLEEVEPASS Randomized Clinical Trial. JAMA Surg. 2022, 157, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Felsenreich, D.M.; Artemiou, E.; Wintersteller, L.; Jedamzik, J.; Eichelter, J.; Gensthaler, L.; Bichler, C.; Sperker, C.; Beckerhinn, P.; Kristo, I.; et al. 15 Years after Sleeve Gastrectomy: Gastroscopies, Manometries and 24h pH-metries in a Long-term Follow-up—A Multicenter Study. Obes. Facts. 2022, 15, 666–673. [Google Scholar] [CrossRef]
- Greene, C.L.; Worrell, S.G.; DeMeester, T.R. Rat Reflux Model of Esophageal Cancer and Its Implication in Human Disease. Ann. Surg. 2015, 262, 910–924. [Google Scholar] [CrossRef] [PubMed]
- Altieri, M.S.; Shroyer, K.R.; Pryor, A.; Pagnotti, G.M.; Ete Chan, M.; Talamini, M.; Telem, D.A. The association between sleeve gastrectomy and histopathologic changes consistent with esophagitis in a rodent model. Surg. Obes. Relat. Dis. 2015, 11, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Arapis, K.; Cavin, J.B.; Gillard, L.; Cluzeaud, F.; Lettéron, P.; Ducroc, R.; Le Beyec, J.; Hourseau, M.; Couvelard, A.; Marmuse, J.-P.; et al. Remodeling of the residual gastric mucosa after roux-en-y gastric bypass or vertical sleeve gastrectomy in diet-induced obese rats. PLoS ONE 2015, 10, e0121414. [Google Scholar] [CrossRef]
- Martín, M.; Burrell, M.A.; Gómez-Ambrosi, J.; Valentí, V.; Bueno, Á.; Ramírez, B.; Becerril, S.; Lancha, A.; del Sol Calderón, P.; Méndez-Giménez, L.; et al. Short- and long-term changes in gastric morphology and histopathology following sleeve gastrectomy in diet-induced obese rats. Obes. Surg. 2012, 22, 634–640. [Google Scholar] [CrossRef]
- Gulcicek, O.B.; Ozdogan, K.; Solmaz, A.; Yigitbas, H.; Altınay, S.; Gunes, A.; Celik, D.S.; Yavuz, E.; Celik, A.; Celebi, F. Metabolic and histopathological effects of sleeve gastrectomy and gastric plication: An experimental rodent model. Food Nutr. Res. 2016, 60, 30888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, P. The laboratory rat: Relating its age with human’s. Int. J. Prev. Med. 2013, 4, 624–630. [Google Scholar]
- Ribeiro-Parenti, L.; Jarry, A.C.; Cavin, J.B.; Willemetz, A.; Le Beyec, J.; Sannier, A.; Benadda, S.; Pelletier, A.-L.; Hourseau, M.; Léger, T.; et al. Bariatric surgery induces a new gastric mucosa phenotype with increased functional glucagon-like peptide-1 expressing cells. Nat. Commun. 2021, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Duboc, H.; Nguyen, C.C.; Cavin, J.B.; Ribeiro-Parenti, L.; Jarry, A.C.; Rainteau, D.; Humbert, L.; Coffin, B.; Le Gall, M.; Bado, A.; et al. Roux-en-Y Gastric-Bypass and sleeve gastrectomy induces specific shifts of the gut microbiota without altering the metabolism of bile acids in the intestinal lumen. Int. J. Obes. 2019, 43, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Bruzzi, M.; Duboc, H.; Gronnier, C.; Rainteau, D.; Couvelard, A.; Le Gall, M.; Bado, A.; Chevallier, J.-M. Long-Term Evaluation of Biliary Reflux After Experimental One-Anastomosis Gastric Bypass in Rats. Obes. Surg. 2017, 27, 1119–1122. [Google Scholar] [CrossRef]
- Siebert, M.; Ribeiro-Parenti, L.; Nguyen, N.D.; Hourseau, M.; Duchêne, B.; Humbert, L.; Jonckheere, N.; Nuel, G.; Chevallier, J.-M.; Duboc, H.; et al. Long-term consequences of one anastomosis gastric bypass on esogastric mucosa in a preclinical rat model. Sci. Rep. 2020, 10, 7393. [Google Scholar] [CrossRef]
- Wang, M.; Widjaja, J.; Dolo, P.R.; Yao, L.; Hong, J.; Zhu, X. The Protective Effect of Transit Bipartition and Its Modification Against Sleeve Gastrectomy-Related Esophagitis in a Rodent Model. Obes. Surg. 2022, 32, 1149–1156. [Google Scholar] [CrossRef]
- Wang, S.; Wang, Q.; Xu, L.; Yu, P.; Li, Q.; Li, X.; Guo, M.; Lian, B.; Ji, G. Beware Pathological Findings of the Stomach in Patients Undergoing Bariatric Surgery: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 337–342. [Google Scholar] [CrossRef]
- White, J.R.; Banks, M. Identifying the pre-malignant stomach: From guidelines to practice. Transl. Gastroenterol. Hepatol. 2022, 7, 8. [Google Scholar] [CrossRef]
- Huang, R.J.; Choi, A.Y.; Truong, C.D.; Yeh, M.M.; Hwang, J.H. Diagnosis and Management of Gastric Intestinal Metaplasia: Current Status and Future Directions. Gut Liver 2019, 13, 596–603. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coupaye, M.; Ribeiro-Parenti, L.; Baratte, C.; Hourseau, M.; Willemetz, A.; Duboc, H.; Ledoux, S.; Bado, A.; Couvelard, A.; Le Gall, M. No Long-Term Mucosal Lesions in the Esophagus but More Gastric Mucosal Lesions after Sleeve Gastrectomy in Obese Rats. J. Clin. Med. 2023, 12, 1848. https://doi.org/10.3390/jcm12051848
Coupaye M, Ribeiro-Parenti L, Baratte C, Hourseau M, Willemetz A, Duboc H, Ledoux S, Bado A, Couvelard A, Le Gall M. No Long-Term Mucosal Lesions in the Esophagus but More Gastric Mucosal Lesions after Sleeve Gastrectomy in Obese Rats. Journal of Clinical Medicine. 2023; 12(5):1848. https://doi.org/10.3390/jcm12051848
Chicago/Turabian StyleCoupaye, Muriel, Lara Ribeiro-Parenti, Clément Baratte, Muriel Hourseau, Alexandra Willemetz, Henri Duboc, Séverine Ledoux, André Bado, Anne Couvelard, and Maude Le Gall. 2023. "No Long-Term Mucosal Lesions in the Esophagus but More Gastric Mucosal Lesions after Sleeve Gastrectomy in Obese Rats" Journal of Clinical Medicine 12, no. 5: 1848. https://doi.org/10.3390/jcm12051848