
Shortening the Biliopancreatic Limb Length of One Anastomosis Gastric Bypass Maintains Glucose Homeostasis Improvement with Limited Weight Loss
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Surgery
2.3. Intestinal Nutrient Absorption
2.4. Meal Test, Oral Glucose Tolerance Test and Insulin Tolerance Test
2.5. Statistical Analyses
3. Results
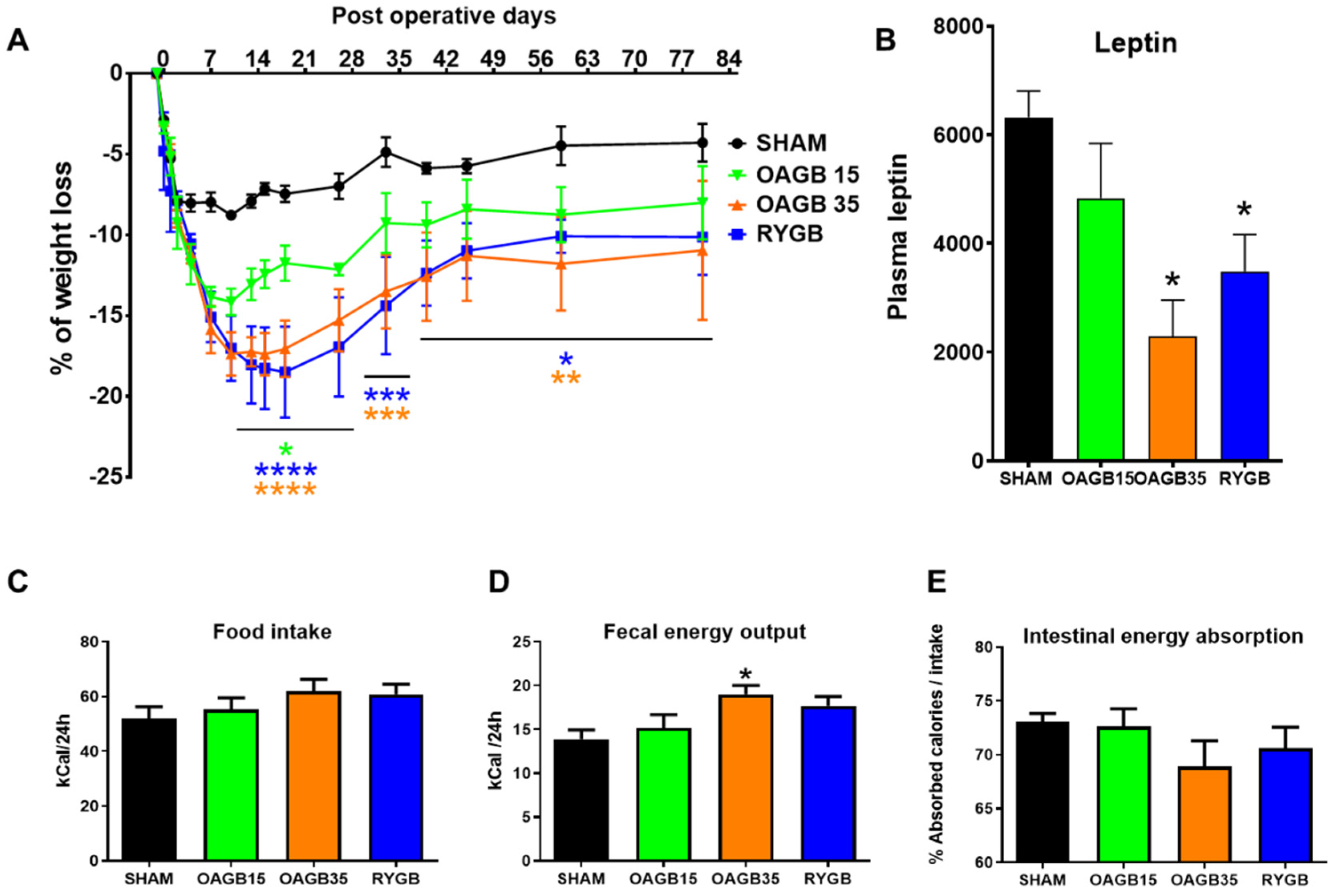
3.1. Shortening the BPL in Obese Rats Affects Body Weight but Not Food Intake and Absorption in the Long Term
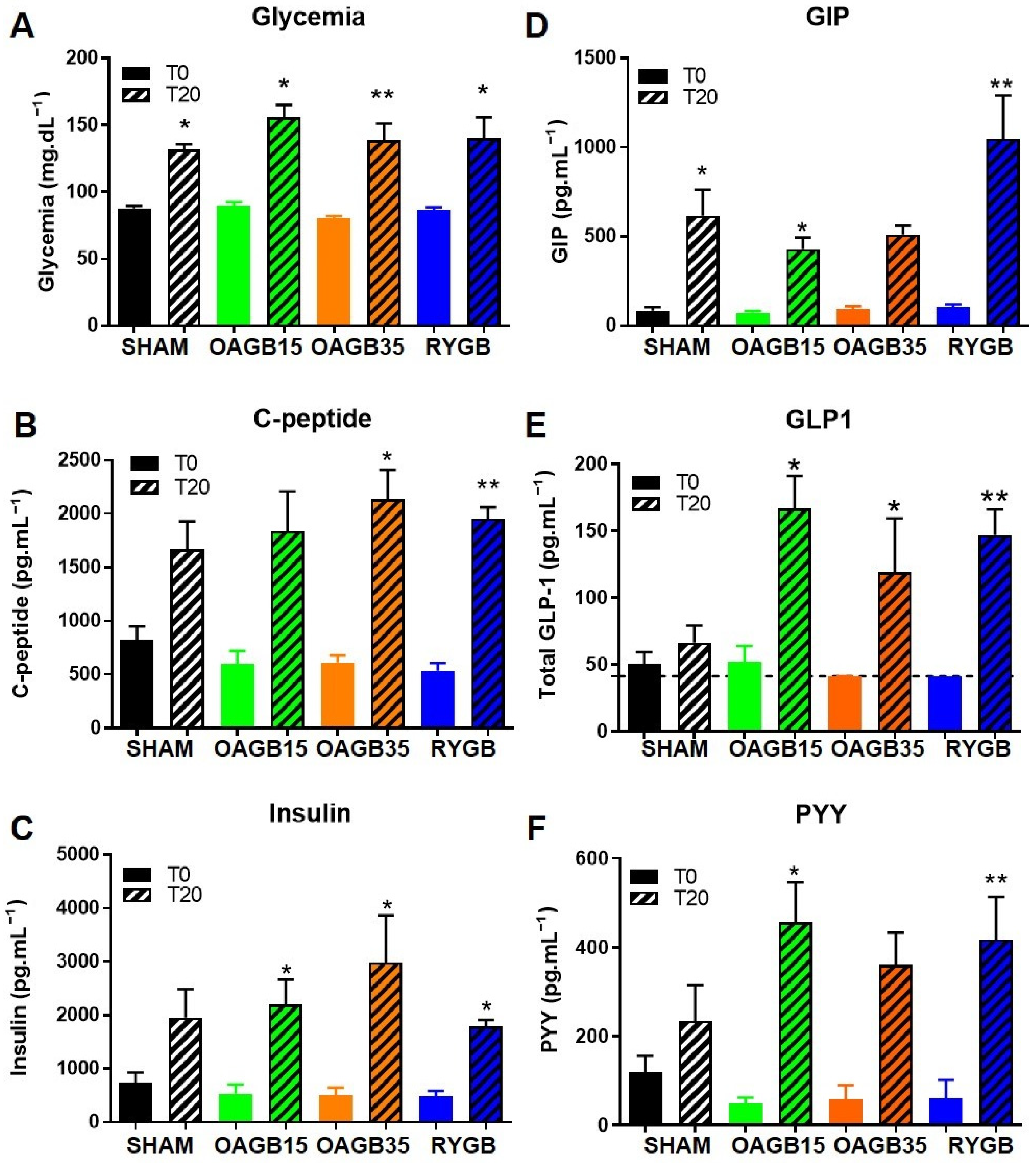
3.2. Shortening the BPL in OAGB Does Not Affect Enterohormone Secretion in Obese Animals
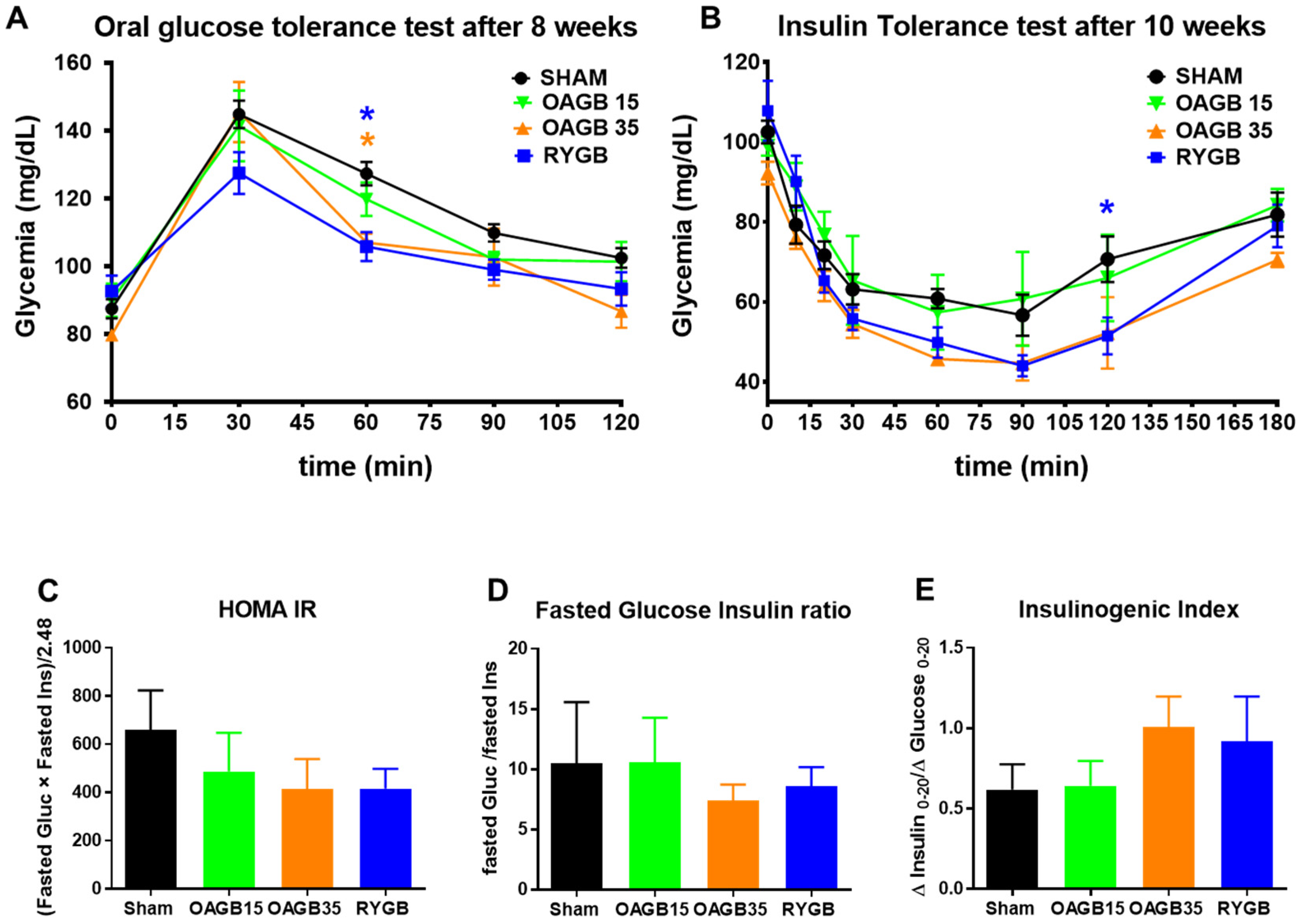
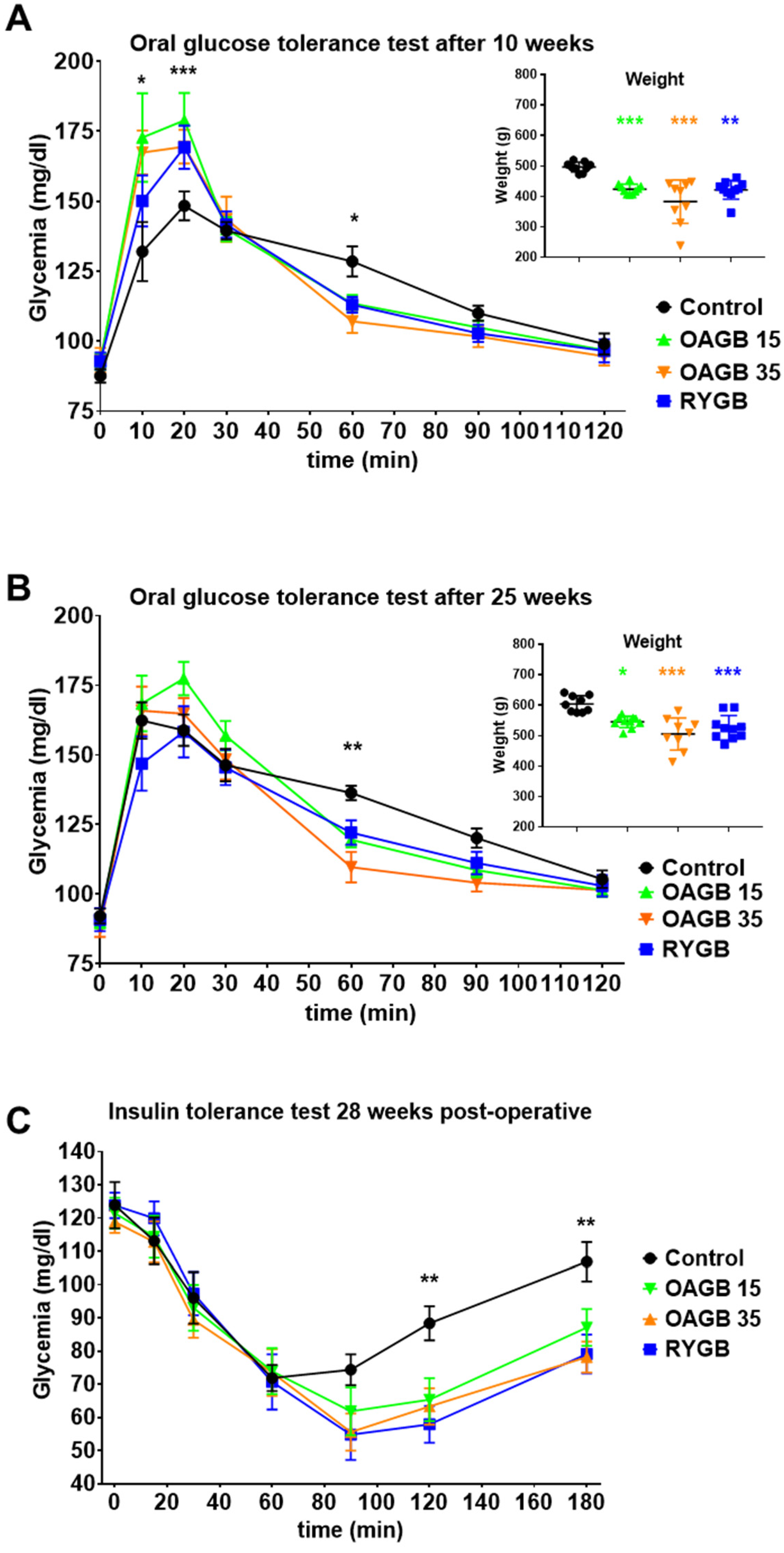
3.3. OAGB with a Short BPL Ameliorates Glucose Regulation in Non-Obese Animals
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arterburn, D.; Wellman, R.; Emiliano, A.; Smith, S.R.; Odegaard, A.O.; Murali, S.; Williams, N.; Coleman, K.J.; Courcoulas, A.; Coley, R.Y.; et al. Comparative Effectiveness and Safety of Bariatric Procedures for Weight Loss: A PCORnet Cohort Study. Ann. Intern. Med. 2018, 169, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, A.; Czernichow, S.; Hertig, A.; Ledoux, S.; Poghosyan, T.; Quilliot, D.; Gall, M.L.; Bado, A.; Joly, F. Prevention and Treatment of Nutritional Complications after Bariatric Surgery. Lancet Gastroenterol. Hepatol. 2021, 6, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, R. The Mini-Gastric Bypass: Experience with the First 1274 Cases. Obes. Surg. 2001, 11, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.; Espalieu, P.; Pelascini, E.; Caiazzo, R.; Sterkers, A.; Khamphommala, L.; Poghosyan, T.; Chevallier, J.-M.; Malherbe, V.; Chouillard, E.; et al. Efficacy and Safety of One Anastomosis Gastric Bypass versus Roux-En-Y Gastric Bypass for Obesity (YOMEGA): A Multicentre, Randomised, Open-Label, Non-Inferiority Trial. Lancet 2019, 393, 1299–1309. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Carbajo, M.A.; Jimenez, J.M.; Castro, M.J.; Gonzalez, G.; Ortiz-de-Solorzano, J.; Zubiaga, L. Long-Term Follow-up after Sleeve Gastrectomy versus Roux-En-Y Gastric Bypass versus One-Anastomosis Gastric Bypass: A Prospective Randomized Comparative Study of Weight Loss and Remission of Comorbidities. Surg. Endosc. 2019, 33, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.C.; Chevallier, J.-M.; Mahawar, K.; Brown, W.; Kow, L.; White, K.P.; Shikora, S. IFSO Consensus Conference Contributors IFSO (International Federation for Surgery of Obesity and Metabolic Disorders) Consensus Conference Statement on One-Anastomosis Gastric Bypass (OAGB-MGB): Results of a Modified Delphi Study. Obes. Surg. 2020, 30, 1625–1634. [Google Scholar] [CrossRef]
- Mahawar, K.K.; Borg, C.-M.; Kular, K.S.; Courtney, M.J.; Sillah, K.; Carr, W.R.J.; Jennings, N.; Madhok, B.; Singhal, R.; Small, P.K. Understanding Objections to One Anastomosis (Mini) Gastric Bypass: A Survey of 417 Surgeons Not Performing This Procedure. Obes. Surg. 2017, 27, 2222–2228. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.; Tie, T.; Ooi, G.; Higa, K.; Himpens, J.; Carbajo, M.-A.; Mahawar, K.; Shikora, S.; Brown, W.A. Mini Gastric Bypass-One Anastomosis Gastric Bypass (MGB-OAGB)-IFSO Position Statement. Obes. Surg. 2018, 28, 1188–1206. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, A.; Tantia, O.; Goyal, G.; Chaudhuri, T.; Khanna, S.; Poddar, A.; Gupta, S.; Majumdar, K. MGB-OAGB: Effect of Biliopancreatic Limb Length on Nutritional Deficiency, Weight Loss, and Comorbidity Resolution. Obes. Surg. 2018, 28, 3439–3445. [Google Scholar] [CrossRef] [PubMed]
- Pizza, F.; Lucido, F.S.; D’Antonio, D.; Tolone, S.; Gambardella, C.; Dell’Isola, C.; Docimo, L.; Marvaso, A. Biliopancreatic Limb Length in One Anastomosis Gastric Bypass: Which Is the Best? Obes. Surg. 2020, 30, 3685–3694. [Google Scholar] [CrossRef]
- Poghosyan, T.; Alameh, A.; Bruzzi, M.; Faul, A.; Rives-Lange, C.; Zinzindohoue, F.; Douard, R.; Chevallier, J.-M. Conversion of Sleeve Gastrectomy to One Anastomosis Gastric Bypass for Weight Loss Failure. Obes. Surg. 2019, 29, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Cavin, J.-B.; Couvelard, A.; Lebtahi, R.; Ducroc, R.; Arapis, K.; Voitellier, E.; Cluzeaud, F.; Gillard, L.; Hourseau, M.; Mikail, N.; et al. Differences in Alimentary Glucose Absorption and Intestinal Disposal of Blood Glucose After Roux-En-Y Gastric Bypass vs Sleeve Gastrectomy. Gastroenterology 2016, 150, 454–464.e9. [Google Scholar] [CrossRef] [PubMed]
- Siebert, M.A.; Chevallier, J.-M.; D’Aurelle de Paladines, D.; Pottier, Y.; Msika, S.; Le Gall, M.; Bado, A.; Ribeiro-Parenti, L. One-Anastomosis Gastric Bypass (OAGB) in Rats. J. Vis. Exp. 2018, 10, 141. [Google Scholar] [CrossRef] [PubMed]
- Cavin, J.-B.; Voitellier, E.; Cluzeaud, F.; Kapel, N.; Marmuse, J.-P.; Chevallier, J.-M.; Msika, S.; Bado, A.; Le Gall, M. Malabsorption and Intestinal Adaptation after One Anastomosis Gastric Bypass Compared with Roux-En-Y Gastric Bypass in Rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 311, G492–G500. [Google Scholar] [CrossRef] [PubMed]
- Siebert, M.; Ribeiro-Parenti, L.; Nguyen, N.D.; Hourseau, M.; Duchêne, B.; Humbert, L.; Jonckheere, N.; Nuel, G.; Chevallier, J.-M.; Duboc, H.; et al. Long-Term Consequences of One Anastomosis Gastric Bypass on Esogastric Mucosa in a Preclinical Rat Model. Sci. Rep. 2020, 10, 7393. [Google Scholar] [CrossRef] [PubMed]
- Tessier, R.; Ribeiro-Parenti, L.; Bruneau, O.; Khodorova, N.; Cavin, J.-B.; Bado, A.; Azzout-Marniche, D.; Calvez, J.; Le Gall, M.; Gaudichon, C. Effect of Different Bariatric Surgeries on Dietary Protein Bioavailability in Rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 317, G592–G601. [Google Scholar] [CrossRef]
- Patrício, B.G.; Morais, T.; Guimarães, M.; Veedfald, S.; Hartmann, B.; Hilsted, L.; Holst, J.J.; Nora, M.; Monteiro, M.P. Gut Hormone Release after Gastric Bypass Depends on the Length of the Biliopancreatic Limb. Int. J. Obes. 2019, 43, 1009–1018. [Google Scholar] [CrossRef]
- Larraufie, P.; Roberts, G.P.; McGavigan, A.K.; Kay, R.G.; Li, J.; Leiter, A.; Melvin, A.; Biggs, E.K.; Ravn, P.; Davy, K.; et al. Important Role of the GLP-1 Axis for Glucose Homeostasis after Bariatric Surgery. Cell Rep. 2019, 26, 1399–1408.e6. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro-Parenti, L.; El Jindi, H.; Willemetz, A.; Siebert, M.; Kapel, N.; Le Beyec, J.; Bado, A.; Le Gall, M. Shortening the Biliopancreatic Limb Length of One Anastomosis Gastric Bypass Maintains Glucose Homeostasis Improvement with Limited Weight Loss. J. Clin. Med. 2022, 11, 4976. https://doi.org/10.3390/jcm11174976
Ribeiro-Parenti L, El Jindi H, Willemetz A, Siebert M, Kapel N, Le Beyec J, Bado A, Le Gall M. Shortening the Biliopancreatic Limb Length of One Anastomosis Gastric Bypass Maintains Glucose Homeostasis Improvement with Limited Weight Loss. Journal of Clinical Medicine. 2022; 11(17):4976. https://doi.org/10.3390/jcm11174976
Chicago/Turabian StyleRibeiro-Parenti, Lara, Hounayda El Jindi, Alexandra Willemetz, Matthieu Siebert, Nathalie Kapel, Johanne Le Beyec, André Bado, and Maude Le Gall. 2022. "Shortening the Biliopancreatic Limb Length of One Anastomosis Gastric Bypass Maintains Glucose Homeostasis Improvement with Limited Weight Loss" Journal of Clinical Medicine 11, no. 17: 4976. https://doi.org/10.3390/jcm11174976