
Outcome of Kidney Transplants from Viremic and Non-Viremic Hepatitis C Virus Positive Donors into Negative Recipients: Results of the Spanish Registry
 , , ,
on behalf of the Renal Transplantation with HCV Positive Donors Spanish Study Group
, , ,
on behalf of the Renal Transplantation with HCV Positive Donors Spanish Study Group
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Outcome Variables
2.3. Statistics
3. Results
3.1. Patient Characteristics
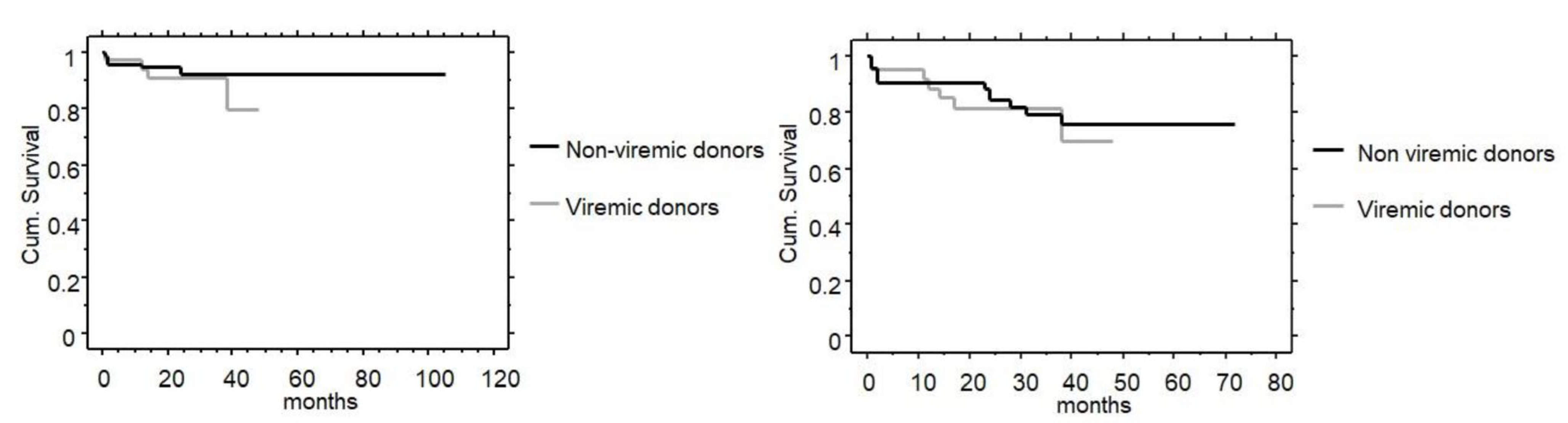
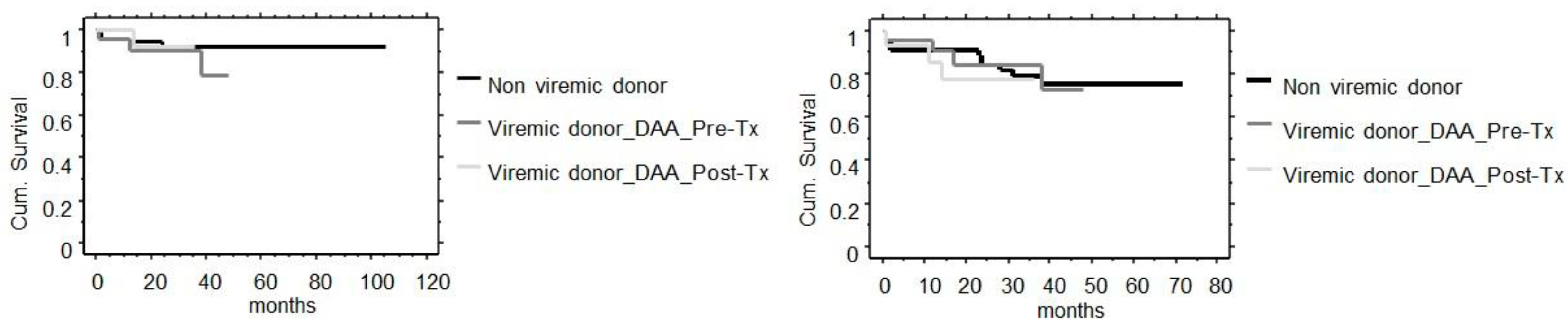
3.2. Outcome Variables
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gastaminza, P.; Dryden, K.A.; Boyd, B.; Wood, M.R.; Law, M.; Yeager, M.; Chisari, F.V. Ultrastructural and biophysical characterization of hepatitis C virus particles produced in cell culture. J. Virol. 2010, 84, 10999–11009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, B.J.; Milford, E.L.; Kirkman, R.L.; Quan, S.; Sayre, K.R.; Johnson, P.J.; Wilber, J.C.; Levey, A.S. Prevalence of hepatitis C virus RNA in organ donors positive for hepatitis C antibody and in the recipients of their organs. N. Engl. J. Med. 1992, 327, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Levitsky, J.; Formica, R.N.; Bloom, R.D.; Charlton, M.; Curry, M.; Friedewald, J.; Friedman, J.; Goldberg, D.; Hall, S.; Ison, M.; et al. The American Society of Transplantation Consensus Conference on the Use of Hepatitis C Viremic Donors in Solid Organ Transplantation. Am. J. Transplant. 2017, 17, 2790–2802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daloul, R.; Pesavento, T.E.; Goldberg, D.S.; Reese, P.P. A review of kidney transplantation from HCV-viremic donors into HCV-negative recipients. Kidney Int. 2021, 100, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Cerutti, R.; Alfieri, C.M.; Messa, P. Updated View on Kidney Transplant from HCV-Infected Donors and DAAs. Pharmaceutics 2021, 13, 496. [Google Scholar] [CrossRef]
- Zeuzem, S.; Foster, G.R.; Wang, S.; Asatryan, A.; Gane, E.; Feld, J.J.; Asselah, T.; Bourlière, M.; Ruane, P.J.; Wedemeyer, H.; et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection. N. Engl. J. Med. 2018, 378, 354–369. [Google Scholar] [CrossRef]
- Sise, M.E.; Goldberg, D.S.; Kort, J.J.; Schaubel, D.E.; Alloway, R.R.; Durand, C.M.; Fontana, R.J.; Brown, R.S., Jr.; Friedewald, J.J.; Prenner, S.; et al. Multicenter Study to Transplant Hepatitis C-Infected Kidneys (MYTHIC): An Open-Label Study of Combined Glecaprevir and Pibrentasvir to Treat Recipients of Transplanted Kidneys from Deceased Donors with Hepatitis C Virus Infection. J. Am. Soc. Nephrol. 2020, 31, 2678–2687. [Google Scholar] [CrossRef]
- Franco, A.; Moreso, F.; Merino, E.; Sancho, A.; Kanter, J.; Gimeno, A.; Balibrea, N.; Rodriguez, M.; Contreras, F.P. Renal transplantation from seropositive hepatitis C virus donors to seronegative recipients in Spain: A prospective study. Transpl. Int. 2019, 32, 710–716. [Google Scholar] [CrossRef]
- Durand, C.M.; Garonzik-Wang, J.; Desai, N.M. Reclaiming missed opportunities: A strategy of targeted direct-acting antiviral prophylaxis for HCV-seronegative recipients of HCV-seropositive donor kidneys. Transpl. Int. 2019, 32, 690–692. [Google Scholar] [CrossRef]
- Documento de Consenso Para la Valoración de Donantes con Serología Positiva Para el Virus de la Hepatitis C. Available online: http://www.ont.es/infesp/DocumentosDeConsenso/Documento%20Consenso%20Valoraci%C3%B3n%20Donantes%20Virus%20C_ABRIL2019.pdf (accessed on 10 August 2022).
- Nowak, K.M.; Witzke, O.; Sotiropoulos, G.C.; Benkö, T.; Fiedler, M.; Timm, J.; Kribben, A.; Wilde, B.; Saner, F.; Paul, A.; et al. Transplantation of Renal Allografts From Organ Donors Reactive for HCV Antibodies to HCV-Negative Recipients: Safety and Clinical Outcome. Kidney Int. Rep. 2017, 2, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Friebus-Kardash, J.; Gäckler, A.; Kribben, A.; Witzke, O.; Wedemeyer, H.; Treckmann, J.; Herzer, K.; Eisenberger, U. Successful early sofosbuvir-based antiviral treatment after transplantation of kidneys from HCV-viremic donors into HCV-negative recipients. Transpl. Infect. Dis. 2019, 21, e13146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organització Catalana de Trasplantaments. Registre de Malalts Renals de Catalunya: Informe Estadístic 2020. Registro de Enfermos Renales de Cataluña: Informe Estadístico 2020. Available online: https://scientiasalut.gencat.cat/handle/11351/7499 (accessed on 10 August 2022).
- Chen, G.; Zhang, W.; Ben, Y. Identification of Key Regulators of Hepatitis C Virus-Induced Hepatocellular Carcinoma by Integrating Whole-Genome and Transcriptome Sequencing Data. Front. Genet. 2021, 12, 741608. [Google Scholar] [CrossRef] [PubMed]
- Hamdane, N.; Jühling, F.; Crouchet, E.; El Saghire, H.; Thumann, C.; Oudot, M.A.; Bandiera, S.; Saviano, A.; Ponsolles, C.; Roca Suarez, A.A.R.; et al. HCV-Induced Epigenetic Changes Associated with Liver Cancer Risk Persist After Sustained Virologic Response. Gastroenterology 2019, 156, 2313–2329.e7. [Google Scholar] [CrossRef] [Green Version]
- El-Serag, H.B.; Kanwal, F.; Richardson, P.; Kramer, J. Risk of hepatocellular carcinoma after sustained virological response in Veterans with hepatitis C virus infection. Hepatology 2016, 64, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Kanwal, F.; Kramer, J.R.; Asch, S.M.; Cao, Y.; Li, L.; El-Serag, H.B. Long-Term Risk of Hepatocellular Carcinoma in HCV Patients Treated with Direct Acting Antiviral Agents. Hepatology 2020, 71, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Czarnecka, P.; Czarnecka, K.; Tronina, O.; Baczkowska, T.; Durlik, M. Utilization of HCV viremic donors in kidney transplantation: A chance or a threat? Renal Failure 2022, 44, 434–449. [Google Scholar] [CrossRef]
- Dao, A.; Cuffy, M.; Kaiser, T.E.; Loethen, A.; Cafardi, J.; Luckett, K.; Rike, A.H.; Cardi, M.; Alloway, R.R.; Govil, A.; et al. Use of HCV Ab+/NAT- donors in HCV naïve renal transplant recipients to expand the kidney donor pool. Clin. Transplant. 2019, 33, e13598. [Google Scholar] [CrossRef] [PubMed]
- de Vera, M.E.; Volk, M.L.; Ncube, Z.; Blais, S.; Robinson, M.; Allen, N.; Evans, R.; Weissman, J.; Baron, P.; Kore, A.; et al. Transplantation of hepatitis C virus (HCV) antibody positive, nucleic acid test negative donor kidneys to HCV negative patients frequently results in seroconversion but not HCV viremia. Am. J. Transplant. 2018, 18, 2451–2456. [Google Scholar] [CrossRef] [Green Version]
- Kucirka, L.M.; Sarathy, H.; Govindan, P.; Wolf, J.H.; Ellison, T.A.; Hart, L.J.; Montgomery, R.A.; Ros, R.L.; Segev, D.L. Risk of window period hepatitis-C infection in high infectious risk donors: Systematic review and meta-analysis. Am. J. Transplant. 2011, 11, 1188–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suryaprasad, S.; Basavaraju, S.V.; Hocevar, S.N.; Theodoropoulos, N.; Zuckerman, R.A.; Hayden, T.; Forbi, J.C.; Pegues, D.; Levine, M.; Martin, S.I.; et al. Transmission of Hepatitis C Virus from Organ Donors Despite Nucleic Acid Test Screening. Am. J. Transplant. 2015, 15, 1827–1835. [Google Scholar] [CrossRef]
- Molnar, M.Z.; Nair, S.; Cseprekal, O.; Yazawa, M.; Talwar, M.; Balaraman, V.; Podila, P.S.B.; Mas, V.; Maluf, D.; Helmick, R.A.; et al. Transplantation of kidneys from hepatitis C-infected donors to hepatitis C-negative recipients: Single center experience. Am. J. Transplant. 2019, 19, 3046–3057. [Google Scholar] [CrossRef] [PubMed]
- Kapila, N.; Menon, K.N.; Al-Khalloufi, K.; Vanatta, J.M.; Murgas, C.; Reino, D.; Ebaid, S.; Shaw, J.J.; Agrawal, N.; Rhazouani, S.; et al. Hepatitis C Virus NAT-Positive Solid Organ Allografts Transplanted into Hepatitis C Virus-Negative Recipients: A Real-World Experience. Hepatology 2020, 72, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Torabi, J.; Rocca, J.P.; Ajaimy, M.; Melvin, J.; Campbell, A.; Akalin, E.; Liriano, L.E.; Azzi, Y.; Pynadath, C.; Greenstein, S.M.; et al. Commercial insurance delays direct-acting antiviral treatment for hepatitis C kidney transplantation into uninfected recipients. Transpl. Infect. Dis. 2021, 23, e13449. [Google Scholar] [CrossRef] [PubMed]
- Reese, P.P.; Abt, P.L.; Blumberg, E.A.; Van Deerlin, V.M.; Bloom, R.D.; Potluri, V.S.; Levine, M.; Porrett, P.; Sawinskiet, D.; Nazarian, S.M.; et al. Twelve-Month Outcomes After Transplant of Hepatitis C-Infected Kidneys into Uninfected Recipients: A Single-Group Trial. Ann. Intern. Med. 2018, 169, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Molnar, M.Z.; Azhar, A.; Tsujita, M.; Talwar, M.; Balaraman, V.; Bhalla, A.; Podila, P.S.B.; Kothadia, K.; Agbim, U.A.; Maliakkal, B.; et al. Transplantation of Kidneys From Hepatitis C Virus-Infected Donors to Hepatitis C Virus-Negative Recipients: One-Year Kidney Allograft Outcomes. Am. J. Kidney Dis. 2021, 77, 739–747.e1. [Google Scholar] [CrossRef] [PubMed]
- Porrett, P.M.; Reese, P.P.; Holzmayer, V.; Coller, K.E.; Kuhns, M.; Van Deerlin, V.M.; Gentile, C.; Smith, J.R.; Sicilia, A.; Woodards, A.; et al. Early emergence of anti-HCV antibody implicates donor origin in recipients of an HCV-infected organ. Am. J. Transplant. 2019, 19, 2525–2532. [Google Scholar] [CrossRef]
- Solà-Porta, E.; Redondo-Pachón, D.; Arias-Cabrales, C.; Navazo, D.; Buxeda, A.; Burballa, C.; Crespo, M.; García-Retortillo, M.; Pascual, J.; Pérez-Sáez, M.J. Early Hypertransaminasemia after Kidney Transplantation: Significance and Evolution According to Donor Type. J. Clin. Med. 2021, 10, 5168. [Google Scholar] [CrossRef]
- Durand, C.M.; Bowring, M.G.; Thomas, A.G.; Kucirka, L.M.; Massie, A.B.; Cameron, A.; Desia, N.M.; Sulkowski, M. The Drug Overdose Epidemic and Deceased-Donor Transplantation in the United States: A National Registry Study. Ann. Intern. Med. 2018, 168, 702–711. [Google Scholar] [CrossRef]
- van Amsterdam, J.; Pierce, M.; van den Brink, W. Is Europe Facing an Emerging Opioid Crisis Comparable to the U.S.? Ther. Drug Monit. 2021, 43, 42–51. [Google Scholar] [CrossRef]
- Girolami, I.; Pantanowitz, L.; Marletta, S.; Hermsen, M.; van der Laak, J.; Munari, E.; Furian, L.; Vistoli, F.; Zaza, G.; Cardillo, M.; et al. Artificial intelligence applications for pre-implantation kidney biopsy pathology practice: A systematic review. J. Nephrol. 2022, 35, 1801–1808. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-Viremic Donors | Viremic Donors | p-Value |
|---|---|---|---|
| Donors (n) | 44 | 25 | |
| Recipients (n) | 75 | 41 | |
| Donor age (years) | 56 ± 15 | 54 ± 7 | 0.458 |
| Donor gender (m/f) | 45/30 | 33/8 | 0.038 |
| Donor type (BDD/cDCD) | 62/13 | 38/3 | 0.169 |
| HCV viral load (log) | n.a. | 5.5 ± 1.2 | n.a. |
| Recipient age (years) | 57 ± 11 | 54 ± 10 | 0.167 |
| Recipient gender (m/f) | 53/22 | 28/13 | 0.777 |
| Recipient weight (kg) | 72 ± 14 | 76 ± 17 | 0.253 |
| Primary renal disease (CGN, CTIN, ADPKD, DN, vascular, other, unknown) | 16/7/10/11/5/9/17 | 7/2/6/2/1/10/13 | 0.166 |
| ABO group (0/A/B/AB) | 37/32/5/1 | 23/14/3/1 | 0.819 |
| Number of transplant (1/>1) | 67/8 | 33/8 | 0.259 |
| ABDR HLA donor-recipient mismatches | 4.1 ± 1.1 | 4.4 ± 1.1 | 0.272 |
| Last cPRA (%) | 11 ± 28 | 11 ± 28 | 0.861 |
| Cold ischemia time (hours) | 17 ± 5 | 16 ± 6 | 0.414 |
| Induction therapy (Basiliximab/Thymoglobulin/none) | 36/24/16 | 19/10/12 | 0.545 |
| Variable | Non-Viremic Donors | Viremic Donors | p-Value |
|---|---|---|---|
| Recipients (n) | 75 | 41 | |
| Primary no function (%) | 3 (4.2%) | 1 (2.4%) | 0.999 |
| DGF (%) | 22 (29.3%) | 14 (34.1%) | 0.745 |
| BPAR (%) | 9 (12%) | 1 (2.4%) | 0.095 |
| Graft loss (%) | 13 (17.3%) | 7 (17.1%) | 0.999 |
| Patient death (%) | 5 (6.8%) | 4 (9.7%) | 0.718 |
| Last eGFR (mL/min/1.73 m2) | 49 ± 17 (n = 62) | 46 ± 16 (n = 34) | 0.354 |
| Follow up (months) | 25 ± 16 | 21 ± 14 | 0.109 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco, A.; Moreso, F.; Solà-Porta, E.; Beneyto, I.; Esforzado, N.; Gonzalez-Roncero, F.; Sancho, A.; Melilli, E.; Ruiz, J.C.; Galeano, C., on behalf of the Renal Transplantation with HCV Positive Donors Spanish Study Group. Outcome of Kidney Transplants from Viremic and Non-Viremic Hepatitis C Virus Positive Donors into Negative Recipients: Results of the Spanish Registry. J. Clin. Med. 2023, 12, 1773. https://doi.org/10.3390/jcm12051773
Franco A, Moreso F, Solà-Porta E, Beneyto I, Esforzado N, Gonzalez-Roncero F, Sancho A, Melilli E, Ruiz JC, Galeano C on behalf of the Renal Transplantation with HCV Positive Donors Spanish Study Group. Outcome of Kidney Transplants from Viremic and Non-Viremic Hepatitis C Virus Positive Donors into Negative Recipients: Results of the Spanish Registry. Journal of Clinical Medicine. 2023; 12(5):1773. https://doi.org/10.3390/jcm12051773
Chicago/Turabian StyleFranco, Antonio, Francesc Moreso, Eulàlia Solà-Porta, Isabel Beneyto, Núria Esforzado, Francisco Gonzalez-Roncero, Asunción Sancho, Edoardo Melilli, Juan Carlos Ruiz, and Cristina Galeano on behalf of the Renal Transplantation with HCV Positive Donors Spanish Study Group. 2023. "Outcome of Kidney Transplants from Viremic and Non-Viremic Hepatitis C Virus Positive Donors into Negative Recipients: Results of the Spanish Registry" Journal of Clinical Medicine 12, no. 5: 1773. https://doi.org/10.3390/jcm12051773