
Association of Circulating Anti-HLA Donor-Specific Antibodies and Their Characteristics, including C1q-Binding Capacity, in Kidney Transplant Recipients with Long-Term Renal Graft Outcomes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Detection of Anti-HLA DSAs and Characterization
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
3.2. Characteristics of Anti-HLA DSAs at the Time of Biopsy
3.3. Clinical Outcomes
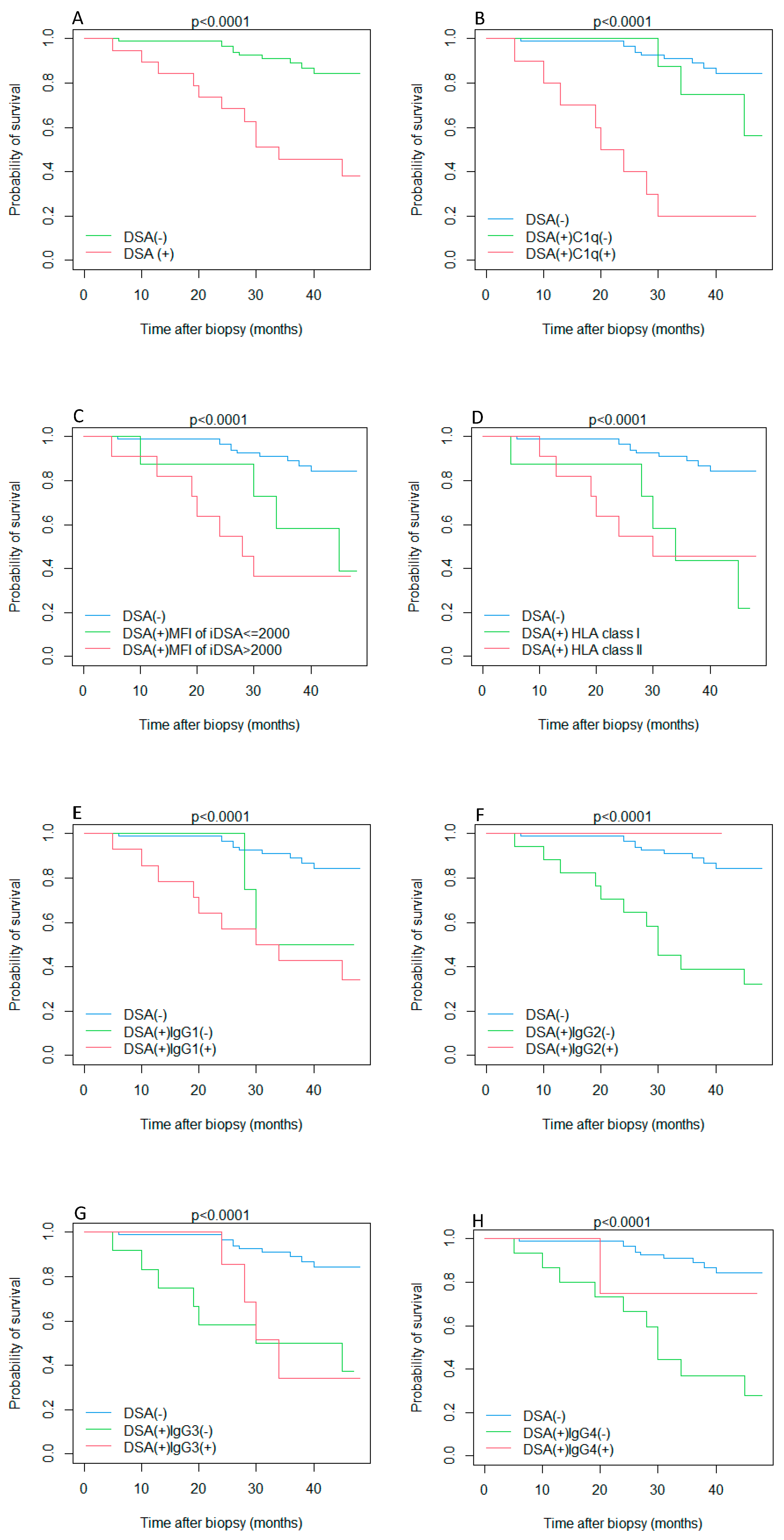
3.4. Survival Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCormick, F.; Held, P.J.; Chertow, G.M. The Terrible Toll of the Kidney Shortage. J. Am. Soc. Nephrol. 2018, 29, 2775–2776. [Google Scholar] [CrossRef] [PubMed]
- Coemans, M.; Süsal, C.; Döhler, B.; Anglicheau, D.; Giral, M.; Bestard, O.; Legendre, C.; Emonds, M.P.; Kuypers, D.; Molenberghs, G.; et al. Analyses of the short- and long-term graft survival after kidney transplantation in Europe between 1986 and 2015. Kidney Int. 2018, 94, 964–973. [Google Scholar] [CrossRef]
- Sellarés, J.; de Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef]
- Cioni, M.; Nocera, A.; Innocente, A.; Tagliamacco, A.; Trivelli, A.; Basso, S.; Quartuccio, G.; Fontana, I.; Magnasco, A.; Drago, F.; et al. De Novo Donor-Specific HLA Antibodies Developing Early or Late after Transplant Are Associated with the Same Risk of Graft Damage and Loss in Nonsensitized Kidney Recipients. J. Immunol. Res. 2017, 2017, 1747030. [Google Scholar] [CrossRef]
- El Band, J.E.K.; Llorente, S.; Martinez-Garcia, P.; Alfaro, R.; Jimenez-Coll, V.; Boix, F.; Galián, J.A.; Martinez-Banaclocha, H.; Botella, C.; Moya-Quiles, M.R.; et al. Evaluation of Antibodies Directed Against Two GPCRs, Anti-AT1R and Anti-ETAR, on Kidney Transplant Outcome. Curr. Protein Pept. Sci. 2021, 22, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Filippone, E.J.; Farber, J.L. Histologic Antibody-mediated Kidney Allograft Rejection in the Absence of Donor-specific HLA Antibodies. Transplantation 2021, 105, e181–e190. [Google Scholar] [CrossRef]
- Hung, S.Y.; Lin, T.M.; Chang, M.Y.; Wang, H.H.; Lee, Y.C.; Ho, L.C.; Chen, Y.T.; Hung, C.M.; Liou, H.H. Risk factors of sensitization to human leukocyte antigen in end-stage renal disease patients. Hum. Immunol. 2014, 75, 531–535. [Google Scholar] [CrossRef]
- Yeung, M.Y. Pre-formed DSA and kidney allograft outcomes. Braz. J. Nephrol. 2020, 42, 136–137. [Google Scholar] [CrossRef] [PubMed]
- Oweira, H.; Ramouz, A.; Ghamarnejad, O.; Khajeh, E.; Ali-Hasan-Al-Saegh, S.; Nikbakhsh, R.; Reißfelder, C.; Rahbari, N.; Mehrabi, A.; Sadeghi, M. Risk Factors of Rejection in Renal Transplant Recipients: A Narrative Review. J. Clin. Med. 2022, 11, 1392. [Google Scholar] [CrossRef] [PubMed]
- Olszowska-Zaremba, N.; Zagożdżon, R.; Gozdowska, J. Accuracy of virtual crossmatch (VXM) prediction of physical crossmatch (PXM) results of donor specific antibody (DSA) in routine pretransplant settings-a single-center experience. Transpl. Immunol. 2022, 72, 101583. [Google Scholar] [CrossRef]
- Leal, R.; Pardinhas, C.; Martinho, A.; Sá, H.O.; Figueiredo, A.; Alves, R. Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss. J. Clin. Med. 2022, 11, 5753. [Google Scholar] [CrossRef]
- Matignon, M.; Pilon, C.; Commereuc, M.; Grondin, C.; Leibler, C.; Kofman, T.; Audard, V.; Cohen, J.; Canoui-Poitrine, F.; Grimbert, P. Intravenous immunoglobulin therapy in kidney transplant recipients with de novo DSA: Results of an observational study. PLoS ONE 2017, 12, e0178572. [Google Scholar] [CrossRef]
- Heilman, R.L.; Nijim, A.; Desmarteau, Y.M.; Khamash, H.; Pando, M.J.; Smith, M.L.; Chakkera, H.A.; Huskey, J.; Valdez, R.; Reddy, K.S. De novo donor-specific human leukocyte antigen antibodies early after kidney transplantation. Transplantation 2014, 98, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Tambur, A.R.; Campbell, P.; Chong, A.S.; Feng, S.; Ford, M.L.; Gebel, H.; Gill, R.G.; Kelsoe, G.; Kosmoliaptsis, V.; Mannon, R.B.; et al. Sensitization in transplantation: Assessment of risk (STAR) 2019 Working Group Meeting Report. Am. J. Transplant. 2020, 20, 2652–2668. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Jorgensen, D.R.; Mehta, R.B.; Sood, P.; Puttarajappa, C.M.; Wu, C.M.; Tevar, A.D.; Molinari, M.; Zeevi, A.; Hariharan, S. The Clinical Impact of Anti-HLA Donor Specific Antibody Detection Through First Year Screening on Stable Kidney Transplant Recipients. Transpl. Int. 2022, 35, 10094. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Watarai, Y.; Takeda, A.; Tsujita, M.; Hiramitsu, T.; Goto, N.; Narumi, S.; Katayama, A.; Morozumi, K.; Uchida, K.; et al. De Novo Anti-HLA DSA Characteristics and Subclinical Antibody-Mediated Kidney Allograft Injury. Transplantation 2016, 100, 2194–2202. [Google Scholar] [CrossRef]
- Nakamura, K.; Sawada, A.; Kita, Y.; Kono, J.; Masui, K.; Sato, T.; Sano, T.; Goto, T.; Akamatsu, S.; Ogawa, O.; et al. Clinical characteristics of renal transplant recipients who developed de novo donor-specific antigen in Kyoto University Hospital: A case series. Ren. Replace Ther. 2022, 8, 10. [Google Scholar] [CrossRef]
- Wu, K.; Schmidt, D.; López Del Moral, C.; Osmanodja, B.; Lachmann, N.; Zhang, Q.; Halleck, F.; Choi, M.; Bachmann, F.; Ronicke, S.; et al. Poor Long-Term Renal Allograft Survival in Patients with Chronic Antibody-Mediated Rejection, Irrespective of Treatment-A Single Center Retrospective Study. J. Clin. Med. 2021, 11, 199. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Viglietti, D.; Bentlejewski, C.; Duong van Huyen, J.P.; Vernerey, D.; Aubert, O.; Verine, J.; Jouven, X.; Legendre, C.; Glotz, D.; et al. IgG Donor-Specific Anti-Human HLA Antibody Subclasses and Kidney Allograft Antibody-Mediated Injury. J. Am. Soc. Nephrol. 2016, 27, 293–304. [Google Scholar] [CrossRef]
- Tatapudi, V.S.; Kopchaliiska, D.; da Gente, G.J.; Buenaventura, O.F.; Singh, M.; Laszik, Z.; Adey, D.B.; Rajalingam, R. Solid-Phase C1q/C3d Fixing Readouts Correlate with High Median Fluorescence Intensity (MFI) De Novo Donor-Specific HLA Antibodies and C4d⁺ Antibody-Mediated Rejection in Kidney Transplant Recipients. Ann. Transplant. 2021, 26, e934175. [Google Scholar] [CrossRef]
- Butiu, M.; Obrisca, B.; Sibulesky, L.; Bakthavatsalam, R.; Smith, K.D.; Gimferrer, I.; Warner, P.; Ismail, G.; Leca, N. Donor-derived Cell-free DNA Complements De Novo Class II DSA in Detecting Late Alloimmune Injury Post Kidney Transplantation. Transpl. Direct 2022, 8, e1285. [Google Scholar] [CrossRef] [PubMed]
- Willicombe, M.; Roufosse, C.; Brookes, P.; Galliford, J.W.; McLean, A.G.; Dorling, A.; Warrens, A.N.; Cook, T.H.; Cairns, T.D.; Taube, D. Antibody-mediated rejection after alemtuzumab induction: Incidence, risk factors, and predictors of poor outcome. Transplantation 2011, 92, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, C.; Loupy, A.; Hill, G.S.; Andrade, J.; Nochy, D.; Antoine, C.; Gautreau, C.; Charron, D.; Glotz, D.; Suberbielle-Boissel, C. Preexisting donor-specific HLA antibodies predict outcome in kidney transplantation. J. Am. Soc. Nephrol. 2010, 21, 1398–1406. [Google Scholar] [CrossRef]
- Mizutani, K.; Terasaki, P.; Hamdani, E.; Esquenazi, V.; Rosen, A.; Miller, J.; Ozawa, M. The importance of anti-HLA-specific antibody strength in monitoring kidney transplant patients. Am. J. Transplant. 2007, 7, 1027–1031. [Google Scholar] [CrossRef]
- Malheiro, J.; Tafulo, S.; Dias, L.; Martins, S.; Fonseca, I.; Beirão, I.; Castro-Henriques, A.; Cabrita, A. Determining donor-specific antibody C1q-binding ability improves the prediction of antibody-mediated rejection in human leucocyte antigen-incompatible kidney transplantation. Transpl. Int. 2017, 30, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Lefaucheur, C.; Vernerey, D.; Prugger, C.; Duong van Huyen, J.P.; Mooney, N.; Suberbielle, C.; Frémeaux-Bacchi, V.; Méjean, A.; Desgrandchamps, F.; et al. Complement-binding anti-HLA antibodies and kidney-allograft survival. N. Engl. J. Med. 2013, 369, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Yell, M.; Muth, B.L.; Kaufman, D.B.; Djamali, A.; Ellis, T.M. C1q Binding Activity of De Novo Donor-specific HLA Antibodies in Renal Transplant Recipients With and Without Antibody-mediated Rejection. Transplantation 2015, 99, 1151–1155. [Google Scholar] [CrossRef]
- Navas, A.; Molina, J.; Agüera, M.L.; Guler, I.; Jurado, A.; Rodríguez-Benot, A.; Alonso, C.; Solana, R. Characterization of the C1q-Binding Ability and the IgG1-4 Subclass Profile of Preformed Anti-HLA Antibodies by Solid-Phase Assays. Front. Immunol. 2019, 10, 1712. [Google Scholar] [CrossRef]
- Schaub, S.; Hönger, G.; Amico, P. The complexity of the humoral immune response against HLA antigens. Transpl. Int. 2014, 27, 249–250. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Hönger, G.; Hopfer, H.; Arnold, M.L.; Spriewald, B.M.; Schaub, S.; Amico, P. Pretransplant IgG subclasses of donor-specific human leukocyte antigen antibodies and development of antibody-mediated rejection. Transplantation 2011, 92, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Freitas, M.C.; Rebellato, L.M.; Ozawa, M.; Nguyen, A.; Sasaki, N.; Everly, M.; Briley, K.P.; Haisch, C.E.; Bolin, P.; Parker, K.; et al. The role of immunoglobulin-G subclasses and C1q in de novo HLA-DQ donor-specific antibody kidney transplantation outcomes. Transplantation 2013, 95, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Snanoudj, R.; Kamar, N.; Cassuto, E.; Caillard, S.; Metzger, M.; Merville, P.; Thierry, A.; Jollet, I.; Grimbert, P.; Anglicheau, D.; et al. Epitope load identifies kidney transplant recipients at risk of allosensitization following minimization of immunosuppression. Kidney Int. 2019, 95, 1471–1485. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Cherukuri, A.; Mehta, R.B.; Sood, P.; Hariharan, S. High Calcineurin Inhibitor Intrapatient Variability Is Associated With Renal Allograft Inflammation, Chronicity, and Graft Loss. Transplant. Direct 2019, 5, e424. [Google Scholar] [CrossRef]
- Coti, I.; Wenda, S.; Andreeva, A.; Kocher, A.; Laufer, G.; Fischer, G.; Andreas, M. Donor-specific HLA antibodies after fresh decellularized vs. cryopreserved native allograft implantation. Hla 2020, 96, 580–588. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Louis, K.; Morris, A.B.; Taupin, J.L.; Nickerson, P.; Tambur, A.R.; Gebel, H.M.; Reed, E.F. Clinical recommendations for posttransplant assessment of anti-HLA (Human Leukocyte Antigen) donor-specific antibodies: A Sensitization in Transplantation: Assessment of Risk consensus document. Am. J. Transplant. 2023, 23, 115–132. [Google Scholar] [CrossRef]
- Aubert, O.; Loupy, A.; Hidalgo, L.; Duong van Huyen, J.-P.; Higgins, S.; Viglietti, D.; Jouven, X.; Glotz, D.; Legendre, C.; Lefaucheur, C.; et al. Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients. J. Am. Soc. Nephrol. 2017, 28, 1912–1923. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Mirocha, J.; Reinsmoen, N.L.; Vo, A.A.; Choi, J.; Kahwaji, J.M.; Peng, A.; Villicana, R.; Jordan, S.C. Differences in pathologic features and graft outcomes in antibody-mediated rejection of renal allografts due to persistent/recurrent versus de novo donor-specific antibodies. Kidney Int. 2017, 91, 729–737. [Google Scholar] [CrossRef]
- Madill-Thomsen, K.S.; Böhmig, G.A.; Bromberg, J.; Einecke, G.; Eskandary, F.; Gupta, G.; Hidalgo, L.G.; Myslak, M.; Viklicky, O.; Perkowska-Ptasinska, A.; et al. Donor-Specific Antibody Is Associated with Increased Expression of Rejection Transcripts in Renal Transplant Biopsies Classified as No Rejection. J. Am. Soc. Nephrol. 2021, 32, 2743–2758. [Google Scholar] [CrossRef]
- Loupy, A.; Hill, G.S.; Suberbielle, C.; Charron, D.; Anglicheau, D.; Zuber, J.; Timsit, M.O.; Duong, J.P.; Bruneval, P.; Vernerey, D.; et al. Significance of C4d Banff scores in early protocol biopsies of kidney transplant recipients with preformed donor-specific antibodies (DSA). Am. J. Transplant. 2011, 11, 56–65. [Google Scholar] [CrossRef]
- Einecke, G.; Sis, B.; Reeve, J.; Mengel, M.; Campbell, P.M.; Hidalgo, L.G.; Kaplan, B.; Halloran, P.F. Antibody-mediated microcirculation injury is the major cause of late kidney transplant failure. Am. J. Transplant. 2009, 9, 2520–2531. [Google Scholar] [CrossRef]
- Lebraud, E.; Eloudzeri, M.; Rabant, M.; Lamarthée, B.; Anglicheau, D. Microvascular Inflammation of the Renal Allograft: A Reappraisal of the Underlying Mechanisms. Front. Immunol. 2022, 13, 864730. [Google Scholar] [CrossRef] [PubMed]
- Gosset, C.; Viglietti, D.; Rabant, M.; Vérine, J.; Aubert, O.; Glotz, D.; Legendre, C.; Taupin, J.L.; Duong Van-Huyen, J.P.; Loupy, A.; et al. Circulating donor-specific anti-HLA antibodies are a major factor in premature and accelerated allograft fibrosis. Kidney Int. 2017, 92, 729–742. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, E.; Lamarthée, B.; Barba, T.; Claes, S.; Coemans, M.; de Loor, H.; Emonds, M.P.; Koshy, P.; Kuypers, D.; Proost, P.; et al. Circulating Donor-Specific Anti-HLA Antibodies Associate With Immune Activation Independent of Kidney Transplant Histopathological Findings. Front. Immunol. 2022, 13, 818569. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Palanisamy, A.; Tsapepas, D.; Tanriover, B.; Crew, R.J.; Dube, G.; Ratner, L.E.; Cohen, D.J.; Radhakrishnan, J. Donor-specific antibodies adversely affect kidney allograft outcomes. J. Am. Soc. Nephrol. 2012, 23, 2061–2071. [Google Scholar] [CrossRef]
- Terasaki, P.I.; Ozawa, M.; Castro, R. Four-year follow-up of a prospective trial of HLA and MICA antibodies on kidney graft survival. Am. J. Transplant. 2007, 7, 408–415. [Google Scholar] [CrossRef]
- Parajuli, S.; Joachim, E.; Alagusundaramoorthy, S.; Aziz, F.; Blazel, J.; Garg, N.; Muth, B.; Mohamed, M.; Redfield, R.R.; Mandelbrot, D.A.; et al. Donor-Specific Antibodies in the Absence of Rejection Are Not a Risk Factor for Allograft Failure. Kidney Int. Rep. 2019, 4, 1057–1065. [Google Scholar] [CrossRef]
- Kang, Z.Y.; Liu, C.; Liu, W.; Li, D.H. Effect of C1q-binding donor-specific anti-HLA antibodies on the clinical outcomes of patients after renal transplantation: A systematic review and meta-analysis. Transpl. Immunol. 2022, 72, 101566. [Google Scholar] [CrossRef]
- Murata, K.; Baldwin, W.M., 3rd. Mechanisms of complement activation, C4d deposition, and their contribution to the pathogenesis of antibody-mediated rejection. Transplant. Rev. 2009, 23, 139–150. [Google Scholar] [CrossRef]
- Patel, J.K.; Coutance, G.; Loupy, A.; Dilibero, D.; Hamilton, M.; Kittleson, M.; Kransdorf, E.; Azarbal, B.; Seguchi, O.; Zhang, X.; et al. Complement inhibition for prevention of antibody-mediated rejection in immunologically high-risk heart allograft recipients. Am. J. Transplant. 2021, 21, 2479–2488. [Google Scholar] [CrossRef]
- Viglietti, D.; Bouatou, Y.; Kheav, V.D.; Aubert, O.; Suberbielle-Boissel, C.; Glotz, D.; Legendre, C.; Taupin, J.L.; Zeevi, A.; Loupy, A.; et al. Complement-binding anti-HLA antibodies are independent predictors of response to treatment in kidney recipients with antibody-mediated rejection. Kidney Int. 2018, 94, 773–787. [Google Scholar] [CrossRef] [PubMed]
- Sigurjonsdottir, V.K.; Purington, N.; Chaudhuri, A.; Zhang, B.M.; Fernandez-Vina, M.; Palsson, R.; Kambham, N.; Charu, V.; Piburn, K.; Maestretti, L.; et al. Complement-Binding Donor-Specific Anti-HLA Antibodies: Biomarker for Immunologic Risk Stratification in Pediatric Kidney Transplantation Recipients. Transpl. Int. 2022, 35, 10158. [Google Scholar] [CrossRef]
- Lowe, D.; Higgins, R.; Zehnder, D.; Briggs, D.C. Significant IgG subclass heterogeneity in HLA-specific antibodies: Implications for pathogenicity, prognosis, and the rejection response. Hum. Immunol. 2013, 74, 666–672. [Google Scholar] [CrossRef]
- Ponsirenas, R.V.G.; Cazarote, H.B.; Araújo, S.A.; Wanderley, D.C.; Shimakura, S.; Valdameri, J.S.; Contieri, F.L.C.; von Glehn, C.; Susin, M.F.; Sotomaior, V.S. Anti-HLA Donor-Specific IgG Subclasses and C1q-binding Evolution in Posttransplant Monitoring. Transpl. Direct 2018, 4, e385. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.M.; Jackson, K.J. A Temporal Model of Human IgE and IgG Antibody Function. Front. Immunol. 2013, 4, 235. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, F.M.; Roth, I.; Rebmann, V.; Arnold, M.L.; Witzke, O.; Wilde, B.; Spriewald, B.M.; Grosse-Wilde, H. Immunoglobulin isotype-specific characterization of anti-human leukocyte antigen antibodies eluted from explanted renal allografts. Hum. Immunol. 2007, 68, 500–506. [Google Scholar] [CrossRef]
- Gu, Y.; Koh, R.W.K.; Lai, M.L.; Pochinco, D.; Teo, R.Z.C.; Chan, M.; Murali, T.M.; Liew, C.W.; Wong, Y.H.; Gascoigne, N.R.J.; et al. Defining the structural basis for human leukocyte antigen reactivity in clinical transplantation. Sci. Rep. 2020, 10, 18397. [Google Scholar] [CrossRef]


{kind=link}
| All Patients (N = 108) | DSA (−) (N = 89) | DSA (+) (N = 19) | p-Value | |
|---|---|---|---|---|
| Recipient characteristic | ||||
| Age at biopsy, years, median (Q1–Q3) | 48.5 (38.8–61.0) | 46.0 (38.0–61.0) | 54.0 (44.0–58.5) | 0.6054 |
| Male, n (%) | 69 (63.9%) | 58 (65.2%) | 11 (57.9%) | 0.7368 |
| Body mass index at biopsy, kg/m2, mean ± SD | 25.24 ± 3.848 | 25.52 ± 3.934 | 23.93 ± 3.188 | 0.1031 |
| Previous transplantation, n (%) | 19 (17.6%) | 4 (4.4%) | 15 (78.9%) | <0.0001 |
| Renal replacement therapy, n (%) | 0.6326 | |||
| Pre-emptive transplantation | 12 (11.1%) | 11 (12.4%) | 1 (5.3%) | |
| Hemodialysis | 83 (76.9%) | 67 (75.2%) | 16 (84.1%) | |
| Peritoneal dialysis | 13 (12.0%) | 11 (12.4%) | 2 (10.6%) | |
| Cause of ESRD, n (%) | 0.2384 | |||
| Glomerulonephritis | 48 (44.4%) | 36 (40.4%) | 12 (63.2%) | |
| ADPKD | 19 (17.6%) | 15 (16.8%) | 4 (21.1%) | |
| Diabetes | 16 (14.8%) | 14 (15.7%) | 2 (10.5%) | |
| Congenital anomaly | 5 (4.6%) | 5 (5.6%) | 0 | |
| Other | 20 (18.5%) | 19 (21.5%) | 1 (5.2%) | |
| Diabetes, n (%) | 31 (28.7%) | 26 (29.2%) | 5 (26.3%) | |
| Donor characteristic | ||||
| Age, years, mean ± SD | 46.2 ± 14.88 | 45.0 ± 14.9 | 52.0 ± 13.8 | 0.0616 |
| Male, n (%) | 68 (63.0%) | 58 (65.2%) | 10 (52.6%) | 0.4439 |
| Transplant characteristic | ||||
| Cold ischemia time, minutes, mean ± SD | 1268 ± 575.4 | 1239 ± 582.9 | 1416 ± 559.8 | 0.4972 |
| Induction therapy, n (%) | <0.0001 | |||
| None | 75 (69.4%) | 70 (78.7%) | 5 (26.3%) | |
| Basiliximab | 18 (16.7%) | 10 (11.2%) | 8 (42.1%) | |
| ATG | 15 (13.9%) | 9 (10.1%) | 6 (31.6%) | |
| HLA mismatches, median, (Q1–Q3) | ||||
| A | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–1.5) | 0.5127 |
| B | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.4485 |
| DR | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 0.1550 |
| Total | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) | 0.4000 |
| Panel-reactive antibody >5%, n (%) | 15 (13.9%) | 8 (9.0%) | 7 (36.8%) | 0.0048 |
| Panel-reactive antibody, median (Q1–Q3) [min–max] | 0 (0–0) [0–86] | 0 (0–0) [0–86] | 0 (0–18.5) [0–66] | 0.0043 |
| Clinical characteristic | ||||
| Immunosuppression, n (%) | 0.3223 | |||
| Tacrolimus | 106 (98.1%) | 88 (89.9%) | 18 (94.7%) | |
| Cyclosporine | 2 (1.9%) | 1 (1.1%) | 1 (5.3%) | |
| eGFR at biopsy, mL/min/1.73 m2, mean ± SD | 53.2 ± 20.76 | 54.6 ± 21.24 | 46.3 ± 17.19 | 0.1107 |
| Proteinuria at biopsy ≥ 50 mg/dL, n (%) | 16 (14.8%) | 11 (12.6%) | 5 (26.3%) | 0.2306 |
| Proteinuria at biopsy, median (Q1–Q3) [min–max] | 0 (0–10.0) [0–100] | 0 (0–10.0) [0–100] | 0 (0–30.0) [0–50] | 0.1363 |
| Protocol biopsy n (%) | 61 (56.5%) | 52 (58.4%) | 9 (47.4%) | 0.4483 |
| Time from transplantation to biopsy, months, median (Q1–Q3) | 5.0 (3.0–12.0) | 5.0 (3.0–12.0) | 4.0 (3.0–10.5) | 0.4374 |
| ABMR at the time of biopsy, n (%) | 9 (8.3%) | 5 (5.6%) | 4 (21.0%) | 0.0492 |
| C4d in biopsy, n (%) | 14 (13.0%) | 10 (11.2%) | 4 (21.1%) | 0.2651 |
| Anti-HLA DSA before transplantation, n (%) | 18 (16.7%) | 9 (10.1%) | 9 (47.4%) | 0.0005 |
| Number, median (Q1–Q3) | 1.0 (1.0–1.8) | 1.0 (1.0–1.0) | 1.0 (1.0–2.0) | 0.5008 |
| Anti-HLA DSA class, n | 1 | |||
| I | 11 | 6 | 5 | |
| II | 6 | 3 | 3 | |
| I + II | 1 | 0 | 1 | |
| MFI of immunodominant anti-HLA DSA before transplantation, mean (SD) | 2009 ± 1230.5 | 1807 ± 1347.3 | 2211 ± 1144.6 | 0.5022 |
| All Anti-HLA DSA | |
|---|---|
| Number, median (Q1–Q3) | 1.0 (1.0–1.0) |
| HLA class specificity, n (%) | |
| I | 7 (36.8) |
| II | 10 (52.6) |
| I + II | 2 (10.5) |
| iDSA | |
| HLA class specificity, n (%) | |
| I | 8 (42.1) |
| II | 11 (57.9) |
| MFI, median (Q1–Q3) | 2900 (1284–4648) |
| C1q binding, n (%) | 10 (52.6) |
| IgG subclasses, n (%) | |
| IgG1 | 14 (73.7) |
| IgG2 | 2 (10.5) |
| IgG3 | 7 (36.8) |
| IgG4 | 4 (21.1) |
| All Patients (N = 108) | DSA (−) (N = 89) | DSA (+) (N = 19) | p-Value | |
|---|---|---|---|---|
| Follow-up postbiopsy, months, median (Q1–Q3) | 39.0 (29.8–45.0) | 37.0 (28.0–44.0) | 44.0 (37.5–47.0) | 0.0631 |
| eGFR at the end of follow-up, mL/min/1.73 m2, median (Q1–Q3) | 48.0 (33.0–62.0) | 51.5 (34.8–63.3) | 36.0 (26.0–42.0) | 0.0049 |
| Proteinuria at the end of follow-up, ≥50 mg/dL, n (%) | 6 (5.6) | 3 (3.4) | 3 (15.8) | 0.1110 |
| Proteinuria at the end of follow-up, median (Q1–Q3) [min–max] | 0 (0–0) [0–311.0] | 0 (0–0) [0–311.0] | 0 (0–6.8) [0–81.0] | 0.4113 |
| >30% decline in eGFR, n (%) | 20 (18.5) | 9 (10.1) | 11 (57.9) | <0.0001 |
| Death-censored graft loss, n (%) | 4 (3.7) | 1 (1.1) | 3 (15.8) | 0.0168 |
| Combined endpoint, >30% decline in eGFR or graft loss, n (%) | 21 (19.4) | 10 (11.2) | 11 (57.9) | <0.0001 |
| Time from biopsy to combined endpoint, months, mean ± SD | 25.0 ± 10.69 | 26.9 ± 9.79 | 23.4 ± 11.60 | 0.482 |
| Death event, n (%) | 6 (5.6) | 4 (4.4) | 2 (10.5) | 0.2842 |
| Univariate | Multivariate 1 | Multivariate 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Recipient characteristic | |||||||||
| Age at biopsy (per 1-year increase) | 1.001 | 0.969–1.035 | 0.9486 | ||||||
| Male (vs. female) | 1.291 | 0.518–3.216 | 0.5835 | ||||||
| Body mass index at biopsy (per 1 kg/m2 increase) | 0.953 | 0.855–1.063 | 0.3918 | ||||||
| Previous transplantation (yes vs. no) | 3.728 | 1.568–8.864 | 0.0029 | ||||||
| Renal replacement therapy | |||||||||
| Pre-emptive | Ref. | ||||||||
| Hemodialysis | 0.821 | 0.239–2.822 | 0.754 | ||||||
| Peritoneal dialysis | 0.761 | 0.127–4.571 | 0.765 | ||||||
| Donor characteristic | |||||||||
| Age (per 1-year increase) | 1.045 | 1.010–1.081 | 0.0106 | 1.034 | 1.002–1.067 | 0.0382 | 1.040 | 1.005–1.077 | 0.0259 |
| Male (vs. female) | 0.353 | 0.146–0.852 | 0.0205 | ||||||
| Transplant characteristic | |||||||||
| Induction therapy | |||||||||
| No | Ref. | ||||||||
| Basiliximab | 3.294 | 1.224–8.862 | 0.0182 | ||||||
| ATG | 2.925 | 0.980–8.735 | 0.0545 | ||||||
| Total HLA mismatches (per 1-mismatch increase) | 1.349 | 0.860–2.116 | 0.1925 | ||||||
| Panel-reactive antibody >5% (vs. ≤5%) | 1.309 | 0.479–3.579 | 0.5993 | ||||||
| Clinical characteristic | |||||||||
| eGFR at biopsy (per 1-mL/min/1.73 m2 increase) | 0.992 | 0.971–1.013 | 0.4490 | ||||||
| Proteinuria at biopsy ≥50 mg/dL (vs. <50 mg/dL) | 2.628 | 1.019–6.776 | 0.0457 | 2.612 | 1.006–6.783 | 0.0486 | 3.504 | 1.281–9.588 | 0.0146 |
| ABMR at the time of biopsy (yes vs. no) | 2.361 | 0.692–8.054 | 0.1698 | ||||||
| C4d in biopsy (yes vs. no) | 1.426 | 0.479–4.245 | 0.5234 | ||||||
| Anti-HLA DSAs before transplantation (yes vs. no) | 3.031 | 1.221–7.524 | 0.0168 | ||||||
| Anti-HLA DSAs at biopsy (yes vs. no) * | 6.01 | 2.546–14.190 | <0.0001 | 5.133 | 2.150–12.253 | 0.0002 | |||
| C1q-binding status | |||||||||
| No anti-HLA DSAs at biopsy ** | Ref. | Ref. | |||||||
| Anti-HLA DSAs (+) C1q (−) at biopsy ** | 2.501 | 0.687–9.107 | 0.164 | 1.927 | 0.524–7.084 | 0.3236 | |||
| Anti-HLA DSAs (+) C1q (+) at biopsy ** | 12.844 | 5.010–32.926 | <0.0001 | 14.639 | 5.320–40.283 | <0.0001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gniewkiewicz, M.; Czerwinska, K.; Zielniok, K.; Durlik, M. Association of Circulating Anti-HLA Donor-Specific Antibodies and Their Characteristics, including C1q-Binding Capacity, in Kidney Transplant Recipients with Long-Term Renal Graft Outcomes. J. Clin. Med. 2023, 12, 1312. https://doi.org/10.3390/jcm12041312
Gniewkiewicz M, Czerwinska K, Zielniok K, Durlik M. Association of Circulating Anti-HLA Donor-Specific Antibodies and Their Characteristics, including C1q-Binding Capacity, in Kidney Transplant Recipients with Long-Term Renal Graft Outcomes. Journal of Clinical Medicine. 2023; 12(4):1312. https://doi.org/10.3390/jcm12041312
Chicago/Turabian StyleGniewkiewicz, Michal, Katarzyna Czerwinska, Katarzyna Zielniok, and Magdalena Durlik. 2023. "Association of Circulating Anti-HLA Donor-Specific Antibodies and Their Characteristics, including C1q-Binding Capacity, in Kidney Transplant Recipients with Long-Term Renal Graft Outcomes" Journal of Clinical Medicine 12, no. 4: 1312. https://doi.org/10.3390/jcm12041312