
The Protective Role of Cognitive Reserve in Mild Cognitive Impairment: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
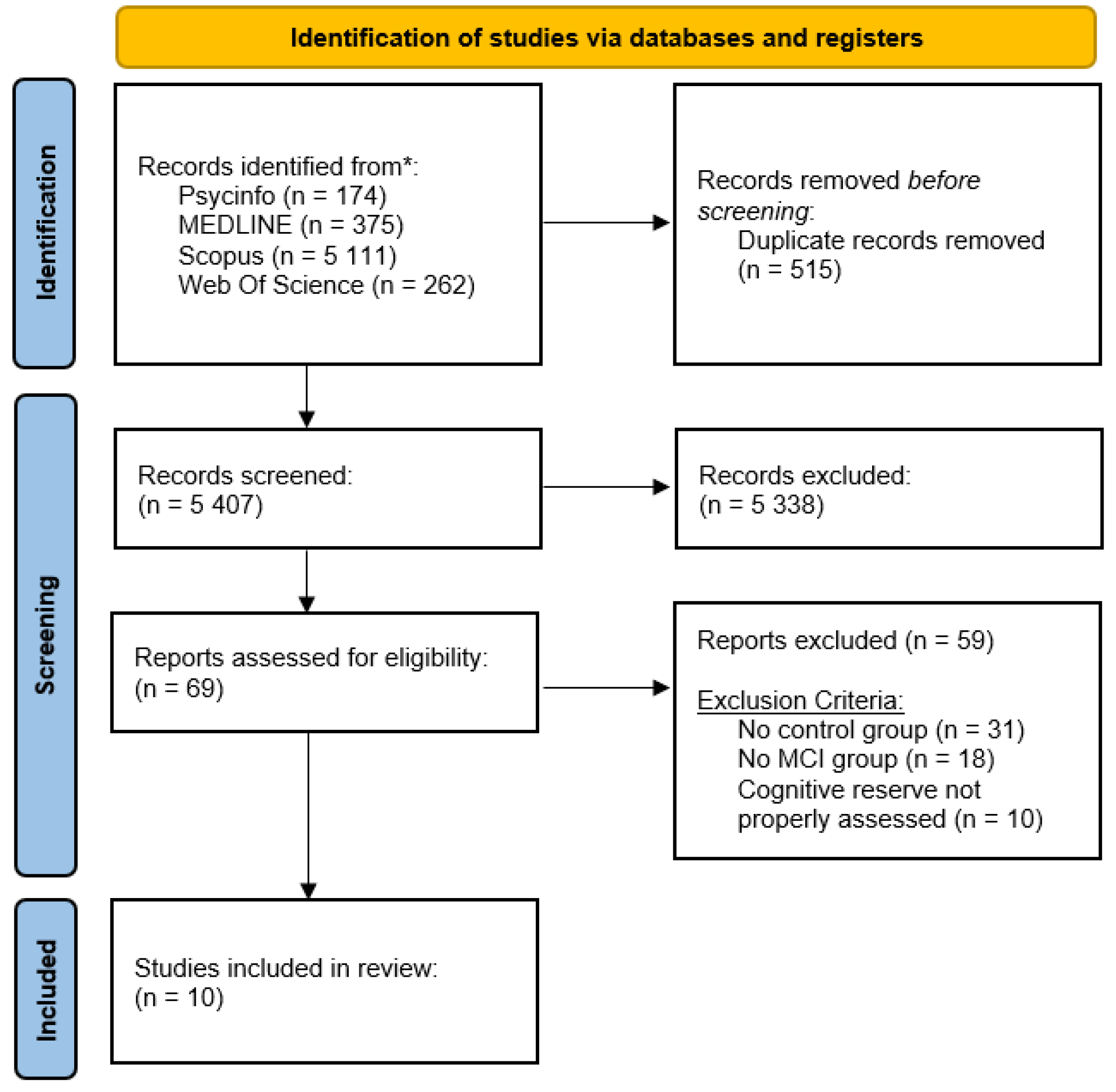
2.1. Research Strategies
2.2. Eligibility Criteria
2.3. Data Collection
2.4. Quality Assessment
- (I)
- attrition bias (i.e., biases caused by the utilization of incomplete outcome data);
- (II)
- reporting bias (i.e., bias due to selective outcome reporting or not reporting relevant results);
- (III)
- sample bias (i.e., bias resulting in samples that do not represent the general population, undermining the generalization of results, or articles reporting scarce demographic information, such as the male/female ratio, participants’ mean age, and schooling years);
- (IV)
- measurement bias (i.e., bias due to using non-validated tasks to measure cognitive reserve or non-specific tasks to measure cognitive functioning).
3. Results
3.1. Publication Bias
3.2. Diagnostic Criteria
3.3. Cognitive Reserve Assessment
3.4. Cognitive Functioning Assessment
3.5. Results of the Selected Studies
3.5.1. Longitudinal Studies
3.5.2. Cross-Sectional Studies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y.; Barnes, C.A.; Grady, C.; Jones, R.N.; Raz, N. Brain reserve, cognitive reserve, compensation, and maintenance: Operationalization, validity, and mechanisms of cognitive resilience. Neurobiol. Aging 2019, 83, 124–129. [Google Scholar] [CrossRef]
- Pettigrew, C.; Soldan, A. Defining Cognitive Reserve and Implications for Cognitive Aging. Curr. Neurol. Neurosci. Rep. 2019, 19, 1. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Chapko, D.; Mccormack, R.; Black, C.; Staff, R.; Murray, A.; Chapko, D.; Mccormack, R.; Black, C.; Staff, R. Life-course determinants of cognitive reserve (CR) in cognitive aging and dementia—A systematic literature review. Aging Ment. Health 2018, 22, 7863. [Google Scholar] [CrossRef]
- Meng, X.; Arcy, C.D. Education and Dementia in the Context of the Cognitive Reserve Hypothesis: A Systematic Review with Meta-Analyses and Qualitative Analyses. PLoS ONE 2012, 7, e38268. [Google Scholar] [CrossRef]
- Nelson, M.E.; Jester, D.J.; Petkus, A.J.; Andel, R. Cognitive Reserve, Alzheimer’s Neuropathology, and Risk of Dementia: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2021, 31, 233–250. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Guarino, A.; Forte, G.; Giovannoli, J.; Casagrande, M. Executive functions in the elderly with mild cognitive impairment: A systematic review on motor and cognitive inhibition, conflict control and cognitive flexibility. Aging Ment. Health 2020, 24, 1028–1045. [Google Scholar] [CrossRef] [PubMed]
- Corbo, I.; Casagrande, M. Higher-Level Executive Functions in Healthy Elderly and Mild Cognitive Impairment: A Systematic Review. J. Clin. Med. 2022, 11, 1204. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Forte, G.; Francesca, F.; Corbo, I. Sleep Quality and Aging: A Systematic Review on Healthy Older People, Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2022, 19, 8457. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 341–354. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.A.E.; Hawrylewicz, K.; Grundy, J.G. Does bilingualism protect against dementia? A meta-analysis. Psychon. Bull. Rev. 2020, 27, 952–965. [Google Scholar] [CrossRef]
- Godinho, F.; Maruta, C.; Borbinha, C.; Martins, I.P. Applied Neuropsychology: Adult Effect of education on cognitive performance in patients with mild cognitive impairment. Appl. Neuropsychol. Adult 2022, 29, 1440–1449. [Google Scholar] [CrossRef]
- Haussmann, R.; von Lieresund Wilkau, A.F.E.; Sauer, C.; Nilles, F.; Donix, M. Impact of cognitive reserve on clinical and neuropsychological measures in patients with mild cognitive impairment. Australas. Psychiatry 2020, 28, 386–390. [Google Scholar] [CrossRef]
- Caffò, A.O.; Lopez, A.; Spano, G.; Saracino, G.; Stasolla, F.; Ciriello, G.; Grattagliano, I.; Lancioni, G.E.; Bosco, A. The role of pre-morbid intelligence and cognitive reserve in predicting cognitive efficiency in a sample of Italian elderly The role of pre-morbid intelligence and cognitive reserve in predicting cognitive efficiency in a sample of Italian elderly. Aging Clin. Exp. Res. 2016, 28, 1203–1210. [Google Scholar] [CrossRef]
- Geda, Y.E.; Topazian, H.M.; Lewis, R.A.; Roberts, R.O.; Knopman, D.S.; Pankratz, V.S.; Christianson, T.J.; Boeve, B.F.; Tangalos, E.G.; Ivnik, R.J.; et al. Engaging in Cognitive Activities, Aging, and Mild Cognitive Impairment: A Population-Based Study Yonas. J. Neuropsychiatry Clin. Neurosci. 2011, 23, 149–154. [Google Scholar] [CrossRef]
- Berezuk, C.; Scott, S.C.; Black, S.E.; Zakzanis, K.K. Cognitive reserve, cognition, and real-world functioning in MCI: A systematic review and meta-analysis. J. Clin. Exp. Neuropsychol. 2021, 43, 991–1005. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. Med. Flum. 2021, 57, 444–465. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Linee guida per il reporting di revisioni sistematiche e meta-analisi: Il PRISMA Statement. Evidence 2015, 7, e1000115. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Cai, Z.; Xue, S.; Zhou, X.; Wu, F. Proxies of cognitive reserve and their effects on neuropsychological performance in patients with mild cognitive impairment. J. Clin. Neurosci. 2013, 20, 548–553. [Google Scholar] [CrossRef]
- Kim, H.; Hong, J.P.; Kang, J.M.; Kim, W.H.; Maeng, S.; Cho, S.E.; Na, K.S.; Oh, S.H.; Park, J.W.; Cho, S.J.; et al. Cognitive reserve and the effects of virtual reality-based cognitive training on elderly individuals with mild cognitive impairment and normal cognition. Psychogeriatrics 2021, 21, 552–559. [Google Scholar] [CrossRef]
- Malave, R. The Association between Cognitive Reserve and Time to Conversion from Normal Cognition to Mild Cognitive Impairment; University of Pittsburgh: Pittsburgh, PA, USA, 2015. [Google Scholar]
- Soldan, A.; Pettigrew, C.; Cai, Q.; Wang, J.; Wang, M.C.; Moghekar, A.; Miller, M.I.; Albert, M. Cognitive reserve and long-term change in cognition in aging and preclinical Alzheimer’s disease. Neurobiol. Aging 2017, 60, 164–172. [Google Scholar] [CrossRef]
- Xu, H.; Yang, R.; Dintica, C.; Qi, X.; Song, R.; Bennett, D.A.; Xu, W. Association of lifespan cognitive reserve indicator with the risk of mild cognitive impairment and its progression to dementia. Alzheimer’s Dement. 2020, 16, 873–882. [Google Scholar] [CrossRef]
- Algarabel, S.; Sales, A.; Pitarque, A.; Meléndez, J.C.; Escudero, J.; Mayordomo, T. Associative and Implicit Memory Performance as a Function of Cognitive Reserve in Elderly Adults with and without Mild Cognitive Impairment. Span. J. Psychol. 2016, 19, E4. [Google Scholar] [CrossRef] [Green Version]
- Andrejeva, N.; Knebel, M.; Dos Santos, V.; Schmidt, J.; Herold, C.J.; Tudoran, R.; Wetzel, P.; Wendelstein, B.; Meyer-Kühling, I.; Navratil, S.D.; et al. Neurocognitive deficits and effects of cognitive reserve in mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2016, 41, 199–209. [Google Scholar] [CrossRef]
- Franzmeier, N.; Buerger, K.; Teipel, S.; Stern, Y.; Dichgans, M.; Ewers, M. Cognitive reserve moderates the association between functional network anti-correlations and memory in MCI. Neurobiol. Aging 2017, 50, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Solé-Padullés, C.; Bartrés-Faz, D.; Junqué, C.; Vendrell, P.; Rami, L.; Clemente, I.C.; Bosch, B.; Villar, A.; Bargalló, N.; Jurado, M.A.; et al. Brain structure and function related to cognitive reserve variables in normal aging, mild cognitive impairment and Alzheimer’s disease. Neurobiol. Aging 2009, 30, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Julkunen, V.; Paajanen, T.; Westman, E.; Wahlund, L.O.; Aitken, A.; Sobow, T.; Mecocci, P.; Tsolaki, M.; Vellas, B.; et al. Education increases reserve against Alzheimer’s disease-Evidence from structural MRI analysis. Neuroradiology 2012, 54, 929–938. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment Clinical Characterization and Outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current Concepts in Mild Cognitive Impairment. Arch. Neurol. 2001, 203, 1985–1992. [Google Scholar] [CrossRef]
- Lopez, O.L.; Jagust, W.J.; DeKosky, S.T.; Becker, J.T.; Fitzpatrick, A.; Dulberg, C.; Breitner, J.; Lyketsos, C.; Jones, B.; Kawas, C.; et al. Prevalence and classification of mild cognitive impairment in the cardiovascular health study cognition study. Arch. Neurol. 2003, 60, 1385–1389. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 1994; Volume IV. [Google Scholar]
- Artero, S.; Petersen, R.; Touchon, J.; Ritchie, K. Revised Criteria for Mild Cognitive Impairment: Validation within a Longitudinal Population Study Sylvaine. Dement. Geriatr. Cogn. Disord. 2006, 5, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Mckhann, G.; Drachman, D.; Folstein, M.; Katzman, R. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939. [Google Scholar] [CrossRef] [Green Version]
- Levy, R. Aging-Associated Cognitive Decline. Int. Psychogeratrics 1994, 6, 63–68. [Google Scholar]
- Casagrande, M.; Marselli, G.; Agostini, F.; Forte, G.; Favieri, F.; Guarino, A. The complex burden of determining prevalence rates of mild cognitive impairment: A systematic review. Front. Psychiatry 2022, 13, 960648. [Google Scholar] [CrossRef] [PubMed]
- Vega, J.N.; Newhouse, P.A. Mild Cognitive Impairment: Diagnosis, Longitudinal Course, and Emerging Treatments. Curr. Psychiatry Rep. 2014, 16, 490. [Google Scholar] [CrossRef] [Green Version]
- Cabeza, R.; Albert, M.; Belleville, S.; Craik, F.I.M.; Duarte, A.; Grady, C.L.; Lindenberger, U.; Nyberg, L.; Park, D.C.; Reuter-lorenz, P.A.; et al. Maintenance, reserve and compensation: The cognitive neuroscience of healthy ageing. Nat. Rev. Neurosci. 2017, 19, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Subramaniapillai, S.; Almey, A.; Natasha Rajah, M.; Einstein, G. Sex and gender differences in cognitive and brain reserve: Implications for Alzheimer’s disease in women. Front. Neuroendocrinol. 2021, 60, 100879. [Google Scholar] [CrossRef] [PubMed]
- Giacomucci, G.; Mazzeo, S.; Padiglioni, S.; Bagnoli, S.; Belloni, L.; Ferrari, C.; Bracco, L.; Nacmias, B.; Sorbi, S.; Bessi, V. Gender differences in cognitive reserve: Implication for subjective cognitive decline in women. Neurol. Sci. 2022, 43, 2499–2508. [Google Scholar] [CrossRef]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [Green Version]
- Casagrande, M.; Agostini, F.; Favieri, F.; Forte, G.; Giovannoli, J.; Guarino, A.; Marotta, A.; Doricchi, F.; Martella, D. Age-Related Changes in Hemispherical Specialization for Attentional Networks. Brain Sci. 2021, 11, 1115. [Google Scholar] [CrossRef] [PubMed]
- Federico, F.; Marotta, A.; Orsolini, M. Aging in cognitive control of social processing: Evidence from the attention network test. Aging Neuropsychol. Cogn. 2021, 28, 128–142. [Google Scholar] [CrossRef]
- Forte, G.; Casagrande, M. Effects of Blood Pressure on Cognitive Performance in Aging: A Systematic Review. Brain Sci. 2020, 10, 919. [Google Scholar] [CrossRef]
- Prince, M.; Guerchet, M.; Prina, M. The Epidemiology and Impact of Dementia: Current State and Future Trends. WHO Thematic Briefing; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Kasper, S.; Bancher, C.; Eckert, A.; Förstl, H.; Frölich, L.; Hort, J.; Korczyn, A.D.; Kressig, R.W.; Levin, O.; Palomo, M.S.M. Management of mild cognitive impairment (MCI): The need for national and international guidelines. World J. Biol. Psychiatry 2020, 21, 579–594. [Google Scholar] [CrossRef]
- Andrieu, S.; Guyonnet, S.; Coley, N.; Cantet, C.; Bonnefoy, M.; Bordes, S.; Bories, L.; Cufi, M. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): A randomised, placebo-controlled trial. Lancet Neurol. 2017, 16, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Script | Database | N° |
|---|---|---|
| (“cognitive reserve”) AND (MCI OR “mild cognitive impairment”) AND (elder* OR aged OR old* OR geriatric OR senior OR aging) | PSYCINFO | 174 |
| MEDLINE | 375 | |
| SCOPUS | 5111 | |
| WEB OF SCIENCE | 262 |
| Study | Attrition Bias | Reporting Bias | Sample Bias | Measurement Bias |
|---|---|---|---|---|
| Algarabel et al. [30] | − | − | + | − |
| Andrejeva et al. [31] | − | − | − | − |
| Franzmeier et al. [32] | − | − | − | − |
| Geda et al. [20] | − | − | − | + |
| Kim et al. [26] | − | − | − | − |
| Liu et al. [25] | − | − | − | + |
| Malave [27] | − | − | − | − |
| Soldan et al. [28] | − | − | + | − |
| Solè-Padulles et al. [33] | − | − | + | − |
| Xu et al. [29] | − | − | + | − |
| Authors | Diagnostic Criteria | Global Functioning | Subjective Cognitive Complaints | Cognitive Decline | Objective Cognitive Impairment | Normal Functional Abilities | Absence of Dementia | Normal Mental Status |
|---|---|---|---|---|---|---|---|---|
| Algarabel et al. [30] | Petersen [10] | ✔ | ✔ | ✔ | ✔ | ✔ | ||
| Andrejeva et al. [31] | Winblad et al. [11]; AACD [42] | ✔ | ✔ | ✔ | ✔ | ✔ | ||
| Franzmeier et al. [32] | Petersen, [10] | ✔ | ✔ | ✔ | ✔ | ✔ | ||
| Geda et al. [20] | Mayo Clinic Revised [39] | CDR = 0 or 0.5 | ✔ | ✔ | ✔ | ✔ | ||
| Kim et al. [26] | Petersen et al. [35] | ✔ | ✔ | ✔ | ✔ | |||
| Liu et al. [25] | DSM-IV [38] | ✔ | ✔ | |||||
| Malave [27] | Winblad et al. [11] | ✔ | ✔ | ✔ | ✔ | |||
| Soldan et al. [28] | Albert et al. [40] | CDR = 0.5 | ✔ | ✔ | ✔ | ✔ | ✔ | |
| Solè-Padullès et al. [33] | Petersen et al. [36]; Lopez et al. [37] | ✔ | ✔ | ✔ | ✔ | ✔ | ||
| Xu et al. [29] | NINCDS-ARDA [41] | ✔ | ✔ | ✔ | ✔ |
| Diagnostic Criteria | Authors | |
|---|---|---|
| Albert et al. [40] |
| Soldan et al. [28] |
| Aging-Associated Cognitive Decline (AACD) [42] | Subjective impairment as reported by the patient or a reliable informant and considered a decline in a broad spectrum of cognitive domains. Deficits in relevant cognitive domains were indicated by neuropsychological test performance of at least 1 standard deviation below normal age and educational levels. | Andrejeva et al. [31] |
| Diagnostical and Statical Manual of Mental Disorders IV (DSM-IV) [38] | Cognitive decline
| Liu et al. [25] |
| Lopez et al. [37] |
| Solè-Padullès et al. [33] |
| Mayo Clinic Revised [39] |
| Geda et al. [20] |
| National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association (NINCDS-ARDA) [41] |
| Xu et al. [29] |
| Petersen [10] |
| Algarabel et al. [30]; Franzmeier et al. [32] |
| Petersen et al. [35] |
| Kim et al. [26] |
| Petersen et al. [36] |
| Solè-Padullès et al. [33] |
| Winblad et al. [11] |
| Andrejeva et al. [31]; Malave, [27] |
| Authors | Global Cognitive Functioning | Visuospatial Abilities | Attention | Executive Functions | Language | Memory (Short Term) | Memory (Long Term) |
|---|---|---|---|---|---|---|---|
| Algarabel et al. [30] |
|
|
|
|
| ||
| Andrejeva et al. [31] |
| ||||||
| Franzmeier et al. [32] |
|
| |||||
| Geda et al. [20] |
|
|
|
|
| ||
| Liu et al. [25] |
| ||||||
| Kim et al. [26] |
| ||||||
| Malave [27] |
|
|
|
|
|
| |
| Soldan et al. [28] |
|
|
|
| |||
| Solè-Padullès et al. [33] |
| ||||||
| Xu et al. [29] |
|
| Authors | Experimental Design | Nationality | Groups | N° | Sex (% F) | Age (SD) | Diagnostic Criteria | Cognitive Reserve Assessment | Cognitive Domain | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Algarabel et al. [30] | Cross-Sectional | Spain | MCI HC | 37 39 | 67% 74% | 74.95 69.75 | Petersen [10] | Schooling, Job position, Leisure activities, Vocabulary (WAIS-III) | Global Cognitive Functioning, Visuospatial Abilities, Language, Memory | The MCI group exhibits worse performance in both memory tasks than HC. MCI with high CR exhibit better performance in implicit associative memory tasks than MCI with low CR. |
| Andrejeva et al. [31] | Cross-Sectional | Germany | aMCI aMCI+ HC | 49 222 65 | 40% 51% 61% | 66.57 (8.02) 72.27 (7.90) 69.56 (8.62) | Winblad et al. [11]; Levy [42] | Schooling | Global Cognitive Functioning | aMCI have a higher level of schooling than the aMCI+ group, which correlates with better cognitive functioning. |
| Franzmeier et al. [32] | Cross-Sectional | Germany | aMCI HC | 76 36 | 47% 58% | 71 (7.50) 75 (6.30) | Petersen [10] | Schooling, Verbal IQ (ANART) | Global Cognitive Functioning, Memory | aMCI with high CR have better performance in episodic memory tasks than MCI with low CR. |
| Geda et al. [20] | Cross-Sectional | USA | MCI HC | 197 1124 | 41.1% 49.8% | 83 80 | Mayo Clinic Revised [39] | Cognitive stimulating activities | Global Cognitive Functioning, Visuospatial Abilities, Executive Functions, Language, Memory | Involvement in cognitively stimulating activities is associated with better cognitive functioning and a lower risk of MCI. |
| Liu et al. [25] | Longitudinal | China | MCI HC | 21 18 | 52% 33% | 68.5 64 | DSM-IV [38] | Schooling, Job position | Global Cognitive Functioning | High CR is associated with lower MCI risk and better cognitive functioning. |
| Kim et al. [26] | Longitudinal | South Korea | MCI HC | 22 22 | 77.3% 90% | 74.23 (7.50) 71.45 (3.95) | Petersen et al. [35] | CRIq | Global Cognitive Functioning | MCI and HC differ in the “CRI-leisure time” section correlated with cognitive functioning. |
| Malave [27] | Longitudinal | USA | MCI HC | 1058 1226 | 43.29% 47.39% | 78 77 | Winblad et al. [11] | LAQ, IQ (ANART, RPM) | Global Cognitive Functioning, Visuospatial Abilities, Attention, Executive Functions, Language, Memory | IQ and participation in cognitively stimulating activities (crossword puzzles and newspaper reading) are associated with a lower risk of MCI. |
| Soldan et al. [28] | Longitudinal | USA | MCI HC | 66 237 | 51.5% 62% | 63 (10.8) 55.7 (9.40) | Albert et al. [40] | Schooling, NART, Vocabulary (WAIS-III) | Executive Functions, Language, Memory | High CR is associated with a lower risk of MCI and better cognitive functioning. Among participants who develop MCI, more rapid cognitive decline is observed in those with higher CR. |
| Solé-Padullés et al. [33] | Cross-Sectional | Spain | aMCI HC | 12 16 | 80% 45% | 74.25 (6.18) 73.31 (4.90) | Petersen et al. [36]; Lopez et al. [37] | Schooling, Job position, Leisure activities, IQ | Memory | aMCI have lower CR and worse mnesic performance than HC. |
| Xu et al. [29] | Longitudinal | China | MCI HC | 420 1182 | 72% 77% | 82.2 78.8 | NINCDS-ADRDA [41] | Schooling, Cognitive stimulating activities, Social stimulating activities | Global Cognitive Functioning | High CR is associated with a lower risk of MCI. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corbo, I.; Marselli, G.; Di Ciero, V.; Casagrande, M. The Protective Role of Cognitive Reserve in Mild Cognitive Impairment: A Systematic Review. J. Clin. Med. 2023, 12, 1759. https://doi.org/10.3390/jcm12051759
Corbo I, Marselli G, Di Ciero V, Casagrande M. The Protective Role of Cognitive Reserve in Mild Cognitive Impairment: A Systematic Review. Journal of Clinical Medicine. 2023; 12(5):1759. https://doi.org/10.3390/jcm12051759
Chicago/Turabian StyleCorbo, Ilaria, Giulia Marselli, Valerio Di Ciero, and Maria Casagrande. 2023. "The Protective Role of Cognitive Reserve in Mild Cognitive Impairment: A Systematic Review" Journal of Clinical Medicine 12, no. 5: 1759. https://doi.org/10.3390/jcm12051759