
Dyslipidemia Treatment and Lipid Control in US Adults with Diabetes by Sociodemographic and Cardiovascular Risk Groups in the NIH Precision Medicine Initiative All of Us Research Program

Abstract
:1. Introduction
2. Materials and Methods
2.1. All of Us Research Program
2.2. Study Sample
2.3. Definitions and Measurements
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J. Diabetes 2015, 6, 1246–1258. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Song, Y.; Inzucchi, S.E.; Sperling, L.; Cannon, C.P.; Arnold, S.V.; Kosiborod, M.; Wong, N.D. Composite cardiovascular risk factor target achievement and its predictors in US adults with diabetes: The Diabetes Collaborative Registry. Diabetes Obes. Metab. 2019, 21, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Philip, S.; Granowitz, C.; Toth, P.P.; Wong, N.D. Residual Hypertriglyceridemia and Estimated Atherosclerotic Cardiovascular Disease Risk by Statin Use in U.S. Adults With Diabetes: National Health and Nutrition Examination Survey 2007-2014. Diabetes Care 2019, 42, 2307–2314. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Kearney, P.M.; Blackwell, L.; Collins, R.; Keech, A.; Simes, J.; Peto, R.; Armitage, J.; Baigent, C. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: A meta-analysis. Lancet 2008, 371, 117–125. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Leiter, L.A.; Wiviott, S.D.; Giugliano, R.P.; Deedwania, P.; De Ferrari, G.M.; Murphy, S.A.; Kuder, J.F.; Gouni-Berthold, I.; Lewis, B.S.; et al. Cardiovascular safety and efficacy of the PCSK9 inhibitor evolocumab in patients with and without diabetes and the effect of evolocumab on glycaemia and risk of new-onset diabetes: A prespecified analysis of the FOURIER randomised controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Ganda, O.P.; Bhatt, D.L.; Mason, R.P.; Miller, M.; Boden, W.E. Unmet Need for Adjunctive Dyslipidemia Therapy in Hypertriglyceridemia Management. J. Am. Coll. Cardiol. 2018, 72, 330–343. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, S.; Har-rington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef]
- Gallego-Colon, E.; Daum, A.; Yosefy, C. Statins and PCSK9 inhibitors: A new lipid-lowering therapy. Eur. J. Pharmacol. 2020, 878, 173114. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- The All of Us Research Program. 2021. Available online: https://allofus.nih.gov/ (accessed on 9 October 2021).
- Force, U.P.S.T.; Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Jaén, C.R.; et al. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2022, 328, 746–753. [Google Scholar] [CrossRef]
- Frank, A.T.; Zhao, B.; Jose, P.O.; Azar, K.M.; Fortmann, S.P.; Palaniappan, L.P. Racial/ethnic differences in dyslipidemia patterns. Circulation 2014, 129, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, M.P.; Lester, C.A.; Ding, Y.; Joseph, M.; Brook, R.D. Effects of Race on Statin Prescribing for Primary Prevention With High Atherosclerotic Cardiovascular Disease Risk in a Large Healthcare System. J. Am. Heart Assoc. 2019, 8, e014709. [Google Scholar] [CrossRef]
- Schroff, P.; Gamboa, C.M.; Durant, R.W.; Oikeh, A.; Richman, J.S.; Safford, M.M. Vulnerabilities to Health Disparities and Statin Use in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) Study. J. Am. Heart Assoc. 2017, 6, e005449. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P.; Cannon, C.P.; Blazing, M.A.; Nicolau, J.C.; Corbalán, R.; Špinar, J.; Park, J.G.; White, J.A.; Bohula, E.A.; Braunwald, E.; et al. Benefit of Adding Ezetimibe to Statin Therapy on Cardiovascular Outcomes and Safety in Patients With Versus Without Diabetes Mellitus: Results From IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). Circulation 2018, 137, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Karagiannis, A.; Athyros, V.G. Rosuvastatin and ezetimibe for the treatment of dyslipidemia and hypercholesterolemia. Expert Rev. Cardiovasc. Ther. 2021, 19, 575–580. [Google Scholar] [CrossRef]
- Lazarte, J.; Hegele, R.A. Dyslipidemia Management in Adults With Diabetes. Can. J. Diabetes 2020, 44, 53–60. [Google Scholar] [CrossRef]
- Available online: https://www.acc.org/Latest-in-Cardiology/Articles/2022/11/01/22/00/sun-7pm-respect-epa-aha-2022 (accessed on 1 February 2023).
- Das Pradhan, A.; Glynn, R.J.; Fruchart, J.C.; MacFadyen, J.G.; Zaharris, E.S.; Everett, B.M.; Campbell, S.E.; Oshima, R.; Amarenco, P.; Blom, D.J.; et al. Triglyceride Lowering with Pemafibrate to Reduce Cardiovascular Risk. N. Engl. J. Med. 2022, 387, 1923–1934. [Google Scholar] [CrossRef] [PubMed]
- Andary, R.; Fan, W.; Wong, N.D. Control of Cardiovascular Risk Factors Among US Adults With Type 2 Diabetes With and Without Cardiovascular Disease. Am. J. Cardiol. 2019, 124, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Derington, C.G.; Bress, A.P.; Herrick, J.S.; Fan, W.; Wong, N.D.; Andrade, K.E.; Johnson, J.; Philip, S.; Abrahamson, D.; Jiao, L.; et al. The potential population health impact of treating REDUCE-IT eligible US adults with Icosapent Ethyl. Am J Prev Cardiol. 2022, 10, 100345. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Blumenthal, R.S.; Braun, L.T.; Heidenreich, P.A.; Lloyd-Jones, D.; Orringer, C.E.; Saseen, J.J.; Smith, S.C.; Sperling, L.S.; et al. High-Intensity Statins Benefit High-Risk Patients: Why and How to Do Better. Mayo Clin. Proc. 2021, 96, 2660–2670. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S125–S143. [Google Scholar] [CrossRef]
- Gianfrancesco, M.A.; Goldstein, N.D. A narrative review on the validity of electronic health record-based research in epidemiology. BMC Med. Res. Methodol. 2021, 21, 234. [Google Scholar] [CrossRef] [PubMed]
- Pareek, M.; Mason, R.P.; Bhatt, D.L. Icosapent ethyl: Safely reducing cardiovascular risk in adults with elevated triglycerides. Expert Opin. Drug Saf. 2022, 21, 31–42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (n = 81,332) |
|---|---|
| Age (years) | 62.0 (±14.1) |
| Male | 31,887 (40.6%) |
| Female | 46,661 (59.4%) |
| Non-Hispanic White | 42,532 (52.3%) |
| Non-Hispanic Black | 18,100 (22.3%) |
| Hispanic or Latino | 13,986 (17.2%) |
| Asian | 1445 (1.8%) |
| Other Race/Ethnicity | 5269 (6.5%) |
| Health Insurance | 74,838 (95.6%) |
| Income | |
| Less than 10 k | 11,678 (19.6%) |
| 10–25 k | 11,793 (19.8%) |
| 25–35 k | 5994 (10.1%) |
| 35–50 k | 6262 (10.5%) |
| 50–75 k | 7990 (13.4%) |
| 75–100 k | 5673 (9.5%) |
| More than 100 k | 10,046 (16.9%) |
| Education | |
| Less than a high school degree or equivalent | 9527 (12.2%) |
| Twelve or GED | 17,147 (21.9%) |
| Some College | 22,394 (28.6%) |
| College Graduate/Advanced Degree | 29,104 (37.2%) |
| BMI (kg/m2) | 32.5 (±12.2) |
| Smoking Status | |
| Non-Smoker | 43,071 (54.7%) |
| Former Smoker | 23,383 (29.7%) |
| Current Smoker | 12,229 (15.5%) |
| Systolic Blood Pressure (mm Hg) | 129.5 (±14.2) |
| Diastolic Blood Pressure (mm Hg) | 76.9 (±9.1) |
| Triglycerides (mg/dL) | 145.7 (±85.1) |
| LDL-C (mg/dL) | 100.9 (±31.3) |
| HDL-C (mg/dL) | 50.1 (±15.2) |
| Diabetes Risk and ASCVD Status | |
| ≤1 Diabetes Risk Factors without ASCVD | 24,787 (31.1%) |
| ≥2 Diabetes Risk Factors without ASCVD | 24,112 (30.3%) |
| Diabetes with ASCVD | 30,682 (38.6%) |
| Diabetes Risk Factors | |
| Age ≥60 years | 50,768 (62.4%) |
| Hypertension | 42,315 (54.9%) |
| LDL-C ≥160 mg/dL | 1835 (3.4%) |
| Smoking History | 12,229 (15.5%) |
| HDL-C < 50 mg/dL in females | 14,861 (18.3%) |
| HDL-C < 40 mg/dL in males | 8641 (10.6%) |
| Proportion (%) | Total (n = 81,332) | ≤1 DM Risk Factors w/o ASCVD (n = 24,780) | ≥2 DM Risk Factors w/o ASCVD (n = 24,119) | DM with ASCVD (n = 30,682) | Female (n = 46,661) | Male (n = 31,887) | Non-Hispanic White (n = 42,532) | Non-Hispanic Black (n = 18,100) | Hispanic or Latino (n = 13,986) | Asian (n = 1445) | Other Race/ Ethnicity (n = 5269) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Statin Category | |||||||||||
| No statin use | 49.8% | 68.5% | 50.5% | 33.5% * | 54.2% | 43.2% * | 46.2% | 53.9% | 54.5% | 51.8% | 51.9% |
| Low intensity | 6.6% | 4.7% | 6.9% | 7.9% * | 6.6% | 6.5% * | 7.6% | 4.8% | 6.0% | 5.3% | 6.1% * |
| Moderate intensity | 31.8% | 20.9% | 32.7% | 40.4% * | 29.4% | 35.7% * | 35.1% | 28.5% | 26.8% | 32.8% | 30.8% * |
| High intensity | 11.8% | 5.9% | 9.9% | 18.2% * | 9.8% | 14.6% * | 11.2% | 12.8% | 12.6% | 10.2% | 11.2% * |
| Ezetimibe Use | 5.1% | 2.1% | 3.2% | 9.1% * | 4.7% | 5.6% * | 6.6% | 3.0% | 2.8% | 5.4% | 5.8% * |
| PCSK9 Inhibitor | 0.6% | 0.1% | 0.2% | 1.3% * | 0.6% | 0.7% | 0.8% | 0.2% | 0.3% | --- | 1.1% * |
| Icosapent Ethyl Use | 1.0% | 0.5% | 0.8% | 1.7% * | 0.5% | 1.8% * | 1.3% | 0.3% | 0.9% | 2.1% | 1.4% * |
| Among those with TG ≥ 150 mg/dL | 1.9% | 0.1% † | 0.5% † | 1.1% † | 0.9% | 2.3% | 2.5% | 0.3% | 0.5% | 2.1% | 1.1% |
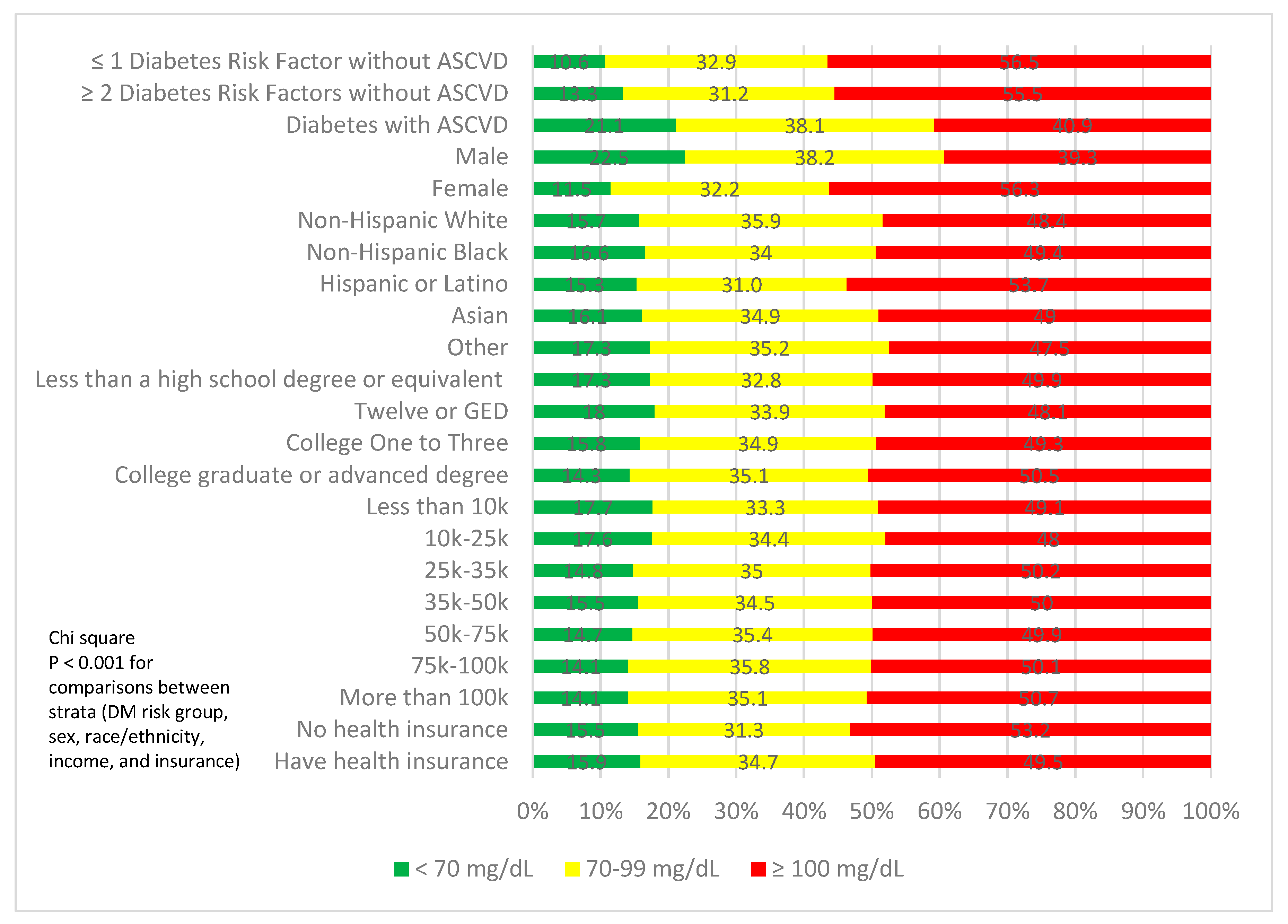
| LDL-C Category | |||||||||||
| <70 mg/dL | 16.0% | 10.6% | 13.3% | 21.1% * | 11.5% | 22.5% * | 15.7% | 16.6% | 15.3% | 16.1% | 17.3% * |
| 70–99 mg/dL | 34.6% | 32.9% | 31.2% | 38.1% * | 32.2% | 38.2% * | 35.9% | 34.0% | 31.0% | 34.9% | 35.2% * |
| ≥100 mg/dL | 49.5% | 56.5% | 55.5% | 40.9% * | 56.3% | 39.3% * | 48.4% | 49.4% | 53.7% | 49.0% | 47.5% * |
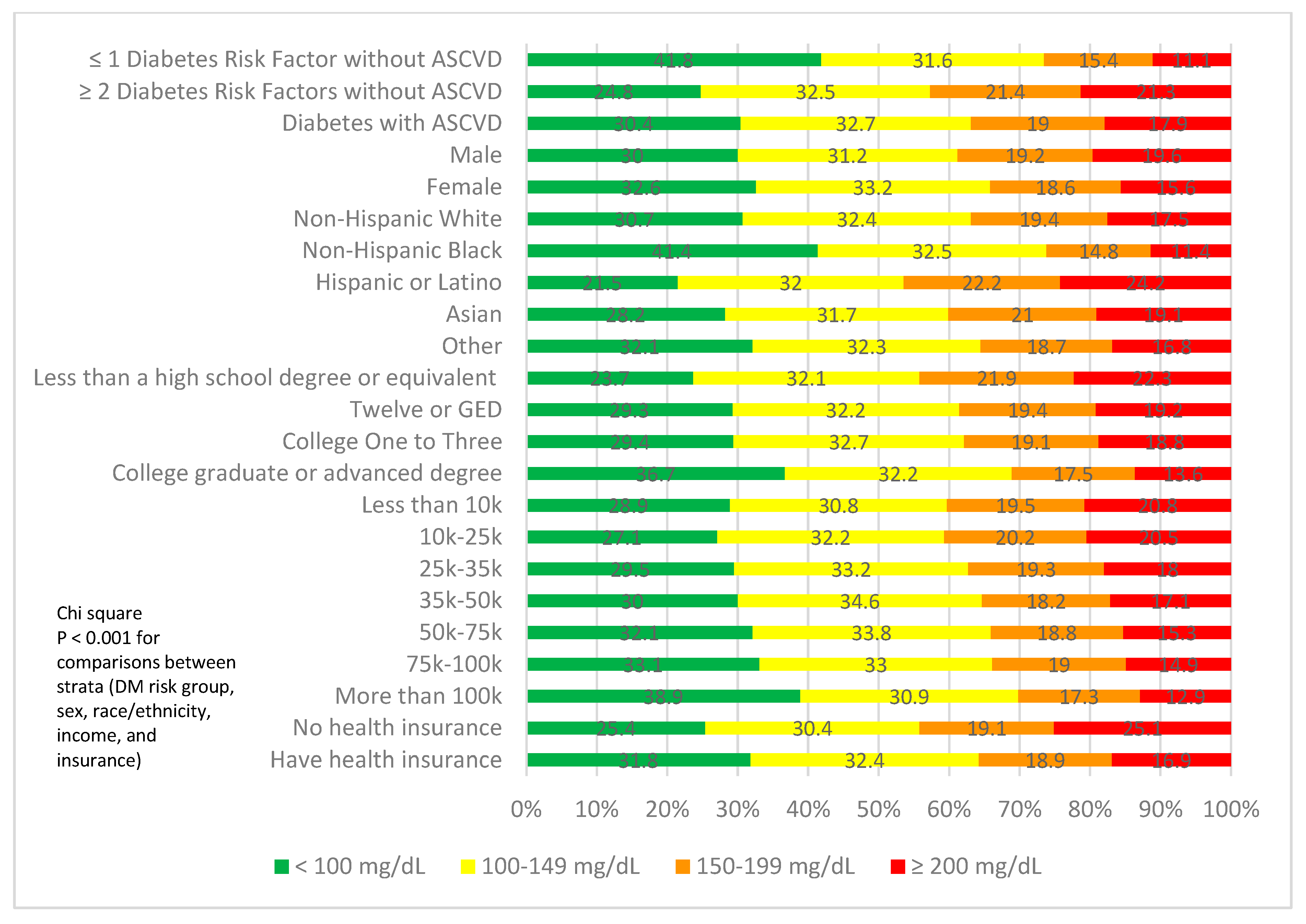
| Triglyceride Category | |||||||||||
| <100 mg/dL | 31.6% | 41.8% | 24.8% | 30.4% * | 32.6% | 30.0% * | 30.7% | 41.4% | 21.5% | 28.2% | 32.1% * |
| 100–149 mg/dL | 32.8% | 32.1% | 33.0% | 33.1% * | 33.6% | 31.7% * | 32.9% | 32.9% | 32.5% | 32.0% | 32.7% * |
| ≥150 mg/dL | 35.6% | 26.1% | 42.2% | 36.5% * | 33.7% | 38.3% * | 36.4% | 25.7% | 46.0% | 39.7% | 35.1% * |
| Proportion (%) | High-Intensity Statin Use | Ezetimibe Use | PCSK9 Inhibitor Use | Icosapent Ethyl Use |
|---|---|---|---|---|
| Health Insurance (n = 74,838) | 27.5% * | 5.3% * | 0.6% * | 1.0% |
| No Health Insurance (n = 3469) | 23.7% * | 1.4% | --- | 1.1% |
| Less than a high school degree (n = 9527) | 31.1% * | 3.1% * | --- | 0.5% * |
| Twelfth Grade or GED (n = 17,147) | 28.1% * | 4.2% * | 0.5% * | 0.9% * |
| College (n = 22,394) | 26.6% * | 4.9% * | 0.6%* | 1.1% * |
| College Graduate or Advanced degree (n = 29,104) | 25.8% * | 6.4% * | 0.8% * | 1.0% * |
| Income Less than 10 k (n = 11,678) | 26.9% * | 2.8% * | 3.0% | 0.5% * |
| 10–25 k (n = 11,793) | 30.8% * | 4.5% * | 0.2% * | 1.0% * |
| 25–35 k (n = 5994) | 26.8% * | 5.2% * | 0.7% * | 1.1% * |
| 35–50 k (n = 6262) | 26.7% * | 5.7% * | 0.5% * | 1.6% * |
| 50–75 k (n = 7990) | 25.6% * | 5.8% * | 0.7% * | 1.3% * |
| 75–100 k (n = 5673) | 25.0% * | 6.8% * | 0.8% * | 1.4% * |
| More than 100 k (n = 10,046) | 24.9% * | 7.2% * | 0.9% * | 1.1% * |
| Variable | High-Intensity Statin Use Odds Ratio [95% CI] | Ezetimibe Use Odds Ratio [95% CI] | PCSK9 Inhibitor Use Odds Ratio [95% CI] | Icosapent Ethyl Use Odds Ratio [95% CI] |
|---|---|---|---|---|
| Age (Per Year) | 1.02 [1.016, 1.023] | 1.02 [1.017, 1.03] | 1.02 [0.99, 1.04] | 1.00 [0.99, 1.03] |
| Gender: Male | 1.73 [1.62, 1.85] | 0.98 [0.87, 1.099] | 1.17 [0.84, 1.63] | 2.98 [2.03, 4.48] |
| BMI (Per kg/m2) | 1.00 [0.999, 1.003] | 1.00 [0.998, 1.004] | 0.995 [0.992, 1.00] | 1.006 [1.003, 1.009] |
| Age ≥60 years | 1.09 [0.99, 1.20] | 1.27 [1.05, 1.54] | 0.47 [0.27, 0.79] | 1.38 [0.85, 2.28] |
| HTN | 1.13 [1.07, 1.19] | 0.91 [0.82, 1.00] | 1.13 [0.86, 1.47] | 0.92 [0.71, 1.18] |
| LDL-C ≥ 160 mg/dL | 1.63 [1.43, 1.86] | 3.02 [2.48, 3.66] | 0.15 [0.10, 0.23] | 0.63 [0.19, 1.50] |
| Smoking History | 1.11 [1.03, 1.19] | 0.87 [0.74, 1.02] | 1.07 [0.71, 1.69] | 0.61 [0.37, 0.96] |
| HDL-C < 50 mg/dL in females | 1.47 [1.37, 1.58] | 1.16 [1.02, 1.32] | 1.34 [0.93, 1.96] | 2.19 [1.41, 3.45] |
| HDL-C < 40 mg/dL in males | 1.27 [1.17, 1.37] | 1.05 [0.91, 1.21] | 0.99 [0.67, 1.49] | 1.92 [1.43, 2.58] |
| Ethnicity: Non-Hispanic Black | 1.30 [1.21, 1.39] | 0.62 [0.54, 0.72] | 2.49 [1.60, 4.04] | 0.22 [0.12, 0.38] |
| Hispanic or Latino | 1.34 [1.24, 1.45] | 0.70 [0.59, 0.84] | 1.57 [0.98, 2.64] | 0.97 [0.64, 1.43] |
| Asian | 0.96 [0.78, 1.17] | 0.88 [0.61, 1.24] | 4.87 [1.08, 8.59] | 2.30 [1.20, 4.01] |
| Other | 1.05 [0.93, 1.19] | 1.05 [0.85, 1.28] | 0.65 [0.41, 1.07] | 1.17 [0.69, 1.88] |
| Have health insurance | 0.79 [0.69, 0.90] | 1.52 [1.03, 2.35] | 0.22 [0.01, 0.99] | 0.60 [0.32, 1.29] |
| Income: 10–25 k | 0.97 [0.89, 1.05] | 1.13 [0.94, 1.35] | 0.58 [0.33, 0.98] | 0.89 [0.54, 1.48] |
| 25–35 k | 0.76 [0.69, 0.84] | 1.17 [0.95, 1.45] | 0.61 [0.32, 1.14] | 1.16 [0.66, 2.03] |
| 35–50 k | 0.76 [0.69, 0.84] | 1.17 [0.95, 1.44] | 0.75 [0.39, 1.42] | 1.41 [0.84, 2.39] |
| 50–75 k | 0.70 [0.64, 0.77] | 1.18 [0.97, 1.44] | 0.68 [0.37, 1.22] | 1.22 [0.74, 2.05] |
| 75–100 k | 0.69 [0.62, 0.77] | 1.46 [1.19, 1.80] | 0.55 [0.29, 1.02] | 1.04 [0.60, 1.83] |
| >100 k | 0.71 [0.65, 0.78] | 1.53 [1.27, 1.85] | 0.53 [0.29, 0.92] | 1.15 [0.71, 1.92] |
| Diabetes Risk Group | ||||
| Diabetes with ≥2 Risk Factors | 1.18 [1.08, 1.30] | 1.11 [0.92, 1.34] | 0.80 [0.41, 1.51] | 1.18 [0.73, 1.96] |
| Diabetes with ASCVD | 3.66 [3.37, 3.97] | 3.12 [2.66, 3.67] | 0.14 [0.08, 0.24] | 2.21 [1.44, 3.47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbarpour, M.; Devineni, D.; Gong, Y.; Wong, N.D. Dyslipidemia Treatment and Lipid Control in US Adults with Diabetes by Sociodemographic and Cardiovascular Risk Groups in the NIH Precision Medicine Initiative All of Us Research Program. J. Clin. Med. 2023, 12, 1668. https://doi.org/10.3390/jcm12041668
Akbarpour M, Devineni D, Gong Y, Wong ND. Dyslipidemia Treatment and Lipid Control in US Adults with Diabetes by Sociodemographic and Cardiovascular Risk Groups in the NIH Precision Medicine Initiative All of Us Research Program. Journal of Clinical Medicine. 2023; 12(4):1668. https://doi.org/10.3390/jcm12041668
Chicago/Turabian StyleAkbarpour, Meleeka, Divya Devineni, Yufan Gong, and Nathan D. Wong. 2023. "Dyslipidemia Treatment and Lipid Control in US Adults with Diabetes by Sociodemographic and Cardiovascular Risk Groups in the NIH Precision Medicine Initiative All of Us Research Program" Journal of Clinical Medicine 12, no. 4: 1668. https://doi.org/10.3390/jcm12041668