
Biliary Atresia in Adolescence and Adult Life: Medical, Surgical and Psychological Aspects

Abstract
:1. Introduction
2. Overall Survival Data up to 30 Years
3. Health Status of Survivors
3.1. Chronic Liver Disease
3.2. Health Related Quality of Life (HRQOL)
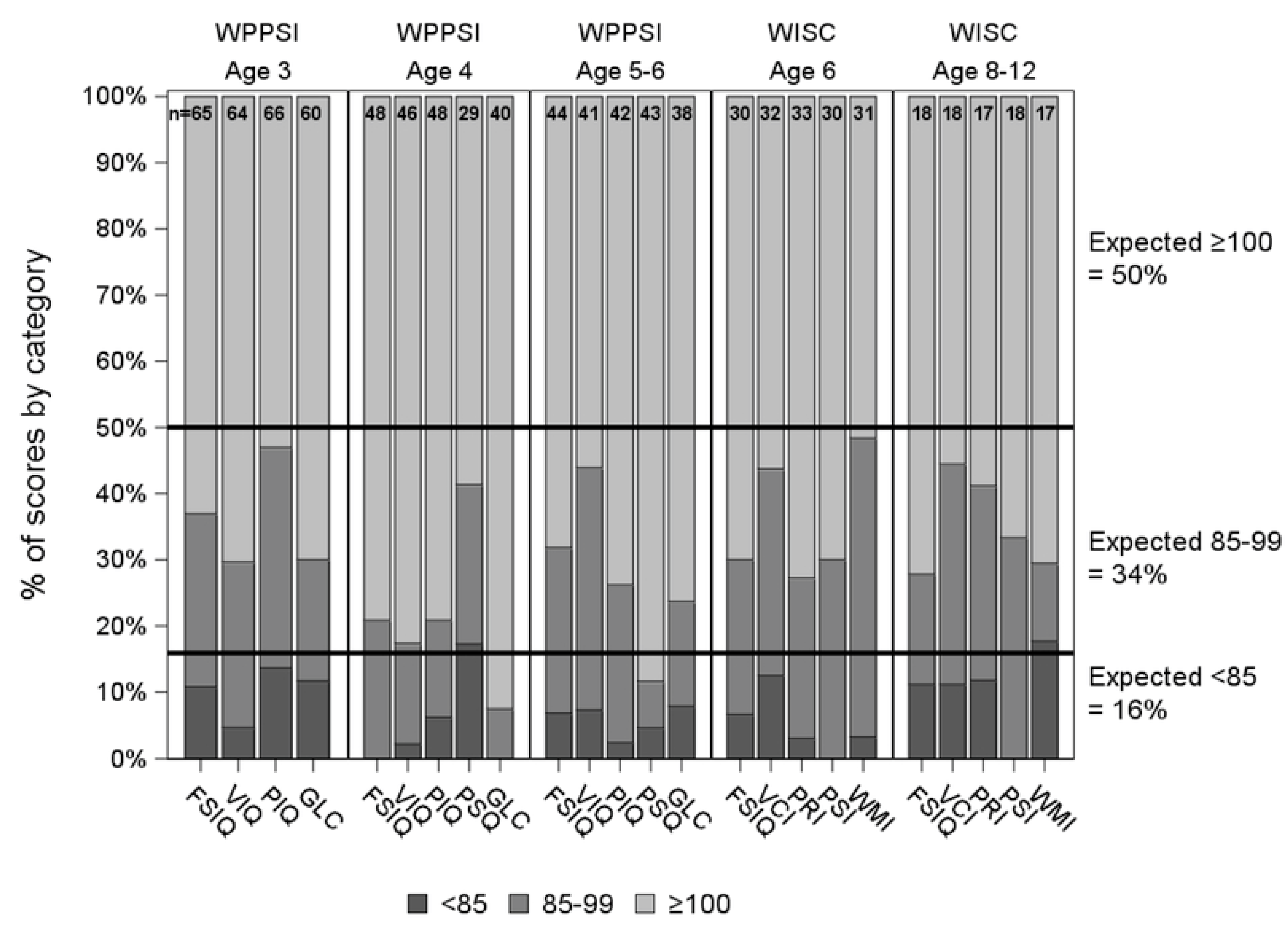
3.3. Neurodevelopmental Outcome
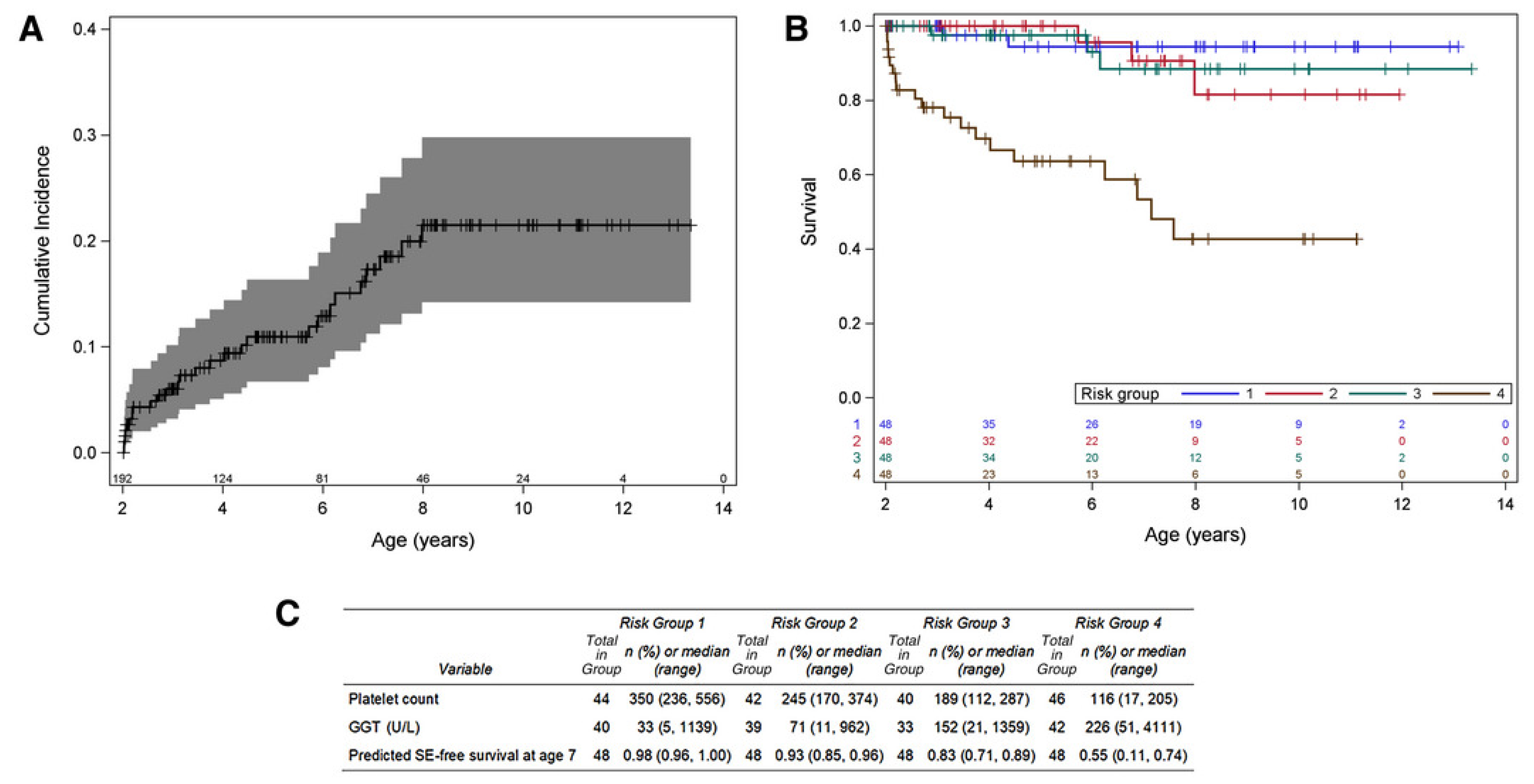
3.4. Predictors of Outcome
4. Adolescence and Transition
4.1. Adolescence
4.2. Transition
4.3. The Transitional Care Programme
4.4. Key Transitional Care Issues
4.4.1. Disease Education
4.4.2. Generic Health Education and Sexual Health
4.4.3. Substance Misuse
4.4.4. Self-Advocacy and Psychosocial Issues
4.4.5. Non-Adherence
5. Medical and Surgical Management in Adolescence and Adult Life
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Kasai, M.; Suzuki, M. A new operation for non-correctable biliary atresia: Hepatic portoenterostomy. Shujutsu 1959, 13, 733–739. [Google Scholar]
- Fanna, M.M.G.; Capito, C.; Girard, M.; Guerin, F.; Hermeziu, B.; Lachaux, A.; Roquelaure, B.; Gottrand, F.; Broue, P.; Dabadie, A.; et al. Management of Biliary Atresia in France 1986 to 2015: Long-Term Results. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 416–424. [Google Scholar] [CrossRef]
- Kelay, A.; Davenport, M. Long-term outlook in biliary atresia. Semin. Pediatr. Surg. 2017, 26, 295–300. [Google Scholar] [CrossRef]
- Rodijk, L.H.; Schins, E.M.W.; Witvliet, M.J.; Verkade, H.J.; de Kleine, R.H.; Hulscher, J.B.F.; Bruggink, J.L.M. Health-Related Quality of Life in Biliary Atresia Patients with Native Liver or Transplantation. Eur. J. Pediatr. Surg. 2020, 30, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Yu, H.; Shu, F.; Huang, W.; Jiang, X.; Xu, Z.; Zhang, T.; Xiang, B.; Jin, S. Factors influencing the quality of life in children after biliary atresia treatment. Transl. Pediatr. 2021, 10, 2496–2505. [Google Scholar] [CrossRef] [PubMed]
- Rodijk, L.H.; Schins, E.M.; Witvliet, M.J.; Alizadeh, B.Z.; Verkade, H.J.; de Kleine, R.H.; Hulscher, J.B.; Bruggink, J.L. Quality of Life in Parents of Children with Biliary Atresia. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 641–646. [Google Scholar] [CrossRef]
- Wong, C.W.Y.; Chung, P.H.Y.; Tam, P.K.H.; Wong, K.K.Y. Long-Term Results and Quality of Life Assessment in Biliary Atresia Patients: A 35-Year Experience in a Tertiary Hospital. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 570–574. [Google Scholar] [CrossRef]
- Squires, J.E.; Ng, V.L.; Hawthorne, K.; Henn, L.L.; Sorensen, L.G.; Fredericks, E.M.; Alonso, E.M.; Murray, K.F.; Loomes, K.M.; Karpen, S.J.; et al. Neurodevelopmental Outcomes in Preschool and School Aged Children With Biliary Atresia and Their Native Liver. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 79–86. [Google Scholar] [CrossRef]
- Ruuska, S.; Lähteenmäki, M.; Häyrinen, T.; Kanerva, K.; Jahnukainen, T.; Haataja, L.; Kolho, K.-L.; Pakarinen, M.P. Neurocognitive and Motor Functions in Biliary Atresia Patients: A Cross-Sectional, Prospective National Cohort Study. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 491–498. [Google Scholar] [CrossRef]
- Rodijk, L.H.; Heijer, A.E.D.; Hulscher, J.B.; Alizadeh, B.Z.; de Kleine, R.H.; Verkade, H.J.; Bruggink, J.L. Long-Term Neurodevelopmental Outcomes in Children with Biliary Atresia. J. Pediatr. 2020, 217, 118–124.e3. [Google Scholar] [CrossRef]
- Van Wessel, D.; Nomden, M.; Bruggink, J.; de Kleine, R.; Kurilshikov, A.; Verkade, H.; Harmsen, H.; Hulscher, J. Gut Microbiota Composition of Biliary Atresia Patients Before Kasai Portoenterostomy Associates with Long-term Outcome. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Madadi-Sanjani, O.; Kuebler, J.F.; Dippel, S.; Gigina, A.; Falk, C.S.; Vieten, G.; Petersen, C.; Klemann, C. Long-term outcome and necessity of liver transplantation in infants with biliary atresia are independent of cytokine milieu in native liver and serum. Cytokine 2018, 111, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Harumatsu, T.; Muraji, T.; Masuya, R.; Ohtani, H.; Nagai, T.; Yano, K.; Onishi, S.; Yamada, K.; Yamada, W.; Matsukubo, M.; et al. Microvascular proliferation of the portal vein branches in the liver of biliary atresia patients at Kasai operation is associated with a better long-term clinical outcome. Pediatr. Surg. Int. 2019, 35, 1437–1441. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Nio, M.; Ando, H.; Kitagawa, H.; Kubota, M.; Suzuki, T.; Taguchi, T.; Hashimoto, T.; Society, T.J.B.A. Anatomical patterns of biliary atresia including hepatic radicles at the porta hepatis influence short- and long-term prognoses. J. Hepato-Biliary-Pancreat. Sci. 2021, 28, 931–941. [Google Scholar] [CrossRef]
- Johansson, H.; Svensson, J.F.; Almström, M.; Van Hul, N.; Rudling, M.; Angelin, B.; Nowak, G.; Fischler, B.; Ellis, E. Regulation of bile acid metabolism in biliary atresia: Reduction of FGF19 by Kasai portoenterostomy and possible relation to early outcome. J. Intern. Med. 2020, 287, 534–545. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, Y.; Peng, C.; Pang, W.; Zhang, T.; Wu, D.; Shen, Q.; Li, M. Five-year native liver survival analysis in biliary atresia from a single large Chinese center: The death/liver transplantation hazard change and the importance of rapid early clearance of jaundice. J. Pediatr. Surg. 2019, 54, 1680–1685. [Google Scholar] [CrossRef]
- Shneider, B.L.; Magee, J.C.; Karpen, S.J.; Rand, E.B.; Narkewicz, M.R.; Bass, L.M.; Schwarz, K.; Whitington, P.F.; Bezerra, J.A.; Kerkar, N.; et al. Total Serum Bilirubin within 3 Months of Hepatoportoenterostomy Predicts Short-Term Outcomes in Biliary Atresia. J. Pediatr. 2016, 170, 211–217.e2. [Google Scholar] [CrossRef] [Green Version]
- Venkat, V.; Ng, V.L.; Magee, J.C.; Ye, W.; Hawthorne, K.; Harpavat, S.; Molleston, J.P.; Murray, K.F.; Wang, K.S.; Soufi, N.; et al. Modeling Outcomes in Children With Biliary Atresia With Native Liver After 2 Years of Age. Hepatol Commun. 2020, 4, 1824–1834. [Google Scholar] [CrossRef]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef]
- Blum, R.W.; Garell, D.; Hodgman, C.H.; Jorissen, T.W.; Okinow, N.A.; Orr, D.P.; Slap, G.B. Transition from child-centered to adult health-care systems for adolescents with chronic conditions: A position paper of the Society for Adolescent Medicine. J. Adolesc. Health 1993, 14, 570–576. [Google Scholar] [CrossRef]
- Radzik, M.S.S.; Neinstein, L. Psychosocial development in normal adolescents. In Adolescent Health Care: A Practical Guide; Neinstein, L.G.C., Katzman, D., Rosen, D., Woods, E., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- WHO. Maternal, Newborn, Child and Adolescent Health; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Ruth, N.; Sharif, K.; Legarda, M.; Smith, M.; Lewis, P.; Lloyd, C.; Mirza, D.; Kelly, D. What is the long-term outlook for young people following liver transplant? A single-centre retrospective analysis of physical and psychosocial outcomes. Pediatr. Transplant. 2020, 24, e13782. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics 2002, 110 Pt 2, 1304–1306. [Google Scholar] [CrossRef]
- Kennedy, A.; Sawyer, S. Transition from pediatric to adult services: Are we getting it right? Curr. Opin. Pediatr. 2008, 20, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Crowley, R.; Wolfe, I.; Lock, K.; McKee, M. Improving the transition between paediatric and adult healthcare: A systematic review. Arch. Dis. Child. 2011, 96, 548–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- While, A.; Forbes, A.; Ullman, R.; Lewis, S.; Mathes, L.; Griffiths, P. Good practices that address continuity during transition from child to adult care: Synthesis of the evidence. Child Care Health Dev. 2004, 30, 439–452. [Google Scholar] [CrossRef]
- Mayer, K.; Junge, N.; Goldschmidt, I.; Leiskau, C.; Becker, T.; Lehner, F.; Richter, N.; van Dick, R.; Baumann, U.; Pfister, E.-D. Psychosocial outcome and resilience after paediatric liver transplantation in young adults. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Fredericks, E.M.; Dore-Stites, D.; Well, A.; Magee, J.C.; Freed, G.L.; Shieck, V.; Lopez, M.J. Assessment of transition readiness skills and adherence in pediatric liver transplant recipients. Pediatr. Transplant. 2010, 14, 944–953. [Google Scholar] [CrossRef] [Green Version]
- Fredericks, E.M.; Dore-Stites, D.; Lopez, M.J.; Well, A.; Shieck, V.; Freed, G.L.; Eder, S.J.; Magee, J.C. Transition of pediatric liver transplant recipients to adult care: Patient and parent perspectives. Pediatr. Transplant. 2011, 15, 414–424. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.; Elwell, L.; McDonagh, J.E.; Kelly, D.A.; Wray, J. Parents in transition: Experiences of parents of young people with a liver transplant transferring to adult services. Pediatr. Transplant. 2017, 21, e12760. [Google Scholar] [CrossRef] [Green Version]
- Junge, N.; Migal, K.; Goldschmidt, I.; Baumann, U. Transition after pediatric liver transplantation—Perceptions of adults, adolescents and parents. World J. Gastroenterol. 2017, 23, 2365–2375. [Google Scholar] [CrossRef]
- Wright, J.; Elwell, L.; McDonagh, J.; Kelly, D.; McClean, P.; Ferguson, J.; Wray, J. Healthcare transition in pediatric liver transplantation: The perspectives of pediatric and adult healthcare professionals. Pediatr. Transplant. 2019, 23, e13530. [Google Scholar] [CrossRef] [PubMed]
- Toft, A.; Taylor, R.; Claridge, L.; Clowes, C.; Ferguson, J.; Hind, J.; Jones, R.; McClean, P.; McKiernan, P.; Samyn, M.; et al. The Experiences of Young Liver Patients Transferring from Children’s to Adult Services and Their Support Needs for a Successful Transition. Prog. Transplant. 2018, 28, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.A.; Bucuvalas, J.C.; Alonso, E.M.; Karpen, S.J.; Allen, U.; Green, M.; Farmer, D.; Shemesh, E.; McDonald, R.A. Long-term medical management of the pediatric patient after liver transplantation: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transplant. 2013, 19, 798–825. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.L.; Hays, R.D.; Wells, K.B.; Rogers, W.H.; Spritzer, K.L.; Greenfield, S. Long-term functioning and well-being outcomes associated with physical activity and exercise in patients with chronic conditions in the medical outcomes study. J. Clin. Epidemiol. 1994, 47, 719–730. [Google Scholar] [CrossRef]
- Choudhary, N.S.; Saigal, S. Preventive Strategies for Nonalcoholic Fatty Liver Disease After Liver Transplantation. J. Clin. Exp. Hepatol. 2019, 9, 619–624. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.E.; Hillman, C.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Med. Sci. Sports Exerc. 2016, 48, 1223–1224. [Google Scholar] [CrossRef]
- Naya, I.; Sanada, Y.; Katano, T.; Miyahara, G.; Hirata, Y.; Yamada, N.; Okada, N.; Onishi, Y.; Sakuma, Y.; Sata, N. Pregnancy Outcomes Following Pediatric Liver Transplantation: A Single-Center Experience in Japan. Ann. Transplant. 2020, 25, e921193. [Google Scholar] [CrossRef]
- Le, H.L.; Francke, M.I.; Andrews, L.M.; de Winter, B.C.M.; van Gelder, T.; Hesselink, D.A. Usage of Tacrolimus and Mycophenolic Acid During Conception, Pregnancy, and Lactation, and Its Implications for Therapeutic Drug Monitoring: A Systematic Critical Review. Ther. Drug Monit. 2020, 42, 518–531. [Google Scholar] [CrossRef]
- Lurie, S.; Shemesh, E.; Sheiner, P.A.; Emre, S.; Tindle, H.L.; Melchionna, L.; Shneider, B.L. Non-adherence in pediatric liver transplant recipients—An assessment of risk factors and natural history. Pediatr. Transplant. 2000, 4, 200–206. [Google Scholar] [CrossRef]
- Croft, C.A.; Asmussen, L. A developmental approach to sexuality education: Implications for medical practice. J. Adolesc. Health 1993, 14, 109–114. [Google Scholar] [CrossRef]
- Mellanby, A.R.; Phelps, F.A.; Crichton, N.J.; Tripp, J.H. School sex education: An experimental programme with educational and medical benefit. BMJ 1995, 311, 414–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagar, N.; Leithead, J.A.; Lloyd, C.; Smith, M.; Gunson, B.K.; Adams, D.H.; Kelly, D.; Ferguson, J.W. Pediatric Liver Transplant Recipients Who Undergo Transfer to the Adult Healthcare Service Have Good Long-Term Outcomes. Am. J. Transplant. 2015, 15, 1864–1873. [Google Scholar] [CrossRef] [PubMed]
- Hoegy, D.; Bleyzac, N.; Robinson, P.; Bertrand, Y.; Dussart, C.; Janoly-Dumenil, A. Medication adherence in pediatric transplantation and assessment methods: A systematic review. Patient Prefer. Adherence 2019, 13, 705–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.; Gao, W.; Wang, K.; Han, C.; Zhang, W.; Sun, C. Adherence to medical regimen after paediatric liver transplantation: A systematic review and meta-analysis. Patient Prefer. Adherence 2018, 13, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annunziato, R.A.; Bucuvalas, J.C.; Yin, W.; Arnand, R.; Alonso, E.M.; Mazariegos, G.V.; Venick, R.S.; Stuber, M.L.; Shneider, B.L.; Shemesh, E. Self-Management Measurement and Prediction of Clinical Outcomes in Pediatric Transplant. J. Pediatr. 2018, 193, 128–133.e2. [Google Scholar] [CrossRef]
- Chung, P.H.Y.; Chan, E.K.W.; Yeung, F.; Chan, A.C.Y.; Mou, J.W.C.; Lee, K.H.; Hung, J.W.S.; Leung, M.W.Y.; Tam, P.K.H.; Wong, K.K.Y. Life long follow up and management strategies of patients living with native livers after Kasai portoenterostomy. Sci. Rep. 2021, 11, 11207. [Google Scholar] [CrossRef]
- Bijl, E.J.; Bharwani, K.D.; Houwen, R.H.J.; De Man, R.A. The long-term outcome of the Kasai operation in patients with biliary atresia: A systematic review. Neth. J. Med. 2013, 71, 170–173. [Google Scholar]
- Samyn, M. Transitional care of biliary atresia. Semin. Pediatr. Surg. 2020, 29, 150948. [Google Scholar] [CrossRef]
- Cortes-Cerisuelo, M.; Boumpoureka, C.; Cassar, N.; Joshi, D.; Samyn, M.; Heneghan, M.; Menon, K.; Prachalias, A.; Srinivasan, P.; Jassem, W.; et al. Liver Transplantation for Biliary Atresia in Adulthood: Single-Centre Surgical Experience. J. Clin. Med. 2021, 10, 4969. [Google Scholar] [CrossRef]
- Westbrook, R.H.; Yeoman, A.D.; O’Grady, J.G.; Harrison, P.M.; Devlin, J.; Heneghan, M.A. Model for End-Stage Liver Disease Score Predicts Outcome in Cirrhotic Patients During Pregnancy. Clin. Gastroenterol. Hepatol. 2011, 9, 694–699. [Google Scholar] [CrossRef]
- Matarazzo, L.; Assandro, P.; Martelossi, S.; Maggiore, G.; Ventura, A. Multiple successful pregnancies in a woman with biliary atresia and native liver. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 221, 194–195. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Nio, M.; Hayashi, Y.; Ishii, T.; Sano, N.; Ohi, R. Problems during and after pregnancy in female patients with biliary atresia. J. Pediatr. Surg. 2007, 42, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- Mass, K.; Quint, E.H.; Punch, M.R.; Merion, R.M. Gynecological and Reproductive Function after Liver Transplantation. Transplantation 1996, 62, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Jabiry-Zieniewicz, Z.; Kaminski, P.; Bobrowska, K.; Pietrzak, B.; Wielgos, M.; Smoter, P.; Zieniewicz, K.; Krawczyk, M. Menstrual Function in Female Liver Transplant Recipients of Reproductive Age. Transplant. Proc. 2009, 41, 1735–1739. [Google Scholar] [CrossRef]
- Hukkinen, M.; Lohi, J.; Heikkilä, P.; Kivisaari, R.; Jahnukainen, T.; Jalanko, H.; Pakarinen, M.P. Noninvasive Evaluation of Liver Fibrosis and Portal Hypertension After Successful Portoenterostomy for Biliary Atresia. Hepatol. Commun. 2019, 3, 382–391. [Google Scholar] [CrossRef] [Green Version]
- Moazzam, Z.; Ziogas, I.A.; Wu, W.K.; Rauf, M.A.; Pai, A.K.; Hafberg, E.T.; Gillis, L.A.; Izzy, M.; Matsuoka, L.K.; Alexopoulos, S.P. Delay in liver transplantation referral for adolescents with biliary atresia transitioning to adult care: A slippery slope. Br. J. Surg. 2021, 108, e324–e325. [Google Scholar] [CrossRef]
- Jain, V.; Burford, C.; Alexander, E.C.; Dhawan, A.; Joshi, D.; Davenport, M.; Heaton, N.; Hadzic, N.; Samyn, M. Adult Liver Disease Prognostic Modelling for Long-term Outcomes in Biliary Atresia: An Observational Cohort Study. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 93–98. [Google Scholar] [CrossRef]
- Alexander, E.C.M.; Greaves, W.M.; Vaidya, H.J.M.; Burford, C.M.; Jain, V.M.; Samyn, M. Social and Educational Outcomes in Patients with Biliary Atresia: A Systematic Review. J. Pediatr. Gastroenterol. Nutr. 2021, 74, 104–109. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Europe | America | Asia | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| France (this study) | France (last 3 cohorts) | UK (16) | Switzerland (19) | Netherlands (17) | Netherlands (18) | Nordic countries (20) | Canada (21,22) | USA: BARC (9 Expert centers) (23) | Taiwan (15) | Japan (13) | |
| Years | 1986–2015 | 1997–2015 | 1999–2009 | 1994–2004 | 1977–1988 | 1987–2008 | 2005–2016 | 1985–2002 | 1997–2000 | 2004–2009/2010 * | 1989–2015 |
| Max follow-up | 30 y | 20 y | 10 y | 10 y | 31 y | 22 y | 12 y | 18 y | 2 y | 7 y | 28 y |
| N patients | 1428 | 951 | 443 | 48 | 104 | 231 | 154 | 349 | 104 (All after Kop) | 197 (170 *) | 3160 |
| N Kasai op | 1340 (94%) | 895 (94%) | 424 (96%) | 43 (90%) | 104 (100%) | 214 (93%) | 148 (96%) | 312 (89%) | 104 (-) | 193 (98%) | 3090 (98%) |
| Age at KOp, days | 59 (6–199) | 57 (6–199) | 54 (7–209) | 68 (30–126) | 59 (25–222) | 59 (20–210) | 60 (4–165) | 65 (6–200) | 61 | Term: 53 +/− 19 | 68 |
| Median (range) or mean ± SD | Preterm: 72 +/− 28 | ||||||||||
| Documented clearance of jaundice after Kasai op | 38% | 39% | 55% | 39.5% | – | 34% | 64% | NA | NA | Term: 62% Preterm 37% (bilirubin < 34 µmol/L) | 58% † |
| SNL after K op | |||||||||||
| At last follow-up | 34% | 41% | 50% | 40% | – | – | 55% ‡ | 27% | 56% | 18 months SNL: | |
| 10 y (CI 95%) | 35% (34–36) | 36% (34–38) | 40% (34–46) | 33% (26–40) | – | 4 y: 46% (42–50) | 45% (35–55) ‡ | 26% (20–32) | – | Term 73% | – |
| 20 y (CI 95%) | 26% (24–28) | 26% (24–28) | – | – | 27% § | – | – | – | – | Preterm: 50% | – |
| 30 y (CI 95%) | 22% (20–24) | – | – | – | – | – | – | – | – | 49% | |
| Death without LT | 10% | 7% | 6% | 8% | 50% | – | 8% | 12% | 4% (all after Kop) | – | – |
| N transplanted patients at last follow-up | 793 (56%) | 512 (54%) | 194 (44%) | 27 (56%) | 26 (25%) | 69 (32%)‖ | 64 (42%) | 210 (60%) | 42 (40%) | 41 (20%) | 1236 (39%) |
| Survival after LT | ‖ | ||||||||||
| At last follow-up | 84% | 90% | 93% | 100% | 73% | NA | 86% | 80% | 88% | 32 (78%) | 1134 (92%) |
| 5 y (CI 95%) | 85% (84–86) | 90% (89–91) | – | 100% | 4 y: 79% ‖ | 84% (74–94) | 4 y: 83% (77–88) | – | – | ||
| 10 y (CI 95%) | 84% (83–85) | 90% (89–91) | – | – | – | 84% (74–94) | 80% (75–86) | – | – | ||
| 20 y (CI 95%) | 80 (78–82) | 89% (87–91) | – | – | – | – | – | – | – | ||
| 28 y | 79 (77–81) | – | – | – | – | – | – | – | – | ||
| Overall survival | |||||||||||
| At last follow-up | 81% | 87% | 91% | 92% | 43% | NA | 87% | 77% | 91% | – | |
| 5 y (CI 95%) | 82% (81–83) | 87% (86–88) | 90% (88–93) | 92% (87–96) | – | 4 y: 73 (70–76) ‖ | 88% (83–94) | 4 y: 77 (72–82) | – | – | – |
| 10 y (CI 95%) | 80% (79–81) | 86% (85–87) | 89% (86–93) | – | – | – | 87% (81–93) | 75% (70–80) | – | – | – |
| 20 y (CI 95%) | 78% (77–79) | 85% (84–86) | – | – | – | – | – | – | – | – | 89% |
| 30 y (CI 95%) | 76% (74–78) | – | – | – | 43% | – | – | – | – | – | – |
| Population 2018 (million people) | 68 | 66 | 8.6 | 17 | 27 | 36 | 326 | 24 | 127 | ||
| Incidence of BA (CI 95%) | 1/19,600 (1/18,200–1/21,100) | 1/17,000 – | 1/17,800 (1/13,900–1/24,800) | 1/18,600 | – | – | 1/19,000 (1/17,800–1/20,300) | – | 1/6600 (1/ 4200–1/7000) | 1/13,500 (1/11, 300–1/17,000) | |
| % of BASM | 8.2% | 11% (37) | 8% | 5% | 12% | 14% | 11% | – | 2% | ||
| Univariate Analysis | ||||||
|---|---|---|---|---|---|---|
| SNL _ SE standard error (number of patients alive with native liver at follow-up) | ||||||
| Prognostic factor | N patients | 5-Y SNL | 10-Y SNL | 20-Y SNL | 30-Y SNL | p |
| Anatomical pattern of the extra hepatic biliary remnant | <0.0001 | |||||
| Type 1 | 20 | 89.7% ± 6.9% (18) | 84.1% ± 8.4% (16) | 75.7% ± 11.2% (11) | 75.7% ± 11.2% (11) | |
| Type 2 | 104 | 60.4% ± 5.1% (47) | 51.6% ± 5.7% (26) | 44.3% ± 6.3% (15) | 36.9% ± 8.6% (6) | |
| Type 3 | 235 | 48.2% ± 3.4% (92) | 42.9% ± 3.5% (68) | 29.9% ± 3.8% (25) | 29.9% ± 3.8% (25) | |
| Type 4 | 917 | 36.0% ± 1.7% (264) | 30.7% ± 1.6% (184) | 23.1% ± 1.8% (48) | 18.1% ± 2.8% (11) | |
| Missing data | 64 | |||||
| BASM syndrome | <0.0001 | |||||
| No | 1002 | 44.0% ± 1.6% (366) | 38.5% ± 1.6% (258) | 28.4% ± 1.8% (72) | 24.7% ± 2.4% (19) | |
| Yes | 118 | 20.8% ± 3.8% (20) | 15.4% ± 3.7% (11) | 15.4% ± 3.7% (11) | 7.7% ± 5.7% (2) | |
| Missing data | ||||||
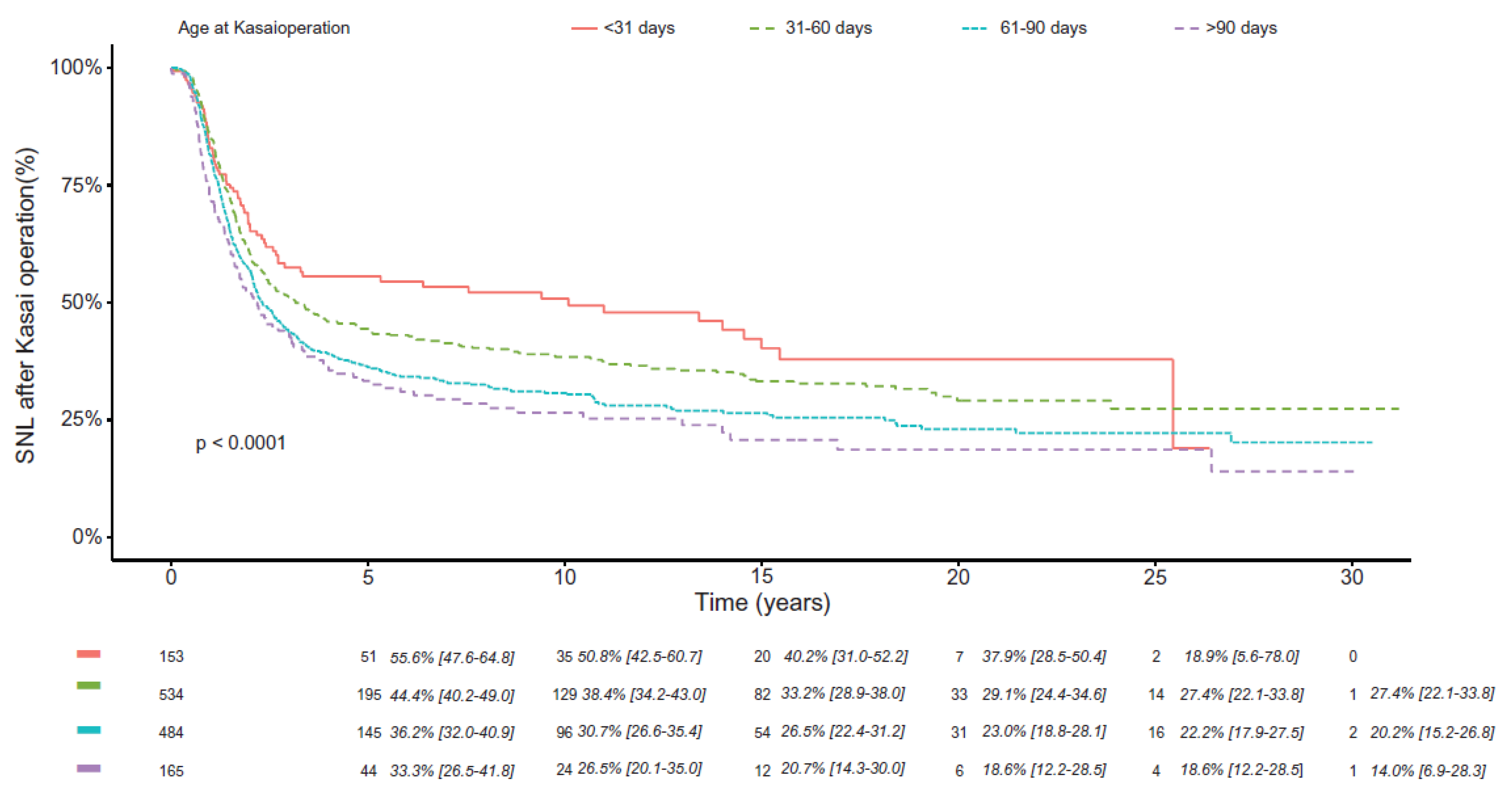
| Age at Kasai operation | <0.0001 | |||||
| <31 days | 153 | 55.6% ± 4.4% (60) | 50.8% ± 4.6% (39) | 37.9% ± 5.5% (17) | 18.9% ± 13.7% (2) | |
| 31–60 days | 534 | 44.4% ± 2.2% (197) | 38.4% ± 2.2% (134) | 29.1% ± 2.6% (34) | 27.4% ± 2.9% (17) | |
| 61–90 days | 484 | 36.2% ± 2.3% (146) | 30.7% ± 2.2% (102) | 23.0% ± 2.4% (35) | 20.2% ± 2.9% (11) | |
| >90 days | 165 | 33.3% ± 3.8% (45) | 26.7% ± 3.7% (27) | 18.6% ± 4.0% (10) | 14.0% ± 5.0% (4) | |
| Missing data | 4 | |||||
| Multivariate analysis | ||||||
| Prognostic factor | Hazard ratio | 95% CI | p | |||
| Anatomical pattern of the extrahepatic biliary remnant | ||||||
| Type 1 | 0.145 | 0.046–0.453 | 0.0009 | |||
| Type 2 | 0.531 | 0.387–0.728 | ||||
| Type 3 | 0.746 | 0.605–0.920 | ||||
| Type 4 | 1 | |||||
| BASM syndrome | ||||||
| No | 0.550 | 0.438–0.691 | <0.0001 | |||
| Yes | 1 | |||||
| Age at Kasai operation | ||||||
| <31 days | 0.538 | 0.388–0.745 | 0.0002 | |||
| 31–60 days | 0.616 | 0.488–0.779 | ||||
| 61–90 days | 0.766 | 0.604–0.971 | ||||
| >90 days | 1 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kelly, D.; Samyn, M.; Schwarz, K.B. Biliary Atresia in Adolescence and Adult Life: Medical, Surgical and Psychological Aspects. J. Clin. Med. 2023, 12, 1594. https://doi.org/10.3390/jcm12041594
Kelly D, Samyn M, Schwarz KB. Biliary Atresia in Adolescence and Adult Life: Medical, Surgical and Psychological Aspects. Journal of Clinical Medicine. 2023; 12(4):1594. https://doi.org/10.3390/jcm12041594
Chicago/Turabian StyleKelly, Deirdre, Marianne Samyn, and Kathleen B. Schwarz. 2023. "Biliary Atresia in Adolescence and Adult Life: Medical, Surgical and Psychological Aspects" Journal of Clinical Medicine 12, no. 4: 1594. https://doi.org/10.3390/jcm12041594