
Gut Microbiota in Patients with Postoperative Atrial Fibrillation Undergoing Off-Pump Coronary Bypass Graft Surgery


Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
2.2. DNA Isolation, 16S rRNA Gene Amplification and Bioinformatics
2.3. Plasma Vitamin D Measurement
2.4. Systemic Inflammation
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients
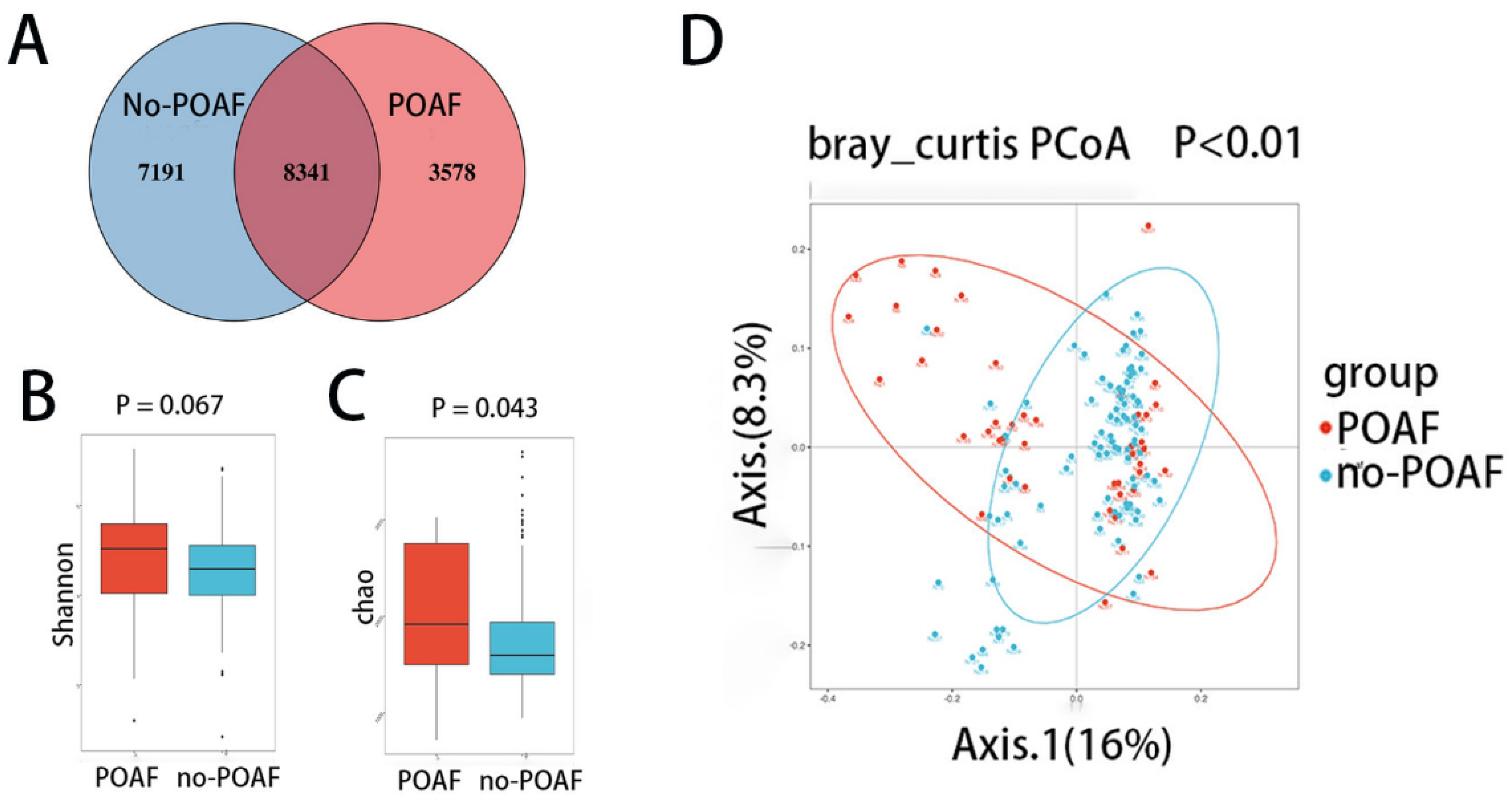
3.2. Diversity of the Fecal Microbiota in POAF Patients
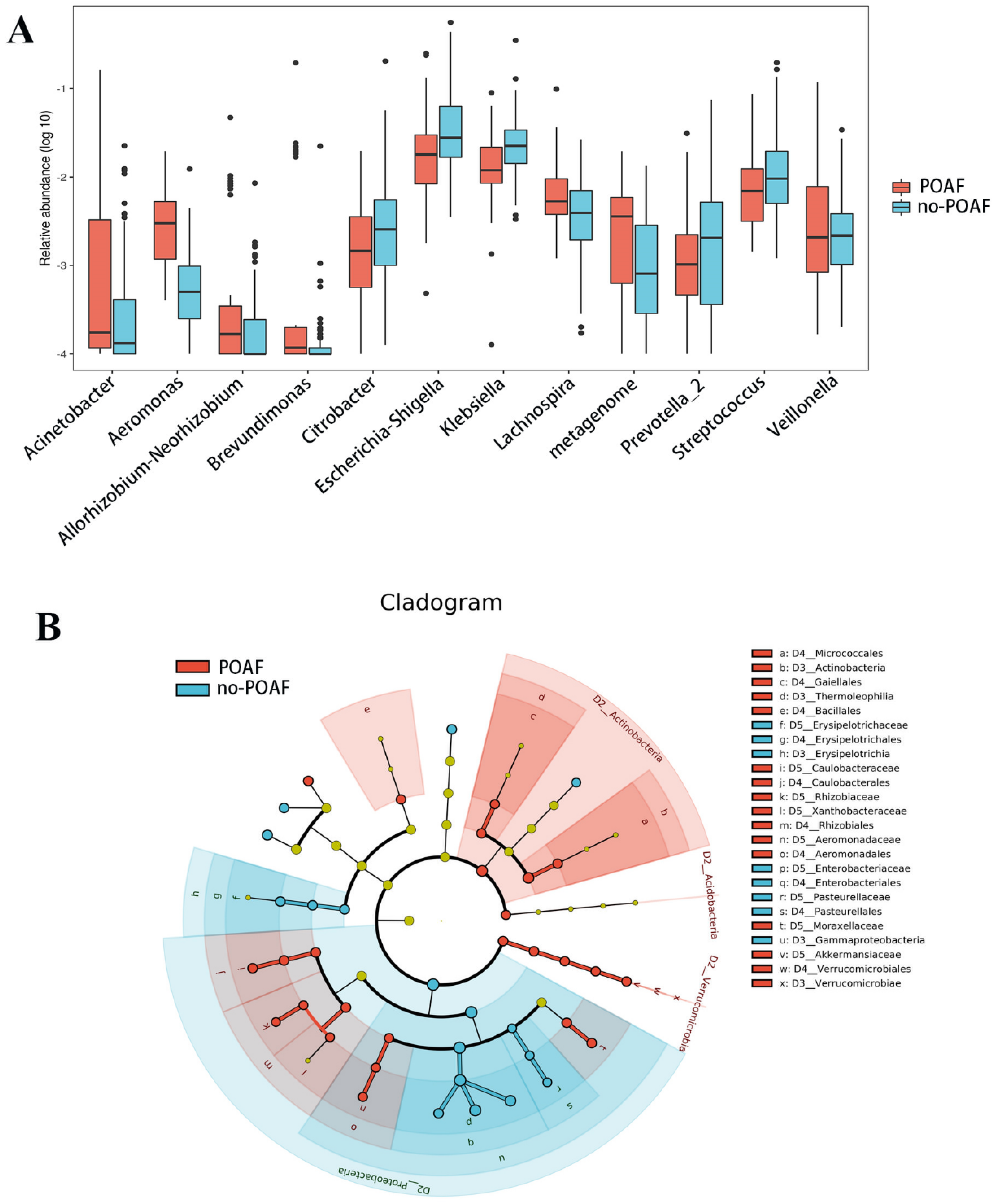
3.3. Taxonomic Changes in Gut Microbiota
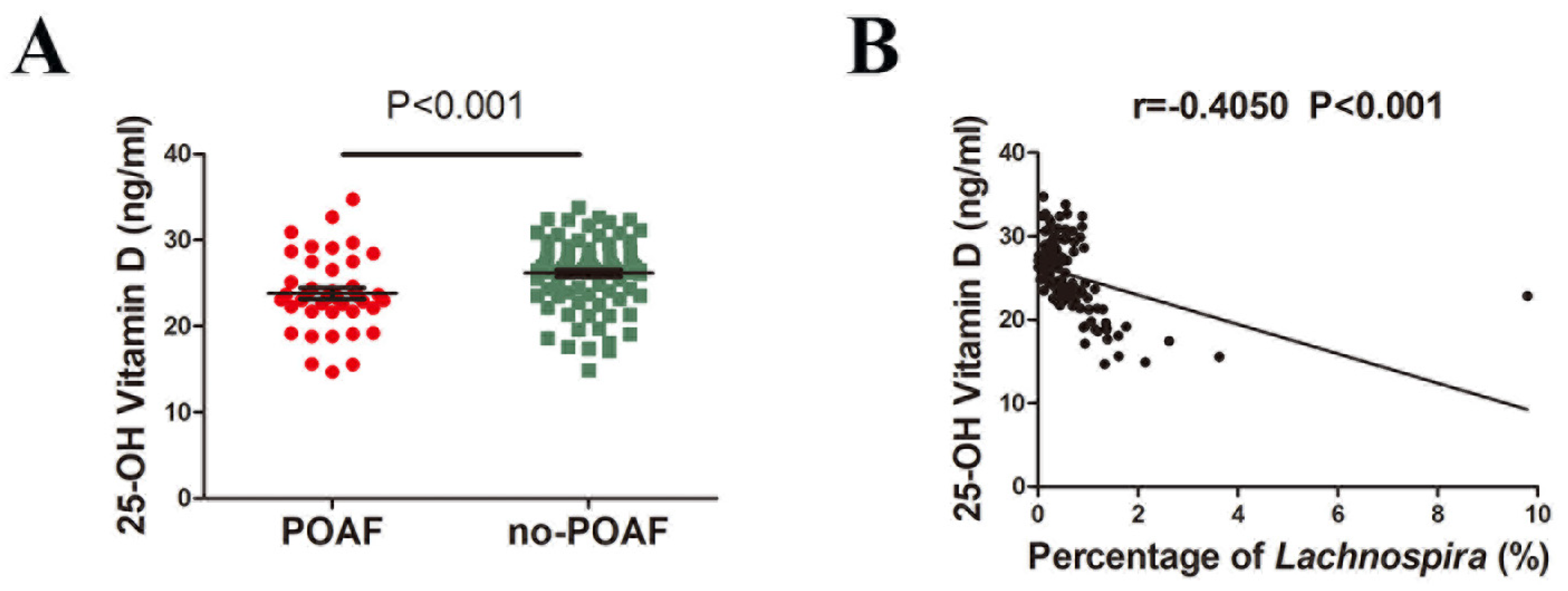
3.4. Correlations between Lachnospira and Plasma Vitamin D Levels
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, H.; Zhang, Y.; Xin, F.; Jiang, H.; Tao, D.; Jin, Y.; He, Y.; Wang, Q.; Po, S.S. Calcium-Induced Autonomic Denervation in Patients with Post-Operative Atrial Fibrillation. J. Am. Coll. Cardiol. 2021, 77, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.F.; Saraiva, F.; Moreira, R.; Cerqueira, R.; Amorim, M.; Pinho, P.; Lourenço, A.; Leite-Moreira, A. Postoperative Atrial Fibrillation After Coronary Artery Bypass Grafting Surgery. Rev. Port. Cir. Cardio-Torac. Vasc. 2017, 24, 129. [Google Scholar]
- Filardo, G.; Damiano, R.J., Jr.; Ailawadi, G.; Thourani, V.H.; Pollock, B.D.; Sass, D.M.; Phan, T.K.; Nguyen, H.; Da Graca, B. Epidemiology of new-onset atrial fibrillation following coronary artery bypass graft surgery. Heart 2018, 104, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, M.; Ahmed, A.; Massie, V.; Marshall, E.; Harky, A. Determinants of atrial fibrillation after cardiac surgery. Rev. Cardiovasc. Med. 2021, 22, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Musa, A.F.; Cheong, X.P.; Dillon, J.; Nordin, R.B. Validation of EuroSCORE II in patients undergoing coronary artery bypass grafting (CABG) surgery at the National Heart Institute, Kuala Lumpur: A retrospective review. F1000Research 2018, 7, 534. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.A.; Mahajan, A.; Cabaj, M.; Kimball, T.H.; Morselli, M.; Soehalim, E.; Chapski, D.J.; Montoya, D.; Farrell, C.P.; Scovotti, J.; et al. DNA Methylation-Based Prediction of Post-operative Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 9, 837725. [Google Scholar] [CrossRef]
- Wang, M.K.; Meyre, P.B.; Heo, R.; Devereaux, P.; Birchenough, L.; Whitlock, R.; McIntyre, W.F.; Chen, Y.C.P.; Ali, M.Z.; Biancari, F.; et al. Short-term and Long-term Risk of Stroke in Patients With Perioperative Atrial Fibrillation After Cardiac Surgery: Systematic Review and Meta-analysis. CJC Open 2022, 4, 85–96. [Google Scholar] [CrossRef]
- Maesen, B.; Nijs, J.; Maessen, J.; Allessie, M.; Schotten, U. Post-operative atrial fibrillation: A maze of mechanisms. Europace 2012, 14, 159–174. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, S.; Xu, Y.; Liu, Y.; Li, Z.; Zhang, Y.; Jin, Y.; Xue, X.; Wang, H. Relation of Mitochondrial DNA Copy Number in Peripheral Blood to Postoperative Atrial Fibrillation After Isolated Off-Pump Coronary Artery Bypass Grafting. Am. J. Cardiol. 2017, 119, 473–477. [Google Scholar] [CrossRef]
- Tang, W.H.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef]
- Gebrayel, P.; Nicco, C.; Al Khodor, S.; Bilinski, J.; Caselli, E.; Comelli, E.M.; Egert, M.; Giaroni, C.; Karpinski, T.M.; Loniewski, I.; et al. Microbiota medicine: Towards clinical revolution. J. Transl. Med. 2022, 20, 111. [Google Scholar] [CrossRef]
- Li, J.; Zhao, F.; Wang, Y.; Chen, J.; Tao, J.; Tian, G.; Wu, S.; Liu, W.; Cui, Q.; Geng, B.; et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome 2017, 5, 14. [Google Scholar] [CrossRef]
- Zuo, K.; Yin, X.; Li, K.; Zhang, J.; Wang, P.; Jiao, J.; Liu, Z.; Liu, X.; Liu, J.; Li, J.; et al. Different Types of Atrial Fibrillation Share Patterns of Gut Microbiota Dysbiosis. mSphere 2020, 5, e00071-20. [Google Scholar] [CrossRef]
- Drapkina, O.M.; Yafarova, A.A.; Kaburova, A.N.; Kiselev, A.R. Targeting Gut Microbiota as a Novel Strategy for Prevention and Treatment of Hypertension, Atrial Fibrillation and Heart Failure: Current Knowledge and Future Perspectives. Biomedicines 2022, 10, 2019. [Google Scholar] [CrossRef] [PubMed]
- Zuo, K.; Li, J.; Wang, P.; Liu, Y.; Liu, Z.; Yin, X.; Liu, X.; Yang, X. Duration of Persistent Atrial Fibrillation Is Associated with Alterations in Human Gut Microbiota and Metabolic Phenotypes. mSystems 2019, 4, e00422-19. [Google Scholar] [CrossRef] [PubMed]
- Tabata, T.; Yamashita, T.; Hosomi, K.; Park, J.; Hayashi, T.; Yoshida, N.; Saito, Y.; Fukuzawa, K.; Konishi, K.; Murakami, H.; et al. Gut microbial composition in patients with atrial fibrillation: Effects of diet and drugs. Heart Vessel. 2021, 36, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.-L.; Li, S.-J.; Lee, T.-I.; Lee, T.-W.; Chung, C.-C.; Kao, Y.-H.; Chen, Y.-J. Sugar Fructose Triggers Gut Dysbiosis and Metabolic Inflammation with Cardiac Arrhythmogenesis. Biomedicines 2021, 9, 728. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, S.; Li, B.; Luo, Y.; Gong, Y.; Jin, X.; Zhang, J.; Zhou, Y.; Zhuo, X.; Wang, Z.; et al. Gut microbiota dysbiosis promotes age-related atrial fibrillation by lipopolysaccharide and glucose-induced activation of NLRP3-inflammasome. Cardiovasc. Res. 2022, 118, 785–797. [Google Scholar] [CrossRef]
- Lu, D.; Zou, X.; Zhang, H. The Relationship Between Atrial Fibrillation and Intestinal Flora With Its Metabolites. Front. Cardiovasc. Med. 2022, 9, 948755. [Google Scholar] [CrossRef]
- Yuan, X.; Long, Y.; Ji, Z.; Gao, J.; Fu, T.; Yan, M.; Zhang, L.; Su, H.; Zhang, W.; Wen, X.; et al. Green Tea Liquid Consumption Alters the Human Intestinal and Oral Microbiome. Mol. Nutr. Food Res. 2018, 62, e1800178. [Google Scholar] [CrossRef]
- Magoc, T.; Salzberg, S.L. FLASH: Fast length adjustment of short reads to improve genome assemblies. Bioinformatics 2011, 27, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Gonzalez Peña, A.; Goodrich, J.K.; Gordon, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Han, J.; Zengwei, W.; Zongtao, Y.; Yan, J.; Jian, Z. A Modified Maze Versus Cut-and-Sew Maze for Long-Standing Persistent Atrial Fibrillation Concomitant with Mitral Valve Surgery: A Propensity Score-Matched Cohort Study. Heart Lung Circ. 2022, 31, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Jian, Z.; Xu, Y.; Shu, X.; Yu, L.; Wang, H. Plasma Circular RNAs, Hsa_circRNA_025016, Predict Postoperative Atrial Fibrillation After Isolated Off-pump Coronary Artery Bypass Grafting. J. Am. Heart Assoc. 2018, 7, e006642. [Google Scholar]
- Matsumoto, N.; Park, J.; Tomizawa, R.; Kawashima, H.; Hosomi, K.; Mizuguchi, K.; Honda, C.; Ozaki, R.; Iwatani, Y.; Watanabe, M.; et al. Relationship between Nutrient Intake and Human Gut Microbiota in Monozygotic Twins. Medicina 2021, 57, 275. [Google Scholar] [CrossRef]
- Zuo, K.; Li, J.; Li, K.; Hu, C.; Gao, Y.; Chen, M.; Hu, R.; Liu, Y.; Chi, H.; Wang, H.; et al. Disordered gut microbiota and alterations in metabolic patterns are associated with atrial fibrillation. GigaScience 2019, 8, giz058. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Jiang, H.; Tao, D.; Zhao, K.; Yin, Z.; Han, J.; Xin, F.; Jin, Y.; Wang, H. Preventive Effect of Berberine on Postoperative Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2022, 15, e011160. [Google Scholar] [CrossRef]
- Qu, L.; Dong, Z.; Ma, S.; Liu, Y.; Zhou, W.; Wang, Z.; Wu, C.; Ma, R.; Jiang, X.; Zu, T.; et al. Gut Microbiome Signatures Are Predictive of Cognitive Impairment in Hypertension Patients-A Cohort Study. Front. Microbiol. 2022, 13, 841614. [Google Scholar] [CrossRef]
- Hayashi, T.; Yamashita, T.; Watanabe, H.; Kami, K.; Yoshida, N.; Tabata, T.; Emoto, T.; Sasaki, N.; Mizoguchi, T.; Irino, Y.; et al. Gut Microbiome and Plasma Microbiome-Related Metabolites in Patients With Decompensated and Compensated Heart Failure. Circ. J. 2018, 83, 182–192. [Google Scholar] [CrossRef]
- Barsan, M.; Brata, A.M.; Ismaiel, A.; Dumitrascu, D.I.; Badulescu, A.-V.; Duse, T.A.; Dascalescu, S.; Popa, S.L.; Grad, S.; Muresan, L.; et al. The Pathogenesis of Cardiac Arrhythmias in Vitamin D Deficiency. Biomedicines 2022, 10, 1239. [Google Scholar] [CrossRef]
- Canpolat, U.; Aytemir, K.; Hazirolan, T.; Ozer, N.; Oto, A. Relationship between vitamin D level and left atrial fibrosis in patients with lone paroxysmal atrial fibrillation undergoing cryoballoon-based catheter ablation. J. Cardiol. 2017, 69, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Kostin, S.; Klein, G.; Szalay, Z.; Hein, S.; Bauer, E.P.; Schaper, J. Structural correlate of atrial fibrillation in human patients. Cardiovasc. Res. 2002, 54, 361–379. [Google Scholar] [CrossRef]
- Li, D.; Fareh, S.; Leung, T.K.; Nattel, S. Promotion of atrial fibrillation by heart failure in dogs: Atrial remodeling of a different sort. Circulation 1999, 100, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Xu, C.; Xue, X.; Xu, Y.; Zhao, J.; Huang, T.; Wang, Z.; Zhao, Q.; Zhou, Z.; Huang, Y.; et al. Activation of cannabinoid receptor 2 attenuates Angiotensin II-induced atrial fibrillation via a potential NOX/CaMKII mechanism. Front. Cardiovasc. Med. 2022, 9, 968014. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.-M.; Dong, X.; Zhao, J.-K.; Xu, Y.-L.; Xu, D.-Y.; Xue, X.-D.; Zhou, Z.-J.; Huang, Y.-T.; Zhao, Q.-S.; Luo, L.-Y.; et al. Activation of PKG-CREB-KLF15 by melatonin attenuates Angiotensin II-induced vulnerability to atrial fibrillation via enhancing branched-chain amino acids catabolism. Free Radic. Biol. Med. 2022, 178, 202–214. [Google Scholar] [CrossRef]
- Rahimi, M.; Taban-Sadeghi, M.; Nikniaz, L.; Pashazadeh, F. The relationship between preoperative serum vitamin D deficiency and postoperative atrial fibrillation: A systematic review and meta-analysis. J. Cardiovasc. Thorac. Res. 2021, 13, 102–108. [Google Scholar] [CrossRef]
- Skuladottir, G.V.; Cohen, A.; Arnar, D.O.; Hougaard, D.M.; Torfason, B.; Palsson, R.; Indridason, O.S. Plasma 25-hydroxyvitamin D2 and D3 levels and incidence of postoperative atrial fibrillation. J. Nutr. Sci. 2016, 5, e10. [Google Scholar] [CrossRef]
- Talasaz, A.H.; Salehiomran, A.; Heidary, Z.; Gholami, K.; Aryannejad, H.; Jalali, A.; Daei, M. The effects of vitamin D supplementation on postoperative atrial fibrillation after coronary artery bypass grafting in patients with vitamin D deficiency. J. Card. Surg. 2022, 37, 2219–2224. [Google Scholar] [CrossRef]
- Kara, H.; Yasim, A. Effects of high-dose vitamin D supplementation on the occurrence of post-operative atrial fibrillation after coronary artery bypass grafting: Randomized controlled trial. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 477–484. [Google Scholar] [CrossRef]
- Cerit, L.; Ozcem, B.; Cerit, Z.; Duygu, H. Preventive Effect of Preoperative Vitamin D Supplementation on Postoperative Atrial Fibrillation. Braz. J. Cardiovasc. Surg. 2018, 33, 347–352. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | POAF (n = 45) | NO-POAF (n = 89) | p |
|---|---|---|---|
| Age (y) | 64.6 (60, 69.50) | 63.5 (59.75, 67.25) | 0.495 |
| Female sex, % | 13 (28.88) | 24 (26.96) | 0.887 |
| Body mass index | 24.78 (22.4, 27.1) | 25.17 (23.15, 26.65) | 0.425 |
| Smoking history, % | 24 (53.33) | 49 (55.05) | 0.903 |
| Hypertension, % | 24 (53.33) | 55 (61.79) | 0.389 |
| Diabetes mellitus, % | 17 (37.78) | 35 (39.3) | 0.804 |
| Hyperlipidemia, % | 19 (42.22) | 36 (40.45) | 0.806 |
| NYHA = I–III | |||
| I | 18 (40.00) | 29 (32.22) | 1.000 |
| II | 24 (53.33) | 55 (61.79) | |
| III | 3 (6.67) | 5 (5.56) | |
| Left ventricular ejection fraction, % | 57.1 (56, 60) | 56.2 (53, 60) | 0.459 |
| Left atrial size (mm) | 37.78 (34, 41) | 36.76 (33.75, 39) | 0.122 |
| LVEDV (mL) | 100.4 (89, 105) | 101.44 (83.75, 112.50) | 0.785 |
| LMCA stenosis (≥50%) | 14 (31.11) | 27 (30.30) | 0.895 |
| Right coronary stenosis (≥70%) | 36 (80.00) | 73 (82.02) | 0.878 |
| Calcium channel blockers, % | 25 (55.56) | 52 (58.24) | 0.806 |
| Beta-blockers, % | 45 (100) | 89 (100) | 1.000 |
| Use statins, % | 7 (15.56) | 15 (16.85) | 0.870 |
| creatinine (mg/dL) | 69.35 (54.9, 77.47) | 73.80 (61.91, 85.43) | 0.144 |
| BNP (pg/mL) | 447.72 (85.6, 427.25) | 538.98 (108.47, 581.05) | 0.444 |
| CKMB | 11.12 (7.60, 13.75) | 11.90 (9.00, 14.00) | 0.176 |
| HsTnT (ng/mL) | 0.173 (0.010, 0.059) | 0.098 (0.01, 0.463) | 0.567 |
| CRP (mg/L) | 2.80 (0.20, 29.20) | 3.050 (0.20, 76.60) | 0.758 |
| IL-6 (pg/mL) | 6.56 (1.85, 34.97) | 5.36 (1.58, 70.81) | 0.268 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; He, Y.; Li, R.; Jiang, H.; Tao, D.; Zhao, K.; Yin, Z.; Zhang, J.; Wang, H. Gut Microbiota in Patients with Postoperative Atrial Fibrillation Undergoing Off-Pump Coronary Bypass Graft Surgery. J. Clin. Med. 2023, 12, 1493. https://doi.org/10.3390/jcm12041493
Wang Y, He Y, Li R, Jiang H, Tao D, Zhao K, Yin Z, Zhang J, Wang H. Gut Microbiota in Patients with Postoperative Atrial Fibrillation Undergoing Off-Pump Coronary Bypass Graft Surgery. Journal of Clinical Medicine. 2023; 12(4):1493. https://doi.org/10.3390/jcm12041493
Chicago/Turabian StyleWang, Yang, Yuanchen He, Rui Li, Hui Jiang, Dengshun Tao, Keyan Zhao, Zongtao Yin, Jian Zhang, and Huishan Wang. 2023. "Gut Microbiota in Patients with Postoperative Atrial Fibrillation Undergoing Off-Pump Coronary Bypass Graft Surgery" Journal of Clinical Medicine 12, no. 4: 1493. https://doi.org/10.3390/jcm12041493