

Development and Validation of a Nomogram for Predicting Blood Pressure Change Failure in Patients with Pheochromocytoma and Concomitant Hypertension after Adrenalectomy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
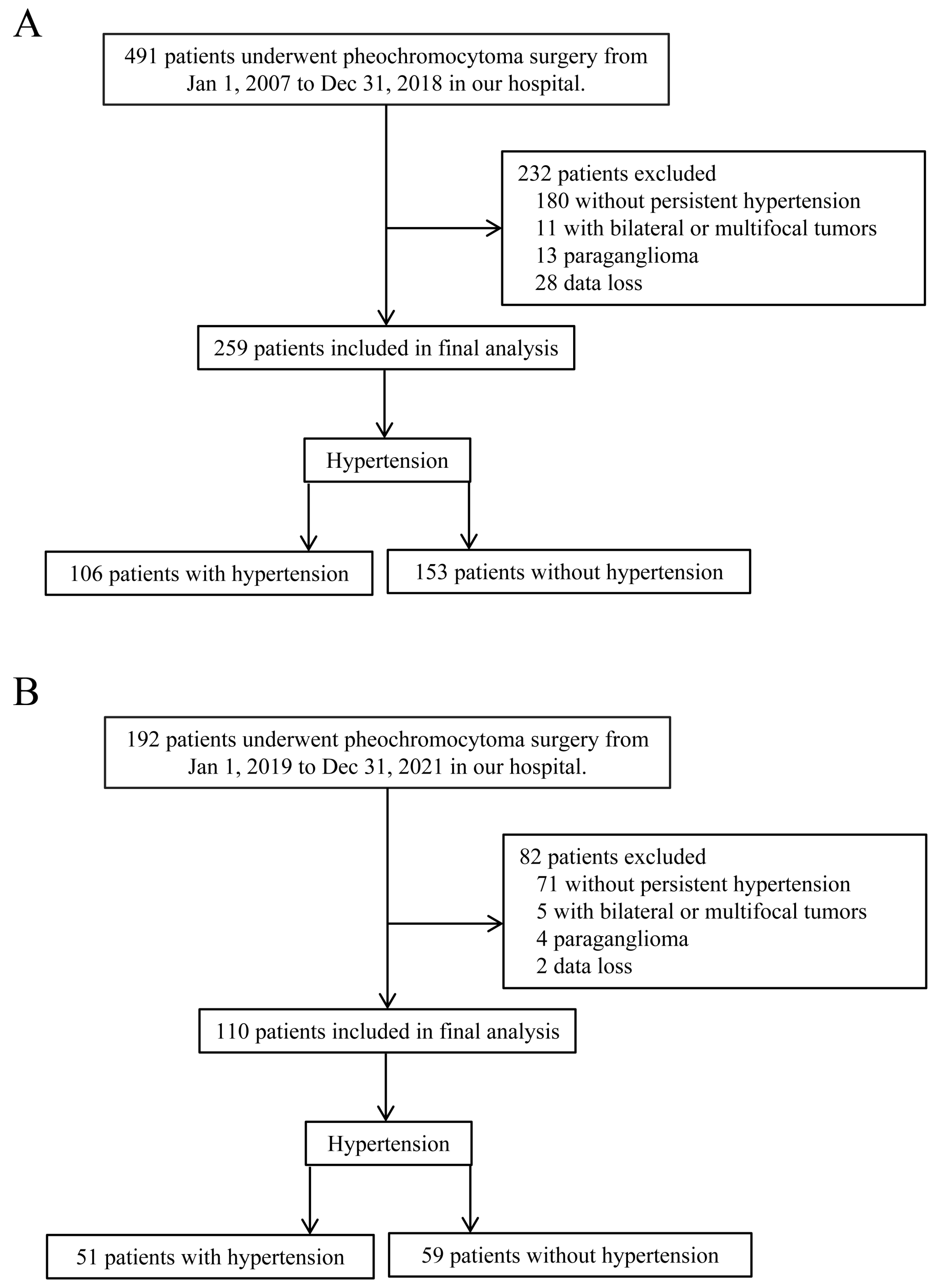
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Preoperative Preparation
2.4. Characteristics and Outcome
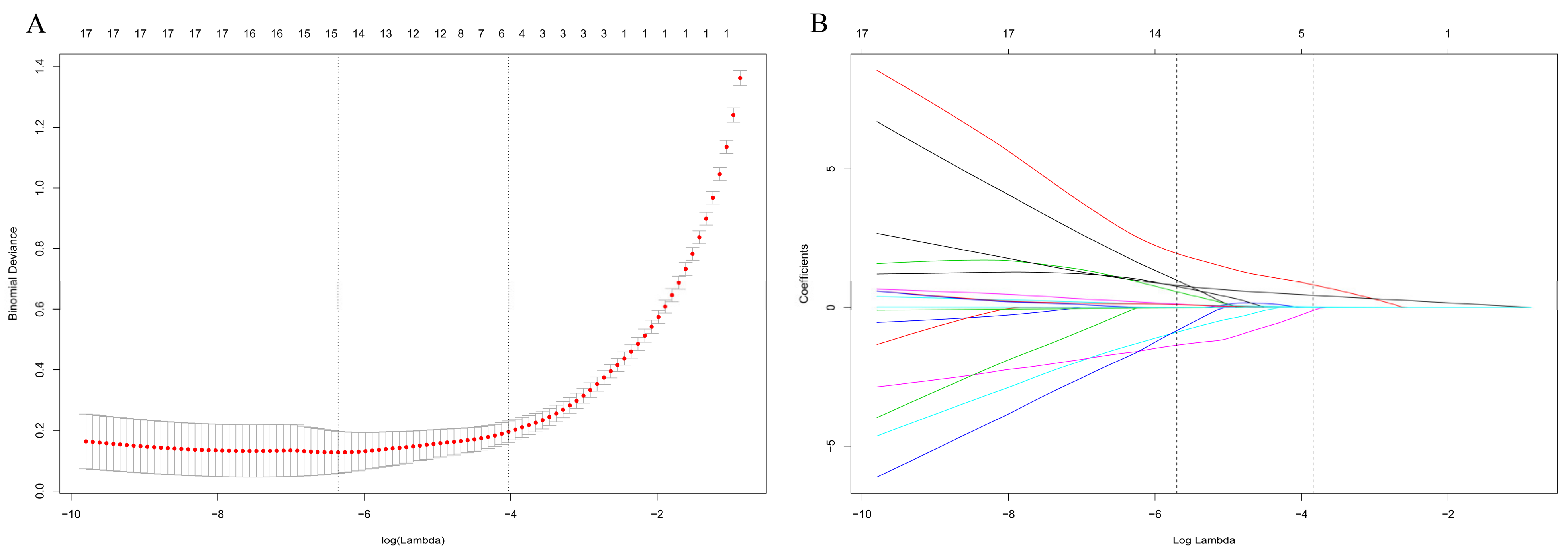
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berends, A.M.A.; Buitenwerf, E.; de Krijger, R.R.; Veeger, N.; van der Horst-Schrivers, A.N.A.; Links, T.P.; Kerstens, M.N. Incidence of pheochromocytoma and sympathetic paraganglioma in the Netherlands: A nationwide study and systematic review. Eur. J. Intern. Med. 2018, 51, 68–73. [Google Scholar] [CrossRef]
- Anderson, G.H., Jr.; Blakeman, N.; Streeten, D.H. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J. Hypertens. 1994, 12, 609–615. [Google Scholar] [CrossRef]
- Omura, M.; Saito, J.; Yamaguchi, K.; Kakuta, Y.; Nishikawa, T. Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens. Res. 2004, 27, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenders, J.W.; Duh, Q.Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.P.; Grebe, S.K.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F., Jr.; Endocrine, S. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelinka, T.; Eisenhofer, G.; Pacak, K. Pheochromocytoma as a catecholamine producing tumor: Implications for clinical practice. Stress 2007, 10, 195–203. [Google Scholar] [CrossRef]
- Werbel, S.S.; Ober, K.P. Pheochromocytoma. Update on diagnosis, localization, and management. Med. Clin. N. Am. 1995, 79, 131–153. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Duh, Q.Y. Benign and malignant pheochromocytoma: Diagnosis, treatment, and follow-Up. Surg. Oncol. Clin. N. Am. 1998, 7, 765–789. [Google Scholar] [CrossRef]
- Lenders, J.W.; Eisenhofer, G.; Mannelli, M.; Pacak, K. Phaeochromocytoma. Lancet 2005, 366, 665–675. [Google Scholar] [CrossRef]
- Neumann, H.P.H.; Young, W.F., Jr.; Eng, C. Pheochromocytoma and Paraganglioma. N. Engl. J. Med. 2019, 381, 552–565. [Google Scholar] [CrossRef]
- Weingarten, T.N.; Welch, T.L.; Moore, T.L.; Walters, G.F.; Whipple, J.L.; Cavalcante, A.; Bancos, I.; Young, W.F., Jr.; Gruber, L.M.; Shah, M.Z.; et al. Preoperative Levels of Catecholamines and Metanephrines and Intraoperative Hemodynamics of Patients Undergoing Pheochromocytoma and Paraganglioma Resection. Urology 2017, 100, 131–138. [Google Scholar] [CrossRef]
- Sapienza, P.; Cavallaro, A. Persistent hypertension after removal of adrenal tumours. Eur. J. Surg. 1999, 165, 187–192. [Google Scholar]
- Plouin, P.F.; Chatellier, G.; Fofol, I.; Corvol, P. Tumor recurrence and hypertension persistence after successful pheochromocytoma operation. Hypertension 1997, 29, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Karakiewicz, P.I.; Briganti, A.; Chun, F.K.; Trinh, Q.D.; Perrotte, P.; Ficarra, V.; Cindolo, L.; De la Taille, A.; Tostain, J.; Mulders, P.F.; et al. Multi-institutional validation of a new renal cancer-specific survival nomogram. J. Clin. Oncol. 2007, 25, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Stolk, R.F.; Bakx, C.; Mulder, J.; Timmers, H.J.; Lenders, J.W. Is the excess cardiovascular morbidity in pheochromocytoma related to blood pressure or to catecholamines? J. Clin. Endocrinol. Metab. 2013, 98, 1100–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, P.; Ramachandran, R.; Tandon, N.; Kumar, R. Changes in blood pressure, blood sugar, and quality of life in patients undergoing pheochromocytoma surgery: A prospective cohort study. Indian J. Urol. 2019, 35, 34–40. [Google Scholar] [PubMed]
- Pogorzelski, R.; Toutounchi, S.; Krajewska, E.; Fiszer, P.; Lykowski, M.; Zapala, L.; Szostek, M.; Jakuczun, W.; Pachucki, J.; Skorski, M. The effect of surgical treatment of phaeochromocytoma on concomitant arterial hypertension and diabetes mellitus in a single-centre retrospective study. Cent. Eur. J. Urol. 2014, 67, 361–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, D.; Fisher, P.B. Molecular mechanisms of aging-associated inflammation. Cancer Lett. 2006, 236, 13–23. [Google Scholar] [CrossRef]
- Buford, T.W. Hypertension and aging. Ageing Res. Rev. 2016, 26, 96–111. [Google Scholar] [CrossRef] [Green Version]
- Andrus, E.C.; Allen, E.V.; Merritt, H.H.; Duff, G.L.; Moore, R.A.; Kendall, F.E.; Shumacker, H.B., Jr.; Levy, R.L.; Wright, I.S. The pathogenesis of arteriosclerosis. Int. J. Epidemiol. 2015, 44, 1791–1793. [Google Scholar]
- Benetos, A.; Adamopoulos, C.; Bureau, J.M.; Temmar, M.; Labat, C.; Bean, K.; Thomas, F.; Pannier, B.; Asmar, R.; Zureik, M.; et al. Determinants of accelerated progression of arterial stiffness in normotensive subjects and in treated hypertensive subjects over a 6-year period. Circulation 2002, 105, 1202–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenfeld, J.D.; Sealey, J.E.; Schlussel, Y.; Vaughan, E.D., Jr.; Sos, T.A.; Atlas, S.A.; Muller, F.B.; Acevedo, R.; Ulick, S.; Laragh, J.H. Diagnosis and treatment of primary hyperaldosteronism. Ann. Intern. Med. 1994, 121, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Dao, H.H.; Essalihi, R.; Bouvet, C.; Moreau, P. Evolution and modulation of age-related medial elastocalcinosis: Impact on large artery stiffness and isolated systolic hypertension. Cardiovasc. Res. 2005, 66, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Streeten, D.H.P.; Anderson, G.H.; Wagner, S. Effect of age on response of secondary hypertension to specific treatment. Am. J. Hypertens. 1990, 3, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Plouin, P.F.; Duclos, J.M.; Soppelsa, F.; Boublil, G.; Chatellier, G. Factors associated with perioperative morbidity and mortality in patients with pheochromocytoma: Analysis of 165 operations at a single center. J. Clin. Endocrinol. Metab. 2001, 86, 1480–1486. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Development Cohort | Validation Cohort |
|---|---|---|
| Number of patients (%) | 259 (100) | 110 (100) |
| Demographic characteristics | ||
| Mean age (years) | 56.0 (49.0, 66.0) | 53.0 (49.0, 64.0) |
| Gender (male/female) | 114 (44.0)/145 (56.0) | 52 (47.3)/58 (52.7) |
| BMI (kg/m2) | 23.5 (21.1, 25.4) | 23.9 (21.1, 25.6) |
| Comorbidities | ||
| Duration of hypertension (months) | 23.0 (21.0, 33.0) | 25.0 (20.0, 33.0) |
| Cardiovascular events (yes) | 101 (39.0) | 44 (28.8) |
| Diabetes Mellitus (yes) | 107 (41.3) | 45 (40.9) |
| Preoperative data | ||
| Tumor side (left/right) | 117 (45.2)/142 (54.8) | 46 (41.8)/64 (58.2) |
| Tumor size (cm) | 5.0 (3.9, 6.5) | 5.0 (3.9, 6.0) |
| Enhanced CT difference (Hu) | 41 (20, 65) | 40.0 (21.0, 70.0) |
| Types of α adrenoreceptor antagonists (prazosin)(prazosinothers) | 148 (57.1) | 66 (60.0) |
| Use of crystalloid and colloid infusion (yes) | 162 (62.54) | 74 (67.3) |
| VMA/upper limits of normal value | 1.9 (1.3, 2.8) | 1.97 (1.38, 2.78) |
| Intraoperative data | ||
| Operation approach (open/laparoscopy) | 48 (18.5)/211 (81.5) | 18 (16.4.)/92(83.6) |
| IHD | 78 (30.1) | 28 (25.5) |
| Estimated blood loss (ml) | 200 (100, 500) | 200 (100, 400) |
| Operation duration (minutes) | 150 (95, 185) | 141 (103, 184) |
| Postoperative data | ||
| Use of NE | 61 (23.6) | 23 (20.9) |
| Postoperative transfusion | 53 (20.5) | 23 (20.9) |
| Development Cohort 259 (100) | Validation Cohort 110 (100) | |||||
|---|---|---|---|---|---|---|
| Variables | Without Hypertension | Hypertension | p-Value | Without Hypertension | Hypertension | p-Value |
| Number of patients (%) | 153 (59.1) | 106 (40.9) | 59 (53.6) | 51 (46.4) | ||
| Demographic characteristics | ||||||
| Mean age (years) | 52.0 (44.0, 61.0) | 64.0 (52.0, 72.0) | <0.001 | 51.0 (44.0, 56.0) | 64.0 (52.0, 71.0) | < 0.001 |
| Gender (male/female) | 68 (44.4)/85 (55.6) | 46 (43.4)/60 (56.6) | 0.867 | 27 (45.8)/32 (52.4) | 25 (49.0)/26 (51.0) | 0.733 |
| BMI (kg/m2) | 23.4 (21.3, 25.3) | 24.2 (20.8, 25.6) | 0.827 | 24.2 (21.5, 25.4) | 23.4 (20.8, 25.8) | 0.442 |
| Comorbidities | ||||||
| Duration of hypertension (months) | 21.0 (19.0, 23.0) | 36.0 (32.0, 41.0) | <0.001 | 21.0 (17.0, 23.0) | 34.0 (31.0, 40.0) | 0.001 |
| Cardiovascular events (yes) | 44 (28.8) | 57 (53.8) | <0.001 | 20 (33.9) | 29 (56.9) | 0.017 |
| Diabetes Mellitus (yes) | 47 (30.7) | 60 (56.6) | <0.001 | 18 (30.5) | 27 (52.9) | 0.018 |
| Preoperative data | ||||||
| Tumor side (left/right) | 80 (52.3)/73 (47.7) | 37 (34.9)/69 (65.1) | 0.006 | 31 (52.5)/28 (47.5) | 15 (29.4)/36 (70.4) | 0.015 |
| Tumor size (cm) | 4.7 (35, 6.2) | 5.2 (4.3, 7.0) | <0.001 | 4.3 (3.1, 5.9) | 5.2 (4.5, 6.5) | 0.004 |
| Enhanced CT difference (Hu) | 40.0 (21.0, 65.0) | 45.0 (20.0, 79.0) | 0.079 | 40.0 (21.0, 65.0) | 45.0 (20.0, 79.0) | 0.285 |
| Types of α adrenoreceptor antagonists (prazosin vs. others) | 89 (58.2) | 59 (55.7) | 0.548 | 40 (67.8) | 26 (51.0) | 0.074 |
| Use of crystalloid and colloid infusion | 98 (64.1) | 64 (60.4) | 0.368 | 40 (67.8) | 34 (66.7) | 0.900 |
| VMA/upper limits of normal value | 1.57 (1.05, 2.38) | 2.29 (1.87,3.71) | <0.001 | 1.59 (1.22, 2.32) | 2.24 (1.70,3.72) | 0.008 |
| Intraoperative data | ||||||
| Operation approach (open/laparoscopy) | 32 (20.9)/121(79.1) | 16 (15.1)/90 (84.9) | 0.238 | 10 (16.9)/49 (83.1) | 8 (15.7)/43 (84.3) | 0.858 |
| IHD (yes) | 41 (26.8) | 37 (34.9) | 0.163 | 10 (16.9) | 18 (35.3) | 0.030 |
| Estimated blood loss (ml) | 200 (100, 500) | 200 (100, 600) | 0.683 | 200 (100, 300) | 300 (100, 600) | 0.041 |
| Operation duration (minutes) | 150 (100, 195) | 143 (92, 175) | 0.586 | 140 (100, 184) | 160 (103, 185) | 0.243 |
| Postoperative data | ||||||
| Use of NE | 39 (25.5) | 20 (20.8) | 0.378 | 14 (23.7) | 9 (17.6) | 0.435 |
| Postoperative transfusion | 32 (20.9) | 21 (19.8) | 0.829 | 11 (18.6) | 12 (23.5) | 0.531 |
| Variables | β (95% CI) | OR (95% CI) | p |
|---|---|---|---|
| Constant | −33.068 (−49.128, −17.009) | 4.35 × 10−15 (4.61 × 10−22, 4.10 × 10−8) | |
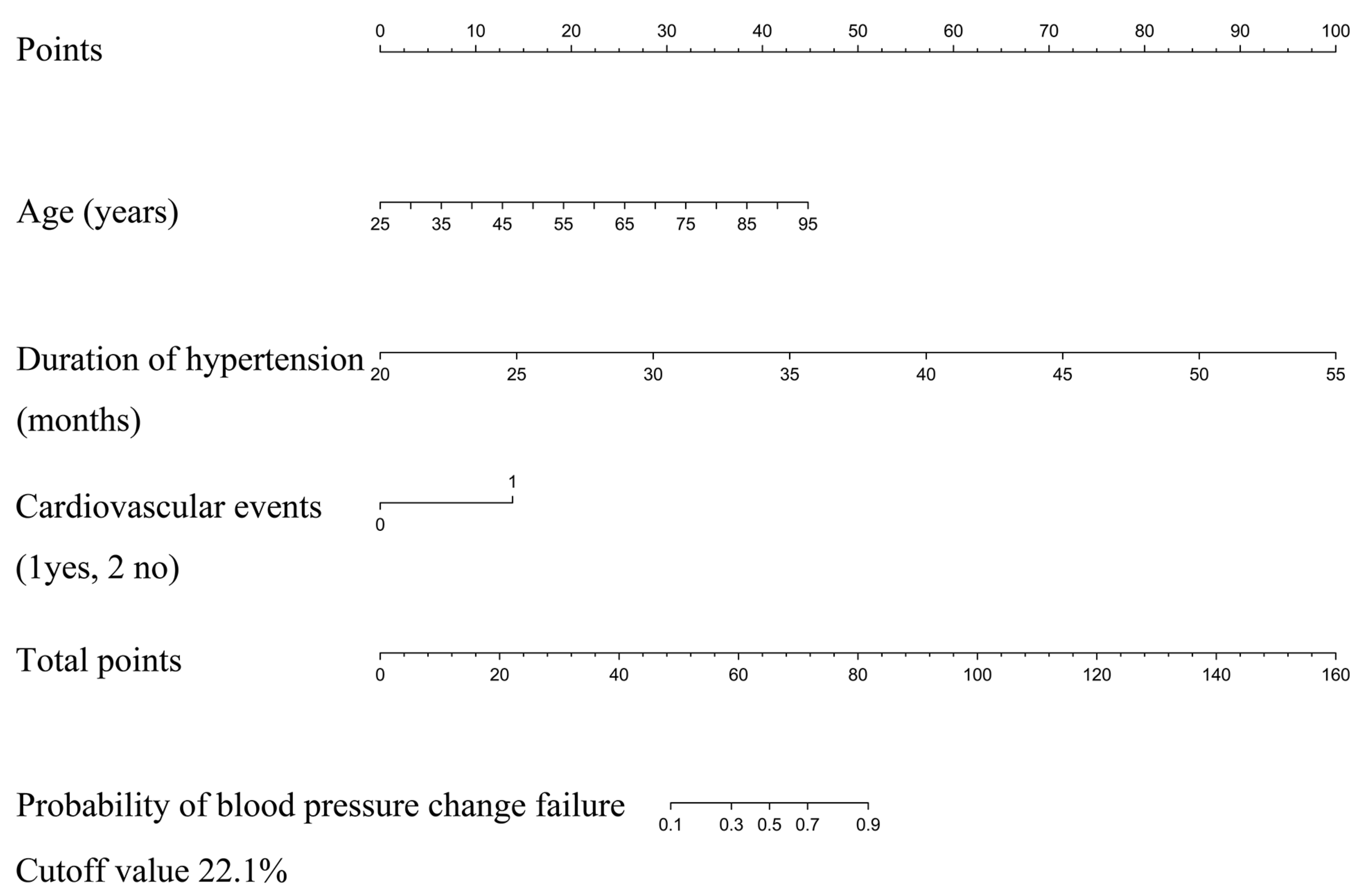
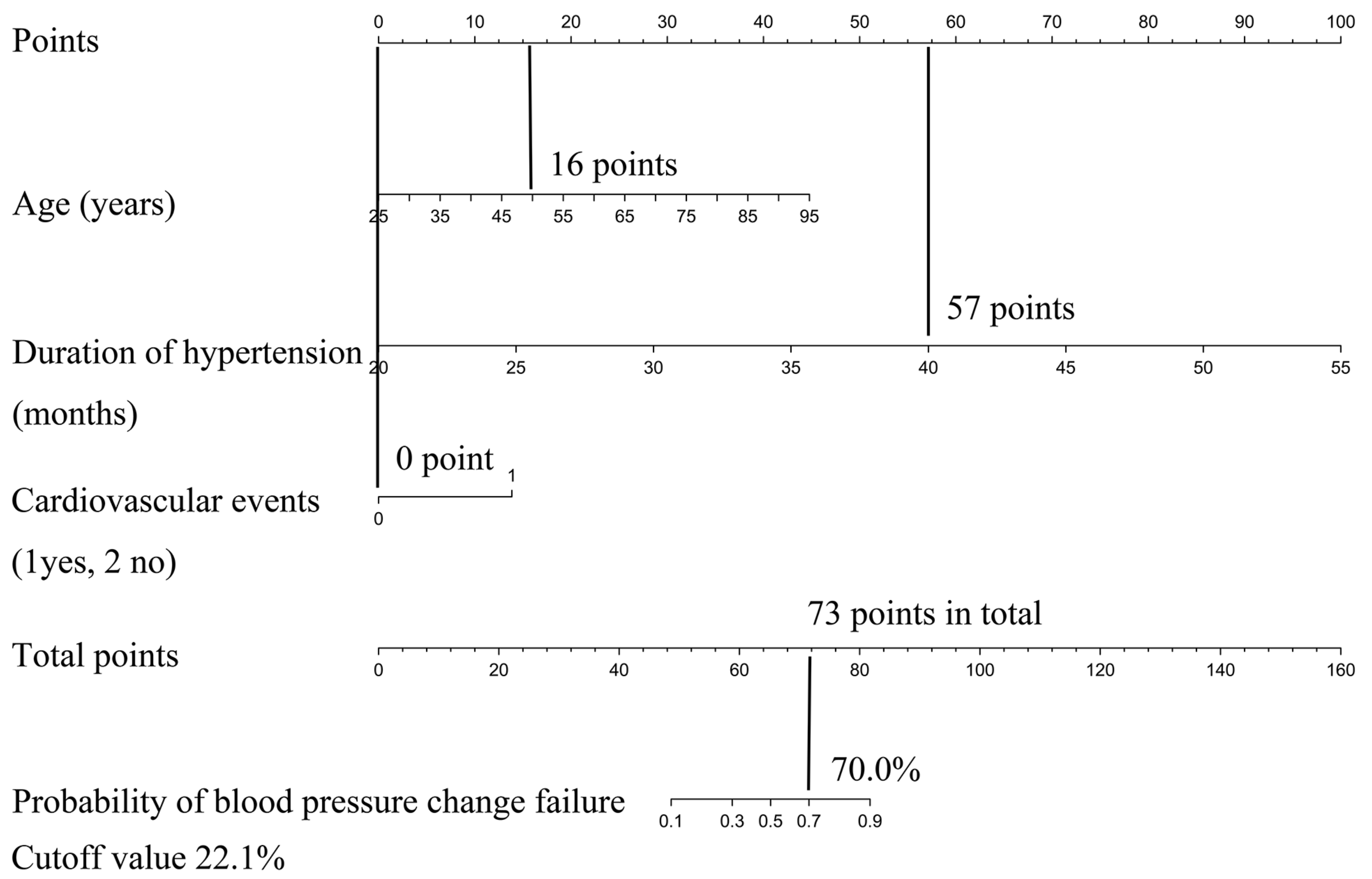
| Mean age (years) | 0.145 (0.008, 0.282) | 1.156 (1.009, 1.324) | 0.037 |
| Duration of hypertension (months) | 1.132 (0.493, 1.771) | 3.103 (1.637, 5.883) | 0.001 |
| Cardiovascular events (yes versus no) | 2.843 (0.011, 5.675) | 17.168 (1.011, 291.414) | 0.049 |
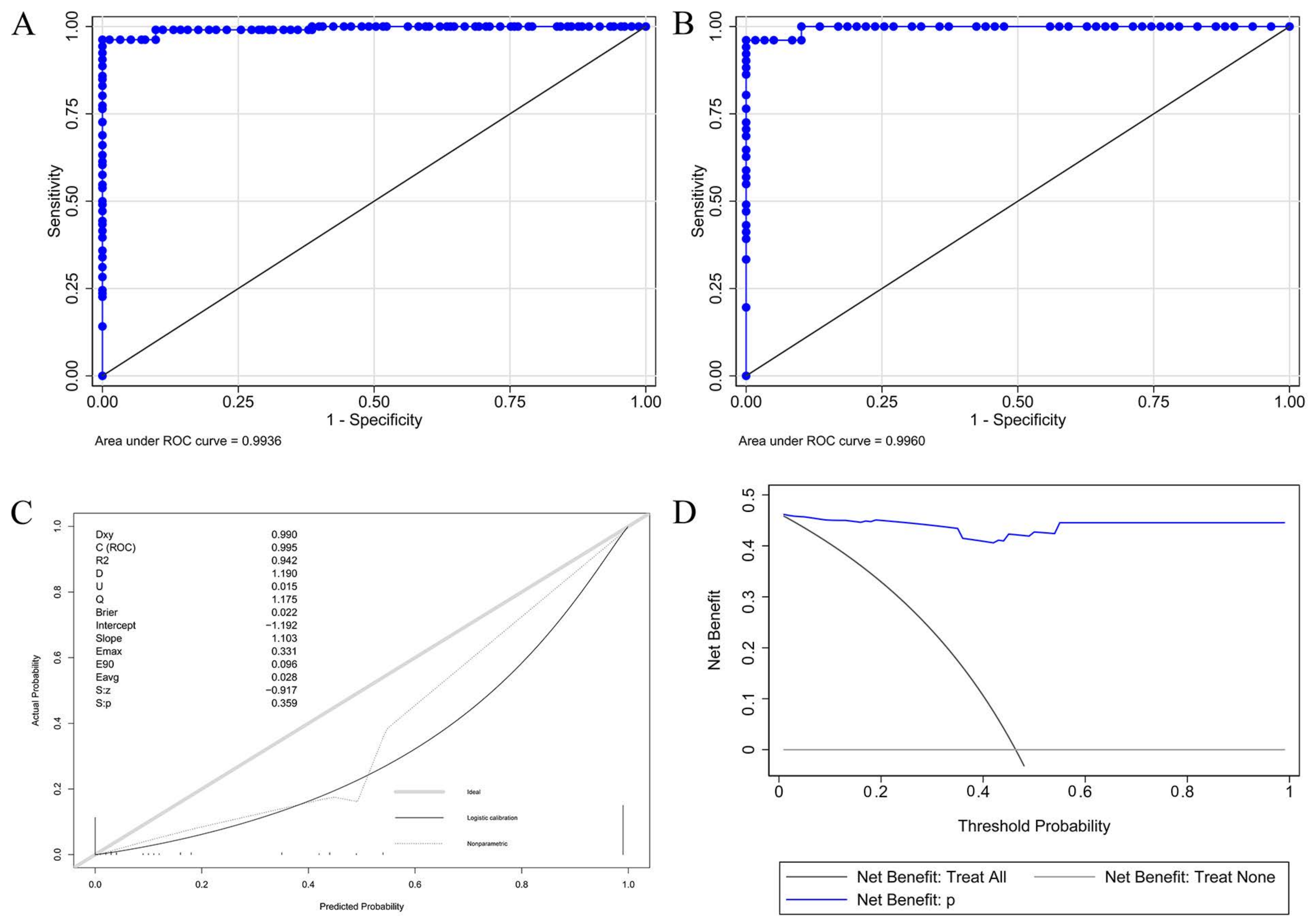
| Area under ROC curve | AUROC 95% CI | ||
| Development cohort | 0.994 (0.986, 1.000) | <0.001 | |
| Validation cohort | 0.996 (0.990, 1.000) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ge, Y.; Zhan, Y.; Pan, C.; Li, J.; Li, Z.; Bai, S.; Liu, L. Development and Validation of a Nomogram for Predicting Blood Pressure Change Failure in Patients with Pheochromocytoma and Concomitant Hypertension after Adrenalectomy. J. Clin. Med. 2023, 12, 874. https://doi.org/10.3390/jcm12030874
Ge Y, Zhan Y, Pan C, Li J, Li Z, Bai S, Liu L. Development and Validation of a Nomogram for Predicting Blood Pressure Change Failure in Patients with Pheochromocytoma and Concomitant Hypertension after Adrenalectomy. Journal of Clinical Medicine. 2023; 12(3):874. https://doi.org/10.3390/jcm12030874
Chicago/Turabian StyleGe, Yuntian, Yunhong Zhan, Chunyu Pan, Jia Li, Zhenhua Li, Song Bai, and Lina Liu. 2023. "Development and Validation of a Nomogram for Predicting Blood Pressure Change Failure in Patients with Pheochromocytoma and Concomitant Hypertension after Adrenalectomy" Journal of Clinical Medicine 12, no. 3: 874. https://doi.org/10.3390/jcm12030874