
Acute Heart Failure: Diagnostic–Therapeutic Pathways and Preventive Strategies—A Real-World Clinician’s Guide
 , , , , , , , , , , , , ,
, , , , , , , , , , , , ,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Epidemiology
3. Management
3.1. Pre-Hospital
3.2. In Hospital
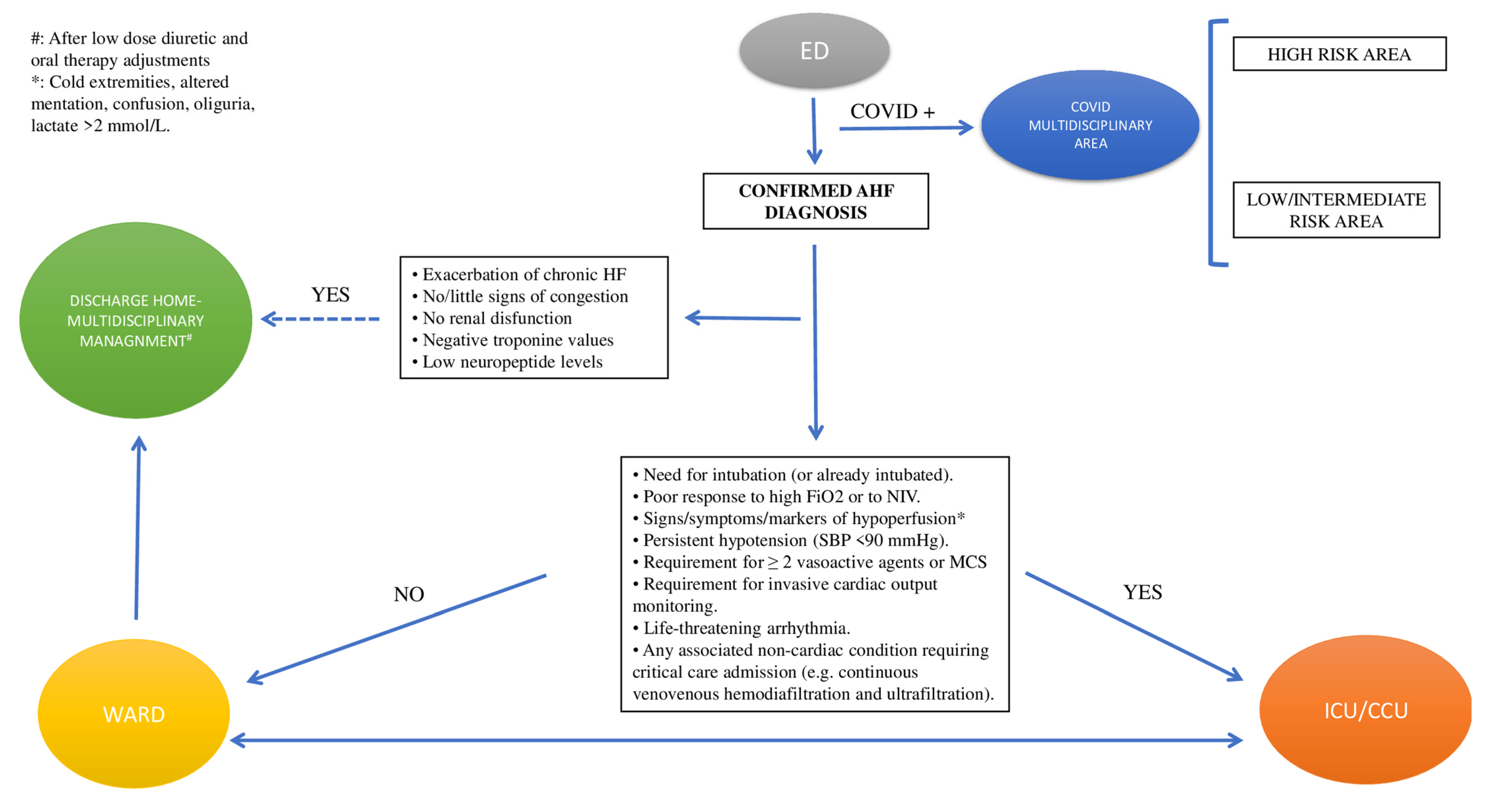
3.2.1. Triage
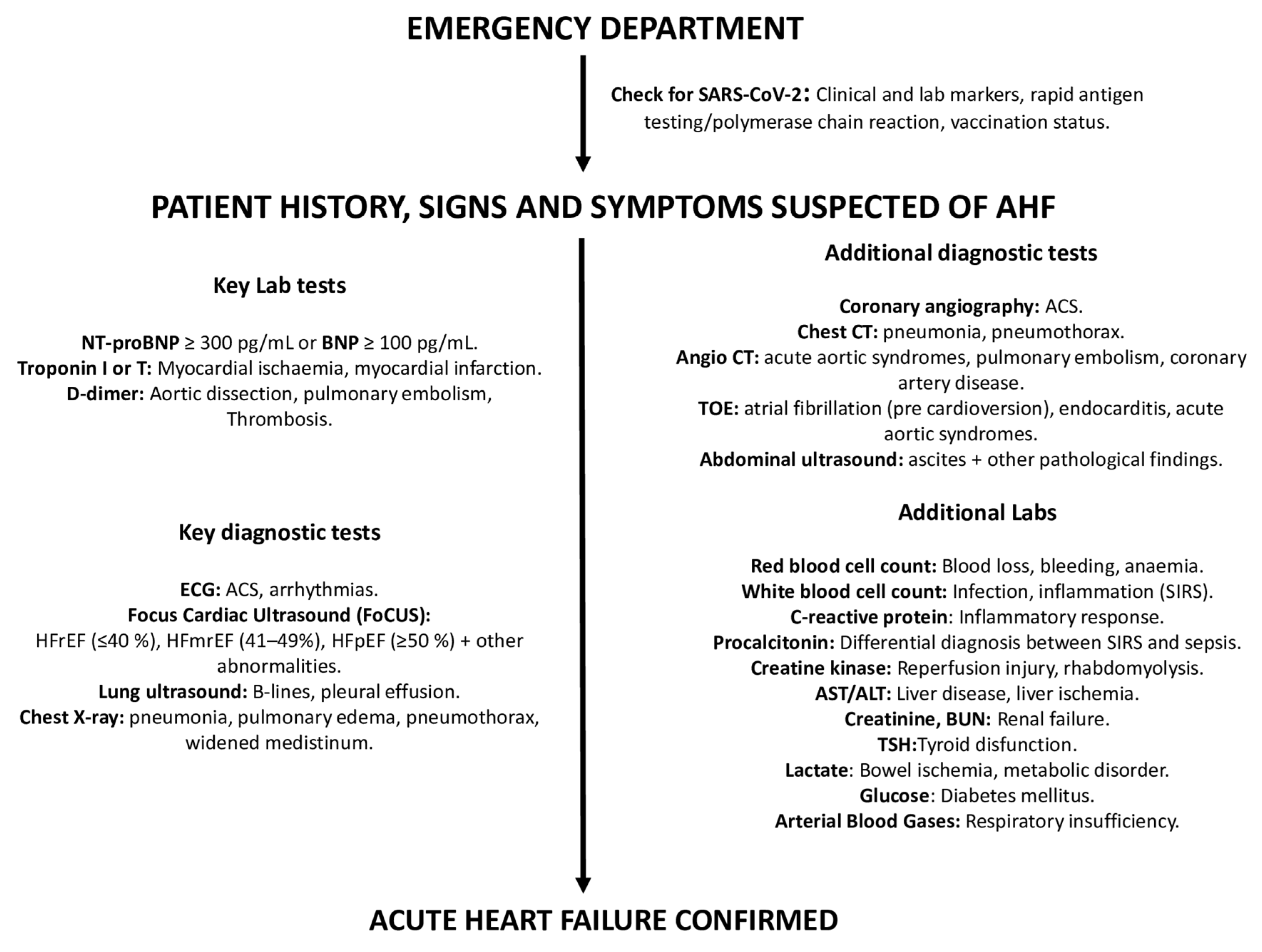
3.2.2. Diagnostic Workup (Figure 2)
Step 1
- a.
- Search for reversible causes (Table 2)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Triggers | Lab Test | Invasive/Non-Invasive Test | Notes |
|---|---|---|---|
| ACS [19,20] | hs-cTn (I or T) |
|
|
| Arrhythmias [21,22,23] | Electrolytes, TFTs |
|
|
| Acute Myocarditis [24] | hs-cTn (I or T), PCR, ESR, WBC count |
|
|
| Endocarditis [25] | ESR, CRP, blood culture, autoimmunity testing in selected cases |
| Patients presenting with severe heart failure or cardiogenic shock should be referred early and managed in a reference center with immediate surgical facilities. |
| Acute aortic syndromes [26] | D-dimer |
| D-dimer is highly sensitive to rule out classical AAD within the first 6 h of symptom onset in low–moderate-risk patients. |
| Mechanical cause (free wall rupture, ventricular septal defect, acute mitral regurgitation, cardiac tamponade) [19,20] | hs-cTn (I or T), D-dimer | TTE | Prompt intervention/surgery is needed; transfer to Hub center. |
| Pulmonary embolism [27] | D-dimer, hs-cTn, ABG |
| If hemodynamically unstable, transfer to ICU. |
| Hypertension emergency [28] | FBC, creatinine, electrolytes, LDH, haptoglobin, hs-cTn, pregnancy test in women of child-bearing age |
| Patients with severe hypertension associated with AHF require an urgent reduction of BP with IV drug administration. |
| Pneumonia [29] | FBC, ESR, CRP, PCT |
| Admission to an ICU for patients with hypotension requiring vasopressors or respiratory failure requiring mechanical ventilation. |
| COPD exacerbation or asthma [30] | ABG, PCR, PCT |
| Admission to an ICU for patients with hypotension requiring vasopressors or respiratory failure requiring mechanical ventilation. |
| Thyroid dysfunction [31] | TFTs |
| Management of myxedema coma and thyroid storm requires both medical and supportive therapies and should be treated in an ICU setting. |
| Anemia [32] | FBC | - | Urgent RBC transfusion needed. |
- b.
- -
- Search for clinical and laboratory clues suggesting COVID-19 infection;
- -
- Perform SARS-CoV-2 rapid antigen testing/polymerase chain reaction;
- -
- Check for COVID-19 vaccination status.
- c.
- Assess presenting symptoms and signs
Step 2
- a.
- Lab tests
- b.
- ECG
- c.
- Chest X-ray
- d.
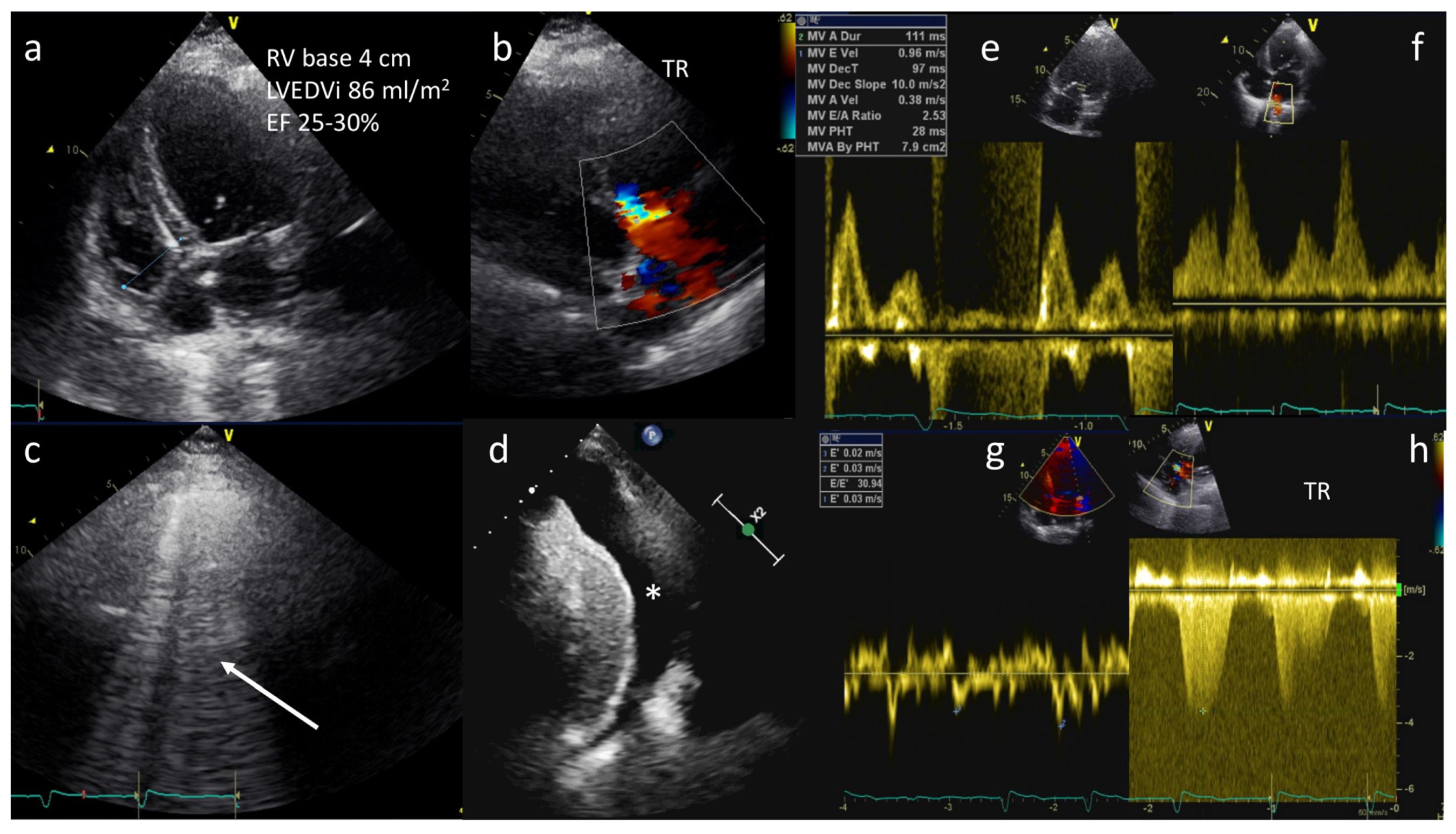
- Transthoracic echocardiography (TTE)
- e.
- Lung ultrasound (LUS)
- f.
- Abdominal ultrasound (AUS)
- g.
- Transesophageal echocardiogram (TEE)
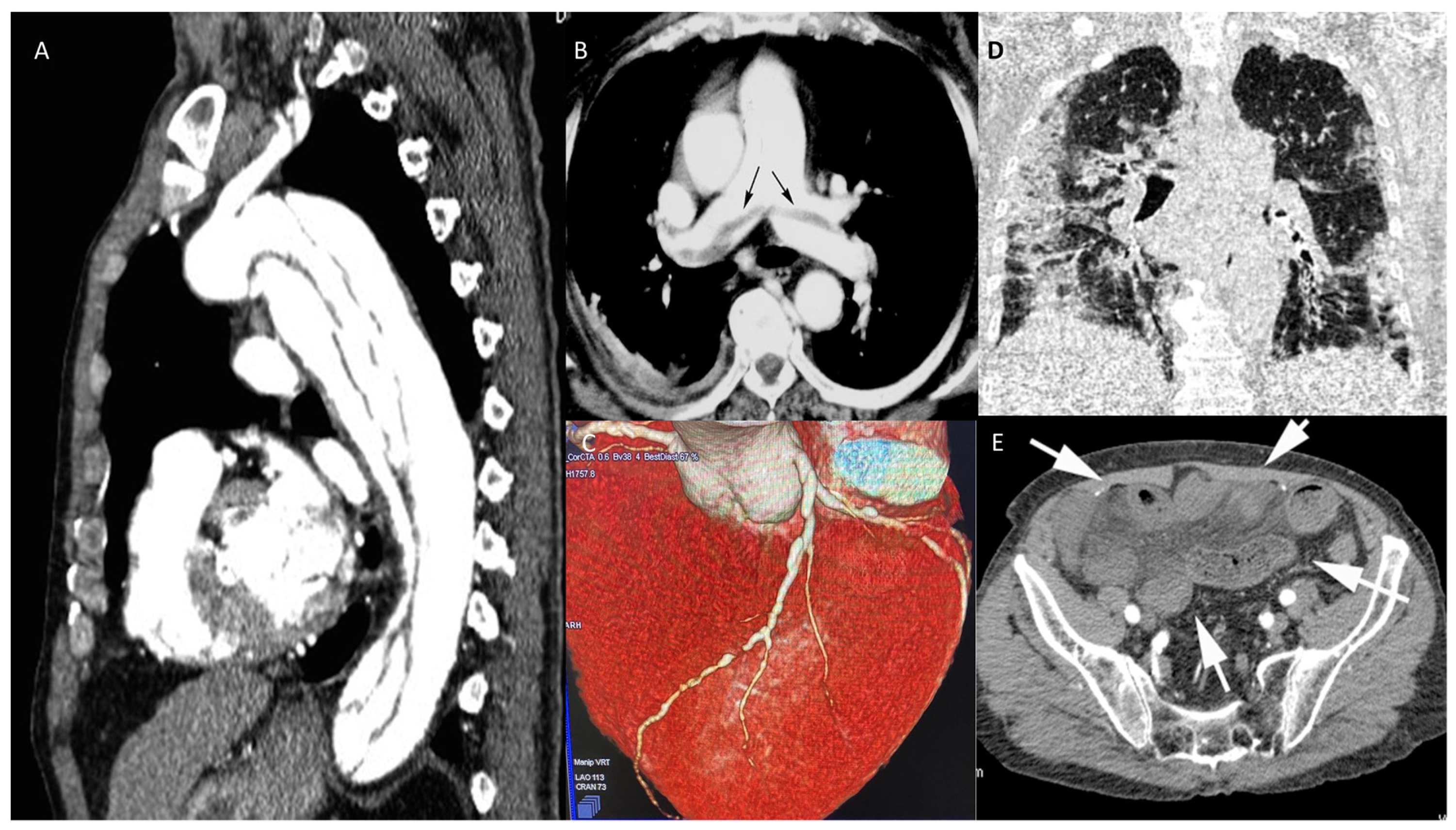
Step 3. Additional Non-Invasive and Invasive Tests
- a.
- High-resolution chest computed tomography (Chest HR-CT)
- b.
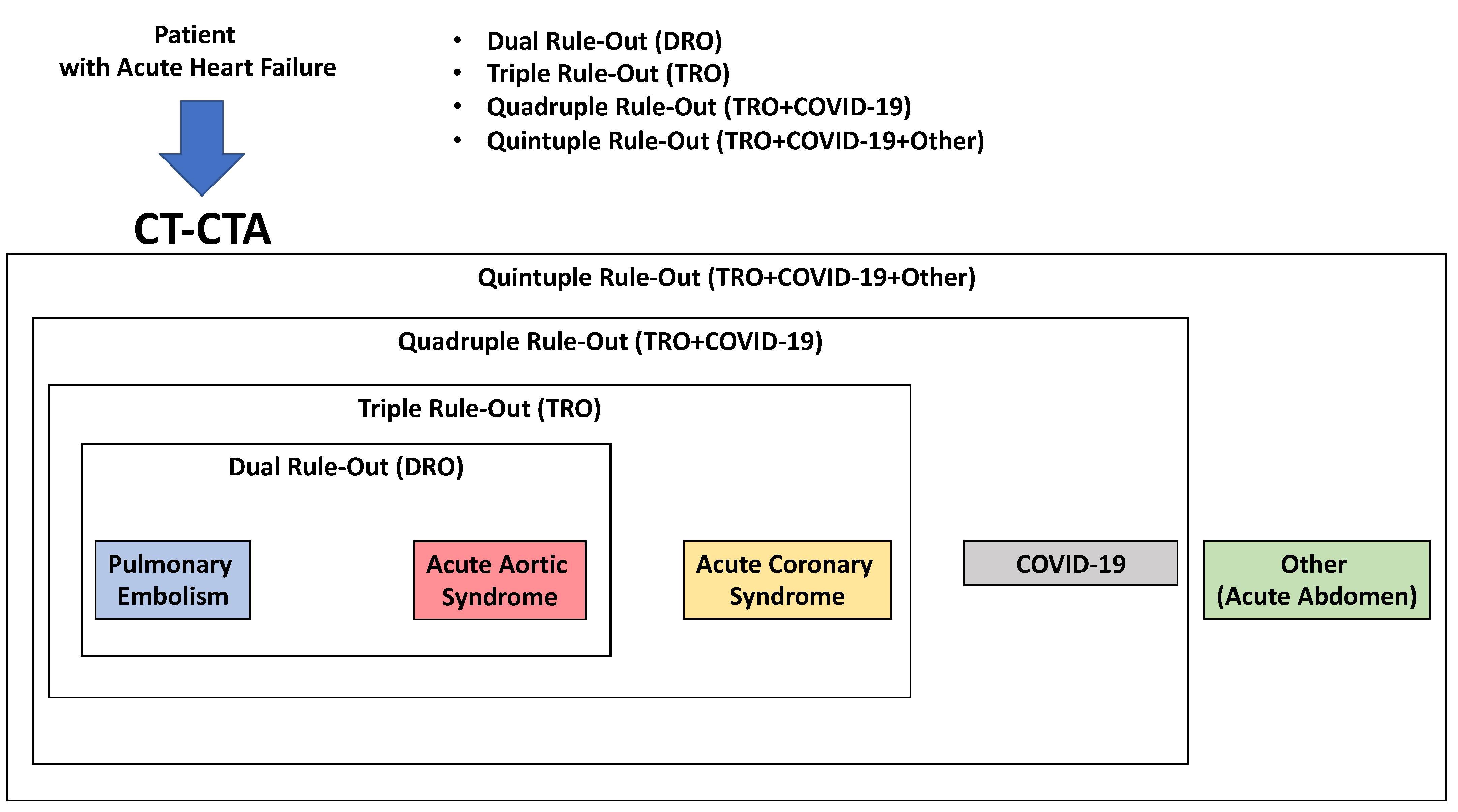
- Chest CT angiography (CTA)
- c.
- Coronary angiography
4. In-Hospital Therapeutic Interventions
4.1. Pharmacologic
4.1.1. Diuretics (Table 5)
| Drug | Mechanism of Action | Dose | Adverse Reactions | Notes |
|---|---|---|---|---|
| Diuretics | ||||
| Used in hypervolemia to relief symptoms of congestion | ||||
| Loop diuretics | ||||
| Furosemide *, Torsemide *, Bumetanide. | Sulfonamide loop diuretics. Inhibit cotransport system (Na+/K+/2Cl−) of thick ascending limb of loop of Henle. Abolish hypertonicity of medulla, preventing concentration of urine. Associated with increased PGE (vasodilatory effect on afferent arteriole). Increase Ca2+ excretion. | Initial dose, diuretic-naive:
Adjust dose to relieve symptoms, reduce volume excess, and avoid hypotension. | Ototoxicity, hypokalemia, hypomagnesemia, dehydration, allergy, metabolic alkalosis, nephritis, gout. | Monitor symptoms, urine output, renal function, and serum electrolytes regularly during therapy. Consider continuous infusion in diuretic-resistant patients. A satisfactory diuretic response can be defined as a urine sodium content >50–70 mEq/L at 2 h and/or by a urine output >100–150 mL/h during the first 6 h. |
| Thiazide diuretics | ||||
| Hydrochlorothiazide *, chlorthalidone, metolazone. | Inhibit NaCl reabsorption in early distal convolute tubule. Decrease Ca2+ excretion. |
| Hypokalemic metabolic alkalosis, hyponatremia, hyperglycemia, hyperlipidemia, hyperuricemia, hypercalcemia. Sulfa allergy. | Use with caution in patients with severe renal disease, hepatic impairment, or progressive liver disease. |
| Potassium-sparing diuretics | ||||
| Spironolactone *, Eplerenone *, Amiloride, Triamterene. | Spironolactone and eplerenone are competitive aldosterone receptor antagonists in cortical collecting tubule. Amiloride blocks Na+ channels at the same part of the tubule. |
| Hyperkalemia (can lead to arrhythmias), endocrine effects with spironolactone (e.g., gynecomastia, antiandrogen effects). | Monitor serum potassium. |
4.1.2. Vasodilators (Table 6)
| Drug | Mechanism of action | Dose | Adverse reactions | Notes |
|---|---|---|---|---|
| Vasodilators | ||||
| Used for relief of dyspnea in patients without hypotension (SBP > 110 mmHg), potentially useful in severely congested patients with hypertension or severe mitral valve regurgitation complicating LV dysfunction. | ||||
| Nitroglycerine Isosorbide dinitrate | Vasodilate by increasing NO in vascular smooth muscle that leads to increase of cGMP and smooth muscle relaxation (veins > arteries). | Nitroglycerine: start with 10–20 μg/min, increase up to 200 μg/min IV. Isosorbide dinitrate: start with 1 mg/h, increase up to 10 mg/h IV. | Hypotension, reflex tachycardia, headache. Tolerance in continuous use. | Contraindicated in right ventricular infarction, hypertrophic cardiomyopathy, severe aortic stenosis and with concurrent PDE-5 inhibitor use. |
| Nitroprusside | Short acting vasodilator (arteries = veins). Increases cGMP via direct release of NO. | Start with 0.3 μg/kg/min and increase up to 5 μg/kg/min IV. | Hypotension, isocyanate toxicity, light sensitivity. | Contraindicated in right ventricular infarction, hypertrophic cardiomyopathy, severe aortic stenosis, and with concurrent PDE-5 inhibitor use. |
4.1.3. Opiates
4.1.4. Digoxin
4.1.5. Anticoagulants
4.1.6. Inotropes/Vasopressors (Table 7)
| Drug | Mechanism of Action | Dose | Adverse Reactions | Notes |
|---|---|---|---|---|
| Inotropes/Vasopressors | ||||
| Used for maintenance of systemic perfusion and preservation of end organ function in patients with severe systolic dysfunction presenting with hypotension (<90 mmHg) or low cardiac output in the presence of congestion and organ hypoperfusion. | ||||
| Dobutamine | Agonist of both beta1- and beta2-adrenergic receptors with variable effects on the alpha receptors | Continuous IV infusion rate of 2–20 mcg/kg/minute | Hypotension, increased myocardial oxygen demand, phlebitis | Continuously monitor ECG and blood pressure. Dobutamine is preferred over milrinone in patients who are acutely unstable or hypotensive, or those with renal insufficiency. |
| Dopamine | Agonist of both adrenergic and dopaminergic receptors | Infusion rate of 3–5 μg/kg/min; inotropic (beta+); >5 μg/kg/min: (beta+), vasopressor (alpha+) | Arrhythmias, tachycardia | Continuously monitor ECG and blood pressure. Clinical effects are dose-related; low doses increase renal blood flow/urine output, intermediate doses also increase cardiac contractility and chronotropy, and high doses result in vasoconstriction. |
| Milrinone | PDE inhibitor (increases cAMP) | Bolus: 25–75 μg/kg over 10–20 min then infusion rate of 0.375–0.75 μg/kg/min continuous IV infusion. | Tachycardia, ventricular arrhythmias, hypotension | Continuously monitor ECG and blood pressure. Not recommended in acutely worsened ischemic heart failure. |
| Levosimendan | Cardiac Ca2+ channels sensitizer. Activator of K+ channels of vascular smooth muscle cells. | Optional bolus: 2 μg/kg over 10 min, infusion rate of 0.1 μg/kg/min, which can be decreased to 0.05 or increased to 0.2 μg/kg/min. | Tachycardia, ventricular arrhythmias, hypotension. | Continuously monitor ECG and blood pressure. Bolus not recommended in hypotensive patients. |
| Norepinephrine | Potent agonist of the beta1 and the alpha 1 receptors | Infusion rate of 0.2–1.0 μg/kg/min. | End-organ hypoperfusion and tissue necrosis, arrhythmias. | Continuously monitor ECG and blood pressure. |
| Epinephrine | Full beta receptor agonist | Infusion rate of 0.05–0.5 μg/kg/min. A bolus of 1 mg can be given IV during resuscitation, repeated every 3–5 min. | End-organ hypoperfusion and tissue necrosis, arrhythmias. | Continuously monitor ECG and blood pressure. Use should be restricted to patients with persistent hypotension despite adequate cardiac filling pressures and the use of other vasoactive agents, as well as for resuscitation protocols. |
4.1.7. Future Directions
4.1.8. Management of Chronic HF Therapy
4.2. Non-Pharmacologic
4.2.1. Mechanical Ventilation
- Cardiac or respiratory arrest;
- Anatomical abnormality (unable to fit the interface);
- Inability to keep patent airway (uncontrolled agitation, coma or obtunded mental status);
- Refractory hypotension.
- Cardiac or respiratory arrest;
- Progressive worsening of altered mental status;
- Progressive worsening of pH, PaCO2, or PaO2 despite NIV;
- Progressive signs of fatigue during NIV;
- Need to protect the airway;
- Persistent hemodynamic instability;
- Agitation or intolerance to NIV with progressive respiratory failure.
4.2.2. Electric Cardioversion
4.2.3. Mechanical Circulatory Support (MCS)
4.2.4. Renal Replacement Therapy
- Oliguria unresponsive to fluid resuscitation measures;
- Severe hyperkalemia (K+ > 6.5 mmol/L);
- Severe acidemia (pH < 7.2);
- Serum urea level > 25 mmol/L (> 150 mg/dL);
- Serum creatinine > 300 mmol/L (> 3.4 mg/dL) that is worsening.
5. Daily Patient Monitoring
- Weight check along with completion of an accurate fluid balance chart;
- Standard non-invasive monitoring of HR, RR, BP;
- Renal function and electrolyte measurement.
6. Pre-Discharge and Post-Discharge Planning
6.1. Pre-Discharge
- Patient-reported subjective improvement;
- Resting HR < 100 bpm
- Lack of orthostatic changes in BP;
- Adequate urine output;
- SpO2 > 95% in room air;
- Decreased body weight.
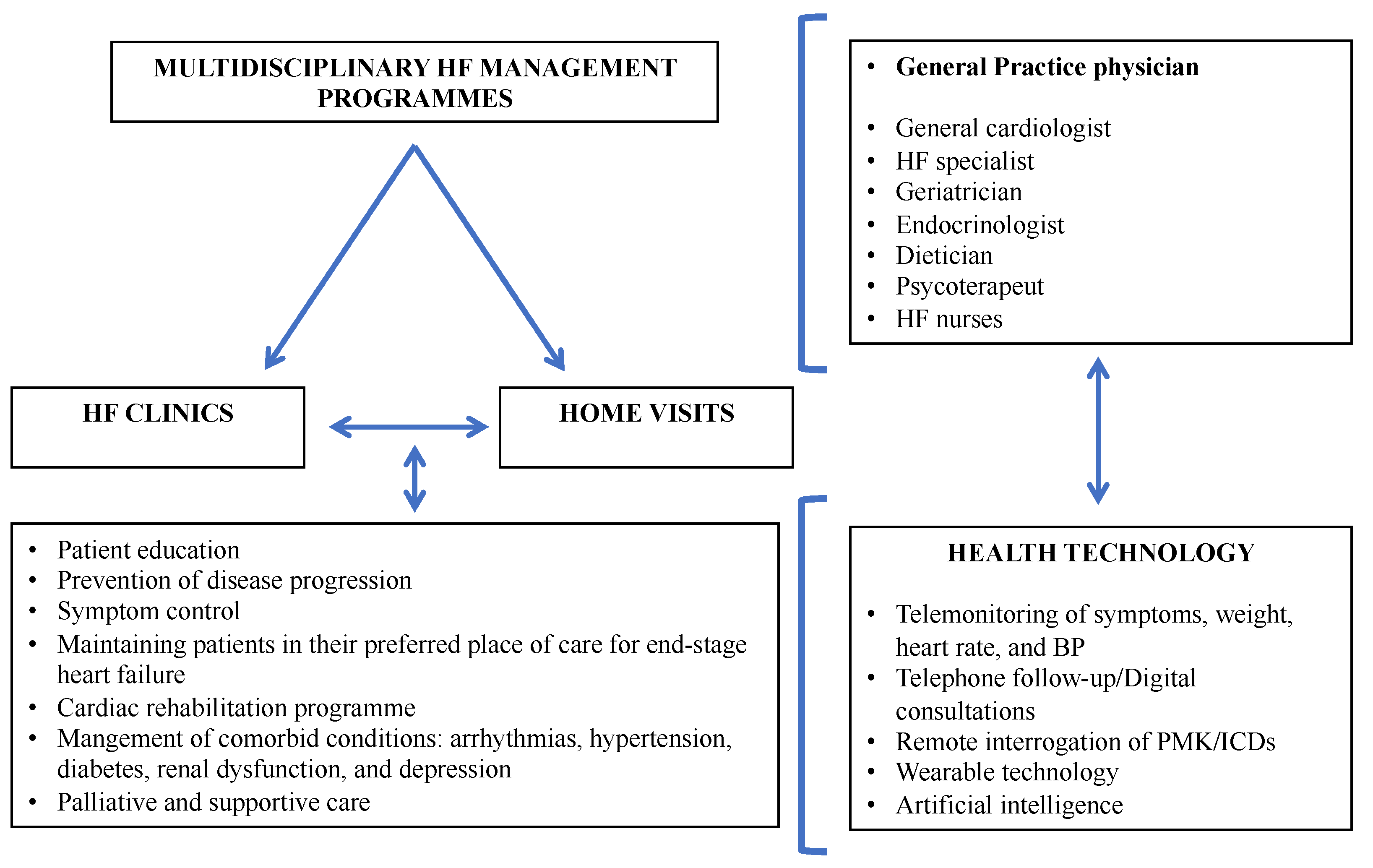
6.2. Post-Discharge (Figure 6)
- Patient self-monitoring (i.e., regular weight checks, adherence to therapy, structured exercise program, and dietary sodium and fluid restriction).
- Periodic follow-up visits, including monitoring of signs and symptoms of HF, assessment of volume status, BP, HR, and laboratory tests primarily of renal function, electrolytes, iron status, hepatic function, and NP. In patients with minimal symptoms of HF, comparison of NP level with predischarge values should be considered to detect worsening subclinical congestion. At the visit, the physician should also verify that the patient is receiving all guideline-directed chronic HF therapies for which they are eligible. Likewise, laboratory monitoring for corresponding drug adverse effects (i.e., renal insufficiency, electrolyte disturbances) should be considered [3]. Furthermore, planning for additional diagnostic and interventional procedures can be undertaken, including device therapy. It should be highlighted that the 2021 European Society of Cardiology (ESC) HF guidelines recommend the first follow-up outpatient visit within 1 to 2 weeks after discharge [83].
- Remote monitoring via telemedicine/teleconsulting evaluations. Home telemonitoring can help maintain quality of care, facilitate rapid access to care when needed, reduce patient travel costs, and minimize the frequency of clinic visits [84]. Remote pulmonary arterial pressure monitoring with implantable pressure sensors, with adjustment of diuretic therapy according to pulmonary arterial pressure measurements, substantially reduced HF hospitalizations and improved outcomes in both patients with HFpEF and HFrEF [85].

7. In-Hospital and Long-Term Outcomes
7.1. In-Hospital Outcomes
7.2. Long-Term Outcomes
8. Preventive Strategies
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Teerlink, J.R. Diagnosis and Management of Acute Heart Failure. In Braunwald’s Heart Disease a Textbook of Cardiovascular Medicine, 11th ed.; Zipes, D.P., Libby, P., Bonow, R., Mann, L.D., Tomaselli, G.F., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 462–489. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Primer 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.-P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [Green Version]
- Urbich, M.; Globe, G.; Pantiri, K.; Heisen, M.; Bennison, C.; Wirtz, H.S.; Di Tanna, G.L. A Systematic Review of Medical Costs Associated with Heart Failure in the USA (2014–2020). PharmacoEconomics 2020, 38, 1219–1236. [Google Scholar] [CrossRef]
- Farmakis, D.; Filippatos, G. Acute heart failure: Epidemiology, classification, and pathophysiology. In The ESC Textbook of Intensive and Acute Cardiovascular Care, 3rd ed.; Tubaro, M., Vranckx, P., Bonnefoy, E., Price, S., Vrints, C., Eds.; Oxford University Press: Oxford, UK, 2021; pp. 603–616. [Google Scholar]
- Di Palo, K.E.; Barone, N.J. Hypertension and Heart Failure. Heart Fail. Clin. 2020, 16, 99–106. [Google Scholar] [CrossRef]
- Kim, I.-C. Atrial Fibrillation and Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 377–386. [Google Scholar] [CrossRef]
- Pellicori, P.; Cleland, J.G.F.; Clark, A.L. Chronic Obstructive Pulmonary Disease and Heart Failure. Heart Fail. Clin. 2020, 16, 33–44. [Google Scholar] [CrossRef]
- Ananthram, M.G.; Gottlieb, S.S. Renal Dysfunction and Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2021, 17, 357–367. [Google Scholar] [CrossRef]
- Sugimoto, T. Acute Decompensated Heart Failure in Patients with Heart Failure with Preserved Ejection Fraction. Heart Fail. Clin. 2020, 16, 201–209. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Stough, W.G.; Abraham, W.T.; Albert, N.M.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B. Characteristics, Treatments, and Outcomes of Patients With Preserved Systolic Function Hospitalized for Heart Failure. J. Am. Coll. Cardiol. 2007, 50, 768–777. [Google Scholar] [CrossRef] [Green Version]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Yilmaz, M.B.; Levy, P.; Ponikowski, P.; Peacock, W.F.; Laribi, S.; Ristic, A.D.; Lambrinou, E.; Masip, J.; Riley, J.P.; et al. Recommendations on pre-hospital & early hospital management of acute heart failure: A consensus paper from the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergenc: Recommendations on pre-hospital & early hospital management of acute heart failure. Eur. J. Heart Fail. 2015, 17, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Masip, J.; Gayà, M.; Páez, J.; Betbesé, A.; Vecilla, F.; Manresa, R.; Ruíz, P. Pulsioximetría en el diagnóstico de insuficiencia cardiaca aguda. Rev. Esp. Cardiol. 2012, 65, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, C.-L. Meta-analysis: Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema. Ann. Intern. Med. 2010, 152, 590. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Rev. Esp. Cardiol. Engl. Ed. 2021, 74, 544. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adultThe Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [CrossRef] [Green Version]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Jobs, A.; Simon, R.; de Waha, S.; Rogacev, K.; Katalinic, A.; Babaev, V.; Thiele, H. Pneumonia and inflammation in acute decompensated heart failure: A registry-based analysis of 1939 patients. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Leung, A.M. Thyroid Emergencies. J. Infus. Nurs. 2016, 39, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Sirbu, O. Anemia in heart failure—From guidelines to controversies and challenges. Anatol. J. Cardiol. 2018, 20, 52. [Google Scholar] [CrossRef]
- Rosano, G.; Jankowska, E.A.; Ray, R.; Metra, M.; Abdelhamid, M.; Adamopoulos, S.; Anker, S.D.; Bayes-Genis, A.; Belenkov, Y.; Ben Gal, T.; et al. COVID-19 vaccination in patients with heart failure: A position paper of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 1806–1818. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; de la Espriella, R.; Rossignol, P.; Voors, A.A.; Mullens, W.; Metra, M.; Chioncel, O.; Januzzi, J.L.; Mueller, C.; Richards, A.M.; et al. Congestion in heart failure: A circulating biomarker-based perspective. A review from the Biomarkers Working Group of the Heart Failure Association, European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 1751–1766. [Google Scholar] [CrossRef] [PubMed]
- Salzano, A.; D’Assante, R.; Israr, M.Z.; Eltayeb, M.; D’Agostino, A.; Bernieh, D.; De Luca, M.; Rega, S.; Ranieri, B.; Mauro, C.; et al. Biomarkers in Heart Failure. Heart Fail. Clin. 2021, 17, 223–243. [Google Scholar] [CrossRef]
- Mueller, C.; McDonald, K.; de Boer, R.A.; Maisel, A.; Cleland, J.G.F.; Kozhuharov, N.; Coats, A.J.S.; Metra, M.; Mebazaa, A.; Ruschitzka, F.; et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur. J. Heart Fail. 2019, 21, 715–731. [Google Scholar] [CrossRef] [Green Version]
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized With Heart Failure. J. Am. Coll. Cardiol. 2019, 74, 1966–2011. [Google Scholar] [CrossRef]
- Harjola, V.-P.; Mullens, W.; Banaszewski, M.; Bauersachs, J.; Brunner-La Rocca, H.-P.; Chioncel, O.; Collins, S.P.; Doehner, W.; Filippatos, G.S.; Flammer, A.J.; et al. Organ dysfunction, injury and failure in acute heart failure: From pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC): Organ dysfunction and failure in AHF. Eur. J. Heart Fail. 2017, 19, 821–836. [Google Scholar] [CrossRef] [Green Version]
- Via, G.; Hussain, A.; Wells, M.; Reardon, R.; ElBarbary, M.; Noble, V.E.; Tsung, J.W.; Neskovic, A.N.; Price, S.; Oren-Grinberg, A.; et al. International Evidence-Based Recommendations for Focused Cardiac Ultrasound. J. Am. Soc. Echocardiogr. 2014, 27, 683.e1–683.e33. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Gargani, L. Ultrasound of the Lungs. Heart Fail. Clin. 2019, 15, 297–303. [Google Scholar] [CrossRef]
- Picano, E.; Scali, M.C.; Ciampi, Q.; Lichtenstein, D. Lung Ultrasound for the Cardiologist. JACC Cardiovasc. Imaging 2018, 11, 1692–1705. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A.; Mezière, G.A. Relevance of Lung Ultrasound in the Diagnosis of Acute Respiratory Failure*: The BLUE Protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure: Prognostic value of B-lines after discharge from HF hospitalisation. Eur. J. Heart Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Pellicori, P.; Platz, E.; Dauw, J.; Maaten, J.M.; Martens, P.; Pivetta, E.; Cleland, J.G.F.; McMurray, J.J.V.; Mullens, W.; Solomon, S.D.; et al. Ultrasound imaging of congestion in heart failure: Examinations beyond the heart. Eur. J. Heart Fail. 2021, 23, 703–712. [Google Scholar] [CrossRef]
- Iida, N.; Seo, Y.; Sai, S.; Machino-Ohtsuka, T.; Yamamoto, M.; Ishizu, T.; Kawakami, Y.; Aonuma, K. Clinical Implications of Intrarenal Hemodynamic Evaluation by Doppler Ultrasonography in Heart Failure. JACC Heart Fail. 2016, 4, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, M.D.; Lui, G.K.; Miller-Hance, W.C.; Brook, M.M.; Young, L.T.; Bhat, A.; Roberson, D.A.; Mercer-Rosa, L.; Miller, O.I.; Parra, D.A.; et al. Guidelines for Performing a Comprehensive Transesophageal Echocardiographic. J. Am. Soc. Echocardiogr. 2019, 32, 173–215. [Google Scholar] [CrossRef]
- Suciadi, L.P.; William, Y.; Jorizal, P.; Tarigan, V.N.; Santoso, A.H.; Henrina, J.; Tedjasukmana, F.; Kristanti, N.M. Comparing Lung CT in COVID-19 Pneumonia and Acute Heart Failure: An Imaging Conundrum. Cureus 2021, 13, e15120. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangalat, D.; Kalogeropoulos, A.; Georgiopoulou, V.; Stillman, A.; Butler, J. Value of cardiac CT in patients with heart failure. Curr. Cardiovasc. Imaging Rep. 2009, 2, 410–417. [Google Scholar] [CrossRef] [Green Version]
- Pontone, G.; Baggiano, A.; Conte, E.; Teruzzi, G.; Cosentino, N.; Campodonico, J.; Rabbat, M.G.; Assanelli, E.; Palmisano, A.; Esposito, A.; et al. “Quadruple Rule-Out” With Computed Tomography in a COVID-19 Patient With Equivocal Acute Coronary Syndrome Presentation. JACC Cardiovasc. Imaging 2020, 13, 1854–1856. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreucci, M.; Solomon, R.; Tasanarong, A. Side Effects of Radiographic Contrast Media: Pathogenesis, Risk Factors, and Prevention. BioMed Res. Int. 2014, 2014, 741018. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Ellison, D.H.; Mullens, W.; Cox, Z.L.; Testani, J.M. Diuretic Therapy for Patients With Heart Failure. J. Am. Coll. Cardiol. 2020, 75, 1178–1195. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Damman, K.; Harjola, V.-P.; Mebazaa, A.; Brunner-La Rocca, H.-P.; Martens, P.; Testani, J.M.; Tang, W.H.W.; Orso, F.; Rossignol, P.; et al. The use of diuretics in heart failure with congestion—A position statement from the Heart Failure Association of the European Society of Cardiology: Diuretics in heart failure. Eur. J. Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef] [Green Version]
- Carlson, M.D.; Eckman, P.M. Review of Vasodilators in Acute Decompensated Heart Failure: The Old and the New. J. Card. Fail. 2013, 19, 478–493. [Google Scholar] [CrossRef]
- Peacock, W.F.; Hollander, J.E.; Diercks, D.B.; Lopatin, M.; Fonarow, G.; Emerman, C.L. Morphine and outcomes in acute decompensated heart failure: An ADHERE analysis. Emerg. Med. J. 2008, 25, 205–209. [Google Scholar] [CrossRef]
- Sethi, N.J.; Nielsen, E.E.; Safi, S.; Feinberg, J.; Gluud, C.; Jakobsen, J.C. Digoxin for atrial fibrillation and atrial flutter: A systematic review with meta-analysis and trial sequential analysis of randomised clinical trials. PLoS ONE 2018, 13, e0193924. [Google Scholar] [CrossRef]
- Uretsky, B.F.; Young, J.B.; Shahidi, F.E.; Yellen, L.G.; Harrison, M.C.; Jolly, M.K. Randomized study assessing the effect of digoxin withdrawal in patients with mild to moderate chronic congestive heart failure: Results of the PROVED trial. J. Am. Coll. Cardiol. 1993, 22, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Tebbe, U.; Schellong, S.M.; Haas, S.; Gerlach, H.E.; Abletshauser, C.; Sieder, C.; Bramlage, P.; Riess, H. Certoparin versus unfractionated heparin to prevent venous thromboembolic events in patients hospitalized because of heart failure: A subgroup analysis of the randomized, controlled CERTIFY study. Am. Heart J. 2011, 161, 322–328. [Google Scholar] [CrossRef]
- Francis, G.S.; Bartos, J.A.; Adatya, S. Inotropes. J. Am. Coll. Cardiol. 2014, 63, 2069–2078. [Google Scholar] [CrossRef]
- Masarone, D.; Melillo, E.; Gravino, R.; Errigo, V.; Martucci, M.L.; Caiazzo, A.; Petraio, A.; Pölzl, G.; Pacileo, G. Inotropes in Patients with Advanced Heart Failure. Heart Fail. Clin. 2021, 17, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Parissis, J.; Porcher, R.; Gayat, E.; Nikolaou, M.; Boas, F.V.; Delgado, J.F.; Follath, F. Short-term survival by treatment among patients hospitalized with acute heart failure: The global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2011, 37, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Biegus, J.; Voors, A.A.; Collins, S.P.; Kosiborod, M.N.; Teerlink, J.R.; Angermann, C.E.; Tromp, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; et al. Impact of empagliflozin on decongestion in acute heart failure: The EMPULSE trial. Eur. Heart J. 2023, 44, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Voors, A.A.; Angermann, C.E.; Teerlink, J.R.; Collins, S.P.; Kosiborod, M.; Biegus, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; Tromp, J.; et al. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: A multinational randomized trial. Nat. Med. 2022, 28, 568–574. [Google Scholar] [CrossRef]
- Mullens, W.; Dauw, J.; Martens, P.; Verbrugge, F.H.; Nijst, P.; Meekers, E.; Tartaglia, K.; Chenot, F.; Moubayed, S.; Dierckx, R.; et al. Acetazolamide in Acute Decompensated Heart Failure with Volume Overload. N. Engl. J. Med. 2022, 387, 1185–1195. [Google Scholar] [CrossRef]
- Racioppi, M.F.; Burgos, J.I.; Morell, M.; Gonano, L.A.; Vila Petroff, M. Cellular Mechanisms Underlying the Low Cardiotoxicity of Istaroxime. J. Am. Heart Assoc. 2021, 10, e018833. [Google Scholar] [CrossRef]
- Torre, E.; Arici, M.; Lodrini, A.M.; Ferrandi, M.; Barassi, P.; Hsu, S.-C.; Chang, G.-J.; Boz, E.; Sala, E.; Vagni, S.; et al. SERCA2a stimulation by istaroxime improves intracellular Ca2+ handling and diastolic dysfunction in a model of diabetic cardiomyopathy. Cardiovasc. Res. 2022, 118, 1020–1032. [Google Scholar] [CrossRef]
- Carubelli, V.; Zhang, Y.; Metra, M.; Lombardi, C.; Felker, G.M.; Filippatos, G.; O’Connor, C.M.; Teerlink, J.R.; Simmons, P.; Segal, R.; et al. Treatment with 24 hour istaroxime infusion in patients hospitalised for acute heart failure: A randomised, placebo-controlled trial. Eur. J. Heart Fail. 2020, 22, 1684–1693. [Google Scholar] [CrossRef]
- Metra, M.; Chioncel, O.; Cotter, G.; Davison, B.; Filippatos, G.; Mebazaa, A.; Novosadova, M.; Ponikowski, P.; Simmons, P.; Soffer, J.; et al. Safety and efficacy of istaroxime in patients with acute heart failure-related pre-cardiogenic shock—A multicentre, randomized, double-blind, placebo-controlled, parallel group study ( SEISMiC ). Eur. J. Heart Fail. 2022, 24, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Davison, B.A.; Cotter, G.; Maggioni, A.P.; Sato, N.; Chioncel, O.; Ertl, G.; Felker, G.M.; Filippatos, G.; Greenberg, B.H.; et al. Effects of serelaxin in patients admitted for acute heart failure: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 315–329. [Google Scholar] [CrossRef]
- Teerlink, J.; Alburikan, K.; Metra, M.; Rodgers, J. Acute Decompensated Heart Failure Update. Curr. Cardiol. Rev. 2014, 11, 53–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattis, W.A.; O’Connor, C.M. Predischarge initiation of carvedilol in patients hospitalized for decompensated heart failure. Am. J. Cardiol. 2004, 93, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Masip, J.; Peacock, W.F.; Price, S.; Cullen, L.; Martin-Sanchez, F.J.; Seferovic, P.; Maisel, A.S.; Miro, O.; Filippatos, G.; Vrints, C.; et al. Indications and practical approach to non-invasive ventilation in acute heart failure. Eur. Heart J. 2018, 39, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, T.M.; Ohman, E.M.; O’Neill, W.W.; Rab, T.; Cigarroa, J.E. A Practical Approach to Mechanical Circulatory Support in Patients Undergoing Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2016, 9, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Schocken, D.D.; Benjamin, E.J.; Fonarow, G.C.; Krumholz, H.M.; Levy, D.; Mensah, G.A.; Narula, J.; Shor, E.S.; Young, J.B.; Hong, Y. Prevention of Heart Failure: A Scientific Statement From the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation 2008, 117, 2544–2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachter, R.; Senni, M.; Belohlavek, J.; Straburzynska-Migaj, E.; Witte, K.K.; Kobalava, Z.; Fonseca, C.; Goncalvesova, E.; Cavusoglu, Y.; Fernandez, A.; et al. Initiation of sacubitril/valsartan in haemodynamically stabilised heart failure patients in hospital or early after discharge: Primary results of the randomised TRANSITION study. Eur. J. Heart Fail. 2019, 21, 998–1007. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, E.J.; Morrow, D.A.; DeVore, A.D.; Duffy, C.I.; Ambrosy, A.P.; McCague, K.; Rocha, R.; Braunwald, E. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. N. Engl. J. Med. 2019, 380, 539–548. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Dixit, N.M.; Ziaeian, B.; Fonarow, G.C. SGLT2 Inhibitors in Heart Failure. Heart Fail. Clin. 2022, 18, 587–596. [Google Scholar] [CrossRef]
- Greene, S.J.; Fonarow, G.C.; Vaduganathan, M.; Khan, S.S.; Butler, J.; Gheorghiade, M. The vulnerable phase after hospitalization for heart failure. Nat. Rev. Cardiol. 2015, 12, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Bossone, E.; Mauro, C.; Maiellaro, A.; Raiola, E.; Cocchia, R.; Ranieri, B.; Sepe, C.; Capone, V.; Chianese, S.; Maramaldi, R.; et al. Cardiac teleconsulting in the time of COVID-19 global pandemic: The “Antonio Cardarelli” Hospital project. Monaldi Arch. Chest Dis. 2021, 91, 1779. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Chioncel, O.; Mebazaa, A.; Harjola, V.-P.; Coats, A.J.; Piepoli, M.F.; Crespo-Leiro, M.G.; Laroche, C.; Seferovic, P.M.; Anker, S.D.; Ferrari, R.; et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: The ESC Heart Failure Long-Term Registry: Outcome of patients hospitalized for acute heart failure. Eur. J. Heart Fail. 2017, 19, 1242–1254. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.M.; Miller, A.B.; Blair, J.E.A.; Konstam, M.A.; Wedge, P.; Bahit, M.C.; Carson, P.; Haass, M.; Hauptman, P.J.; Metra, M.; et al. Causes of death and rehospitalization in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction: Results from efficacy of vasopressin antagonism in heart failure outcome study with tolvaptan (EVEREST) program. Am. Heart J. 2010, 159, 841–849. [Google Scholar] [CrossRef]
- Lund, L.H.; Edwards, L.B.; Dipchand, A.I.; Goldfarb, S.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Yusen, R.D.; Stehlik, J. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Heart Transplantation Report—2016; Focus Theme: Primary Diagnostic Indications for Transplant. J. Heart Lung Transplant. 2016, 35, 1158–1169. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Adamo, M.; Barison, A.; Bestetti, R.B.; Biegus, J.; Böhm, M.; Butler, J.; Carapetis, J.; Ceconi, C.; Chioncel, O.; et al. Preventing heart failure: A position paper of the Heart Failure Association in collaboration with the European Association of Preventive Cardiology. Eur. J. Heart Fail. 2022, 24, 143–168. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- McDonagh, T.; Damy, T.; Doehner, W.; Lam, C.S.P.; Sindone, A.; van der Meer, P.; Cohen-Solal, A.; Kindermann, I.; Manito, N.; Pfister, O.; et al. Screening, diagnosis and treatment of iron deficiency in chronic heart failure: Putting the 2016 European Society of Cardiology heart failure guidelines into clinical practice. Eur. J. Heart Fail. 2018, 20, 1664–1672. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Coats, A.J.S.; Zheng, Z.; Adamo, M.; Ambrosio, G.; Anker, S.D.; Butler, J.; Xu, D.; Mao, J.; Khan, M.S.; et al. Management of heart failure patients with COVID-19: A joint position paper of the Chinese Heart Failure Association & National Heart Failure Committee and the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 941–956. [Google Scholar] [CrossRef]




| Acutely Decompensated Heart Failure | Acute Pulmonary Oedema | Isolated Right Ventricular Failure | Cardiogenic Shock | |
|---|---|---|---|---|
| Description | Progressive fluid retention in patients with history of HF | Lung congestion and acute respiratory failure | RV dysfunction and/or pre-capillary pulmonary hypertension | Severe cardiac dysfunction with marked hypotension (SBP < 90 mmHg) despite adequate LV filling pressure |
| Onset | Gradual (days) | Rapid (hours) | Gradual/rapid | Gradual/rapid |
| Main clinical presentation | Wet and warm (rarely wet and cold) | Wet and warm (rarely wet and cold) | Wet and cold | Wet and cold |
| Heart rate | ↑ | ↑ | Usually ↓ | ↑ |
| SBP | Variable | Variable | ↓ | ↓ |
| Cardiac index | Variable | Variable | ↓ | ↓ |
| Hypoperfusion | +/− | +/− | + | + |
| PCWP | ↑↑ | ↑↑↑ | ↓ | ↑↑ |
| Main treatment | Diuretics Inotropic agents/vasopressors (If peripheral hypoperfusion/hypotension) Short-term MCS or RRT if needed | O2 (CPAP/NIV) Diuretics Vasodilators Inotropic agents/vasopressors (If peripheral hypoperfusion/hypotension) Short-term MCS or RRT if needed | Diuretics for congestion Inotropic agents/vasopressors (If peripheral hypoperfusion/hypotension) Short-term MCS or RRT if needed | Inotropic agents/vasopressors Short-term MCS or RRT if needed |
| GFR ≥ 60 mL/min |
|---|
| Extremely low risk for CIN: specific prophylaxis or follow up not required |
| GFR < 60 mL/min (Moderate–Severe Kidney Disease) |
|
| Reaction Severity | Symptoms | Recommendation |
|---|---|---|
| Mild | Limited urticaria, pruritus, or skin edema; mild nasopharyngeal symptoms such as sneezing, rhinorrhea, or nasal congestion | Do not require premedication |
| Moderate | Generalized erythema, urticaria, pruritus, or edema Hoarseness or throat tightness with or without mild hypoxia; wheezing with mild hypoxia | Premedication is recommended Prednisone—50 mg by mouth at 13 h, 7 h, and 1 h before contrast media injection OR Methylprednisolone—32 mg by mouth 12 h and 2 h before contrast media injection PLUS Diphenhydramine—50 mg intravenously, intramuscularly, or by mouth 1 h before contrast medium |
| Severe | Severe edema, including facial and laryngeal edema, anaphylaxis, hypoxia | Consider alternative tests. If the test is necessary premedication is recommended Prednisone—50 mg by mouth at 13 h, 7 h, and 1 h before contrast media injection OR Methylprednisolone—32 mg by mouth 12 h and 2 h before contrast media injection PLUS Diphenhydramine—50 mg intravenously, intramuscularly, or by mouth 1 h before contrast medium |
| IABP | Impella (2.5, CP, 5.0) | TandemHeart | VA-ECMO | |
|---|---|---|---|---|
| Mechanism | Diastolic augmentation of aortic pressure and improved LV performance via systolic balloon deflation (decrease in afterload) | Expels blood from LV to AO | Aspirates oxygenated blood from LA and returns to iliac artery | Drainage of deoxygenated venous blood via an extracorporeal centrifugal pump over a membrane oxygenator, and pumping back oxygenated blood to iliac artery |
| Indications | Consider in patients with cardiogenic shock refractory to medical therapy | Consider in patients with cardiogenic shock refractory to medical therapy | Consider in patients with cardiogenic shock refractory to medical therapy | Consider in patients with cardiogenic shock coupled with respiratory failure refractory to medical therapy |
| Insertion | Femoral or axillary artery to aorta | Access through femoral artery placed from LV to aorta |
|
|
| Sheath size | 7–8 Fr | 13–14 Fr (2.5, CP)21 Fr (Impella 5) | 15–17 Fr Arterial 21 Fr Venous | 14–16 Fr Arterial 18–21 Fr Venous |
| Cardiac Flow | 0.3–0.5 L/min | 1–5 L/min | 2.5–5 L/min | 3–7 L/min |
| Duration | Weeks | 7 days | 14 days | Weeks |
| Cardiac synchrony/stable rhythm | Yes | No | No | No |
| Preload | --- | ↓↓ | ↓↓ | ↓ |
| Afterload | ↓ | ↓ | ↑ | ↑↑↑ |
| MAP | ↑ | ↑↑ | ↑↑ | ↑↑ |
| PCWP/LVEDP | ↓ | ↓↓ | ↓↓ | --- |
| Coronary perfusion | ↑ | ↑ | --- | --- |
| Complications |
|
|
|
|
| Contraindications |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauro, C.; Chianese, S.; Cocchia, R.; Arcopinto, M.; Auciello, S.; Capone, V.; Carafa, M.; Carbone, A.; Caruso, G.; Castaldo, R.; et al. Acute Heart Failure: Diagnostic–Therapeutic Pathways and Preventive Strategies—A Real-World Clinician’s Guide. J. Clin. Med. 2023, 12, 846. https://doi.org/10.3390/jcm12030846
Mauro C, Chianese S, Cocchia R, Arcopinto M, Auciello S, Capone V, Carafa M, Carbone A, Caruso G, Castaldo R, et al. Acute Heart Failure: Diagnostic–Therapeutic Pathways and Preventive Strategies—A Real-World Clinician’s Guide. Journal of Clinical Medicine. 2023; 12(3):846. https://doi.org/10.3390/jcm12030846
Chicago/Turabian StyleMauro, Ciro, Salvatore Chianese, Rosangela Cocchia, Michele Arcopinto, Stefania Auciello, Valentina Capone, Mariano Carafa, Andreina Carbone, Giuseppe Caruso, Rossana Castaldo, and et al. 2023. "Acute Heart Failure: Diagnostic–Therapeutic Pathways and Preventive Strategies—A Real-World Clinician’s Guide" Journal of Clinical Medicine 12, no. 3: 846. https://doi.org/10.3390/jcm12030846