
Effect of Left Atrial Pulmonary Vein Angiography on Safety and Efficacy for High-Power, Short-Duration Pulmonary Vein Isolation in Patients with Atrial Fibrillation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ablation Procedure
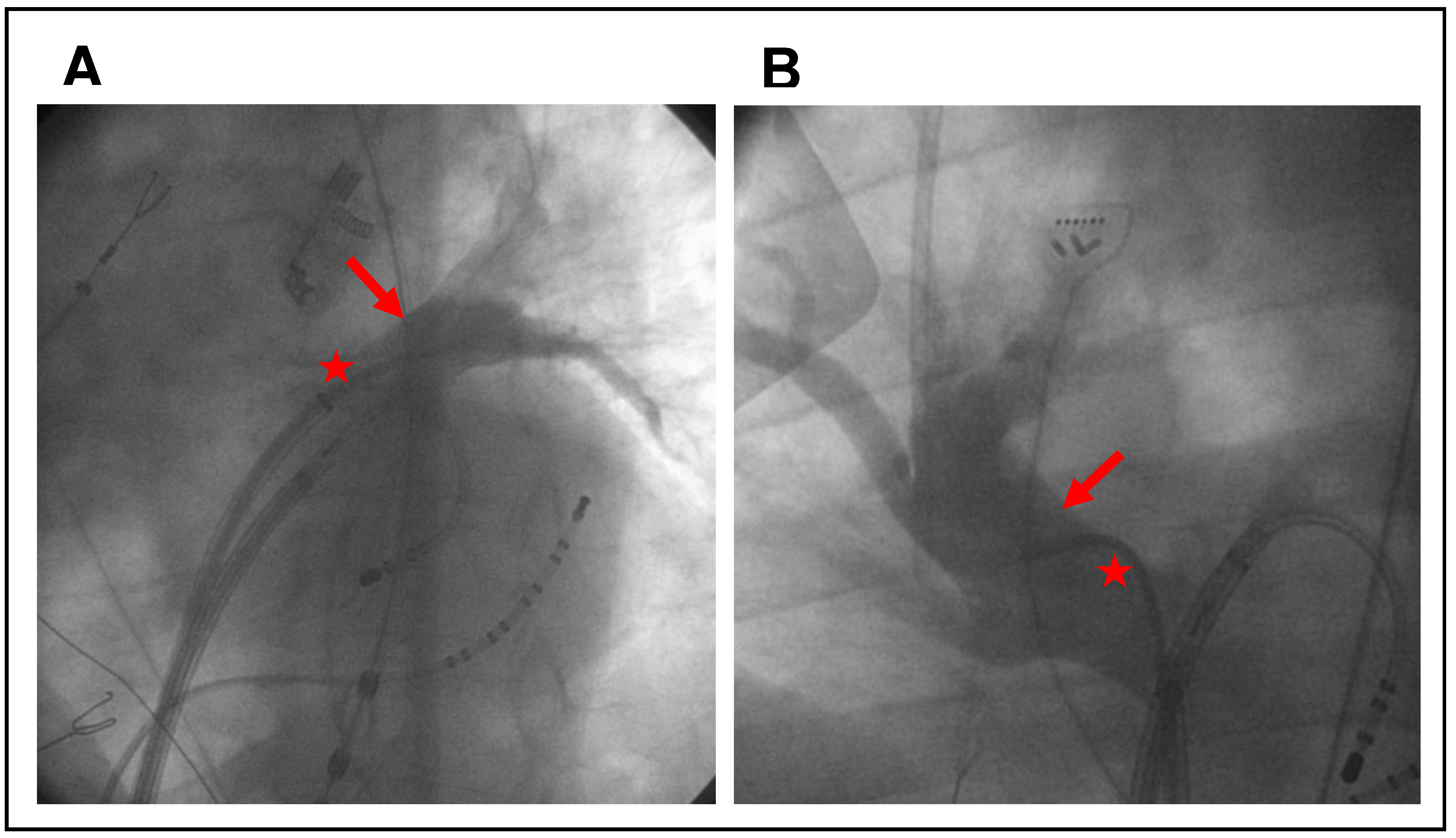
2.2. Pulmonary Vein Angiography
2.3. Follow-Up
2.4. Endpoint
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
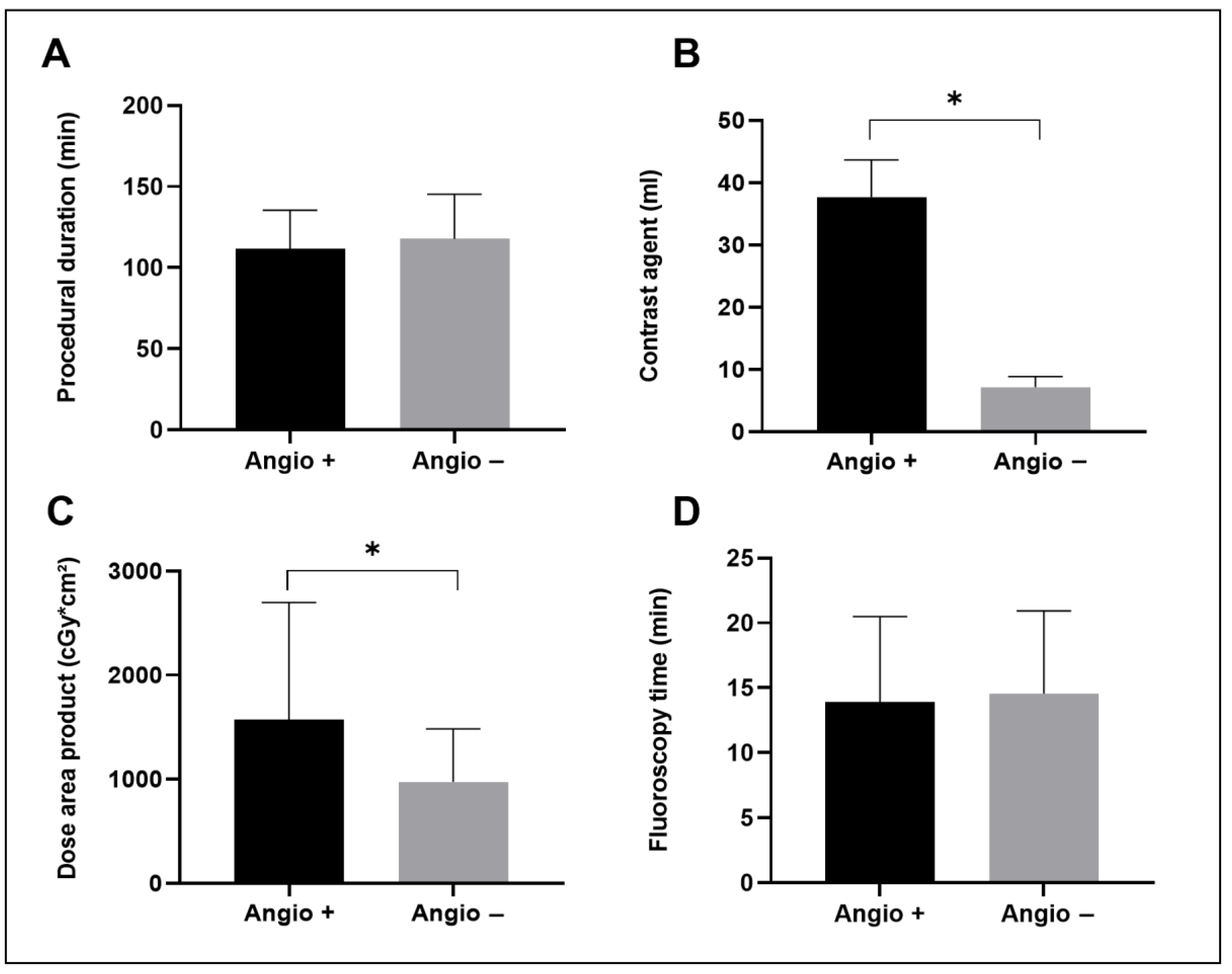
3.2. Procedural Data
3.3. Complications
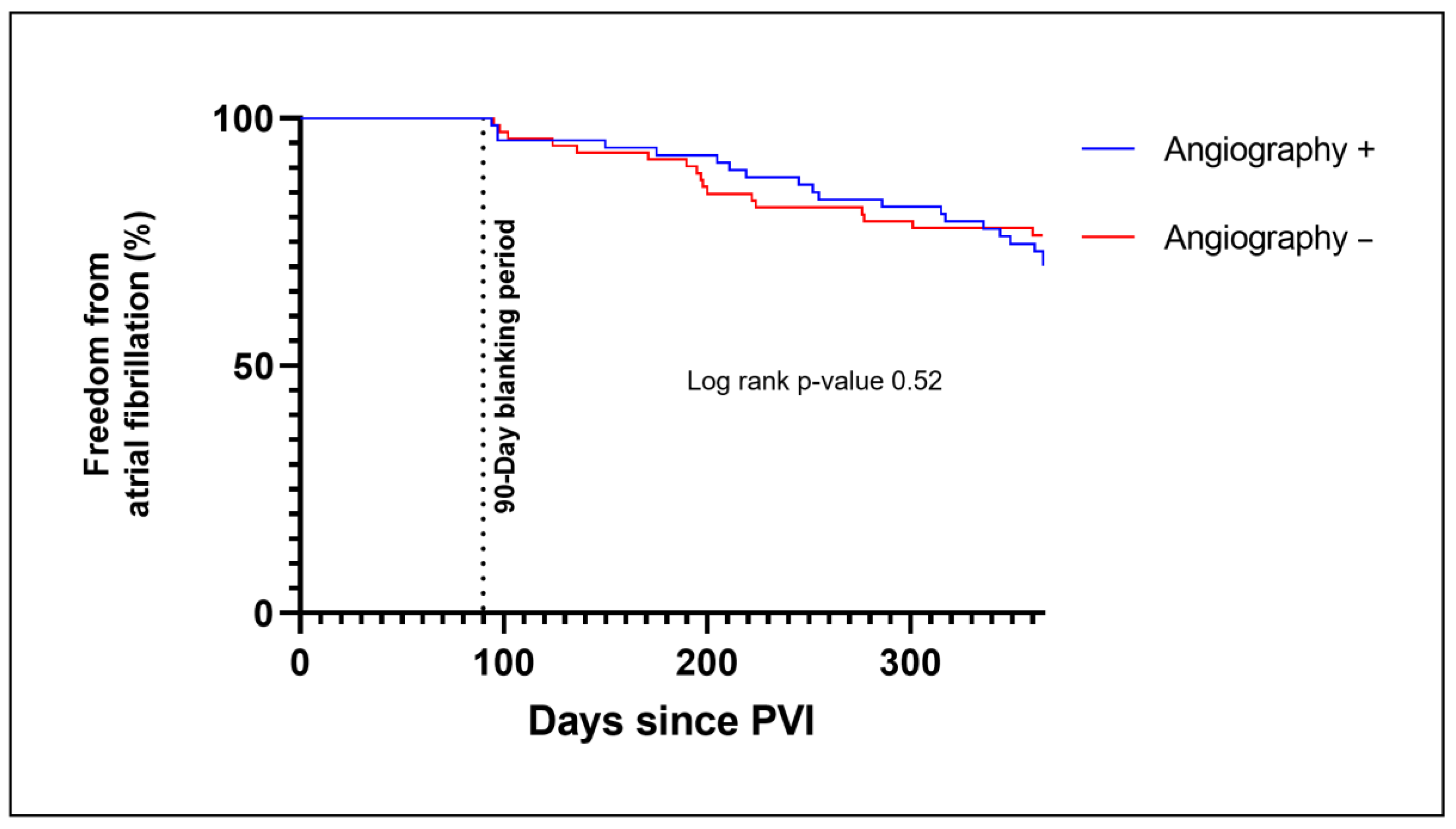
3.4. Clinical Outcome
4. Discussion
4.1. Procedural Data
4.2. Complications
4.3. Clinical Outcome
4.4. Other Forms of Preprocedural PV Imaging
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The clinical profile and pathophysiology of atrial fibrillation: Relationships among clinical features, epidemiology, and mechanisms. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.B.; Anstrom, K.J.; Sheng, S.; Piccini, J.P.; Baloch, K.N.; Monahan, K.H.; Daniels, M.R.; Bahnson, T.D.; Poole, J.E.; Rosenberg, Y.; et al. Effect of Catheter Ablation vs Medical Therapy on Quality of Life Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1275–1285. [Google Scholar] [CrossRef]
- Jaïs, P.; Cauchemez, B.; Macle, L.; Daoud, E.; Khairy, P.; Subbiah, R.; Hocini, M.; Extramiana, F.; Sacher, F.; Bordachar, P.; et al. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: The A4 study. Circulation 2008, 118, 2498–2505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Lu, J.; Lin, J.; Feng, T.; Suo, N.; Zheng, L.; Liu, Z.; Chen, G.; Fan, X.; Zhang, S.; et al. Efficiency, Safety, and Efficacy of High-Power Short-Duration Radiofrequency Ablation in Patients with Atrial Fibrillation. Cardiol. Res. Pract. 2021, 2021, 8821467. [Google Scholar] [CrossRef] [PubMed]
- Seitz, J.; Bars, C.; Théodore, G.; Beurtheret, S.; Lellouche, N.; Bremondy, M.; Ferracci, A.; Faure, J.; Penaranda, G.; Yamazaki, M.; et al. AF Ablation Guided by Spatiotemporal Electrogram Dispersion Without Pulmonary Vein Isolation: A Wholly Patient-Tailored Approach. J. Am. Coll. Cardiol. 2017, 69, 303–321. [Google Scholar] [CrossRef]
- Vasamreddy, C.R.; Jayam, V.; Lickfett, L.; Nasir, K.; Bradley, D.J.; Eldadah, Z.; Dickfeld, T.; Donahue, K.; Halperin, H.S.; Berger, R.; et al. Technique and results of pulmonary vein angiography in patients undergoing catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2004, 15, 21–26. [Google Scholar] [CrossRef]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.-H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018, 20, e1–e160. [Google Scholar] [CrossRef]
- Sagone, A.; Iacopino, S.; Pieragnoli, P.; Arena, G.; Verlato, R.; Molon, G.; Rovaris, G.; Curnis, A.; Rauhe, W.; Lunati, M.; et al. Cryoballoon ablation of atrial fibrillation is effectively feasible without previous imaging of pulmonary vein anatomy: Insights from the 1STOP project. J. Interv. Card. Electrophysiol. 2019, 55, 267–275. [Google Scholar] [CrossRef]
- Weyand, S.; Beuter, M.; Heinzmann, D.; Seizer, P. High-Resolution mapping as an alternative for exit block testing in the presence of entrance block after high-power short-duration pulmonary vein isolation. Herzschrittmacherther. Elektrophysiol. 2022, 33, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Choi, A.D.; Kamath, G.S.; Raiszadeh, F.; Marrero, D.; Badheka, A.; Mittal, S.; Steinberg, J.S. Prevalence, predictors, and prognosis of atrial fibrillation early after pulmonary vein isolation: Findings from 3 months of continuous automatic ECG loop recordings. J. Cardiovasc. Electrophysiol. 2009, 20, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Yang, Y.; Zhang, D.; Jiang, W. Meta-analysis of high power short duration in atrial fibrillation ablation—A superior efficient ablation strategy. Acta Cardiol. 2022, 77, 14–32. [Google Scholar] [CrossRef]
- Liu, X.; Gui, C.; Wen, W.; He, Y.; Dai, W.; Zhong, G. Safety and Efficacy of High Power Shorter Duration Ablation Guided by Ablation Index or Lesion Size Index in Atrial Fibrillation Ablation: A Systematic Review and Meta-Analysis. J. Interv. Cardiol. 2021, 2021, 5591590. [Google Scholar] [CrossRef] [PubMed]
- Chun, K.R.J.; Perrotta, L.; Bordignon, S.; Khalil, J.; Dugo, D.; Konstantinou, A.; Fürnkranz, A.; Schmidt, B. Complications in Catheter Ablation of Atrial Fibrillation in 3,000 Consecutive Procedures: Balloon Versus Radiofrequency Current Ablation. JACC Clin. Electrophysiol. 2017, 3, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Turagam, M.K.; Vuddanda, V.; Atkins, D.; Venkata, R.; Yarlagadda, B.; Korra, H.; Pitchika, J.; Bommana, S.; Lakkireddy, D.R. Assessment of DNA Damage After Ionizing Radiation Exposure in Patients Undergoing Cardiac Resynchronization Therapy Device Implantation or Atrial Fibrillation Ablation (The RADAR Study). J. Atr. Fibrillation 2018, 11, 2094. [Google Scholar] [CrossRef]
- Rudnick, M.R.; Leonberg-Yoo, A.K.; Litt, H.I.; Cohen, R.M.; Hilton, S.; Reese, P.P. The Controversy of Contrast-Induced Nephropathy With Intravenous Contrast: What Is the Risk? Am. J. Kidney Dis. 2020, 75, 105–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.J.; Son, J.H.; Kim, T.-B.; Kang, M.K.; Han, K.; Kim, E.H.; Kim, A.Y.; Park, S.H. Relationship between Lower Dose and Injection Speed of Iodinated Contrast Material for CT and Acute Hypersensitivity Reactions: An Observational Study. Radiology 2019, 293, 565–572. [Google Scholar] [CrossRef] [PubMed]
- de Greef, Y.; Ströker, E.; Schwagten, B.; Kupics, K.; de Cocker, J.; Chierchia, G.-B.; de Asmundis, C.; Stockman, D.; Buysschaert, I. Complications of pulmonary vein isolation in atrial fibrillation: Predictors and comparison between four different ablation techniques: Results from the MIddelheim PVI-registry. Europace 2018, 20, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Pürerfellner, H.; Martinek, M. Pulmonary vein stenosis following catheter ablation of atrial fibrillation. Curr. Opin. Cardiol. 2005, 20, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Marom, E.M.; Herndon, J.E.; Kim, Y.H.; McAdams, H.P. Variations in pulmonary venous drainage to the left atrium: Implications for radiofrequency ablation. Radiology 2004, 230, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Voskoboinik, A.; Sparks, P.B.; Morton, J.B.; Lee, G.; Joseph, S.A.; Hawson, J.J.; Kistler, P.M.; Kalman, J.M. Low Rates of Major Complications for Radiofrequency Ablation of Atrial Fibrillation Maintained Over 14 Years: A Single Centre Experience of 2750 Consecutive Cases. Heart Lung Circ. 2018, 27, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Strohmer, B.; Schernthaner, C.; Pichler, M. Simultaneous angiographic imaging of ipsilateral pulmonary veins for catheter ablation of atrial fibrillation. Clin Res Cardiol 2006, 95, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Good, E.; Oral, H.; Lemola, K.; Han, J.; Tamirisa, K.; Igic, P.; Elmouchi, D.; Tschopp, D.; Reich, S.; Chugh, A.; et al. Movement of the esophagus during left atrial catheter ablation for atrial fibrillation. J. Am. Coll. Cardiol. 2005, 46, 2107–2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heist, E.K.; Holmvang, G.; Abbara, S.; Ruskin, J.N.; Mansour, M. Pre-Procedural Imaging to Direct Catheter Ablation of Atrial Fibrillation: Anatomy and Ablation Strategy. J. Atr. Fibrillation 2008, 1, 13. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Angiography + (n = 67) | Angiography − (n = 72) | p-Value | |
|---|---|---|---|
| Age (years) | 66.09 ± 10.54 | 66.40 ± 12.72 | 0.48 |
| Male, n (%) | 48 (71.64%) | 39 (53.42%) | 0.04 * |
| BMI (kg/m2) | 28.31 ± 5.23 | 28.41 ± 5.17 | 1.00 |
| Paroxysmal AF, n (%) | 21 (31.34%) | 29 (40.28%) | 0.29 |
| CHA2DS2-VASc score | 2.46 ± 1.40 | 2.42 ± 1.47 | 0.87 |
| LV ejection fraction % | 55.23 ± 12.50 | 57.36 ± 9.28 | 0.58 |
| LA diameter, mm | 46.88 ± 8.86 | 46.41 ± 8.40 | 0.87 |
| Atrial fibrosis % | 23.23 ± 26.81 | 18.92 ± 25.21 | 0.12 |
| PV common ostium | 4 (5.97%) | 8 (11.11%) | 0.37 |
| Additional PV | 9 (13.43%) | 15 (20.83%) | 0.27 |
| Chronic kidney disease, n (%) | 12 (17.91%) | 14 (19.44%) | 0.83 |
| Coronary artery disease, n (%) | 17 (25.37%) | 16 (22.22%) | 0.69 |
| Hypertension, n (%) | 41 (61.19%) | 46 (63.89%) | 0.86 |
| Diabetes, n (%) | 8 (11.94%) | 13 (18.06%) | 0.35 |
| Prior stroke/TIA, n (%) | 6 (8.96%) | 1 (1.39%) | 0.06 |
| Angiography + (n = 67) | Angiography − (n = 72) | p-Value | |
|---|---|---|---|
| PV entrance and exit block | 67 (100%) | 72 (100%) | 1.00 |
| Additional ablations (substrate and/or CTI) | 13 (19.4%) | 9 (12.5%) | 0.35 |
| Procedural duration (min) | 111.8 ± 23.65 | 117.7 ± 27.60 | 0.18 |
| Dose area product (cGy*cm2) | 1574 ± 1125 | 976.1 ± 506.9 | 0.01 * |
| Fluoroscopy time (min) | 13.9 ± 6.59 | 14.56 ± 6.36 | 0.45 |
| Contrast agent (ml) | 37.75 ± 5.92 | 7.17 ± 1.74 | <0.01 * |
| Major complication | 0 (0%) | 0 (0%) | 1.00 |
| Minor complication | 3 (4.41%) | 3 (4.47%) | 1.00 |
| Recurrence of AF in the first year after PVI | 20 (29.85%) | 17 (23.61%) | 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weyand, S.; Adam, V.; Beuter, M.; Hanger, S.; Heinzmann, D.; Schrezenmeier, W.; Seizer, P. Effect of Left Atrial Pulmonary Vein Angiography on Safety and Efficacy for High-Power, Short-Duration Pulmonary Vein Isolation in Patients with Atrial Fibrillation. J. Clin. Med. 2023, 12, 1094. https://doi.org/10.3390/jcm12031094
Weyand S, Adam V, Beuter M, Hanger S, Heinzmann D, Schrezenmeier W, Seizer P. Effect of Left Atrial Pulmonary Vein Angiography on Safety and Efficacy for High-Power, Short-Duration Pulmonary Vein Isolation in Patients with Atrial Fibrillation. Journal of Clinical Medicine. 2023; 12(3):1094. https://doi.org/10.3390/jcm12031094
Chicago/Turabian StyleWeyand, Sebastian, Viola Adam, Matthias Beuter, Simon Hanger, David Heinzmann, Willibald Schrezenmeier, and Peter Seizer. 2023. "Effect of Left Atrial Pulmonary Vein Angiography on Safety and Efficacy for High-Power, Short-Duration Pulmonary Vein Isolation in Patients with Atrial Fibrillation" Journal of Clinical Medicine 12, no. 3: 1094. https://doi.org/10.3390/jcm12031094