
Percutaneous Coronary Intervention in Out-of-Hospital Cardiac Arrest Related to Acute Coronary Syndrome: A Literature Review

 , ,
, ,
Abstract
:1. Introduction
2. Epidemiology of CAD in OHCA
3. Rationale and Timing for CAG after OHCA
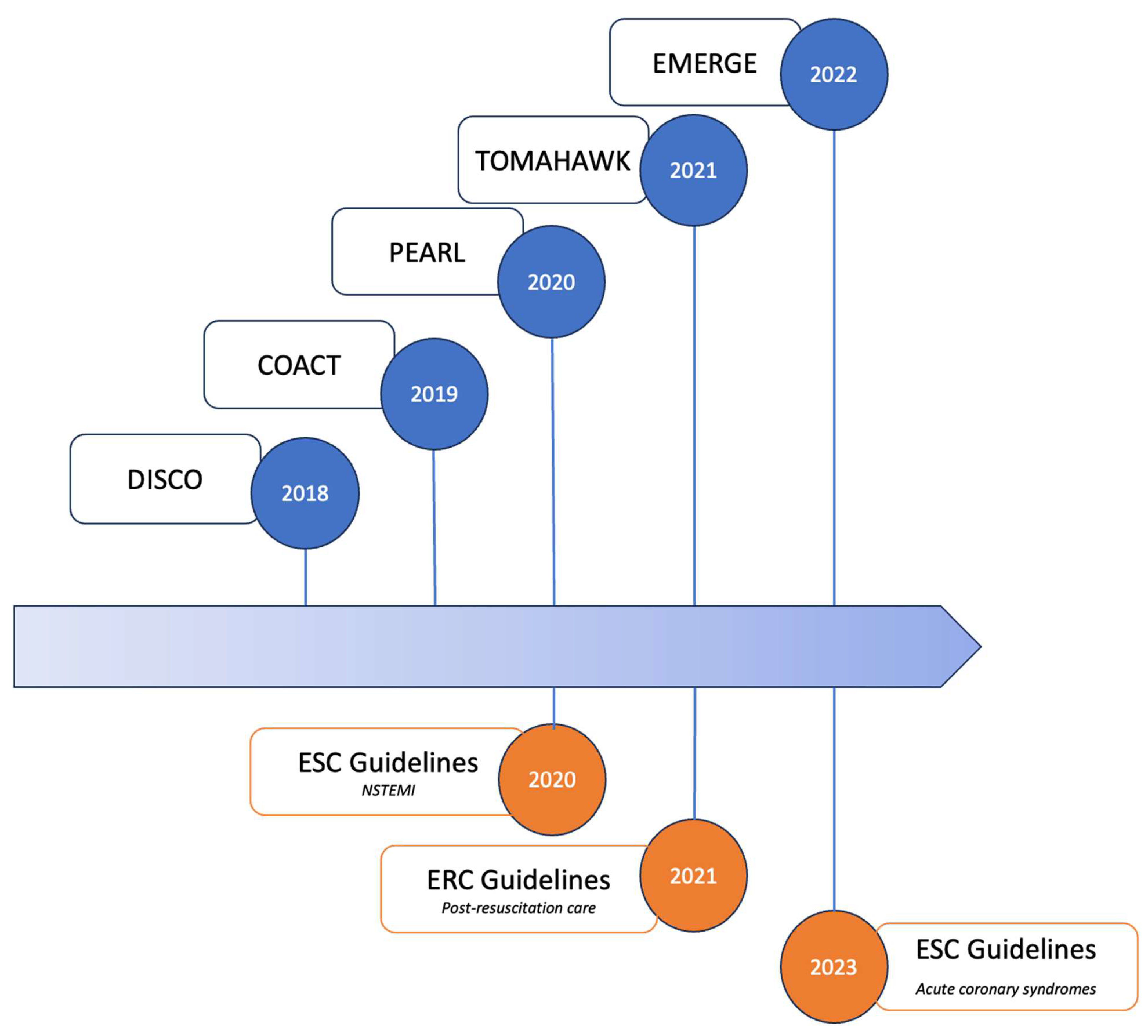
3.1. Current Evidence
3.2. Current Guidelines: Early vs. Delayed Percutaneous Coronary Intervention
4. PCI vs. Surgical Approach with Coronary Artery Bypass Grafting
5. PCI Strategy in OHCA Related to MI
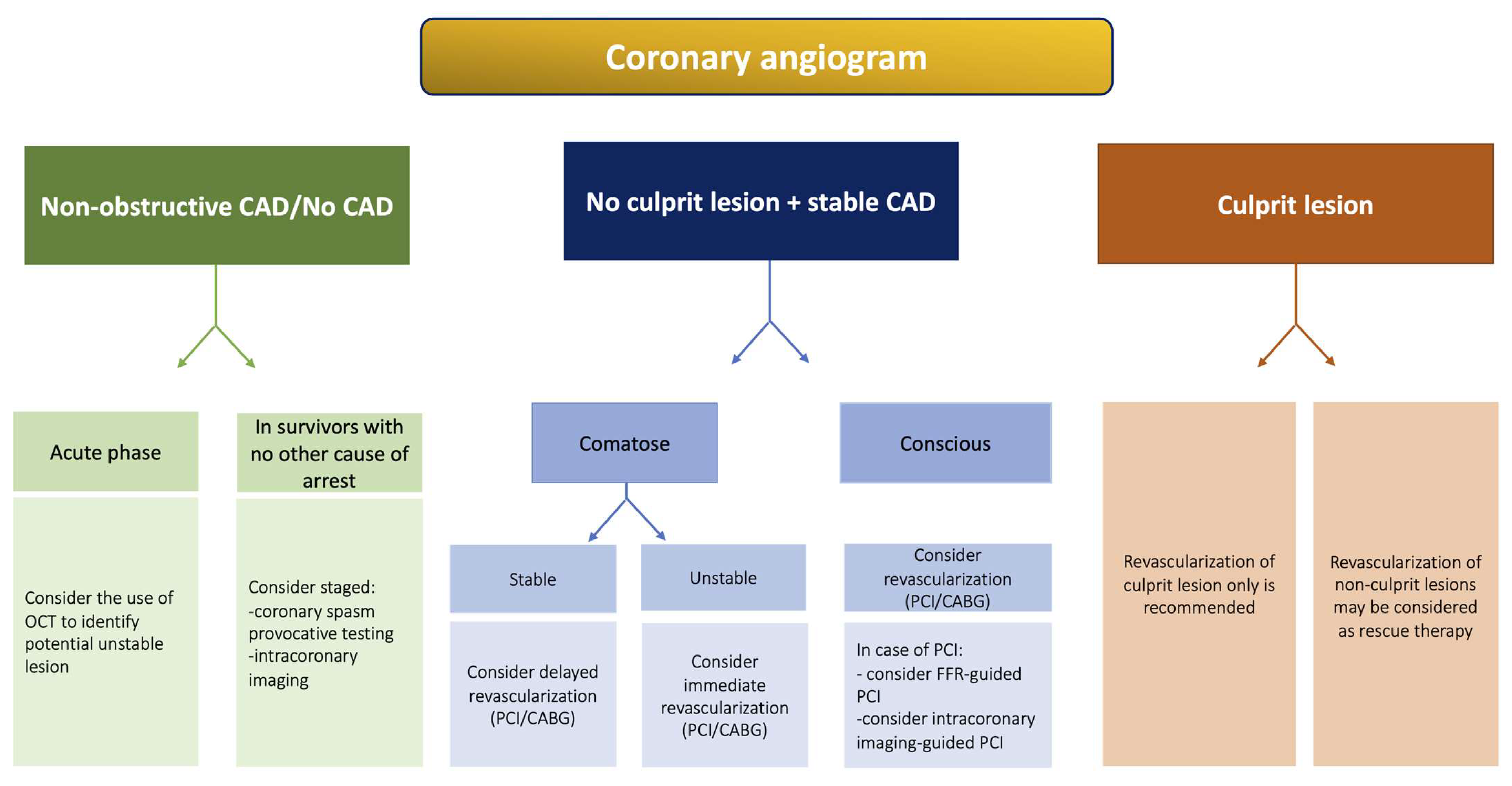
5.1. Culprit vs. Multivessel PCI
5.2. OHCA with Stable CAD
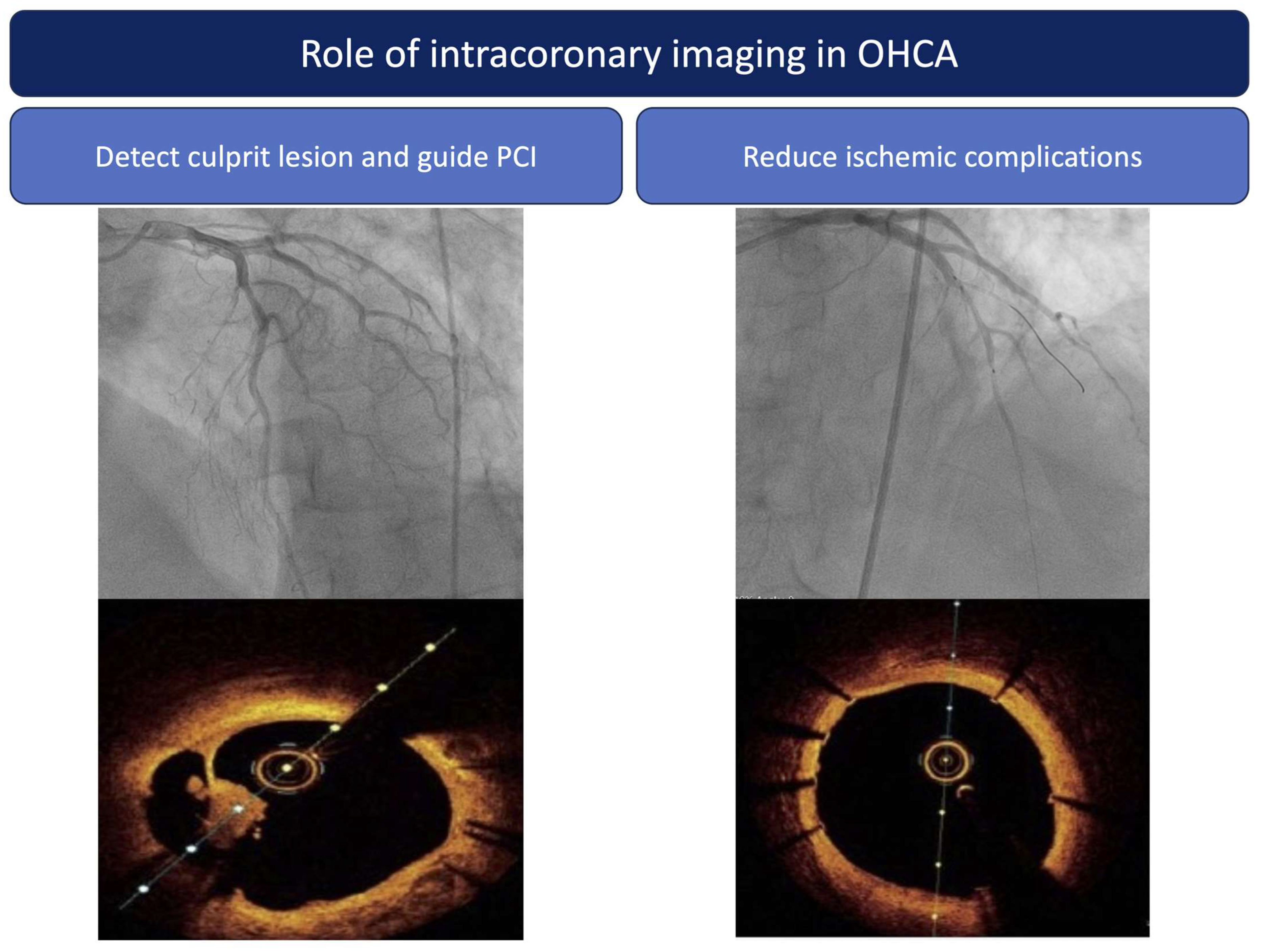
5.3. Role of Intracoronary Imaging in OHCA Related to MI
5.4. Balance between Ischemic and Bleeding Risk after OHCA Related to MI and Further Implications for Anti-Thrombotic Regimen
5.4.1. Ischemic Risk after OHCA
5.4.2. Bleeding Risk after OHCA
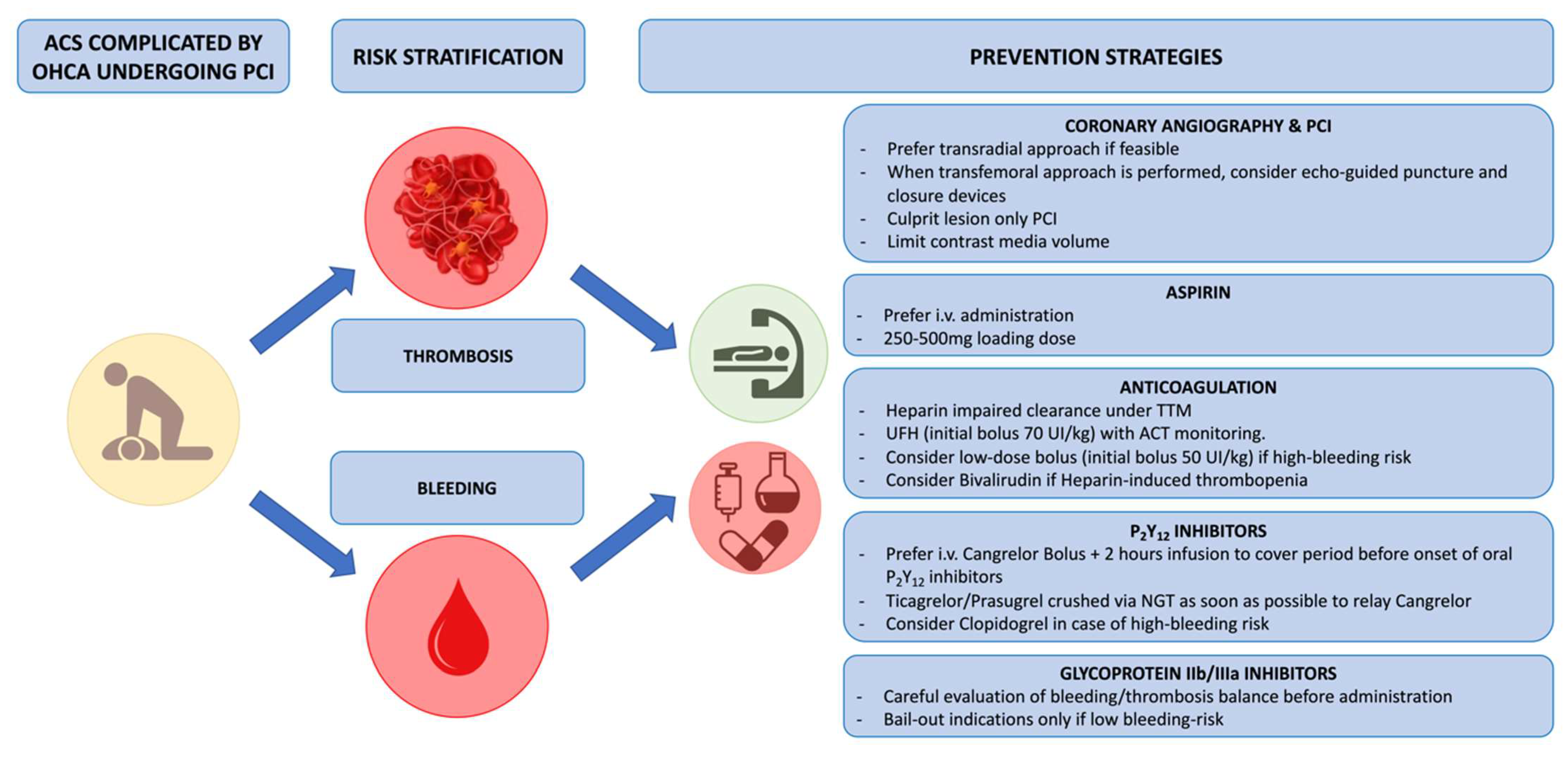
5.5. Implication for Anti-Thrombotic Regimen (Figure 4)

6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACS | acute coronary syndrome |
| CAD | coronary artery disease |
| ECG | electrocardiogram |
| ESC | European Society of Cardiology |
| CAG | coronary angiography |
| ICU | intensive care units |
| MI | myocardial infarction |
| NSTE | non-ST-segment elevation |
| NSTEMI | non-ST segment elevation myocardial infarction |
| OHCA | out-of-hospital cardiac arrest |
| PCI | percutaneous coronary intervention |
| RCT | randomized controlled trial |
| ROSC | return of spontaneous circulation |
| STE | ST-segment elevation |
| STEMI | ST-segment elevation myocardial infarction |
| TTM | targeted temperature management |
References
- Gräsner, J.-T.; Herlitz, J.; Tjelmeland, I.B.M.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef] [PubMed]
- Engdahl, J.; Holmberg, M.; Karlson, B.W.; Luepker, R.; Herlitz, J. The epidemiology of out-of-hospital “sudden” cardiac arrest. Resuscitation 2002, 52, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, C.M.; Joly, L.M.; Rosenberg, A.; Monchi, M.; Weber, S.N.; Dhainaut, J.F.; Carli, P. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N. Engl. J. Med. 1997, 336, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Elfwén, L.; Lagedal, R.; Nordberg, P.; James, S.; Oldgren, J.; Böhm, F.; Lundgren, P.; Rylander, C.; van der Linden, J.; Hollenberg, J.; et al. Direct or subacute coronary angiography in out-of-hospital cardiac arrest (DISCO)-An initial pilot-study of a randomized clinical trial. Resuscitation 2019, 139, 253–261. [Google Scholar] [CrossRef]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.D.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef]
- Kern, K.B.; Radsel, P.; Jentzer, J.C.; Seder, D.B.; Lee, K.S.; Lotun, K.; Janardhanan, R.; Stub, D.; Hsu, C.-H.; Noc, M. Randomized Pilot Clinical Trial of Early Coronary Angiography versus No Early Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: The PEARL Study. Circulation 2020, 142, 2002–2012. [Google Scholar] [CrossRef]
- Desch, S.; Freund, A.; Akin, I.; Behnes, M.; Preusch, M.R.; Zelniker, T.A.; Skurk, C.; Landmesser, U.; Graf, T.; Eitel, I.; et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2021, 385, 2544–2553. [Google Scholar] [CrossRef]
- Hauw-Berlemont, C.; Lamhaut, L.; Diehl, J.-L.; Andreotti, C.; Varenne, O.; Leroux, P.; Lascarrou, J.-B.; Guerin, P.; Loeb, T.; Roupie, E.; et al. Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial. JAMA Cardiol. 2022, 7, 700–707. [Google Scholar] [CrossRef]
- Scquizzato, T.; Sofia, R.; Gazzato, A.; Sudano, A.; Altizio, S.; Biondi-Zoccai, G.; Ajello, S.; Scandroglio, A.M.; Landoni, G.; Zangrillo, A. Coronary angiography findings in resuscitated and refractory out-of-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2023, 189, 109869. [Google Scholar] [CrossRef]
- Garcia, S.; Drexel, T.; Bekwelem, W.; Raveendran, G.; Caldwell, E.; Hodgson, L.; Wang, Q.; Adabag, S.; Mahoney, B.; Frascone, R.; et al. Early Access to the Cardiac Catheterization Laboratory for Patients Resuscitated From Cardiac Arrest Due to a Shockable Rhythm: The Minnesota Resuscitation Consortium Twin Cities Unified Protocol. J. Am. Heart Assoc. 2016, 5, e002670. [Google Scholar] [CrossRef] [PubMed]
- Kern, K.B.; Lotun, K.; Patel, N.; Mooney, M.R.; Hollenbeck, R.D.; McPherson, J.A.; McMullan, P.W.; Unger, B.; Hsu, C.-H.; Seder, D.B.; et al. Outcomes of Comatose Cardiac Arrest Survivors with and without ST-Segment Elevation Myocardial Infarction: Importance of Coronary Angiography. JACC Cardiovasc. Interv. 2015, 8, 1031–1040. [Google Scholar] [CrossRef]
- Yannopoulos, D.; Bartos, J.A.; Raveendran, G.; Conterato, M.; Frascone, R.J.; Trembley, A.; John, R.; Connett, J.; Benditt, D.G.; Lurie, K.G.; et al. Coronary Artery Disease in Patients With Out-of-Hospital Refractory Ventricular Fibrillation Cardiac Arrest. J. Am. Coll. Cardiol. 2017, 70, 1109–1117. [Google Scholar] [CrossRef]
- Lamhaut, L.; Tea, V.; Raphalen, J.-H.; An, K.; Dagron, C.; Jouffroy, R.; Jouven, X.; Cariou, A.; Baud, F.; Spaulding, C.; et al. Coronary lesions in refractory out of hospital cardiac arrest (OHCA) treated by extra corporeal pulmonary resuscitation (ECPR). Resuscitation 2018, 126, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Voicu, S.; Bajoras, V.; Gall, E.; Deye, N.; Malissin, I.; Dillinger, J.-G.; Benajiba, C.; Logeart, D.; Henry, P.; Megarbane, B.; et al. Immediate coronary angiogram in out-of-hospital cardiac arrest patients with non-shockable initial rhythm and without ST-segment elevation—Is there a clinical benefit? Resuscitation 2020, 155, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Degrell, P.; Picard, F.; Combaret, N.; Mogi, S.; Motreff, P.; Cariou, A.; Varenne, O. Coronary atherothrombosis in cardiac arrest survivors without ST-segment elevation on ECG. Resuscitation 2019, 139, 189–191. [Google Scholar] [CrossRef]
- Degrell, P.; Varenne, O. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 381, 188. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef]
- Davies, M.J.; Thomas, A. Thrombosis and acute coronary-artery lesions in sudden cardiac ischemic death. N. Engl. J. Med. 1984, 310, 1137–1140. [Google Scholar] [CrossRef]
- Myerburg, R.J.; Conde, C.A.; Sung, R.J.; Mayorga-Cortes, A.; Mallon, S.M.; Sheps, D.S.; Appel, R.A.; Castellanos, A. Clinical, electrophysiologic and hemodynamic profile of patients resuscitated from prehospital cardiac arrest. Am. J. Med. 1980, 68, 568–576. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 61, e78–e140. [Google Scholar] [CrossRef] [PubMed]
- Bro-Jeppesen, J.; Kjaergaard, J.; Wanscher, M.; Pedersen, F.; Holmvang, L.; Lippert, F.K.; Møller, J.E.; Køber, L.; Hassager, C. Emergency coronary angiography in comatose cardiac arrest patients: Do real-life experiences support the guidelines? Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Dankiewicz, J.; Nielsen, N.; Annborn, M.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Kjaergaard, J.; Pellis, T.; Friberg, H. Survival in patients without acute ST elevation after cardiac arrest and association with early coronary angiography: A post hoc analysis from the TTM trial. Intensive Care Med. 2015, 41, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Dumas, F.; Bougouin, W.; Geri, G.; Lamhaut, L.; Rosencher, J.; Pène, F.; Chiche, J.-D.; Varenne, O.; Carli, P.; Jouven, X.; et al. Emergency Percutaneous Coronary Intervention in Post-Cardiac Arrest Patients Without ST-Segment Elevation Pattern: Insights From the PROCAT II Registry. JACC Cardiovasc. Interv. 2016, 9, 1011–1018. [Google Scholar] [CrossRef]
- Caniato, F.; Lazzeri, C.; Bonizzoli, M.; Mattesini, A.; Batacchi, S.; Cappelli, F.; Di Mario, C.; Peris, A. Urgent coronary angiography in out-of-hospital cardiac arrest: A retrospective single centre investigation. J. Cardiovasc. Med. 2023, 24, 637–641. [Google Scholar] [CrossRef]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.M.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C.; et al. European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensive Care Med. 2015, 41, 2039–2056. [Google Scholar] [CrossRef]
- Welsford, M.; Nikolaou, N.I.; Beygui, F.; Bossaert, L.; Ghaemmaghami, C.; Nonogi, H.; O’Connor, R.E.; Pichel, D.R.; Scott, T.; Walters, D.L.; et al. Part 5: Acute Coronary Syndromes: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015, 132, S146–S176. [Google Scholar] [CrossRef]
- Maupain, C.; Bougouin, W.; Lamhaut, L.; Deye, N.; Diehl, J.-L.; Geri, G.; Perier, M.-C.; Beganton, F.; Marijon, E.; Jouven, X.; et al. The CAHP (Cardiac Arrest Hospital Prognosis) score: A tool for risk stratification after out-of-hospital cardiac arrest. Eur. Heart J. 2016, 37, 3222–3228. [Google Scholar] [CrossRef]
- Pareek, N.; Beckley-Hoelscher, N.; Kanyal, R.; Cannata, A.; Kordis, P.; Sunderland, N.; Kirresh, A.; Nevett, J.; Fothergill, R.; Webb, I.; et al. MIRACLE2 Score and SCAI Grade to Identify Patients With Out-of-Hospital Cardiac Arrest for Immediate Coronary Angiography. JACC Cardiovasc. Interv. 2022, 15, 1074–1084. [Google Scholar] [CrossRef]
- Aldous, R.; Roy, R.; Cannata, A.; Abdrazak, M.; Mohanan, S.; Beckley-Hoelscher, N.; Stahl, D.; Kanyal, R.; Kordis, P.; Sunderland, N.; et al. MIRACLE2 Score Compared with Downtime and Current Selection Criterion for Invasive Cardiovascular Therapies After OHCA. JACC Cardiovasc. Interv. 2023, 16, 2439–2450. [Google Scholar] [CrossRef]
- Noc, M.; Fajadet, J.; Lassen, J.F.; Kala, P.; MacCarthy, P.; Olivecrona, G.K.; Windecker, S.; Spaulding, C. Invasive coronary treatment strategies for out-of-hospital cardiac arrest: A consensus statement from the European association for percutaneous cardiovascular interventions (EAPCI)/stent for life (SFL) groups. EuroIntervention 2014, 10, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Rab, T.; Kern, K.B.; Tamis-Holland, J.E.; Henry, T.D.; McDaniel, M.; Dickert, N.W.; Cigarroa, J.E.; Keadey, M.; Ramee, S.; Interventional Council, American College of Cardiology. Cardiac Arrest: A Treatment Algorithm for Emergent Invasive Cardiac Procedures in the Resuscitated Comatose Patient. J. Am. Coll. Cardiol. 2015, 66, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367, Erratum in Eur. Heart J. 2021, 42, 1908; Erratum in Eur. Heart J. 2021, 42, 1925; Erratum in Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Gall, E.; Lafont, A.; Varenne, O.; Dumas, F.; Cariou, A.; Picard, F. Balancing thrombosis and bleeding after out-of-hospital cardiac arrest related to acute coronary syndrome: A literature review. Arch. Cardiovasc. Dis. 2021, 114, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.; Bloom, J.E.; Dawson, L.; Shirwaiker, A.; Bernard, S.; Nehme, Z.; Donner, D.; Hauw-Berlemont, C.; Vilfaillot, A.; Chan, W.; et al. Early versus deferred coronary angiography following cardiac arrest. A systematic review and meta-analysis. Resusc. Plus 2023, 14, 100381. [Google Scholar] [CrossRef] [PubMed]
- Al Lawati, K.; Forestell, B.; Binbraik, Y.; Sharif, S.; Ainsworth, C.; Mathew, R.; Amin, F.; Al Fawaz, M.; Pinilla-Echeverri, N.; Belley-Côté, E.; et al. Early Versus Delayed Coronary Angiography After Out-of-Hospital Cardiac Arrest Without ST-Segment Elevation-A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Explor. 2023, 5, e0874. [Google Scholar] [CrossRef]
- Spirito, A.; Vaisnora, L.; Papadis, A.; Iacovelli, F.; Sardu, C.; Selberg, A.; Bär, S.; Kavaliauskaite, R.; Temperli, F.; Asatryan, B.; et al. Acute Coronary Occlusion in Patients With Non-ST-Segment Elevation Out-of-Hospital Cardiac Arrest. J. Am. Coll. Cardiol. 2023, 81, 446–456. [Google Scholar] [CrossRef]
- Farooq, V.; van Klaveren, D.; Steyerberg, E.W.; Meliga, E.; Vergouwe, Y.; Chieffo, A.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.; et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: Development and validation of SYNTAX score II. Lancet 2013, 381, 639–650. [Google Scholar] [CrossRef] [PubMed]
- Moscucci, M.; Fox, K.A.; Cannon, C.P.; Klein, W.; López-Sendón, J.; Montalescot, G.; White, K.; Goldberg, R.J. Predictors of major bleeding in acute coronary syndromes: The Global Registry of Acute Coronary Events (GRACE). Eur. Heart J. 2003, 24, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Chase, A.J.; Fretz, E.B.; Warburton, W.P.; Klinke, W.P.; Carere, R.G.; Pi, D.; Berry, B.; Hilton, J.D. Association of the arterial access site at angioplasty with transfusion and mortality: The M.O.R.T.A.L study (Mortality benefit Of Reduced Transfusion after percutaneous coronary intervention via the Arm or Leg). Heart Br. Card. Soc. 2008, 94, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Montalescot, G.; Ongen, Z.; Guindy, R.; Sousa, A.; Lu, S.-Z.; Pahlajani, D.; Pellois, A.; Vicaut, E.; RIVIERA Investigators. Predictors of outcome in patients undergoing PCI. Results of the RIVIERA study. Int. J. Cardiol. 2008, 129, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.S.; Yusuf, S.; Cairns, J.; Niemelä, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemelä, M.; Valentin, V.; Lewis, B.S.; et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet 2011, 377, 1409–1420. [Google Scholar] [CrossRef]
- Gargiulo, G.; Valgimigli, M.; Sunnåker, M.; Vranckx, P.; Frigoli, E.; Leonardi, S.; Spirito, A.; Gragnano, F.; Manavifar, N.; Galea, R.; et al. Choice of access site and type of anticoagulant in acute coronary syndromes with advanced Killip class or out-of-hospital cardiac arrest. Rev. Espanola Cardiol. Engl. Ed. 2020, 73, 893–901. [Google Scholar] [CrossRef]
- Le May, M.; Wells, G.; So, D.; Chong, A.Y.; Dick, A.; Froeschl, M.; Glover, C.; Hibbert, B.; Marquis, J.-F.; Blondeau, M.; et al. Safety and Efficacy of Femoral Access vs Radial Access in ST-Segment Elevation Myocardial Infarction: The SAFARI-STEMI Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 126–134. [Google Scholar] [CrossRef]
- Guedeney, P.; Thiele, H.; Kerneis, M.; Barthélémy, O.; Baumann, S.; Sandri, M.; de Waha-Thiele, S.; Fuernau, G.; Rouanet, S.; Piek, J.J.; et al. Radial versus femoral artery access for percutaneous coronary artery intervention in patients with acute myocardial infarction and multivessel disease complicated by cardiogenic shock: Subanalysis from the CULPRIT-SHOCK trial. Am. Heart J. 2020, 225, 60–68. [Google Scholar] [CrossRef]
- Marquis-Gravel, G.; Tremblay-Gravel, M.; Lévesque, J.; Généreux, P.; Schampaert, E.; Palisaitis, D.; Doucet, M.; Charron, T.; Terriault, P.; Tessier, P. Ultrasound guidance versus anatomical landmark approach for femoral artery access in coronary angiography: A randomized controlled trial and a meta-analysis. J. Interv. Cardiol. 2018, 31, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.S.; AlRashidi, S.; d’Entremont, M.-A.; Alansari, O.; Brochu, B.; Heenan, L.; Skuriat, E.; Tyrwhitt, J.; Raco, M.; Tsang, M.; et al. Routine Ultrasonography Guidance for Femoral Vascular Access for Cardiac Procedures: The UNIVERSAL Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 1110–1118. [Google Scholar] [CrossRef]
- d’Entremont, M.-A.; Alrashidi, S.; Alansari, O.; Brochu, B.; Heenan, L.; Skuriat, E.; Tyrwhitt, J.; Raco, M.; Tsang, M.; Valettas, N.; et al. Ultrasound-guided femoral access in patients with vascular closure devices: A prespecified analysis of the randomised UNIVERSAL trial. EuroIntervention 2023, 19, 73–79. [Google Scholar] [CrossRef]
- Sugizaki, Y.; Shinke, T.; Doi, T.; Igarashi, N.; Otake, H.; Kawamori, H.; Hirata, K.-I. Impact of the angiographic burden on the incidence of out-of-hospital ventricular fibrillation in patients with acute myocardial infarction. Heart Vessel. 2019, 34, 52–61. [Google Scholar] [CrossRef]
- Stähli, B.E.; Varbella, F.; Linke, A.; Schwarz, B.; Felix, S.B.; Seiffert, M.; Kesterke, R.; Nordbeck, P.; Witzenbichler, B.; Lang, I.M.; et al. Timing of Complete Revascularization with Multivessel PCI for Myocardial Infarction. N. Engl. J. Med. 2023, 389, 1368–1379. [Google Scholar] [CrossRef]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; de Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Yang, J.H.; Park, T.K.; Lee, J.M.; Song, Y.B.; Hahn, J.-Y.; Choi, S.-H.; Ahn, C.-M.; Yu, C.W.; Park, I.H.; et al. Culprit-Only versus Immediate Multivessel Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction Complicating Advanced Cardiogenic Shock Requiring Venoarterial-Extracorporeal Membrane Oxygenation. J. Am. Heart Assoc. 2023, 12, e029792. [Google Scholar] [CrossRef] [PubMed]
- Mylotte, D.; Morice, M.C.; Eltchaninoff, H.; Garot, J.; Louvard, Y.; Lefèvre, T.; Garot, P. Primary percutaneous coronary intervention in patients with acute myocardial infarction, resuscitated cardiac arrest, and cardiogenic shock: The role of primary multivessel revascularization. JACC Cardiovasc. Interv. 2013, 6, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Task Force Members; Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003, Erratum in Eur. Heart J. 2014, 35, 2260–2261. [Google Scholar] [CrossRef]
- Kaziród-Wolski, K.; Sielski, J.; Gąsior, M.; Bujak, K.; Hawranek, M.; Pyka, Ł.; Gierlotka, M.; Pawłowski, T.; Siudak, Z. Factors Affecting Short- and Long-Term Survival of Patients with Acute Coronary Syndrome Treated Invasively Using Intravascular Ultrasound and Fractional Flow Reserve: Analysis of Data from the Polish Registry of Acute Coronary Syndromes 2017–2020. Kardiol. Pol. (Pol. Heart J.) 2023, 81, 265–272. Available online: https://pubmed.ncbi.nlm.nih.gov/36404732/ (accessed on 13 November 2023). [CrossRef] [PubMed]
- Sideris, G.; Voicu, S.; Dillinger, J.G.; Stratiev, V.; Logeart, D.; Broche, C.; Vivien, B.; Brun, P.-Y.; Deye, N.; Capan, D.; et al. Value of post-resuscitation electrocardiogram in the diagnosis of acute myocardial infarction in out-of-hospital cardiac arrest patients. Resuscitation 2011, 82, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Bogale, N.; Lempereur, M.; Sheikh, I.; Wood, D.; Saw, J.; Fung, A. Optical coherence tomography (OCT) evaluation of intermediate coronary lesions in patients with NSTEMI. Cardiovasc. Revasculariz. Med. Mol. Interv. 2016, 17, 113–118. [Google Scholar] [CrossRef]
- Picard, F.; Llitjos, J.-F.; Diefenbronn, M.; Laghlam, D.; Seret, G.; Sokoloff, A.; Cariou, A.; Dumas, F.; Varenne, O. The balance of thrombosis and hemorrhage in STEMI patients with or without associated cardiac arrest: An observational study. Resuscitation 2019, 145, 83–90. [Google Scholar] [CrossRef]
- Johnson, T.W.; Räber, L.; di Mario, C.; Bourantas, C.; Jia, H.; Mattesini, A.; Gonzalo, N.; de la Torre Hernandez, J.M.; Prati, F.; Koskinas, K.; et al. Clinical use of intracoronary imaging. Part 2: Acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2019, 40, 2566–2584. [Google Scholar] [CrossRef]
- Brami, P.; Picard, F.; Seret, G.; Fischer, Q.; Pham, V.; Varenne, O. Intracoronary imaging in addition to coronary angiography for patients with out-of-hospital cardiac arrest: More information for better care? Arch. Cardiovasc. Dis. 2023, 116, 272–281. [Google Scholar] [CrossRef]
- Souteyrand, G.; Arbustini, E.; Motreff, P.; Gatto, L.; Di Vito, L.; Marco, V.; Amabile, N.; Chisari, A.; Kodama, T.; Romagnoli, E.; et al. Serial optical coherence tomography imaging of ACS-causing culprit plaques. EuroIntervention 2015, 11, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Witzenbichler, B.; Weisz, G.; Rinaldi, M.J.; Neumann, F.-J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; Duffy, P.L.; Mazzaferri, E.; et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): A prospective multicentre registry study. Lancet 2013, 382, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Clinical use of intracoronary imaging. Part 1: Guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Choi, K.H.; Song, Y.B.; Lee, J.-Y.; Lee, S.-J.; Lee, S.Y.; Kim, S.M.; Yun, K.H.; Cho, J.Y.; Kim, C.J.; et al. Intravascular Imaging-Guided or Angiography-Guided Complex PCI. N. Engl. J. Med. 2023, 388, 1668–1679. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Landmesser, U.; Maehara, A.; Matsumura, M.; Shlofmitz, R.A.; Guagliumi, G.; Price, M.J.; Hill, J.M.; Akasaka, T.; Prati, F.; et al. Optical Coherence Tomography-Guided versus Angiography-Guided PCI. N. Engl. J. Med. 2023, 389, 1466–1476. [Google Scholar] [CrossRef] [PubMed]
- Holm, N.R.; Andreasen, L.N.; Neghabat, O.; Laanmets, P.; Kumsars, I.; Bennett, J.; Olsen, N.T.; Odenstedt, J.; Hoffmann, P.; Dens, J.; et al. OCT or Angiography Guidance for PCI in Complex Bifurcation Lesions. N. Engl. J. Med. 2023, 389, 1477–1487. [Google Scholar] [CrossRef]
- Ducrocq, G.; Schulte, P.J.; Budaj, A.; Cornel, J.H.; Held, C.; Himmelmann, A.; Husted, S.; Storey, R.F.; Cannon, C.P.; Becker, R.C.; et al. Balancing the risk of spontaneous ischemic and major bleeding events in acute coronary syndromes. Am. Heart J. 2017, 186, 91–99. [Google Scholar] [CrossRef]
- Spirito, A.; Gargiulo, G.; Siontis, G.C.M.; Mitsis, A.; Billinger, M.; Windecker, S.; Valgimigli, M. Cardiovascular mortality and morbidity in patients undergoing percutaneous coronary intervention after out-of-hospital cardiac arrest: A systematic review and meta-analysis. EuroIntervention 2021, 16, e1245–e1253. [Google Scholar] [CrossRef] [PubMed]
- Rauber, M.; Nicol, P.; Sabic, E.; Joner, M.; Noc, M. Timing and predictors of definite stent thrombosis in comatose survivors of out-of-hospital cardiac arrest undergoing percutaneous coronary intervention and therapeutic hypothermia (ST-OHCA study). EuroIntervention 2022, 18, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Xavier, R.G.; White, A.E.; Fox, S.C.; Wilcox, R.G.; Heptinstall, S. Enhanced platelet aggregation and activation under conditions of hypothermia. Thromb. Haemost. 2007, 98, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Steblovnik, K.; Blinc, A.; Bozic-Mijovski, M.; Kranjec, I.; Melkic, E.; Noc, M. Platelet reactivity in comatose survivors of cardiac arrest undergoing percutaneous coronary intervention and hypothermia. EuroIntervention 2015, 10, 1418–1424. [Google Scholar] [CrossRef]
- Rosillo, S.O.; Lopez-de-Sa, E.; Iniesta, A.M.; de Torres, F.; del Prado, S.; Rey, J.R.; Armada, E.; Moreno, R.; López-Sendón, J.L. Is therapeutic hypothermia a risk factor for stent thrombosis? J. Am. Coll. Cardiol. 2014, 63, 939–940. [Google Scholar] [CrossRef]
- Shah, N.; Chaudhary, R.; Mehta, K.; Agarwal, V.; Garg, J.; Freudenberger, R.; Jacobs, L.; Cox, D.; Kern, K.B.; Patel, N. Therapeutic Hypothermia and Stent Thrombosis: A Nationwide Analysis. JACC Cardiovasc. Interv. 2016, 9, 1801–1811. [Google Scholar] [CrossRef]
- Farag, M.; Spinthakis, N.; Srinivasan, M.; Sullivan, K.; Wellsted, D.; Gorog, D.A. Morphine Analgesia Pre-PPCI Is Associated with Prothrombotic State, Reduced Spontaneous Reperfusion and Greater Infarct Size. Thromb. Haemost. 2018, 118, 601–612. [Google Scholar] [CrossRef]
- Hobl, E.-L.; Stimpfl, T.; Ebner, J.; Schoergenhofer, C.; Derhaschnig, U.; Sunder-Plassmann, R.; Jilma-Stohlawetz, P.; Mannhalter, C.; Posch, M.; Jilma, B. Morphine decreases clopidogrel concentrations and effects: A randomized, double-blind, placebo-controlled trial. J. Am. Coll. Cardiol. 2014, 63, 630–635. [Google Scholar] [CrossRef]
- Puymirat, E.; Lamhaut, L.; Bonnet, N.; Aissaoui, N.; Henry, P.; Cayla, G.; Cattan, S.; Steg, G.; Mock, L.; Ducrocq, G.; et al. Correlates of pre-hospital morphine use in ST-elevation myocardial infarction patients and its association with in-hospital outcomes and long-term mortality: The FAST-MI (French Registry of Acute ST-elevation and non-ST-elevation Myocardial Infarction) programme. Eur. Heart J. 2016, 37, 1063–1071. [Google Scholar] [CrossRef]
- Furtado, R.H.M.; Nicolau, J.C.; Guo, J.; Im, K.; White, J.A.; Sabatine, M.S.; Newby, L.K.; Giugliano, R.P. Morphine and Cardiovascular Outcomes Among Patients With Non-ST-Segment Elevation Acute Coronary Syndromes Undergoing Coronary Angiography. J. Am. Coll. Cardiol. 2020, 75, 289–300. [Google Scholar] [CrossRef]
- Iqbal, J.; Sumaya, W.; Tatman, V.; Parviz, Y.; Morton, A.C.; Grech, E.D.; Campbell, S.; Storey, R.F.; Gunn, J. Incidence and predictors of stent thrombosis: A single-centre study of 5,833 consecutive patients undergoing coronary artery stenting. EuroIntervention 2013, 9, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, R.; Dinh, D.; Brennan, A.; Lefkovits, J.; Reid, C.; Duffy, S.J.; Cox, N.; Liew, D.; Stub, D.; VCOR Investigators. Incidence, Predictors and Clinical Outcomes of Stent Thrombosis Following Percutaneous Coronary Intervention in Contemporary Practice. Heart Lung Circ. 2020, 29, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Champigneulle, B.; Haruel, P.A.; Pirracchio, R.; Dumas, F.; Geri, G.; Arnaout, M.; Paul, M.; Pène, F.; Mira, J.P.; Bougouin, W.; et al. Major traumatic complications after out-of-hospital cardiac arrest: Insights from the Parisian registry. Resuscitation 2018, 128, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Danial, P.; Hajage, D.; Nguyen, L.S.; Mastroianni, C.; Demondion, P.; Schmidt, M.; Bouglé, A.; Amour, J.; Leprince, P.; Combes, A.; et al. Percutaneous versus surgical femoro-femoral veno-arterial ECMO: A propensity score matched study. Intensive Care Med. 2018, 44, 2153–2161. [Google Scholar] [CrossRef]
- Pancholy, S.B.; Palamaner Subash Shantha, G.; Romagnoli, E.; Kedev, S.; Bernat, I.; Rao, S.V.; Jolly, S.; Bertrand, O.F.; Patel, T.M. Impact of access site choice on outcomes of patients with cardiogenic shock undergoing percutaneous coronary intervention: A systematic review and meta-analysis. Am. Heart J. 2015, 170, 353–361. [Google Scholar] [CrossRef]
- Gorog, D.A.; Price, S.; Sibbing, D.; Baumbach, A.; Capodanno, D.; Gigante, B.; Halvorsen, S.; Huber, K.; Lettino, M.; Leonardi, S.; et al. Antithrombotic therapy in patients with acute coronary syndrome complicated by cardiogenic shock or out-of-hospital cardiac arrest: A joint position paper from the European Society of Cardiology (ESC) Working Group on Thrombosis, in association with the Acute Cardiovascular Care Association (ACCA) and European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 125–140. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication | Period of Inclusion | N | Performed CAG (%) | CAD Burden (%) | Culprit Lesion (%) | Chronic Total Occlusion (%) | Revascularization (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal or Insignifiant Disease | Presence of Obstructive Stable CAD | 1 Vessel | 2 Vessels | 3 Vessels | PCI Performed among Patients Undergoing CAG | CABG | ||||||
| Elfwen et al., 2018 [5] | 2015–2017 | 79 | 55 | NC | NC | NC | NC | NC | 19.9 | 5.3 | 39.5 | NC |
| Lemkes et al., 2019 [6] | 2015–2018 | 552 | 81.2 | 35 | 64.9 | 27.7 | 20.4 | 17 | 5.0 | 36.8 | 35.2 | 6.9 |
| Kern et al., 2020 [7] | 2015–2018 | 99 | 73.7 | 30.1 | 69.9 | 30.1 | 17.8 | 13.7 | 45.2 | 15.1 | 20.6 | 4.1 |
| Desch et al., 2021 [8] | 2016–2019 | 554 | 78.9 | 34.7 | 65.2 | 13.9 | 13.9 | 37.4 | 40.0 | NC | 39.6 | NC |
| Berlemont et al., 2022 [9] | 2017–2020 | 279 | 71.7 | 49 | 51 | 16.5 | 18 | 16.5 | NC | NC | 27.5 | NC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gall, E.; Mafi, D.; Ghannam, T.; Brami, P.; Pham, V.; Varenne, O.; Picard, F. Percutaneous Coronary Intervention in Out-of-Hospital Cardiac Arrest Related to Acute Coronary Syndrome: A Literature Review. J. Clin. Med. 2023, 12, 7275. https://doi.org/10.3390/jcm12237275
Gall E, Mafi D, Ghannam T, Brami P, Pham V, Varenne O, Picard F. Percutaneous Coronary Intervention in Out-of-Hospital Cardiac Arrest Related to Acute Coronary Syndrome: A Literature Review. Journal of Clinical Medicine. 2023; 12(23):7275. https://doi.org/10.3390/jcm12237275
Chicago/Turabian StyleGall, Emmanuel, Donia Mafi, Tahar Ghannam, Pierre Brami, Vincent Pham, Olivier Varenne, and Fabien Picard. 2023. "Percutaneous Coronary Intervention in Out-of-Hospital Cardiac Arrest Related to Acute Coronary Syndrome: A Literature Review" Journal of Clinical Medicine 12, no. 23: 7275. https://doi.org/10.3390/jcm12237275