
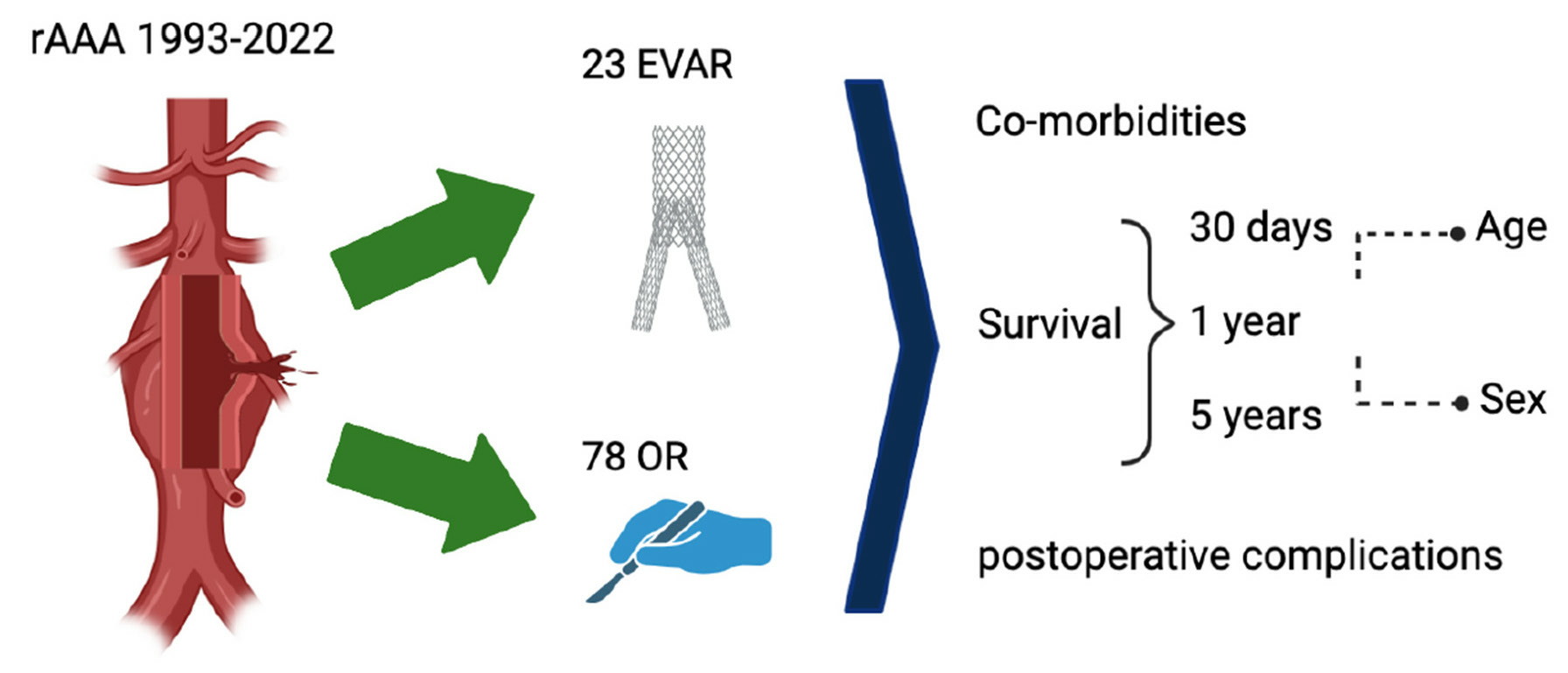
The Comparison of Endovascular and Open Surgical Treatment for Ruptured Abdominal Aortic Aneurysm in Terms of Safety and Efficacy on the Basis of a Single-Center 30-Year Experience
 ,
,  , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics/Emergency Room/Co-Morbidities
3.2. Procedural Parameters
3.3. Postoperative Complications
3.4. Patient Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golledge, J.; Muller, J.; Daugherty, A.; Norman, P. Abdominal aortic aneurysm: Pathogenesis and implications for management. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2605–2613. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Zhao, J.; Chen, X.; Wang, J.; Ma, Y.; Huang, B.; Yuan, D.; Du, X. Systematic review and meta-analysis of sex differences in outcomes after endovascular aneurysm repair for infrarenal abdominal aortic aneurysm. J. Vasc. Surg. 2020, 71, 283–296. [Google Scholar] [CrossRef]
- Reimerink, J.J.; van der Laan, M.J.; Koelemay, M.J.; Balm, R.; A Legemate, D. Systematic review and meta-analysis of population-based mortality from ruptured abdominal aortic aneurysm. Br. J. Surg. 2013, 100, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Karthikesalingam, A.; Holt, P.J.; Vidal-Diez, A.; Ozdemir, B.A.; Poloniecki, J.D.; Hinchliffe, R.J.; Thompson, M.M. Mortality from ruptured abdominal aortic aneurysms: Clinical lessons from a comparison of outcomes in England and the USA. Lancet 2014, 383, 963–969. [Google Scholar] [CrossRef]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice-European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef]
- Greenhalgh, R.M. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: Randomised controlled trial. Lancet 2004, 364, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Participants, U.S.A.T.; Powell, J. Final 12-year follow-up of surgery versus surveillance in the UK Small Aneurysm Trial. Br. J. Surg. 2007, 94, 702–708. [Google Scholar] [CrossRef]
- Patel, R.; Sweeting, M.J.; Powell, J.T.; Greenhalgh, R.M. Endovascular versus open repair of abdominal aortic aneurysm in 15-year follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): A randomised controlled trial. Lancet 2016, 388, 2366–2374. [Google Scholar] [CrossRef]
- Kühnl, A.; Erk, A.; Trenner, M.; Salvermoser, M.; Schmid, V.; Eckstein, H.-H. Incidence, treatment and mortality in patients with abdominal aortic aneurysms. Dtsch. Arztebl. Int. 2017, 114, 391–398. [Google Scholar] [CrossRef]
- IMPROVE Trial Investigators; Braithwaite, B.; Cheshire, N.J.; Greenhalgh, R.M.; Grieve, R.; Hassan, T.B.; Hinchliffe, R.; Howell, S.; Moore, F.; Nicholson , A.A.; et al. Endovascular strategy or open repair for ruptured abdominal aortic aneurysm: One-year outcomes from the IMPROVE randomised trial. Eur. Heart J. 2015, 36, 2061–2069. [Google Scholar]
- McPhee, J.; Eslami, M.H.; Arous, E.J.; Messina, L.M.; Schanzer, A. Endovascular treatment of ruptured abdominal aortic aneurysms in the United States (2001–2006): A significant survival benefit over open repair is independently associated with increased institutional volume. J. Vasc. Surg. 2009, 49, 817–826. [Google Scholar] [CrossRef]
- Stather, P.; Sidloff, D.; Rhema, I.; Choke, E.; Bown, M.; Sayers, R. A review of current reporting of abdominal aortic aneurysm mortality and prevalence in the literature. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, M.J.; Ulug, P.; Powell, J.T.; Desgranges, P.; Balm, R.; Trialists, R.A. Ruptured aneurysm trials: The importance of longer-term outcomes and meta-analysis for 1-year mortality. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Feng, J.; Li, H.; Zhang, Y.; Lu, Q.; Jing, Z. Open surgery (OS) versus endovascular aneurysm repair (EVAR) for haemodynamically stable and unstable ruptured abdominal aortic aneurysm (rAAA). Heart Vessels 2016, 31, 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Alsusa, H.; Shahid, A.; Antoniou, G.A. A comparison of endovascular versus open repair for ruptured abdominal aortic aneurysm-Meta-analysis of propensity score-matched data. Vascular 2022, 30, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Kontopodis, N.; Galanakis, N.; Antoniou, S.A.; Tsetis, D.; Ioannou, C.V.; Veith, F.J.; Powell, J.T.; Antoniou, G.A. Meta-Analysis and Meta-Regression Analysis of Outcomes of Endovascular and Open Repair for Ruptured Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 399–410. [Google Scholar] [CrossRef]
- Wang, L.J.; Locham, S.; Al-Nouri, O.; Eagleton, M.J.; Clouse, W.D.; Malas, M.B. Endovascular repair of ruptured abdominal aortic aneurysm is superior to open repair: Propensity-matched analysis in the Vascular Quality Initiative. J. Vasc. Surg. 2020, 72, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Kontopodis, N.; Galanakis, N.; Ioannou, C.V.; Tsetis, D.; Becquemin, J.-P.; Antoniou, G.A. Time-to-event data meta-analysis of late outcomes of endovascular versus open repair for ruptured abdominal aortic aneurysms. J. Vasc. Surg. 2021, 74, 628–638. [Google Scholar] [CrossRef]
- Wanken, Z.J.; Barnes, J.A.; Trooboff, S.W.; Columbo, J.A.; Jella, T.K.; Kim, D.J.; Khoshgowari, A.; Riblet, N.B.; Goodney, P.P. A systematic review and meta-analysis of long-term reintervention after endovascular abdominal aortic aneurysm repair. J. Vasc. Surg. 2020, 72, 1122–1131. [Google Scholar] [CrossRef]
- Deery, S.E.; O’Donnell, T.F.; Bodewes, T.C.; Dalebout, B.A.; Pothof, A.B.; Shean, K.E.; Darling, J.D.; Schermerhorn, M.L. Early reintervention after open and endovascular abdominal aortic aneurysm repair is associated with high mortality. J. Vasc. Surg. 2018, 67, 433–440. [Google Scholar] [CrossRef]
- Çetinkaya, F.; İşcan, H.Z.; Türkçü, M.A.; Mavioğlu, H.L.; Ünal, E.U. Predictive Parameters of Type 1A Endoleak for Elective Endovascular Aortic Repair: A Single-Center Experience. Ann. Vasc. Surg. 2023. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Lookstein, R.A. Predictive Factors for the Development of Type 2 Endoleak Following Endovascular Aneurysm Repair. Semin. Interv. Radiol. 2015, 32, 272–277. [Google Scholar]
- Sawang, M.; Paravastu, S.C.; Liu, Z.; Thomas, S.D.; Beiles, C.B.; Mwipatayi, B.P.; Verhagen, H.J.; Verhoeven, E.L.; Varcoe, R.L. The Relationship Between Operative Volume and Peri-operative Mortality After Non-elective Aortic Aneurysm Repair in Australia. Eur. J. Vasc. Endovasc. Surg. 2020, 60, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Greenleaf, E.K.; Hollenbeak, C.S.; Aziz, F. Outcomes after ruptured abdominal aortic aneurysm repair in the era of centralized care. J. Vasc. Surg. 2020, 71, 1148–1161. [Google Scholar] [CrossRef] [PubMed]
- Wise, E.S.; Hocking, K.M.; Brophy, C.M. Prediction of in-hospital mortality after ruptured abdominal aortic aneurysm repair using an artificial neural network. J. Vasc. Surg. 2015, 62, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Landahl, S.; Bengtsson, C.; A Sigurdsson, J.; Svanborg, A.; Svärdsudd, K. Age-related changes in blood pressure. Hypertension 1986, 8, 1044–1049. [Google Scholar] [CrossRef]
- Peverill, R.E. Changes in left ventricular size, geometry, pump function and left heart pressures during healthy aging. Rev. Cardiovasc. Med. 2021, 22, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Kohn, J.C.; Lampi, M.C.; Reinhart-King, C.A. Age-related vascular stiffening: Causes and consequences. Front. Genet. 2015, 6, 112. [Google Scholar] [CrossRef] [PubMed]
- Raats, J.W.; Flu, H.C.; Ho, G.H.; Veen, E.J.; Vos, D.; van der Laan, L.; Steyerberg, E.W. Long-term outcome of ruptured abdominal aortic aneurysm: Impact of treatment and age. Clin. Interv. Aging 2014, 9, 1721–1732. [Google Scholar] [CrossRef]
- Shahidi, S.; Schroeder, T.V.; Carstensen, M.; Sillesen, H. Outcome and survival of patients aged 75 years and older compared to younger patients after ruptured abdominal aortic aneurysm repair: Do the results justify the effort? Ann. Vasc. Surg. 2009, 23, 469–477. [Google Scholar] [CrossRef]
- Svensjo, S.; Bjorck, M.; Wanhainen, A. Current prevalence of abdominal aortic aneurysm in 70-year-old women. Br. J. Surg. 2013, 100, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Aneurysm Screening Study Group (CASS Group); Chichester Aneurysm Screening Group (UK); Viborg Aneurysm Screening Study (Denmark); Western Australia Abdominal Aortic Aneurysm Program (Australia); Multicentre Aneurysm Screening Study (MASS) (UK). A comparative study of the prevalence of abdominal aortic aneurysms in the United Kingdom, Denmark, and Australia. J. Med. Screen. 2001, 8, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, R.; Goldie, V.J.; Kelman, J.; Dawson, A.R.W.; A Murie, J.; A Chalmers, R.T. Influence of sex on expansion rate of abdominal aortic aneurysms. Br. J. Surg. 2007, 94, 310–314. [Google Scholar] [CrossRef] [PubMed]
- United Kingdom Small Aneurysm Trial Participants. Long-term outcomes of immediate repair compared with surveillance of small abdominal aortic aneurysms. N. Engl. J. Med. 2002, 346, 1445–1452. [Google Scholar] [CrossRef]
- Mureebe, L.; Egorova, N.; McKinsey, J.F.; Kent, K.C. Gender trends in the repair of ruptured abdominal aortic aneurysms and outcomes. J. Vasc. Surg. 2010, 51 (Suppl. S4), 9S–13S. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.M.; Adam, D.J.; Bradbury, A.W. The influence of gender on outcome after ruptured abdominal aortic aneurysm. J. Vasc. Surg. 2000, 32, 258–262. [Google Scholar] [CrossRef]
- Li, B.; Eisenberg, N.; Witheford, M.; Lindsay, T.F.; Forbes, T.L.; Roche-Nagle, G. Sex differences in outcomes following ruptured abdominal aortic aneurysm repair. JAMA Netw. Open 2022, 5, e221133. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Open Repair (OR) Median ± SD (Min–Max) or Absolute Frequency (%) (n = 14) | Odds Ratio (95% CI) | p Value | Endovascular Aortic Repair (EVAR) Mean ± SD (Min–Max) or Absolute Frequency (%) (n = 23) | Odds Ratio (95% CI) | p Value | |
|---|---|---|---|---|---|---|
| Baseline parameters | ||||||
| Age (years) | 70.07 ± 9.1 (56–85) | 1.045 (0.925, 1.199) | 0.481 | 76.78 ± 10.2 (58–93) | 1.078 (0.980, 1.215) | 0.128 |
| Gender, female (n) | 4 (28.6) | 0.333 (0.014, 3.718) | 0.383 | 5 (21.7) | 0.577 (0.073, 4.550) | 0.606 |
| max. AAA diameter, (mm) | 78.9 ± 20.4 (45–123) | 1.014 (0.960, 1.083) | 0.615 | 67.7 ± 23.0 (22–130) | 1.020 (0.980, 1.069) | 0.340 |
| Emergency room (ER) | ||||||
| Unconsciousness in ER (n) | 3 (21.4) | - | - | 5 (21.7) | 0.500 (0.023, 4.408) | 0.555 |
| Heart rate in the ER (beats/min) | 95.6 ± 17.8 (66–121) | 0.992 (0.923, 1.063) | 0.808 | 96.8 ± 21.3 (59–135) | 0.985 (0.937, 1.031) | 0.507 |
| Preoperative systolic blood pressure, (mmHg) | 118 ± 27.9 (80–165) | 1.009 (0.966, 1.061) | 0.674 | 120.1 ± 27.3 (85–170) | 0.968 (0.918, 1.006) | 0.106 |
| Preoperative blood transfusion, (n) | 18.3 ± 18.1 (1–67) | 1.081 (0.992, 1.264) | 0.087 | 7.5 ± 8.7 | 1.040 (0.934, 1.174) | 0.451 |
| Serum creatinine (mg/dL) | 1.3 (0.64–2.4) | 6.495 (0.526, 312.0) | 0.155 | 1.3 ± 1.1 (0.4–5.75) | 0.808 (0.157, 1.955) | 0.669 |
| Co-morbidities | ||||||
| History of myocardial Infarction | 1 (7.1) | - | - | 1 (4.3) | - | - |
| CHD | 4 (28.6) | 0.667 (0.057, 7.548) | 0.733 | 6 (26.1) | 3.250 (0.449, 25.10) | 0.237 |
| PAOD | 3 (21.4) | 1.667 (0.121, 42.430) | 0.708 | 5 (21.7) | 0.500 (0.023, 4.408) | 0.555 |
| aHT | 9 (64.3) | - | - | 20 (87.0) | 0.167 (0.007, 2.096) | 0.162 |
| Smoking | 3 (21.4) | 0.286 (0.011, 3.931) | 0.348 | 4 (17.4) | - | - |
| Hyperlipidaemia | 1 (7.1) | - | - | 12 (52.2) | 0.240 (0.028, 1.503) | 0.130 |
| Pulmonary disease | 3 (21.4) | 1.667 (0.121, 42.430) | 0.708 | 6 (26.1) | 1.200 (0.135, 8.559) | 0.858 |
| Cerebrovascular disease | 2 (14.3) | - | - | 4 (17.4) | - | - |
| History of stroke or transient ischemic attack | 1 (7.1) | - | - | 4 (17.4) | - | - |
| CKD w/o dialysis | 3 (21.4) | 1.667 (0.121, 42.430) | 0.708 | 5 (21.7) | 5.250 (0.659, 52.510) | 0.116 |
| T2DM | 1 (7.1) | - | - | 2 (8.7) | - | - |
| Treatment-specific parameter | ||||||
| Local anaesthesia (n) | -# | -# | 10 (43.5) | 0.964 (0.160, 5.795) | 0.968 |
| Open Repair (OR) (n = 14) | Endovascular Aortic Repair (EVAR) (n = 23) | p Value | |
|---|---|---|---|
| Operation time (min) | 242.4 ± 81.8 (132–458) | 178.4 ± 121.2 (69–510) | 0.09 |
| Blood loss in (mL), | 3700 ± 2462 (1300–6800) | 915 ± 827 (330–1500) | 0.184 |
| ICU stay (days) | 6.1 ± 5.4 (0–15) | 6.5 ± 6.2 (0–19) | 0.824 |
| 30-day mortality (n) | 7 (50.0) | 2 (8.7) | 0.023 |
| In-hospital mortality (n) | 8 (57.1) | 3 (13.0) | 0.008 |
| In-hospital stay (days) | 14.5 ± 23.8 (1–95) | 16.6 ± 13.6 (1–48) | 0.738 |
| Open Repair (OR) (n = 14) | Endovascular Aortic Repair (EVAR) (n = 18) | p Value | |
|---|---|---|---|
| Overall | 10 (71.4) | 18 (78.3) | |
| Grade I (n) | 0 | 6 (26.1) | 0.65 |
| Type II endoleak (n = 3), respiratory insufficiency (n = 1), lymph fistula (n = 1), myocardial infarction (n = 1), tachyarrhythmia (n = 1), aortic syndrome with aortic intramural haematoma (n = 1) | |||
| Grade II (n) | 1 (7.1) | 2 (8.7) | 1.0 |
| Nosocomial pneumonia | Lymph fistula (n = 1), bradyarrhythmia (n = 1), cardiac arrhythmia (n = 1), acute renal failure (n = 1) | ||
| Grade III (n) | 0 | 3 (13.0) | 0.275 |
| Lymph fistula (n = 1), wound infection (n = 2), bleeding femoral artery (n = 1), type II endoleak (n = 1), pleural effusion (n = 1), retroperitoneal haematoma (n = 1) | |||
| Grade IV (n) | 2 (14.3) | 4 (17.4) | 1.0 |
| Respiratory insufficiency with pneumonia (n = 2), tracheotomy (n = 1), acute renal failure (n = 1), burst abdomen (n = 1) | Acute renal failure (n = 2), dialysis (n = 2), myocardial infarction (n = 1), type Ia endoleak with revision and OR (n = 1), respiratory insufficiency with pneumonia (n = 2), arrhythmia (n = 1), tracheotomy (n = 1) | ||
| Grade V (n) | 7 (50) | 3 (13.0) | 0.023 |
| Cardiac arrest (n = 1), pulmonary embolism (n = 1), acute mesenteric ischemia (n = 2), bleeding (n = 2), splenectomy because of bleeding (n = 1), pneumonia (n = 1), sepsis (n = 3). acute limb ischemia (n = 1), leriche syndrome (n = 1), multiple-organ dysfunction (n = 5), respiratory insufficiency (n = 2), dialysis (n = 2) | Reintervention (n = 3), bypass (n = 1), limb ischemia (n = 1), respiratory insufficiency (n = 3), acute renal failure (n = 3), multi-organ dysfunction (n = 3), type 1 endoleak (n = 1), type III endoleak, rupture iliac artery (n = 1), bleeding (n = 2), infection of retroperitoneal haematoma (n = 1), spondylodiscitis (n = 1) |
| Type of Endoleak | Endovascular Aortic Repair (EVAR) (n = 23) | Odds Ratio (95% CI) (Cox Regression) | p-Value |
|---|---|---|---|
| No EL (n) | 15 (65.2) | 0.392 (0.086, 1.779) | 0.225 |
| EL (n) | 8 (34.8) | 2.553 (0.562, 11.599) | 0.225 |
| Type II EL (n) | 5 (21.7) | 1.140 (0.209, 6.208) | 0.880 |
| Type I and type III EL (n) | 3 (13.0) | 4.883 (0.809, 29.473) | 0.084 |
| Re-intervention (n) | 7 (30.4) | 10.608 (1.156, 97.335) | 0.037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duran, M.; Arnautovic, A.; Kilic, C.; Rembe, J.-D.; Mulorz, J.; Schelzig, H.; Wagenhäuser, M.U.; Garabet, W. The Comparison of Endovascular and Open Surgical Treatment for Ruptured Abdominal Aortic Aneurysm in Terms of Safety and Efficacy on the Basis of a Single-Center 30-Year Experience. J. Clin. Med. 2023, 12, 7186. https://doi.org/10.3390/jcm12227186
Duran M, Arnautovic A, Kilic C, Rembe J-D, Mulorz J, Schelzig H, Wagenhäuser MU, Garabet W. The Comparison of Endovascular and Open Surgical Treatment for Ruptured Abdominal Aortic Aneurysm in Terms of Safety and Efficacy on the Basis of a Single-Center 30-Year Experience. Journal of Clinical Medicine. 2023; 12(22):7186. https://doi.org/10.3390/jcm12227186
Chicago/Turabian StyleDuran, Mansur, Amir Arnautovic, Cem Kilic, Julian-Dario Rembe, Joscha Mulorz, Hubert Schelzig, Markus Udo Wagenhäuser, and Waseem Garabet. 2023. "The Comparison of Endovascular and Open Surgical Treatment for Ruptured Abdominal Aortic Aneurysm in Terms of Safety and Efficacy on the Basis of a Single-Center 30-Year Experience" Journal of Clinical Medicine 12, no. 22: 7186. https://doi.org/10.3390/jcm12227186