
Optimal Lymphadenectomy in Patients with Well-Differentiated Nonfunctioning Pancreatic Neuroendocrine Neoplasms
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgical Procedures
2.3. LN Stations
2.4. Frequency of LNM at Each Station according to the Tumor Site
2.5. Postoperative Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinicopathological Characteristics
3.2. Frequency of LNM at Each Station according to the Tumor Site
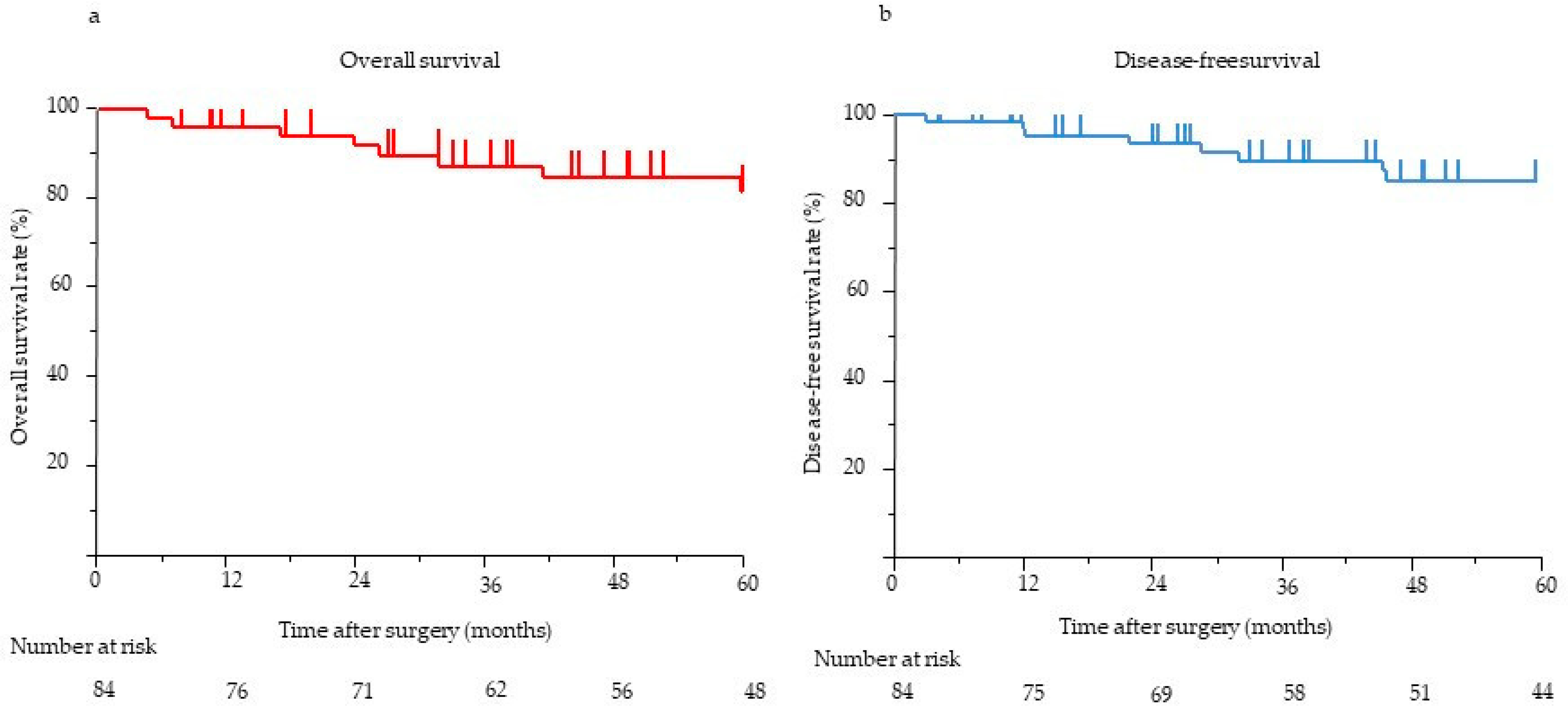
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuo, E.J.; Salem, R.R. Population-level analysis of pancreatic neuroendocrine tumors 2 cm or less in size. Ann. Surg. Oncol. 2013, 20, 2815–2821. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Talamonti, M.S.; Tomlinson, J.S.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y.; Bentrem, D.J. Prognostic score predicting survival after resection of pancreatic neuroendocrine tumors: Analysis of 3851 patients. Ann. Surg. 2008, 247, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Franko, J.; Feng, W.; Yip, L.; Genovese, E.; Moser, A.J. Non-functional neuroendocrine carcinoma of the pancreas: Incidence, tumor biology, and outcomes in 2158 patients. J. Gastrointest. Surg. 2016, 14, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Sandvik, O.M.; Søreide, K.; Gudlaugsson, E.; Kvaløy, J.T.; Søreide, J.A. Epidemiology and classification of gastroenteropancreatic neuroendocrine neoplasms using current coding criteria. Br. J. Surg. 2016, 103, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, D.J.; Turrini, O.; Ewald, J.; Barbier, L.; Autret, A.; Hardwigsen, J.; Brunet, C.; Moutardier, V.; Le Treut, Y.P.; Delpero, J.R. Pancreatic neuroendocrine tumor: A multivariate analysis of factors influencing survival. Eur. J. Surg. Oncol. 2014, 40, 1564–1571. [Google Scholar] [CrossRef]
- Lindner, K.; Binte, D.; Hoeppner, J.; Wellner, U.F.; Schulte, D.M.; Schmid, S.M.; Luley, K.; Buchmann, I.; Tharun, L.; Keck, T.; et al. Resection of non-functional pancreatic neuroendocrine neoplasms-a single-center retrospective outcome analysis. Curr. Oncol. 2021, 28, 3071–3080. [Google Scholar] [CrossRef]
- Gao, Y.; Gao, H.; Wang, G.; Yin, L.; Xu, W.; Peng, Y.; Wu, J.; Jiang, K.; Miao, Y. A meta-analysis of prognostic factor of pancreatic neuroendocrine neoplasms. Sci. Rep. 2018, 8, 7271. [Google Scholar] [CrossRef]
- Norton, J.A.; Kivlen, M.; Li, M.; Schneider, D.; Chuter, T.; Jensen, R.T. Morbidity and mortality of aggressive resection in patients with advanced neuroendocrine tumors. Arch. Surg. 2003, 138, 859–866. [Google Scholar] [CrossRef]
- Partelli, S.; Gaujoux, S.; Boninsegna, L.; Cherif, R.; Crippa, S.; Couvelard, A.; Scarpa, A.; Ruszniewski, P.; Sauvanet, A.; Falconi, M. Pattern and clinical predictors of lymph node involvement in nonfunctioning pancreatic neuroendocrine tumors (NF-PanNETs). JAMA Surg. 2013, 148, 932–939. [Google Scholar] [CrossRef]
- Tanaka, M.; Heckler, M.; Mihaljevic, A.L.; Probst, P.; Klaiber, U.; Heger, U.; Schimmack, S.; Büchler, M.W.; Hackert, T. Systematic review and metaanalysis of lymph node metastases of resected pancreatic neuroendocrine tumors. Ann. Surg. Oncol. 2021, 28, 1614–1624. [Google Scholar] [CrossRef]
- Andreasi, V.; Ricci, C.; Partelli, S.; Guarneri, G.; Ingaldi, C.; Muffatti, F.; Crippa, S.; Casadei, R.; Falconi, M. Predictors of disease recurrence after curative surgery for nonfunctioning pancreatic neuroendocrine neoplasms (NF-PanNENs): A systematic review and meta-analysis. J. Endocrinol. Investig. 2022, 45, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Genç, C.G.; Falconi, M.; Partelli, S.; Muffatti, F.; van Eeden, S.; Doglioni, C.; Klümpen, H.J.; van Eijck, C.H.J.; Nieveen van Dijkum, E.J.M. Recurrence of pancreatic neuroendocrine tumors and survival predicted by Ki67. Ann. Surg. Oncol. 2018, 25, 2467–2474. [Google Scholar] [CrossRef]
- Nanno, Y.; Matsumoto, I.; Zen, Y.; Otani, K.; Uemura, J.; Toyama, H.; Asari, S.; Goto, T.; Ajiki, T.; Okano, K.; et al. Pancreatic duct involvement in well-differentiated neuroendocrine tumors is an independent poor prognostic factor. Ann. Surg. Oncol. 2017, 24, 1127–1133. [Google Scholar] [CrossRef]
- Ricci, C.; Partelli, S.; Landoni, L.; Rinzivillo, M.; Ingaldi, C.; Andreasi, V.; Nessi, C.; Muffatti, F.; Fontana, M.; Tamburrino, D.; et al. Sporadic non-functioning pancreatic neuroendocrine tumours: Multicentre analysis. Br. J. Surg. 2021, 108, 811–816. [Google Scholar] [CrossRef]
- Falconi, M.; Bartsch, D.K.; Eriksson, B.; Klöppel, G.; Lopes, J.M.; O’Connor, J.M.; Salazar, R.; Taal, B.G.; Vullierme, M.P.; O’Toole, D.; et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: Well-differentiated pancreatic non-functioning tumors. Neuroendocrinology 2012, 95, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Howe, J.R.; Merchant, N.B.; Conrad, C.; Keutgen, X.M.; Hallet, J.; Drebin, J.A.; Minter, R.M.; Lairmore, T.C.; Tseng, J.F.; Zeh, H.J.; et al. The North American Neuroendocrine Tumor Society consensus paper on the surgical management of pancreatic neuroendocrine tumors. Pancreas 2020, 49, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Partelli, S.; Bartsch, D.K.; Capdevila, J.; Chen, J.; Knigge, U.; Niederle, B.; Nieveen van Dijkum, E.J.M.; Pape, U.F.; Pascher, A.; Ramage, J.; et al. ENETS Consensus Guidelines for standard of care in neuroendocrine tumours: Surgery for small intestinal and pancreatic neuroendocrine tumours. Neuroendocrinology 2017, 105, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.; Bergmann, F.; Schimmack, S.; Hinz, U.; Prieß, S.; Müller-Stich, B.P.; Werner, J.; Hackert, T.; Büchler, M.W. Outcome of surgery for pancreatic neuroendocrine neoplasms. Br. J. Surg. 2014, 101, 1405–1412. [Google Scholar] [CrossRef]
- Tan, Q.Q.; Wang, X.; Yang, L.; Chen, Y.H.; Tan, C.L.; Zhu, X.M.; Ke, N.W.; Liu, X.B. Analysis of recurrence after resection of well-differentiated non-functioning pancreatic neuroendocrine tumors. Medicine 2020, 99, e20324. [Google Scholar] [CrossRef]
- Shah, M.H.; Goldner, W.S.; Halfdanarson, T.R.; Bergsland, E.; Berlin, J.D.; Halperin, D.; Chan, J.; Kulke, M.H.; Benson, A.B.; Blaszkowsky, L.S.; et al. NCCN guidelines insights: Neuroendocrine and adrenal tumors, version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 693–702. [Google Scholar] [CrossRef]
- Ito, T.; Masui, T.; Komoto, I.; Doi, R.; Osamura, R.Y.; Sakurai, A.; Ikeda, M.; Takano, K.; Igarashi, H.; Shimatsu, A.; et al. JNETS clinical practice guidelines for gastroenteropancreatic neuroendocrine neoplasms: Diagnosis, treatment, and follow-up: A synopsis. J. Gastroenterol. 2021, 56, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Umeda, Y.; Yoshida, R.; Yoshida, K.; Fuji, T.; Kumano, K.; Yasui, K.; Yagi, T.; Fujiwara, T. Prognostic value of the regional lymph node station in pancreatic neuroendocrine tumor. Anticancer Res. 2022, 42, 2797–2801. [Google Scholar] [CrossRef] [PubMed]
- Masui, T.; Sato, A.; Nakano, K.; Uchida, Y.; Yogo, A.; Anazawa, T.; Nagai, K.; Kawaguchi, Y.; Takaori, K.; Uemoto, S. Predictive value of the Ki67 index for lymph node metastasis of small non-functioning pancreatic neuroendocrine neoplasms. Surg. Today 2019, 49, 593–600. [Google Scholar] [CrossRef]
- Tol, J.A.; Gouma, D.J.; Bassi, C.; Dervenis, C.; Montorsi, M.; Adham, M.; Andrén-Sandberg, A.; Asbun, H.J.; Bockhorn, M.; Büchler, M.W.; et al. Definition of a standard lymphadenectomy in surgery for pancreatic ductal adenocarcinoma: A consensus statement by the International Study Group on Pancreatic Surgery (ISGPS). Surgery 2014, 156, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.; Uemura, K.; Sumiyoshi, T.; Kondo, N.; Okada, K.; Otsuka, H.; Murakami, Y.; Takahashi, S. Optimal lymph-node dissection for pancreatic tail cancer. Surg. Today 2022, 52, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Partelli, S.; Javed, A.A.; Andreasi, V.; He, J.; Muffatti, F.; Weiss, M.J.; Sessa, F.; La Rosa, S.; Doglioni, C.; Zamboni, G.; et al. The number of positive nodes accurately predicts recurrence after pancreaticoduodenectomy for nonfunctioning neuroendocrine neoplasms. Eur. J. Surg. Oncol. 2018, 44, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Trikalinos, N.A.; Tan, B.R.; Amin, M.; Liu, J.; Govindan, R.; Morgensztern, D. Effect of metastatic site on survival in patients with neuroendocrine neoplasms (NENs). An analysis of SEER data from 2010 to 2014. BMC Endocr. Disord. 2020, 20, 44. [Google Scholar] [CrossRef]
- Sallinen, V.J.; Le Large, T.Y.S.; Tieftrunk, E.; Galeev, S.; Kovalenko, Z.; Haugvik, S.P.; Antila, A.; Franklin, O.; Martinez-Moneo, E.; Robinson, S.M.; et al. Prognosis of sporadic resected small (≤2 cm) nonfunctional pancreatic neuroendocrine tumors—A multi-institutional study. HPB 2018, 20, 251–259. [Google Scholar] [CrossRef]
- Marchegiani, G.; Landoni, L.; Andrianello, S.; Masini, G.; Cingarlini, S.; D’Onofrio, M.; De Robertis, R.; Davì, M.; Capelli, P.; Manfrin, E.; et al. Patterns of recurrence after resection for pancreatic neuroendocrine tumors: Who, when, and where? Neuroendocrinology 2019, 108, 161–171. [Google Scholar] [CrossRef]
- Kunz, P.L.; Reidy-Lagunes, D.; Anthony, L.B.; Bertino, E.M.; Brendtro, K.; Chan, J.A.; Chen, H.; Jensen, R.T.; Kim, M.K.; Klimstra, D.S.; et al. Consensus guidelines for the management and treatment of neuroendocrine tumors. Pancreas 2013, 42, 557–577. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age, median (IQR), years | 71.2 (39–82) |
| Sex | |
| Male/female | 49 (58%)/35 (42%) |
| BMI, median (IQR), kg/m2 | 22.8 (15.7–32.6) |
| Tumor location | |
| Head/body/tail | 32 (38%)/20 (24%)/32 (38%) |
| Procedure | |
| Standard surgery | 59 (71%) |
| PD/DP/TP | 32 (38%)/27 (33%)/0 (0%) |
| PSR | 25 (29%) |
| MP/SPDP/enucleation | 12 (14%)/12 (14%)/1 (1%) |
| Main pancreatic duct, median (IQR), mm | 2.0 (1–13) |
| Pathological tumor diameter, median (IQR), mm | 10.0 (3–90) |
| R0 rate | |
| R0/R1/R2 | 79 (94%)/5 (6%)/0 (0%) |
| Lymph node metastasis | |
| Yes/No | 10 (12%)/74 (88%) |
| Lymphatic invasion | |
| Yes/No | 11 (14%)/66 (86%) |
| Venous invasion | |
| Yes/No | 19 (25%)/58 (75%) |
| Perineural invasion | |
| Yes/No | 17 (20%)/66 (80%) |
| Ki-67 (%), median (IQR) | 1.3 (0–50) |
| WHO classification | |
| G1/G2/G3 | 48 (57%)/32 (38%)/3 (5%) |
| Follow-up, median (IQR), months | 58.1 (range, 0.5–275.3) |
| Pancreatic Head (n = 32) | Pancreatic Body and Tail (n = 52) | |||
|---|---|---|---|---|
| Number of Patients with LNM/Number of Patients with LNs Detected in the Resected Specimen | Total Number of Metastasized LNs/Total Number of Harvested LNs | Number of Patients with LNM/Number of Patients with LNs Detected in the Resected Specimen | Total Number of Metastasized LNs/total Number of Harvested LNs | |
| Station 5 | 0/26 (0%) | 0/38 (0%) | NA | NA |
| Station 6 | 0/30 (0%) | 0/42 (0%) | NA | NA |
| Station 7 | 0/4 (0%) | 0/7 (0%) | 0/29 (0%) | 0/39 (0%) |
| Station 8 | 1/32 (3.1%) | 1/51 (2.0%) | 0/37 (0%) | 0/52 (0%) |
| Station 9 | 0/2 (0%) | 0/4 (0%) | 0/19 (0%) | 0/28 (0%) |
| Station 10 | NA | NA | 0/29 (0%) | 0/44 (0%) |
| Station 11 | NA | NA | 2/39 (5.1%) | 3/132 (2.2%) |
| Station 12 | 0/27 (0%) | 0/38 (0%) | NA | NA |
| Station 13 | 4/32 (12.5%) | 7/71 (9.8%) | NA | NA |
| Station 14 | 0/30 (0%) | 0/72 (0%) | 0/23 (0%) | 0/36 (0%) |
| Station 17 | 3/32 (9.3%) | 3/82 (3.6%) | NA | NA |
| Station 18 | NA | NA | 0/37 (0%) | 0/52 (0%) |
| Factor | DFS | OS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | ||||||||||
| No. | Five-Year Survival Rate (%) | Median DFS (Months) | p Value | HR | 95% CI | p Value | Five-Year Survival Rate (%) | Median OS (Months) | p Value | HR | 95% CI | p Value | |
| Sex | |||||||||||||
| Male | 49 (58%) | 88.2 | NA | 0.805 | 86.0 | NA | 0.657 | ||||||
| Female | 35 (42%) | 87.1 | NA | 90.9 | NA | ||||||||
| Tumor location | |||||||||||||
| Head | 32 (38%) | 85.7 | NA | 0.884 | 76.3 | NA | 0.183 | ||||||
| Body, tail | 52 (62%) | 87.2 | NA | 94.5 | NA | ||||||||
| Main pancreatic duct diameter | |||||||||||||
| ≥5 mm | 13 (15%) | 77.8 | NA | 0.115 | 63.5 | 142.6 | 0.001 | 6.34 | 0.34–111.5 | 0.192 | |||
| <5 mm | 70 (85%) | 89.6 | NA | 95.7 | NA | 1.0 | |||||||
| Pathological tumor size | |||||||||||||
| >20 mm | 19 (23%) | 67.3 | NA | <0.001 | 1.32 | 0.074–23.64 | 0.848 | 85.3 | 142.6 | 0.481 | |||
| ≤20 mm | 65 (77%) | 97.8 | NA | 1.0 | 91.2 | NA | |||||||
| R1 | |||||||||||||
| Yes | 5 (6%) | 30.1 | 32.2 | <0.001 | 2.67 | 0.44–16.2 | 0.283 | 80.0 | 113.4 | 0.018 | 16.3 | 0.0015–2.48 | 0.104 |
| No | 79 (94%) | 91.4 | NA | 1.0 | 88.1 | NA | 1.0 | ||||||
| Lymph node metastasis | |||||||||||||
| Yes | 10 (12%) | 26.7 | 32.2 | <0.001 | 14.06 | 1.16–169.9 | 0.012 | 76.1 | 87.57 | <0.001 | 108.5 | 1.94–6046.2 | 0.005 |
| No | 74 (88%) | 96.1 | NA | 1.0 | 88.9 | NA | 1.0 | ||||||
| Lymphatic invasion | |||||||||||||
| Yes | 11 (14%) | 78.5 | NA | 0.312 | 90.0 | NA | 0.208 | ||||||
| No | 66 (86%) | 86.0 | NA | 95.7 | NA | ||||||||
| Venous invasion | |||||||||||||
| Yes | 19 (25%) | 51.6 | NA | <0.001 | 3.1 | 0.21–44.8 | 0.357 | 87.4 | 113.4 | <0.001 | 1.01 | 0.019–51.74 | 0.995 |
| No | 58 (75%) | 97.9 | NA | 1.0 | 97.4 | NA | 1.0 | ||||||
| Perineural invasion | |||||||||||||
| Yes | 17 (20%) | 83.0 | NA | 0.704 | 85.5 | NA | 0.952 | ||||||
| No | 66 (80%) | 87.6 | NA | 87.9 | NA | ||||||||
| WHO classification of specimens | |||||||||||||
| G1 | 48 (58%) | 72.3 | NA | 0.002 | 1.0 | 86.4 | NA | 0.027 | 1.0 | ||||
| G2, G3 | 35 (42%) | 50.0 | NA | 8.04 | 0.83–77.9 | 0.076 | 60.2 | NA | 3.71 | 0.043–313.0 | 0.560 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shintakuya, R.; Uemura, K.; Sumiyoshi, T.; Okada, K.; Baba, K.; Harada, T.; Murakami, Y.; Serikawa, M.; Ishii, Y.; Arihiro, K.; et al. Optimal Lymphadenectomy in Patients with Well-Differentiated Nonfunctioning Pancreatic Neuroendocrine Neoplasms. J. Clin. Med. 2023, 12, 6778. https://doi.org/10.3390/jcm12216778
Shintakuya R, Uemura K, Sumiyoshi T, Okada K, Baba K, Harada T, Murakami Y, Serikawa M, Ishii Y, Arihiro K, et al. Optimal Lymphadenectomy in Patients with Well-Differentiated Nonfunctioning Pancreatic Neuroendocrine Neoplasms. Journal of Clinical Medicine. 2023; 12(21):6778. https://doi.org/10.3390/jcm12216778
Chicago/Turabian StyleShintakuya, Ryuta, Kenichiro Uemura, Tatsuaki Sumiyoshi, Kenjiro Okada, Kenta Baba, Takumi Harada, Yoshiaki Murakami, Masahiro Serikawa, Yasutaka Ishii, Koji Arihiro, and et al. 2023. "Optimal Lymphadenectomy in Patients with Well-Differentiated Nonfunctioning Pancreatic Neuroendocrine Neoplasms" Journal of Clinical Medicine 12, no. 21: 6778. https://doi.org/10.3390/jcm12216778