
Is There a Correlation between Endoscopic Sinus Surgery and Improvement in Erectile Dysfunction?

 , ,
, ,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preoperative Assessment
- Male patients aged between 40 and 70 years old;
- Nasal obstruction caused by CRS and or NP confirmed by nasal endoscopic examination and paranasal sinus CT scan;
- Patient with indication for FESS;
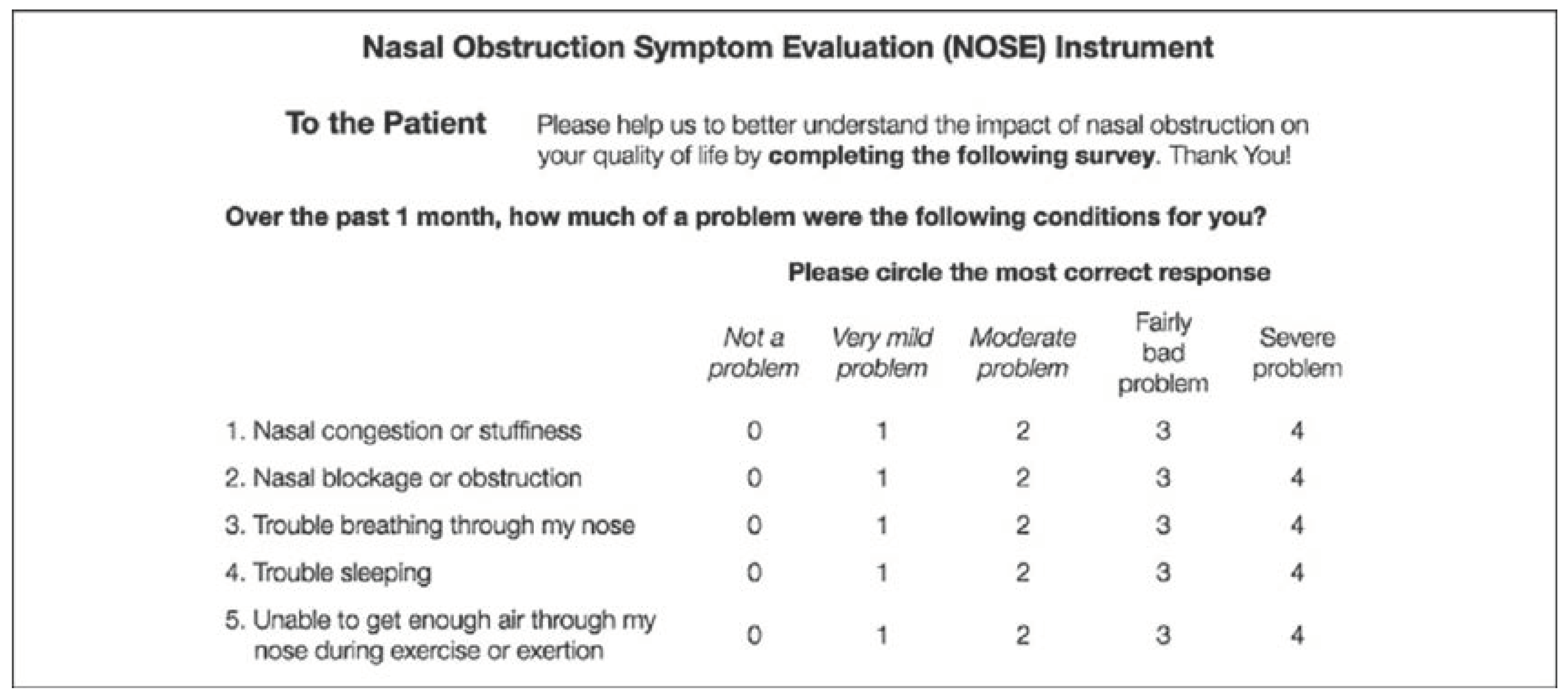
- Personal perception of the nasal obstruction assessed through the Nasal Obstruction Symptom Evaluation (NOSE) scale questionnaire before surgery and 3 months after (development and validation of the Nasal Obstruction Symptom Evaluation (NOSE) scale);
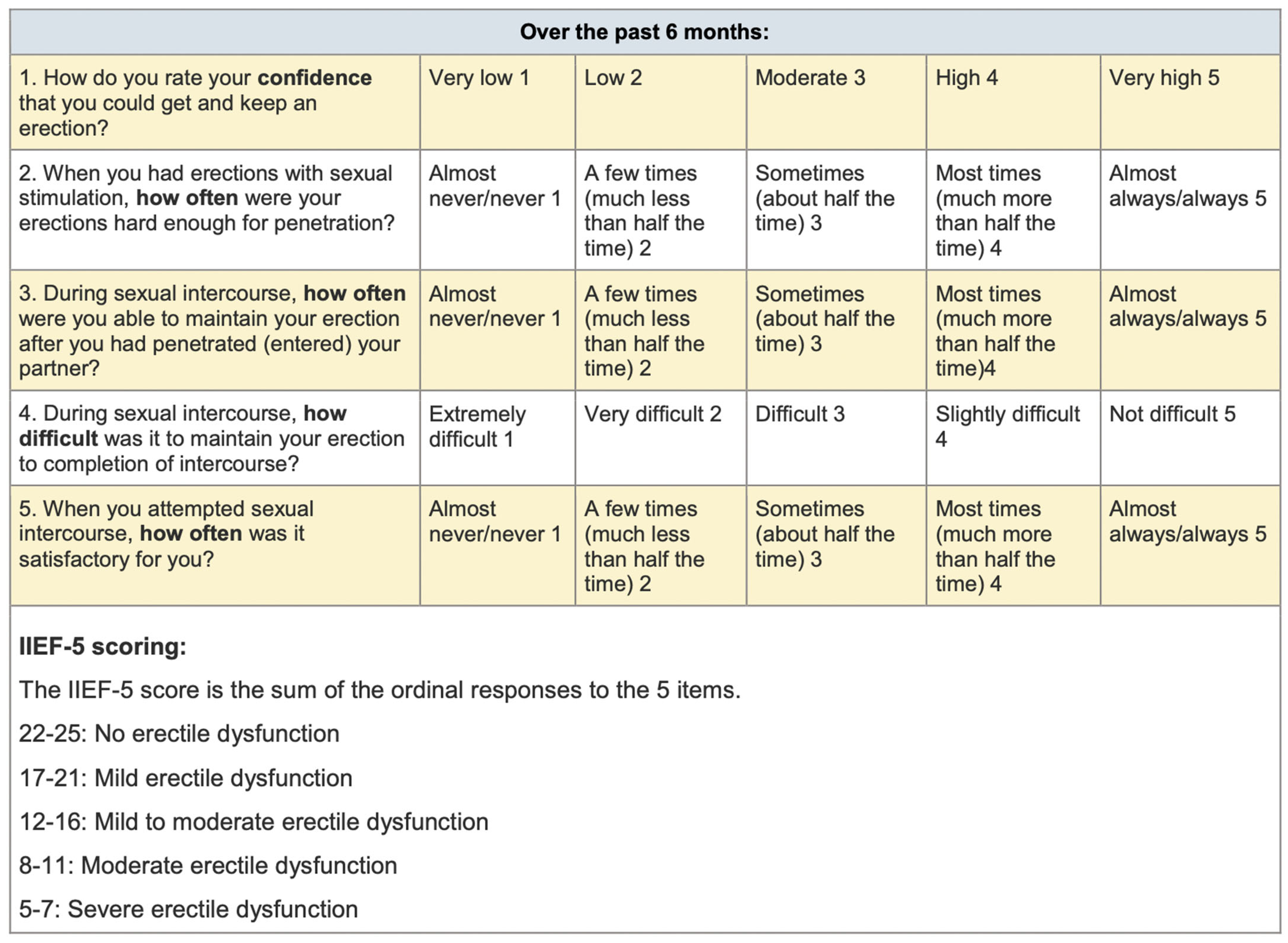
- Clinical diagnosis of erectile dysfunction by using the 5th International Index Erectile Function Score (the use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction) [16].
2.2. Surgical Procedure
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsu, D.W.; Suh, J.D. Anatomy and Physiology of Nasal Obstruction. Otolaryngol. Clin. N. Am. 2018, 51, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.-S.; Liang, K.-L.; Hsin, C.-H.; Su, M.-C. The impact of chronic rhinosinusitis on sleep-disordered breathing. Rhinology 2016, 54, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Droller, M.J.A.J.; Beck, J.C. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270, 83–90. [Google Scholar]
- Corona, G.; Lee, D.M.; Forti, G.; O’connor, D.B.; Maggi, M.; O’neill, T.W.; Pendleton, N.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; et al. Age-Related Changes in General and Sexual Health in Middle-Aged and Older Men: Results from the European Male Ageing Study (EMAS). J. Sex. Med. 2010, 7, 1362–1380. [Google Scholar] [CrossRef]
- Nicolosi, A.; Laumann, E.O.; Glasser, D.B.; Moreira, E.D., Jr.; Paik, A.; Gingell, C. Sexual behavior and sexual dysfunctions after age 40: The global study of sexual attitudes and behaviors. Urology 2004, 64, 991–997. [Google Scholar] [CrossRef]
- Laumann, E.O.; Nicolosi, A.; Glasser, D.B.; Paik, A.; Gingell, C.; Moreira, E.; Wang, T. Sexual problems among women and men aged 40–80y: Prevalence and correlates identified in the global Study of Sexual Attitudes and Behaviors. Int. J. Impot. Res. 2005, 17, 39–57. [Google Scholar] [CrossRef]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; et al. Erectile dysfunction. Nat. Rev. Dis. Primers 2016, 2, 16003. [Google Scholar] [CrossRef]
- Benninger, M.S.; Khalid, A.N.; Ba, R.M.B.; Smith, T.L. Surgery for chronic rhinosinusitis may improve sleep and sexual function. Laryngoscope 2010, 120, 1696–1700. [Google Scholar] [CrossRef]
- Gunhan, K.; Zeren, F.; Uz, U.; Gumus, B.; Unlu, H. Impact of nasal polyposis on erectile dysfunction. Am. J. Rhinol. Allergy 2011, 25, 112–115. [Google Scholar] [CrossRef]
- Tai, S.Y.; Wang, L.F.; Tai, C.F.; Huang, Y.T.; Chien, C.Y. Chronic Rhinosinusitis Associated with Erectile Dysfunction: A Population-Based Study. Sci. Rep. 2016, 6, 32195. [Google Scholar] [CrossRef]
- Wu, C.W.; Chao, P.Z.; Hao, W.R.; Liou, T.H.; Lin, H.W. Risk of stroke among patients with rhinosinusitis: A population-based study in Taiwan. Am. J. Rhinol. Allergy 2012, 26, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-H.; Wu, C.-S.; Keller, J.J.; Lin, H.-C. Chronic rhinosinusitis increased the risk of stroke: A 5-year follow-up study. Laryngoscope 2013, 123, 835–840. [Google Scholar] [CrossRef]
- Wang, P.-C.; Lin, H.-C.; Kang, J.-H. Chronic Rhinosinusitis Confers an Increased Risk of Acute Myocardial Infarction. Am. J. Rhinol. Allergy 2013, 27, e178–e182. [Google Scholar] [CrossRef] [PubMed]
- Fidan, V.; Aksakal, E. Impact of septoplasty on pulmonary artery pressure in patients with markedly deviated septum. J. Craniofacial Surg. 2011, 22, 1591–1593. [Google Scholar] [CrossRef] [PubMed]
- Gelardi, M.; Piccininni, K.; Quaranta, N.; Quaranta, V.; Silvestri, M.; Ciprandi, G. Olfactory dysfunction in patients with chronic rhinosinusitis with nasal polyps is associated with clinical-cytological grading severity. Acta Otorhinolaryngol. Ital. 2019, 39, 329–335. [Google Scholar] [CrossRef]
- van Kollenburg, R.A.A.; de Bruin, D.M.; Wijkstra, H. Validation of the Electronic Version of the International Index of Erectile Function (IIEF-5 and IIEF-15): A Crossover Study. J. Med. Internet Res. 2019, 21, e13490. [Google Scholar] [CrossRef]
- Sobh, E.; Elhussieny, F.; Ismail, T. Elimination of nasal obstruction improves pulmonary functions and oxygenation. Egypt. J. Bronc- 2021, 15, 32. [Google Scholar] [CrossRef]
- Menashe, V.D.; Farrehi, C.; Miller, M. Hypoventilation and cor pulmonale due to chronic upper airway obstruction. J. Pediatr. 1965, 67, 198–203. [Google Scholar] [CrossRef]
- Gandaglia, G.; Briganti, A.; Jackson, G.; Kloner, R.A.; Montorsi, F.; Montorsi, P.; Vlachopoulos, C. A Systematic Review of the Association Between Erectile Dysfunction and Cardiovascular Disease. Eur. Urol. 2014, 65, 968–978. [Google Scholar] [CrossRef]
- Bacon, C.G.; Mittleman, M.A.; Kawachi, I.; Giovannucci, E.; Glasser, D.B.; Rimm, E.B. A Prospective Study of Risk Factors for Erectile Dysfunction. J. Urol. 2006, 176, 217–221. [Google Scholar] [CrossRef]
- Pfeiffer, C.A.; Johnston, R.E. Hormonal and behavioral responses of male hamsters to females and female odors: Roles of olfaction, the vomeronasal system, and sexual experience. Physiol. Behav. 1994, 55, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.J. An Initial Evaluation of the Functions of Human Olfaction. Chem. Senses 2010, 35, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.Y.; Feng, J.R.; Zhou, W.H.; Kong, W.F.; Ma, G.C.; Hu, T.F.; Luo, S.G.; Xi, Y.; Zhang, Y.; Yang, Q.T. Olfactory Sensitivity Is Related to Erectile Function in Adult Males. Front. Cell Dev. Biol. 2020, 8, 93. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, E.; Fallara, G.; Capogrosso, P.; Boeri, L.; Belladelli, F.; Corsini, C.; Costa, A.; Candela, L.; Cignoli, D.; Cazzaniga, W.; et al. Primary organic versus primary psychogenic erectile dysfunction: Findings from a real-life cross-sectional study. Andrology 2022, 10, 1302–1309. [Google Scholar] [CrossRef]
- Lindberg, S.; Cervin, A.; Runer, T. Nitric Oxide (NO) Production in the Upper Airways is Decreased in Chronic Sinusitis. Acta Oto-Laryngologica 1997, 117, 113–117. [Google Scholar] [CrossRef]
- Ragab, S.M.; Lund, V.J.; Saleh, H.A.; Scadding, G. Nasal nitric oxide in objective evaluation of chronic rhinosinusitis therapy. Allergy 2006, 61, 717–724. [Google Scholar] [CrossRef]
- Bank, A.; Billups, K.; Kaiser, D.R.; Kelly, A.; Wetterling, R.; Tsai, M.; Hanson, N. Relation of C-reactive protein and other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. Int. J. Impot. Res. 2003, 15, 231–236. [Google Scholar] [CrossRef]
- Giugliano, F.; Esposito, K.; Di Palo, C.; Ciotola, M.; Giugliano, G.; Marfella, R.; D’armiento, M.; Giugliano, D. Erectile dysfunction associates with endothelial dysfunction and raised proinflammatory cytokine levels in obese men. J. Endocrinol. Investig. 2004, 27, 665–669. [Google Scholar] [CrossRef]
- Hansen, J.G.; Højbjerg, T.; Rosborg, J. Symptoms and signs in culture-proven acute maxillary sinusitis in a general practice population. APMIS 2009, 117, 724–729. [Google Scholar] [CrossRef]
- Cals, J.W.L.; Schot, M.J.C.; de Jong, S.A.M.; Dinant, G.-J.; Hopstaken, R.M. Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial. Ann. Fam. Med. 2010, 8, 124–133. [Google Scholar] [CrossRef]
- Moon, K.H.; Park, S.Y.; Kim, Y.W. Obesity and Erectile Dysfunction: From Bench to Clinical Implication. World J. Men’s Health 2019, 37, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Nunes, K.P.; Labazi, H.; Webb, R.C. New insights into hypertension-associated erectile dysfunction. Curr. Opin. Nephrol. Hypertens. 2012, 21, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Nutalapati, S.; Ghagane, S.C.; Nerli, R.; Jali, M.; Dixit, N.S. Association of erectile dysfunction and type II diabetes mellitus at a tertiary care centre of south India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 649–653. [Google Scholar] [CrossRef]
- Tamrakar, D.; Bhatt, D.S.; Sharma, V.K.; Poudyal, A.K.; Yadav, B.K. Association between Erectile Dysfunction and Type 2 Diabetes Mellitus. J. Nepal Health Res. Counc. 2021, 19, 378–383. [Google Scholar]
- Hirshoren, N.; Hirschenbein, A.; Eliashar, R. Risk stratification of severe acute rhinosinusitis unresponsive to oral antibiotics. Acta Oto-Laryngologica 2010, 130, 1065–1069. [Google Scholar] [CrossRef]
- Oyer, S.L.; Mulligan, J.K.; Psaltis, A.J.; Henriquez, O.A.; Schlosser, R.J. Cytokine correlation between sinus tissue and nasal secretions among chronic rhinosinusitis and controls. Laryngoscope 2013, 123, E72–E78. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, F.S.; Webb, R.C.; Tostes, R.C. Emerging Role for TNF-α in Erectile Dysfunction. J. Sex. Med. 2010, 7, 3823–3834. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Question n° 1 | Question n° 2 | Question n° 3 | Question n° 2 | Question n° 3 | IIEF-5 PRE | IIEF-5 POST | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | PRE | POST | PRE | POST | PRE | POST | |||
| 40 | 4 | 5 | 2 | 3 | 2 | 3 | 3 | 4 | 4 | 4 | 15 | 19 |
| 40 | 4 | 4 | 3 | 5 | 5 | 5 | 4 | 5 | 4 | 4 | 20 | 23 |
| 40 | 3 | 3 | 2 | 2 | 3 | 3 | 3 | 3 | 4 | 5 | 15 | 16 |
| 40 | 4 | 5 | 3 | 5 | 3 | 5 | 4 | 5 | 4 | 4 | 18 | 24 |
| 40 | 3 | 4 | 2 | 2 | 3 | 4 | 3 | 4 | 5 | 5 | 16 | 19 |
| 40 | 3 | 4 | 3 | 5 | 4 | 4 | 4 | 5 | 5 | 5 | 19 | 23 |
| 41 | 4 | 5 | 3 | 5 | 3 | 3 | 4 | 5 | 4 | 5 | 18 | 23 |
| 41 | 5 | 5 | 2 | 2 | 4 | 4 | 5 | 5 | 4 | 4 | 20 | 20 |
| 42 | 5 | 5 | 2 | 3 | 3 | 5 | 5 | 5 | 4 | 4 | 19 | 22 |
| 42 | 5 | 5 | 3 | 5 | 2 | 4 | 4 | 5 | 5 | 5 | 19 | 24 |
| 42 | 3 | 5 | 5 | 5 | 2 | 3 | 3 | 5 | 5 | 5 | 18 | 23 |
| 42 | 3 | 4 | 1 | 2 | 3 | 3 | 2 | 2 | 5 | 5 | 14 | 16 |
| 43 | 4 | 5 | 5 | 5 | 3 | 3 | 5 | 5 | 4 | 4 | 21 | 22 |
| 44 | 3 | 5 | 5 | 5 | 3 | 5 | 3 | 3 | 4 | 4 | 18 | 22 |
| 44 | 4 | 5 | 3 | 5 | 3 | 3 | 3 | 5 | 4 | 4 | 17 | 22 |
| 44 | 2 | 5 | 5 | 5 | 2 | 2 | 5 | 5 | 5 | 5 | 19 | 22 |
| 46 | 3 | 5 | 1 | 2 | 2 | 3 | 2 | 2 | 5 | 5 | 13 | 17 |
| 46 | 3 | 5 | 5 | 5 | 3 | 4 | 5 | 5 | 5 | 5 | 21 | 24 |
| 46 | 2 | 5 | 5 | 5 | 3 | 5 | 3 | 3 | 4 | 4 | 17 | 22 |
| 47 | 3 | 5 | 3 | 5 | 2 | 2 | 3 | 5 | 4 | 4 | 15 | 21 |
| 48 | 4 | 5 | 5 | 5 | 3 | 3 | 5 | 5 | 4 | 4 | 21 | 22 |
| 49 | 5 | 5 | 1 | 2 | 2 | 2 | 2 | 2 | 3 | 5 | 13 | 16 |
| 49 | 3 | 5 | 5 | 5 | 2 | 3 | 5 | 5 | 4 | 4 | 19 | 22 |
| 49 | 2 | 4 | 5 | 5 | 3 | 4 | 3 | 3 | 5 | 5 | 18 | 21 |
| 50 | 1 | 4 | 5 | 5 | 3 | 5 | 5 | 5 | 4 | 5 | 18 | 24 |
| 50 | 2 | 4 | 5 | 5 | 3 | 3 | 3 | 3 | 3 | 5 | 16 | 20 |
| 50 | 3 | 4 | 3 | 5 | 4 | 4 | 5 | 5 | 4 | 4 | 19 | 22 |
| 50 | 3 | 5 | 5 | 5 | 5 | 5 | 3 | 5 | 5 | 5 | 21 | 25 |
| 50 | 3 | 4 | 1 | 2 | 4 | 4 | 2 | 2 | 4 | 4 | 14 | 16 |
| 51 | 4 | 5 | 1 | 2 | 5 | 5 | 3 | 3 | 3 | 3 | 16 | 18 |
| 51 | 3 | 5 | 5 | 4 | 3 | 5 | 4 | 4 | 4 | 4 | 19 | 22 |
| 52 | 4 | 4 | 4 | 5 | 4 | 4 | 3 | 3 | 5 | 5 | 20 | 21 |
| 53 | 5 | 5 | 1 | 2 | 3 | 3 | 3 | 3 | 4 | 4 | 16 | 17 |
| 53 | 3 | 5 | 5 | 5 | 3 | 3 | 3 | 4 | 3 | 4 | 17 | 21 |
| 53 | 3 | 4 | 4 | 5 | 2 | 3 | 3 | 3 | 4 | 5 | 16 | 20 |
| 54 | 1 | 2 | 1 | 3 | 2 | 3 | 3 | 3 | 5 | 4 | 12 | 15 |
| 55 | 2 | 3 | 2 | 3 | 3 | 3 | 4 | 4 | 4 | 4 | 15 | 17 |
| 57 | 3 | 3 | 4 | 5 | 2 | 3 | 3 | 3 | 5 | 5 | 17 | 19 |
| 59 | 1 | 3 | 2 | 3 | 2 | 3 | 4 | 4 | 4 | 4 | 13 | 17 |
| 60 | 2 | 2 | 4 | 5 | 3 | 3 | 3 | 5 | 3 | 3 | 15 | 18 |
| 61 | 2 | 3 | 3 | 3 | 4 | 4 | 4 | 4 | 4 | 4 | 17 | 18 |
| 61 | 2 | 3 | 1 | 2 | 3 | 3 | 3 | 3 | 4 | 4 | 13 | 15 |
| 61 | 1 | 4 | 2 | 3 | 3 | 5 | 5 | 5 | 3 | 3 | 14 | 20 |
| 62 | 2 | 3 | 3 | 3 | 2 | 4 | 3 | 4 | 5 | 5 | 15 | 19 |
| 62 | 3 | 4 | 1 | 2 | 2 | 4 | 3 | 3 | 3 | 3 | 12 | 16 |
| 63 | 2 | 5 | 1 | 2 | 2 | 3 | 3 | 3 | 4 | 4 | 12 | 17 |
| 63 | 3 | 3 | 2 | 3 | 4 | 4 | 2 | 3 | 5 | 5 | 16 | 18 |
| 63 | 3 | 3 | 3 | 3 | 2 | 4 | 3 | 4 | 4 | 4 | 15 | 18 |
| 64 | 4 | 4 | 1 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 14 | 15 |
| 65 | 3 | 4 | 1 | 3 | 2 | 2 | 3 | 3 | 4 | 4 | 13 | 16 |
| 66 | 2 | 2 | 2 | 3 | 3 | 2 | 3 | 4 | 5 | 5 | 15 | 16 |
| 66 | 1 | 1 | 3 | 3 | 2 | 3 | 3 | 4 | 4 | 5 | 13 | 16 |
| 70 | 3 | 3 | 1 | 2 | 1 | 2 | 3 | 3 | 3 | 4 | 11 | 14 |
| 51.320 | 2.9811 | 4.0943 | 2.9245 | 3.6981 | 2.8679 | 3.5283 | 3.4528 | 3.8867 | 4.1320 | 4.3207 | 16.3584 | 19.5283 |
| Variable | Pre, N = 53 | Post, N = 53 | Controls, N = 49 | p-Value * (Cases Pre vs. Post) | p-Value ** (Cases Pre vs. Controls) |
|---|---|---|---|---|---|
| Nasal stuffiness | 3.02 (0.93) | 1.34 (1.06) | 0.39 (0.49) | <0.001 | <0.001 |
| Nasal obstruction | 3.19 (0.74) | 0.51 (0.64) | 0.35 (0.48) | <0.001 | <0.001 |
| Trouble breathing through the nose | 2.94 (0.82) | 0.77 (0.67) | 0.12 (0.33) | <0.001 | <0.001 |
| Trouble sleeping | 2.25 (1.22) | 1.00 (0.88) | 0.29 (0.46) | <0.001 | <0.001 |
| Unable to get air through the nose during exercise | 3.13 (0.83) | 1.36 (0.94) | 0.14 (0.35) | <0.001 | <0.001 |
| Confidence to get and keep an erection | 2.98 (1.08) | 4.09 (1.02) | 4.86 (0.35) | <0.001 | <0.001 |
| Erection hard enough for penetration | 2.92 (1.53) | 3.70 (1.31) | 4.96 (0.20) | <0.001 | <0.001 |
| Able to maintain the erection after penetration | 2.87 (0.88) | 3.53 (0.93) | 4.98 (0.14) | <0.001 | <0.001 |
| Difficult to maintain the erection to completion of intercourse | 3.45 (0.91) | 3.89 (1.01) | 4.94 (0.24) | <0.001 | <0.001 |
| Grade of satisfaction | 4.13 (0.68) | 4.32 (0.64) | 4.94 (0.24) | 0.015 | <0.001 |
| Fixed Effects | Estimate | p-Value |
|---|---|---|
| Nasal Stuffiness | −0.06009 | 0.569 |
| Nasal Obstruction | 0.30565 | 0.088 |
| Trouble Breathing | −0.08294 | 0.619 |
| Trouble Sleeping | 0.16158 | 0.102 |
| Unable to get air | 0.04342 | 0.704 |
| Fixed Effects | Estimate | p-Value |
|---|---|---|
| Nasal stuffiness | −0.2335 | 0.080 |
| Nasal obstruction | 0.5082 | 0.024 |
| Trouble breathing | −0.2187 | 0.299 |
| Trouble sleeping | −0.3360 | 0.008 |
| Unable to get air | 0.4056 | 0.006 |
| Fixed Effects | Estimate | p-Value |
|---|---|---|
| Nasal stuffiness | 0.13764 | 0.135 |
| Nasal obstruction | 0.22629 | 0.144 |
| Trouble breathing | −0.02678 | 0.853 |
| Trouble sleeping | 0.01877 | 0.826 |
| Unable to get air | 0.04239 | 0.670 |
| Fixed Effects | Estimate | p-Value |
|---|---|---|
| Nasal stuffiness | −0.09336 | 0.308 |
| Nasal obstruction | 0.02070 | 0.876 |
| Trouble breathing | −0.15772 | 0.302 |
| Trouble sleeping | −0.13655 | 0.131 |
| Unable to get air | 0.09636 | 0.327 |
| Fixed Effects | Estimate | p-Value |
|---|---|---|
| Nasal stuffiness | −0.07023 | 0.266 |
| Nasal obstruction | 0.38287 | <0.001 |
| Trouble breathing | −0.09171 | 0.358 |
| Trouble sleeping | −0.04029 | 0.492 |
| Unable to get air | 0.09166 | 0.181 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Committeri, U.; Abbate, V.; Sarcinella, M.; Maffia, F.; Barone, S.; Troise, S.; Salzano, G.; Nocini, R.; Bonavolontà, P.; et al. Is There a Correlation between Endoscopic Sinus Surgery and Improvement in Erectile Dysfunction? J. Clin. Med. 2023, 12, 6626. https://doi.org/10.3390/jcm12206626
Romano A, Committeri U, Abbate V, Sarcinella M, Maffia F, Barone S, Troise S, Salzano G, Nocini R, Bonavolontà P, et al. Is There a Correlation between Endoscopic Sinus Surgery and Improvement in Erectile Dysfunction? Journal of Clinical Medicine. 2023; 12(20):6626. https://doi.org/10.3390/jcm12206626
Chicago/Turabian StyleRomano, Antonio, Umberto Committeri, Vincenzo Abbate, Marco Sarcinella, Francesco Maffia, Simona Barone, Stefania Troise, Giovanni Salzano, Riccardo Nocini, Paola Bonavolontà, and et al. 2023. "Is There a Correlation between Endoscopic Sinus Surgery and Improvement in Erectile Dysfunction?" Journal of Clinical Medicine 12, no. 20: 6626. https://doi.org/10.3390/jcm12206626