
Reliability and Validity of Non-Instrumental Clinical Assessments for Adults with Oropharyngeal Dysphagia: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Abstract and Measure Selection
2.4. Data Extraction
2.5. Methodological Quality
2.6. Conceptual Mapping of Measures
3. Results
3.1. Systematic Literature Search
3.2. Characteristics of Included Measures and Psychometric Studies
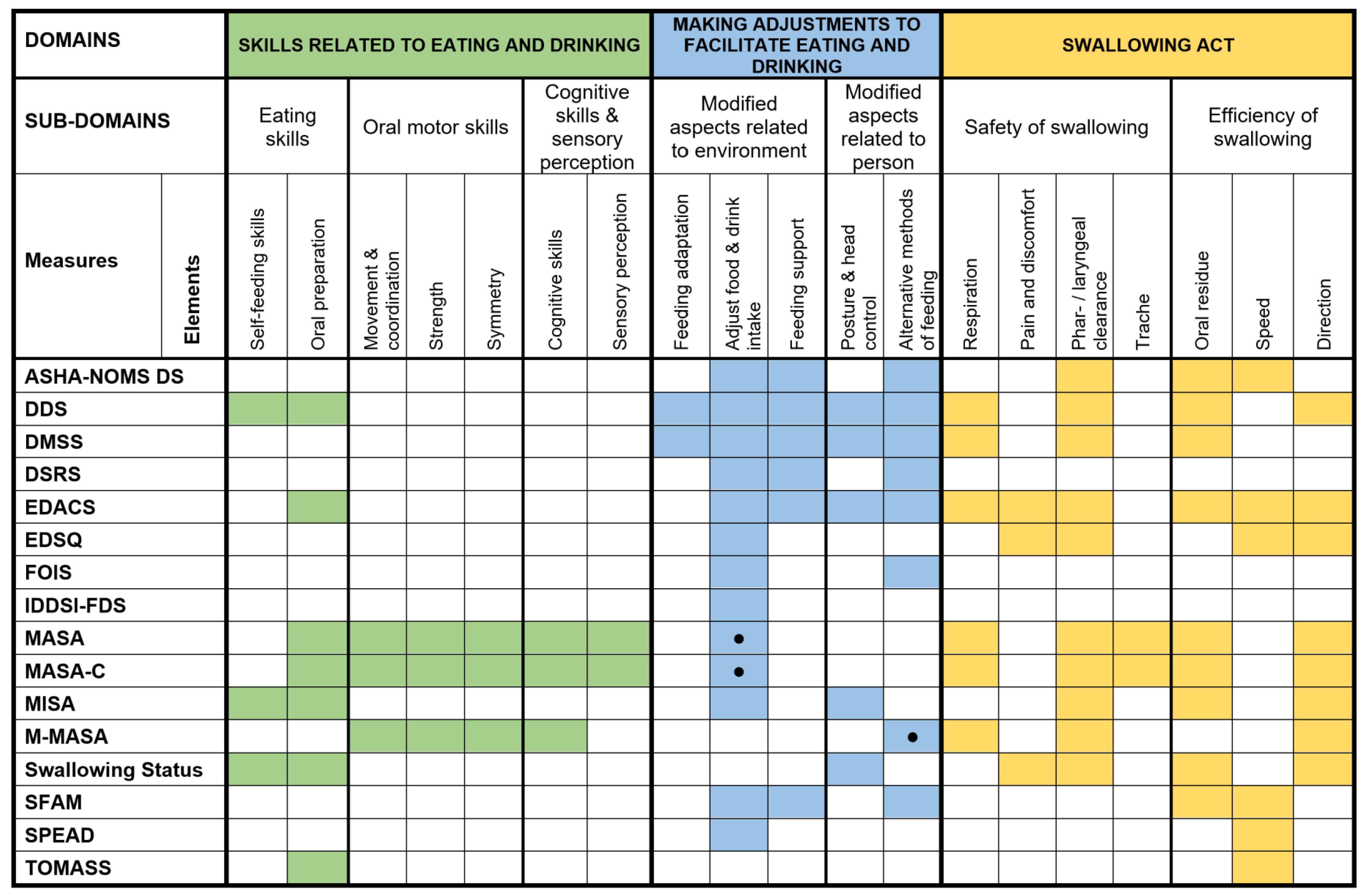
3.3. Conceptual Mapping of Non-Instrumental Clinical Measures
3.4. Validity Evidence
3.5. Reliability Evidence
3.6. Conceptual Mapping of Included Measures
3.7. Methodological Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Speyer, R.; Cordier, R.; Denman, D.; Windsor, C.; Krisciunas, G.P.; Smithard, D.; Heijnen, B.J. Development of Two Patient Self-Reported Measures on Functional Health Status (FOD) and Health-Related Quality of Life (QOD) in Adults with Oropharyngeal Dysphagia Using the Delphi Technique. J. Clin. Med. 2022, 11, 5920. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Speyer, R.; Kertscher, B.; Denman, D.; Swan, K.; Cordier, R. Health-related quality of life and oropharyngeal dysphagia: A systematic review. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nativ-Zeltzer, N.; Nachalon, Y.; Kaufman, M.W.; Seeni, I.C.; Bastea, S.; Aulakh, S.S.; Makkiyah, S.; Wilson, M.D.; Evangelista, L.; Kuhn, M.A. Predictors of aspiration pneumonia and mortality in patients with dysphagia. Laryngoscope 2022, 132, 1172–1176. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R. Oropharyngeal dysphagia: Screening and assessment. Otolaryngol. Clin. N. Am. 2013, 46, 989–1008. [Google Scholar] [CrossRef] [PubMed]
- Swan, K.; Cordier, R.; Brown, T.; Speyer, R. Psychometric properties of visuoperceptual measures of videofluoroscopic and fibre-endoscopic evaluations of swallowing: A systematic review. Dysphagia 2019, 34, 2–33. [Google Scholar] [CrossRef] [Green Version]
- Speyer, R.; Cordier, R.; Farneti, D.; Nascimento, W.; Pilz, W.; Verin, E.; Walshe, M.; Woisard, V. White paper by the European society for Swallowing Disorders: Screening and non-instrumental assessment for dysphagia in adults. Dysphagia 2022, 37, 333–349. [Google Scholar] [CrossRef]
- Benfield, J.K.; Everton, L.F.; Bath, P.M.; England, T.J. Accuracy and clinical utility of comprehensive dysphagia screening assessments in acute stroke: A systematic review and meta-analysis. J. Clin. Nurs. 2020, 29, 1527–1538. [Google Scholar] [CrossRef]
- Bours, G.J.; Speyer, R.; Lemmens, J.; Limburg, M.; De Wit, R. Bedside screening tests vs. videofluoroscopy or fibreoptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: Systematic review. J. Adv. Nurs. 2009, 65, 477–493. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.B.; Suiter, D.M.; González-Fernández, M.; Michtalik, H.J.; Frymark, T.B.; Venediktov, R.; Schooling, T. Screening accuracy for aspiration using bedside water swallow tests: A systematic review and meta-analysis. Chest 2016, 150, 148–163. [Google Scholar] [CrossRef] [Green Version]
- Kertscher, B.; Speyer, R.; Palmieri, M.; Plant, C. Bedside screening to detect oropharyngeal dysphagia in patients with neurological disorders: An updated systematic review. Dysphagia 2014, 29, 204–212. [Google Scholar] [CrossRef] [PubMed]
- O’Horo, J.C.; Rogus-Pulia, N.; Garcia Arguello, L.; Robbins, J.; Safdar, N. Bedside diagnosis of dysphagia: A systematic review. J. Hosp. Med. 2015, 10, 256. [Google Scholar] [CrossRef] [Green Version]
- Speyer, R.; Cordier, R.; Kertscher, B.; Heijnen, B.J. Psychometric properties of questionnaires on functional health status in oropharyngeal dysphagia: A systematic literature review. Bio. Med. Res. Int. 2014, 2014, 458678. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, A.A.; Speyer, R.; Heijnen, B.J.; Klijn-Zwijnenberg, I.R. Psychometric characteristics of health-related quality-of-life questionnaires in oropharyngeal dysphagia. Dysphagia 2014, 29, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Cordier, R.; Parsons, L.; Denman, D.; Kim, J.-H. Psychometric characteristics of non-instrumental swallowing and feeding assessments in pediatrics: A systematic review using COSMIN. Dysphagia 2018, 33, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Prinsen, C.; Patrick, D.L.; Alonso, J.; Bouter, L.; de Vet, H.C.W.; Terwee, C.B. COSMIN methodology for systematic reviews of patient-reported outcome measures (PROMs). User Man. 2018, 78, 1–78. [Google Scholar]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Islam, R.M.; Oldroyd, J.; Karim, M.N.; Hossain, S.M.; Hoque, D.M.E.; Romero, L.; Fisher, J. Systematic review and meta-analysis of prevalence of, and risk factors for, pelvic floor disorders in community-dwelling women in low and middle-income countries: A protocol study. BMJ Open 2017, 7, e015626. [Google Scholar] [CrossRef] [Green Version]
- Kmet, L.M.; Cook, L.S.; Lee, R.C. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004. [Google Scholar]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; De Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dungan, S.; Gregorio, D.; Abrahams, T.; Harrison, B.; Abrahams, J.; Brocato, D.; Davis, C.; Espana, E.; Garcia, R.; Carnaby, G.; et al. Comparative Validity of the American Speech-Language-Hearing Association’s National Outcomes Measurement System, Functional Oral Intake Scale, and G-Codes to Mann Assessment of Swallowing Ability Scores for Dysphagia. Am. J. Speech-Lang. Pathol. 2019, 28, 424–429. [Google Scholar] [CrossRef]
- Antonios, N.; Carnaby-Mann, G.; Crary, M.; Miller, L.; Hubbard, H.; Hood, K.; Sambandam, R.; Xavier, A.; Silliman, S. Analysis of a Physician Tool for Evaluating Dysphagia on an Inpatient Stroke Unit: The Modified Mann Assessment of Swallowing Ability. J. Stroke Cerebrovasc. Dis. 2010, 19, 49–57. [Google Scholar] [CrossRef]
- Crary, M.A.; Carnaby Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Sim, J.; Park, J.; Jung, Y.; Cho, K.H.; Min, K.; Kim, M.; Kim, J.M.; Im, S.H. Assessment of Aspiration Risk Using the Mann Assessment of Swallowing Ability in Brain-Injured Patients With Cognitive Impairment. Front. Neurol. 2019, 10, 1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira-Kumakura, A.R.S.; de Araujo, T.L.; Costa, A.G.S.; Cavalcante, T.F.; Lopes, M.V.O.; Carvalho, E.C. Clinical Validation of the Nursing Outcome “Swallowing Status” in People with Stroke: Analysis According to the Classical and Item Response Theories. Int. J. Nurs. Knowl. 2018, 29, 234–241. [Google Scholar] [CrossRef]
- Everton, L.F.; Benfield, J.; Hedstrom, A.; Wilkinson, G.; Michou, E.; England, T.; Dziewas, R.; Bath, P.B.; Hamdy, S. Psychometric assessment and validation of the dysphagia severity rating scale in stroke patients. Sci. Rep. 2020, 10, 7268. [Google Scholar] [CrossRef]
- Mann, G. MASA, The Mann Assessment of Swallowing Ability; Shirley Ryan Abilitylab: Chicago, IL, USA, 2002. [Google Scholar]
- Sheppard, J.J.; Hochman, R.; Baer, C. The Dysphagia Disorder Survey: Validation of an assessment for swallowing and feeding function in developmental disability. Res. Dev. Disabil. 2014, 35, 929–942. [Google Scholar] [CrossRef]
- Carnaby, G.D.; Crary, M.A. Development and validation of a cancer-specific swallowing assessment tool: MASA-C. Support. Care Cancer 2014, 22, 595–602. [Google Scholar] [CrossRef]
- Karsten, R.T.; Hilgers, F.J.M.; van der Molen, L.; van Sluis, K.; Smeele, L.E.; Stuiver, M.M. The Timed Swallowing Proficiency for Eating and Drinking (SPEAD) Test.: Development and Initial Validation of an Instrument to Objectify (Impaired) Swallowing Capacity in Head and Neck Cancer Patients. Dysphagia 2021, 36, 1072–1087. [Google Scholar] [CrossRef] [PubMed]
- Huckabee, M.-L.; McIntosh, T.; Fuller, L.; Morgan, C.; Paige, T.; Walshe, M.; Engel-Hoek, L.v.d.; Sella-Weiss, O. The Test of Masticating and Swallowing Solids (TOMASS): Reliability, validity and international normative data. Int. J. Lang. Commun. Disord. 2018, 53, 144–156. [Google Scholar] [CrossRef]
- Lambert, H.C.; Gisel, E.G.; Groher, M.E.; Abrahamowicz, M.; Wood-Dauphinee, S. Psychometric Testing of the McGill Ingestive Skills Assessment. Am. J. Occup. Ther. 2006, 60, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Sellers, D.; Mandy, A.; Hankins, M.; Pennington, L.; Carter, M.; Ford, S.; Pountney, T.; Morris, C. Development of an Eating and Drinking Ability Classification System (EDACS) for people with cerebral palsy. Dev. Med. Child Neurol. 2013, 2, 49–50. [Google Scholar]
- American Speech-Language-Hearing Association. National Outcomes Measurement System Speech-Language Pathology Registry. Available online: https://www.asha.org/noms/noms-speech-language-pathology-registry/ (accessed on 1 April 2022).
- Uhm, K.E.; Kim, M.; Lee, Y.M.; Kim, B.R.; Kim, Y.S.; Choi, J.; Han, S.H.; Kim, H.J.; Yoo, K.H.; Lee, J. The Easy Dysphagia Symptom Questionnaire (EDSQ): A new dysphagia screening questionnaire for the older adults. Eur. Geriatr. Med. 2019, 10, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.M.; Namasivayam-MacDonald, A.M.; Guida, B.T.; Cichero, J.A.; Duivestein, J.; Hanson, B.; Lam, P.; Riquelme, L.F. Creation and Initial Validation of the International Dysphagia Diet. Standardisation Initiative Functional Diet Scale. Arch. Phys. Med. Rehabil. 2018, 99, 934–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, H.C.; Gisel, E.G.; Groher, M.E.; Wood-Dauphinee, S. McGill Ingestive Skills Assessment (MISA): Development and first field test of an evaluation of functional ingestive skills of elderly persons. Dysphagia 2003, 18, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.M. Overview of functional assessment scales in brain injury rehabilitation. NeuroRehabilitation 1992, 2, 98–113. [Google Scholar] [CrossRef]
- Moorhead, S.; Johnson, M.; Maas, M.; Swanson, E. Nursing Outcomes Classification (NOC); Elsevier: St. Louis, MO, USA, 2013. [Google Scholar]
- Athukorala, R.P.; Jones, R.D.; Sella, O.; Huckabee, M.-L. Skill training for swallowing rehabilitation in patients with Parkinson’s disease. Arch. Phys. Med. Rehabil. 2014, 95, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.H.; Kim, D.; Chang, M.C. Comparison of dysphagia outcomes between rostral and caudal lateral medullary infarct patients. Int. J. Neurosci. 2017, 127, 965–970. [Google Scholar] [CrossRef]
- Hyun, S.E.; Yi, Y.G.; Shin, H.-I. Reliability and Validity of the Eating and Drinking Ability Classification System in Adults with Cerebral Palsy. Dysphagia 2021, 36, 351–361. [Google Scholar] [CrossRef]
- Nordio, S.; Di Stadio, A.; Koch, I.; Stritoni, P.; Meneghello, F.; Palmer, K. The correlation between pharyngeal residue, penetration/aspiration and nutritional modality: A cross-sectional study in patients with neurogenic dysphagia. Acta Otorhinolaryngol. Ital. 2020, 40, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Ishii, M.; Nakagawa, K.; Yoshimi, K.; Okumura, T.; Hasegawa, S.; Yamaguchi, K.; Nakane, A.; Tamai, T.; Nagasawa, Y.; Tohara, H.; et al. Higher Activity and Quality of Life Correlates with Swallowing Function in Older Adults with Low Activities of Daily Living. Gerontology 2021, 68, 671–681. [Google Scholar] [CrossRef]
- Mitani, Y.; Oki, Y.; Fujimoto, Y.; Yamaguchi, T.; Yamada, Y.; Yamada, K.; Ito, T.; Shiotani, H.; Ishikawa, A. Relationship between the Functional Independence Measure and Mann Assessment of Swallowing Ability in hospitalized patients with pneumonia. Geriatr. Gerontol. Int. 2018, 18, 1620–1624. [Google Scholar] [CrossRef] [Green Version]
- González-Fernández, M.; Sein, M.T.; Palmer, J.B. Clinical Experience Using the Mann Assessment of Swallowing Ability for Identification of Patients at Risk for Aspiration in a Mixed-Disease Population; ASHA: Rockville, MD, USA, 2011. [Google Scholar]
- Lambert, H.C.; Abrahamowicz, M.; Groher, M.; Wood-Dauphinee, S.; Gisel, E.G. The McGill ingestive skills assessment predicts time to death in an elderly population with neurogenic dysphagia: Preliminary evidence. Dysphagia 2005, 20, 123–132. [Google Scholar] [CrossRef]
- Francis-Bacz, C.; Wood-Dauphinee, S.; Gisel, E. The Discriminative Validity of the McGill Ingestive Skills Assessment. Phys. Occup. Ther. Geriatr. 2013, 31, 148–158. [Google Scholar] [CrossRef]
- Ji, E.K.; Wang, H.H.; Jung, S.J.; Lee, K.B.; Kim, J.S.; Hong, B.Y.; Lim, S.H. Is the modified Mann Assessment of Swallowing Ability useful for assessing dysphagia in patients with mild to moderate dementia? J. Clin. Neurosci. 2019, 70, 169–172. [Google Scholar] [CrossRef]
- McMicken, B.L.; Muzzy, C.L.; Calahan, S. Retrospective ratings of 100 first time-documented stroke patients on the Functional Oral Intake Scale. Disabil. Rehabil. 2010, 32, 1163–1172. [Google Scholar] [CrossRef]
- McMicken, B.L.; Muzzy, C.L. Functional outcomes of standard dysphagia treatment in first time documented stroke patients. Disabil. Rehabil. 2009, 31, 806–817. [Google Scholar] [CrossRef] [PubMed]
- McMicken, B.L.; Muzzy, C.L. Prognostic indicators of functional outcomes in first time documented acute stroke patients following standard dysphagia treatment. Disabil. Rehabil. 2009, 31, 2196–2203. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Kumakura, A.R.S.; Alonso, J.B.; de Carvalho, E.C. Psychometric Assessment of the Nursing Outcome Swallowing Status: Rasch Model. Approach. Int. J. Nurs. Knowl. 2019, 30, 197–202. [Google Scholar] [CrossRef]
- Oliveira, A.R.d.S.; Leite de Araujo, T.; Campos de Carvalho, E.; Costa, A.G.d.S.; Cavalcante, T.F.; Lopes, M.V.d.O. Construction and validation of indicators and respective definitions for the nursing outcome Swallowing Status. Rev. Lat.-Am. Enferm. 2015, 23, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Kothari, S.; Krishnamurthy, R.; Balasubramanium, R.K.; Huckabee, M.L. The Test. of Masticating and Swallowing Solids (TOMASS): Reliability, Validity and Normative Data for the Adult Indian Population. Indian J. Otolaryngol. Head Neck Surg. 2021, 73, 327–332. [Google Scholar] [CrossRef]
- Todaro, F.; Pizzorni, N.; Scarponi, L.; Ronzoni, C.; Huckabee, M.-L.; Schindler, A. The test of masticating and swallowing solids (tomass): Reliability and validity in patients with dysphagia. Int. J. Lang. Commun. Disord. 2021, 56, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Borders, J.C.; Sevitz, J.S.; Malandraki, J.B.; Malandraki, G.A.; Trochea, M.S. Objective and Subjective Clinical Swallowing Outcomes via Telehealth: Reliability in Outpatient Clinical Practice. Am. J. Speech-Lang. Pathol. 2021, 30, 598–608. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.; Lovric, L.; Matthelié, J.; Brage, L.; Hägglund, P. A Within-Subject Comparison of Face-to-Face and Telemedicine Screening Using the Timed Water Swallow Test. (TWST) and the Test. of Mastication and Swallowing of Solids (TOMASS). Dysphagia 2022, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. Br. Med. J. 1997, 314, 572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]



{kind=link}
{kind=link}
| Literature Database | Search Strategies |
|---|---|
| Cinahl Plus with Full Text (EBSCO) | ((MH “Deglutition”) OR (MH “Deglutition Disorders”)) AND (ti (assess* OR index* OR indices OR instrument* OR measure* OR subscale* OR scale* OR screen* OR tool* OR survey* OR inventor* OR protocol* self-report* OR patient-report* OR observation* OR rating* OR rated OR score*) OR ti (clinical N2 (outcome* OR evaluat*)) OR ti (funct* N2 (outcome* OR evaluat*)) OR ti (quality of life N2 (outcome* OR evaluat*)) OR ti (health N2 (outcome* OR evaluat*))) AND ((MH “Psychometrics”) OR (MH “Measurement Issues and Assessments”) OR (MH “Validity”) OR (MH “Predictive Validity”) OR (MH “Reliability and Validity”) OR (MH “Internal Validity”) OR (MH “Face Validity”) OR (MH “External Validity”) OR (MH “Discriminant Validity”) OR (MH “Criterion-Related Validity”) OR (MH “Consensual Validity”) OR (MH “Concurrent Validity”) OR (MH “Qualitative Validity”) OR (MH “Construct Validity”) OR (MH “Content Validity”) OR (MH “Instrument Validation”) OR (MH “Validation Studies”) OR (MH “Test-Retest Reliability”) OR (MH “Sensitivity and Specificity”) OR (MH “Reproducibility of Results”) OR (MH “Reliability”) OR (MH “Intrarater Reliability”) OR (MH “Interrater Reliability”) OR (MH “Measurement Error”) OR (MH “Bias (Research)”) OR (MH “Selection Bias”) OR (MH “Sampling Bias”) OR (MH “Precision”) OR (MH “Sample Size Determination”) OR (MH “Repeated Measures”) OR Psychometric* OR reliabilit* OR validit* OR reproducibility OR bias) Narrow by Language: english Narrow by SubjectAge: all adult |
| Embase (Ovid) | (swallowing/OR dysphagia/) AND ((assess* OR index* OR indices OR instrument* OR measure* OR subscale* OR scale* OR screen* OR tool* OR survey* OR inventor* OR protocol* self-report* OR patient-report* OR observation* OR rating* OR rated OR score*).ti. OR (clinical adj2 (outcome* OR evaluat*)).ti. OR (funct* adj2 (outcome* OR evaluat*)).ti. OR (quality of life adj2 (outcome* OR evaluat*)).ti. OR (health adj2 (outcome* OR evaluat*)).ti.) AND (psychometry/OR validity/OR reliability/OR measurement error/OR measurement precision/OR measurement repeatability/OR error/OR statistical bias/OR test retest reliability/OR intrarater reliability/OR interrater reliability/OR accuracy/OR criterion validity/OR internal validity/OR face validity/OR external validity/OR discriminant validity/OR concurrent validity/OR qualitative validity/OR construct validity/OR content validity/OR Psychometric* OR reliabilit* OR validit* OR reproducibility OR bias) Limit to (adults <18 to 64 years> or aged <65+ years> Limit to english language |
| PsychINFO (Ovid) | (swallowing/OR dysphagia/) AND ((assess OR index* OR indices OR instrument* OR measure* OR subscale* OR scale* OR screen* OR tool* OR survey* OR inventor* OR protocol* self-report* OR patient-report* OR observation* OR rating* OR rated OR score*).ti. OR (clinical adj2 (outcome* OR evaluat*)).ti. OR (funct* adj2 (outcome* OR evaluat*)).ti. OR (quality of life adj2 (outcome* OR evaluat*)).ti. OR (health adj2 (outcome* OR evaluat*)).ti.) AND (Psychometrics/OR Statistical Validity/OR Test Validity/OR Statistical Reliability/OR Test Reliability/OR Error of Measurement/OR Errors/OR Response Bias/OR Interrater Reliability/OR Repeated Measures/OR Psychometric* OR reliabilit* OR validit* OR reproducibility OR bias) Limit to “300 adulthood <age 18 yrs and older>” Limit to english language |
| PubMed | (“Deglutition”[Mesh] OR “Deglutition Disorders”[Mesh]) AND (assess*[Title] OR index*[Title] OR indices[Title] OR instrument*[Title] OR measure*[Title] OR subscale*[Title] OR scale*[Title] OR screen*[Title] OR tool*[Title] OR survey*[Title] OR inventor*[Title] OR protocol* self-report*[Title] OR patient-report*[Title] OR observation*[Title] OR rating*[Title] OR rated[Title] OR score*[Title] OR (clinical[Title] AND (outcome*[Title] OR evaluat*[Title])) OR (funct*[Title] AND (outcome*[Title] OR evaluat*[Title])) OR (“quality of life” [Title] AND (outcome*[Title] OR evaluat*[Title])) OR (health[Title] AND (outcome*[Title] OR evaluat*[Title]))) AND (“Psychometrics”[Mesh] OR “Reproducibility of Results”[Mesh] OR “Validation Studies as Topic”[Mesh] OR “Bias”[Mesh] OR “Observer Variation”[Mesh] OR “Selection Bias”[Mesh] OR “Diagnostic Errors”[Mesh] OR “Dimensional Measurement Accuracy”[Mesh] OR “Predictive Value of Tests”[Mesh] OR “Discriminant Analysis”[Mesh] OR psychometric* OR reliabilit* OR validit* OR reproducibilit* OR bias) Adult: 19+ years, English |
| Measurement Tool (Reference) | Purpose | Target Population | Measurement Type | Main Constructs Subscales (Number of Items per Subscale) | Response Options | Range of Score; Interpretation * |
|---|---|---|---|---|---|---|
| ASHA-NOMS Dysphagia Scale American Speech-Language-Hearing Association National Outcomes Measurement System Dysphagia Scale [34] Dungan, Gregorio [21] | A tool designed to measure both the supervision level required and diet level by assigning a single number that describes whether there has been a change in functional status after the speech therapy of patients with dysphagia | Stroke patients and those with brain lesions | Clinician-observed activities | Single scale (1)—Levels:
| Single 7-level ordinal scale (1 = nothing by mouth; 7 = no limit by swallowing) | Range: 1–7 Interpretation: ↓ scores = ↑ dysphagia severity |
| DDS Dysphagia Disorders Survey Sheppard, Hochman [28] | A quantitative observation tool with capability for discriminating swallowing and feeding pathology from functionally competent patterns and providing an objective description of the clinical presentation of swallowing and feeding disorder in developmental disability (SFD-DD) | Adults and children with developmental disability | Clinician-observed | Subscales (n Item Total = 15):
| Part 1: Rate progressive severity on each item (0–4) Part 2: Binary scoring for each item (0 = functionally correct; 1 = functionally deficient) | Range: Raw score (0–39; total from scores per subscale: RF = 0–17, FSC = 0–22) converted to DDS Percentile Interpretation: ↑ scores = ↑ dysphagia severity |
| DMSS Dysphagia Management Staging Scale Sheppard, Hochman [28] | An ordinal scale for presence and severity of swallowing and feeding disorder in developmental disability (SFD-DD) | Adults and children with developmental disability | Clinician-observed | Single scale (1)—Levels:
| Single 5-level ordinal scale (1 = no disorder; 5 = profound disorder) | Range: 1–5 Interpretation: ↑ scores = ↑ dysphagia severity |
| DSRS Dysphagia Severity Rating Scale Everton, Benfield [26] | Grades clinical dysphagia severity by quantifying how much modification is required to fluids and diet, as well as level of supervision, for safe oral intake | Stroke patients | Clinician-observed | Subscales (n Item Total = 3):
| 5-level ordinal assessment (0 = normal; 4 = no oral intake) | Range: 0–12 (total from scores per subscale) Interpretation: ↑ scores = ↑ dysphagia severity |
| EDACS Eating and Drinking Ability Classification System Sellers, Mandy [33] | A classification system for documenting and reporting how individuals with Cerebral Palsy (CP) eat and drink in everyday life. | Patients with CP | Clinician-observed (Optional: Caregiver-observed) | Single scale (1)—Levels:
| Single 5-level ordinal classification system (1 = eats and drinks safely and efficiently; 5 = Unable to eat and drink safely) | Range: 0–5 Interpretation: ↑ scores = ↑ dysphagia severity |
| EDSQ Easy Dysphagia Symptom Questionnaire Uhm, Kim [35] | A simple and rapid dysphagia questionnaire for older adults | Older adults (over 65 years old) | Clinician eliciting information based on questioning | Single scale (12):
| Binary scoring for each item (Yes / No) | Range: 0–12 (total score from the sum of all “yes” responses) Interpretation: ↑ scores = ↑ dysphagia severity |
| FOIS Functional Oral Intake Scale Crary, Carnaby Mann [23] | To determine patients’ oral intake status, developed as an appropriate tool for estimating and documenting changes in the functional eating abilities of stroke patients over time | Stroke patients | Clinician-observed | Single scale (1):
| Single 7-level ordinal scale (1 = nothing by mouth; 7 = total oral diet with no restrictions) | Range: 1–7 Interpretation: ↑ scores = ↓ impairment severity |
| IDDSI-FDS International Dysphagia Diet Standardisation Initiative Functional Diet Scale Steele, Namasivayam-MacDonald [36] | To capture the severity of oropharyngeal dysphagia, as represented by the degree of diet texture restriction recommended for the patient | Patients with dysphagia risk | Clinician-observed | Subscales:
| Foods: 7—Regular 6—Soft & bite-sized 5—Minced & moist 4—Pureed (=Drinks 4) 3—Liquidised (=Drinks 3) Drinks: 4—Extremely thick (=Foods 4) 3—Moderately thick (=Foods 3) 2—Mildly thick 1—Slightly thick 0—Thin | Range: 0 (nothing by mouth)–8 (absence of diet texture restrictions); IDDSI-FDS score based on scoring chart (number in intersecting cell of food level column and drink level row) Interpretation: ↑ scores = ↓ impairment severity |
| MASA Mann Assessment of Swallowing Ability Mann [27] | Developed as a comprehensive clinical examination for identifying eating and swallowing disorders in patients with stroke. | Stroke patients | Clinician-observed | Subscales (n Item Total = 24):
| 3, 4 and 5-level ordinal scales (different weighting) | Range: Raw score (range 38–200; total score of all items) converted to severity grouping (no abnormality detected; mild; moderate; severe) for dysphagia and aspiration. Interpretation: ↑ scores = ↓ impairment severity |
| MASA-C Mann Assessment of Swallowing Ability—Cancer Carnaby and Crary [29] | Modified version of the MASA designed for cancer patients. | Patients receiving radiotherapy for head and neck cancer | Clinician-observed | Adapted from MASA with subscales, but subscales undetermined for adapted measure (n Item Total = 24): Includes 15 of the original 24 items from the MASA, with an additional 9 cancer-specific items added | 3, 4 and 5-level ordinal scales (different weighting) | Range: Raw score (range 40–200; total score of all items) converted to severity grouping (no abnormality detected; mild; moderate; severe) for dysphagia and aspiration. Interpretation: ↑ scores = ↓ impairment severity |
| MISA McGill Ingestive Skills Assessment Lambert, Gisel [37] | An evaluative tool that assigns a numerical score to the functional abilities of the patient in the domains of self-feeding, positioning, oral motor skills for solid and liquid ingestion, and overall feeding safety. | Elderly persons with neurologic impairments | Clinician-observed | Subscales (n Item Total = 42):
| 4-level ordinal scale (1–4) | Range: 42–126 (total from scores per subscale) Interpretation: ↑ scores = ↑ function |
| M-MASA/ mMASA Modified Mann Assessment of Swallowing Ability Antonios, Carnaby-Mann [22] | Simplified version of the MASA designed to utilise highly discriminant items | Acute stroke patients | Clinician-observed | Subscales (n Item Total = 12):
| 4 and 5-level ordinal scales (different weighting) | Range: 20–100 (total score of all items); Cut-off score: ≥95 (start oral diet); <95 (non-oral diet) Interpretation: ↑ scores = ↓ impairment severity |
| SFAM Swallowing portion of the Functional Assessment Measure Hall [38] | Part of the Functional Assessment Measure (FAM) to address the patient’s functional status and document when assistance is required | First-time stroke patients | Clinician-observed | Single scale (1): Ability to safely eat a regular diet by mouth Need for assistance
| Single 7-level ordinal scale (1 = Total assistance; 7 = Complete independence) | Range: 1–7 Interpretation: ↓ scores = ↑ assistance required |
| SPEAD Swallowing Proficiency for Eating and Drinking Karsten, Hilgers [30] | A test which evaluates an individual’s (safe) swallowing capacity for eating as well as drinking | Head and neck cancer patients | Clinician-observed | For three consistencies (IDDSI level 0, 3 and 7; n Item Total = 15):
For each consistency; Mean SPEAD-rate | Numerical values; time | Range: N/A Interpretation (item level): ↑ scores = ↑ dysphagia severity Interpretation (SPEAD-rate): ↑ scores = ↑ swallowing capacity |
| Swallowing Status Moorhead, Johnson [39] | One of the five Nursing Outcome Classification (NOC) nursing outcomes that contain essential indicators to assess the entire swallowing process. | Stroke patients | Clinician-observed | Single scale; Indicators (n Item Total = 10):
| 5-level ordinal scale (1 = worst health outcome; 5 = best health outcome) | Range: 10–50 Interpretation: ↑ scores = ↑ health outcomes |
| TOMASS Test of Masticating and Swallowing Solids Athukorala, Jones [40] | A quantitative assessment of solid bolus ingestion to evaluate oral preparation and oral phase of solids | Patients with Parkinson’s disease | Clinician-observed | During a cracker swallow trial, four measures are quantified (n Item Total = 4):
| Integer values; time | Range: N/A Interpretation: ↑ scores = ↑ dysphagia severity |
| Measurement Tool | Reliability | Validity | ||||||
|---|---|---|---|---|---|---|---|---|
| Internal Consistency | Reliability † | Measurement Error ‡ | Content Validity | Criterion Validity | Construct Validity | |||
| Hypothesis Testing * | Cross-Cultural Validity ** | Structural Validity *** | ||||||
| ASHA-NOMS Dysphagia Scale American Speech-Language-Hearing Association National Outcomes Measurement System [34] Dysphagia Scale Dungan, Gregorio [21] | NR | NR | NR | Development study NR Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Using Spearman correlations coefficient, the following correlations were shown with MASA at baseline (0.623) and discharge (0.832), with G-Codes at baseline (0.858) and at discharge (0.645), as well as with FOIS at baseline (0.919) and discharge (0.950) assessments [21]. Aspect/Method: ROC curve analysis Results: The FOIS and NOMS revealed AUROC coefficients of 0.808 and 0.849, respectively, indicating a similar utility in classifying dysphagia [21]. Aspect/Method: Known group validity Results: In the baseline evaluation, the ASHA NOMS score was significantly lower in the rostral group (2.2 ± 1.9) than in the caudal group (3.7 ± 2.4). At six-month evaluations, there was no significant difference between the two groups [41]. IR (see EDSQ [35]) | N/A | NR |
| DDS Dysphagia Disorders Survey Sheppard, Hochman [28] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha used for RF (α = 0.89) and FSC (α = 0.89) subscales individually as well as together (α = 0.93) for the full DDS ratings [28]. | Aspect/Method: Inter-rater agreement Results: Kappa coefficient used for RF (κ = 0.63) and FSC (κ = 0.71) subscales individually as well as together (κ = 0.53) for the full DDS ratings [28]. | NR | Development study NR Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Using Spearman correlations coefficient, a positive and significant strong correlation was found between the DMSS and RF (ρ = 0.88, p < 0.01) and FSC (ρ = 0.91, p < 0.01) subscales as well as the scores (ρ = 0.93, p < 0.01) for the full DDS [28]. Aspect/Method: Diagnostic accuracy Results: The RF subscale achieved a sensitivity ratio of 0.88 and a specificity ratio of 0.85 whilst these ratios for the FCS subscale were 0.94 and 0.87, respectively. Sensitivity and specificity ratios were 1.00 and 0.81 for the full DSS [28]. Aspect/Method: Predictive validity Results: The NPV was 0.96 for the RF and 0.98 for the FCS, whilst PPV was 0.61 for the RF and 0.67 for the FCS. Negative and positive predictive values were 1.00 and 0.44 for the full DSS [28]. | N/A | Aspect/Method: Factor analysis (principal components analysis) Results: Results of the factor analysis consistently show that regardless of the sample or the sub-scale, that there is a single factor that accounts for approximately 50% of the total variance among the 15 valuables (seven items for the RF and eight items for the FSC) entered into the equation [28]. |
| DMSS Dysphagia Management Staging Scale Sheppard, Hochman [28] | NR | NR | NR | Development study NR Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Discriminative validity Results: Between two test sites, cross tabular analyses were conducted on the DMSS ratings comparing the two samples. Although the chi-square statistic was significant (χ2 = 47.84, 4 df, p < 0.01), the Mann–Whitney U statistic, which assesses ordinal differences between two categories was not (p = 0.41); the gamma statistic, which measures ordinality (γ = 0.06, p = 0.43) was also not significant [28]. IR (see DDS [28]) | N/A | NR |
| DSRS Dysphagia Severity Rating Scale Everton, Benfield [26] | Aspect/Method: Cronbach’s alpha Results: “Good” (Cronbach’s alpha α = 0.89 and α = 0.88) at baseline, varied between “Good” and “Excellent” (α = 0.88, α = 0.87 and α = 0.80–0.92) over the first two weeks, and “Excellent” (α = 0.92, α = 0.91 and α = 0.96) at 12 weeks [26]. | Aspect/Method: Inter-rater agreement Results: ICC was “Good” (ICC = 0.837, 95% CI 0.740, 0.900) for the Fluids subscale, “Excellent” (ICC = 0.985, 95% CI 0.974, 0.991) for the Diet subscale, “Excellent” (ICC = 0.952, 95% CI 0.921, 0.971) for the Supervision subscale, and “Excellent” (ICC = 0.955, 95% CI 0.925, 0.973) for the full DSRS score [26]. Aspect/Method: Intra-rater agreement Results: ICC was “Excellent” (ICC = 1.00, 95% CI 1.00, 1.00) for all three subscales and the full DSRS score [26]. | NR | Development study The DSRS is a clinician-rated scale that was developed from the dysphagia outcome and severity scale (DOSS) [26]. Content validity study Relevance: Determined via survey responded to by 10 SLTs, all but two components of the DSRS subscales had “excellent” relevance (I-CVI > 0.90); The S-CVI was 0.84 (good) for the Fluids subscale, 0.84 (good) for the Diet subscale and 0.96 (excellent) for the Supervision subscale Comprehensibility: “Need for more detailed descriptors”—some respondents felt that more detail was needed to define terms, for example, “selected textures”, or that a description of bolus cohesiveness/food consistency should be included. Respondents also noted that some terms were subjective. Comprehensiveness: Responses from 10 UK-based SLTs indicated that the items were comprehensive for 30% of items in the Fluids subscale, 20% of items in the Solids subscale, and 60% of items in the Supervision subscale. Similarly, the wording was deemed clear for 50%, 30% and 80% of the items in the Fluids, Solids and Supervision subscales, respectively [26]. | N/A | Aspect/Method: Convergent validity Results: For the largest of the four trials reported on, Spearman’s rank correlation coefficients were determined for aspiration (PAS using VFS), swallowing ability (TOR-BSST and FOIS), disability (Barthel index), impairment (NIHSS) and dependency (modified Rankin Scale) at baseline and weeks 2 and 13. These values were rs = 0.488, rs = 0.387, and rs = 0.398 for VFS-PAS; rs = −0.167, rs = −0.459, and rs = −0.520 for TOR-BSST; rs = 0.020, rs = 0.301, and rs = 0.117 for NIHSS; rs = −0.279, rs = −0.517, and rs = −0.407 for the Barthel index, and rs = 0.179, rs = 0.382, and rs = 0.279 for the modified Rankin scale. For other trials, see paper [26]. | N/A | NR |
| EDACS Eating and Drinking Ability Classification System Sellers, Mandy [33] | NR | Aspect/Method: Inter-rater agreement Results: Kappa coefficient was κ = 0.866 (ICC = 0.867, 95% CI 0.813–0.906; p < 0.001) with 80.3% exact agreement between clinicians for EDACS as well as κ = 0.713 (ICC = 0.885, 95% CI 0.837–0.919; p < 0.001) with 88.0% exact agreement for level of assistance [42]. Aspect/Method: Inter-rater agreement Results: Kappa coefficient was κ = 0.884 (ICC = 0.717, 95% CI 0.538–0.830; p < 0.001) with 61.1% exact agreement between clinician and participant/ caregiver for EDACS as well as κ = 0.823 (ICC = 0.826, 95% CI 0.712–0.896; p < 0.001) with 79.6% exact agreement for level of assistance [42]. Aspect/Method: Inter-rater agreement Results: Absolute agreement between clinicians for EDACS was 78%, with kappa = 0.72 and ICC = 0.93 (95% CI 0.90–0.95) indicating substantial agreement. Absolute agreement between clinicians for degree of assistance was 87%, with Kappa = 0.80 and ICC = 0.92 (95% CI 0.88–0.94) indicating excellent agreement [33]. Aspect/Method: Inter-rater agreement Results: Absolute agreement between clinicians and parents for EDACS was 58% with kappa = 0.45 and ICC = 0.86. 95% (CI 0.76–0.92) indicating moderate agreement. Absolute agreement between clinicians and parents for level of assistance was 79% with kappa = 0.64 and ICC = 0.77. 95% (CI 0.62–0.87) indicating moderate to substantial agreement [33]. | NR | Development study Development involved four distinct stages: (1) an original draft was constructed from the literature and clinical experience, (2) the draft was examined and revised using several iterations of a Nominal Group Process, (3) further examination and revision to the EDACS took place within two rounds of an online Delphi survey until agreement about the content was reached, and (4) the final stage assessed reliability between speech and language therapists and between speech and language therapists and parents [33]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Using Kendall’s tau-b, correlations were evaluated with FOIS (Kτ = −0.346), SWAL-QOL (Kτ = −0.389), total symptom score (Kτ = −0.476), GMFCS (Kτ = 0.140), and (Kτ = 0.180) with MACS for EDACS as well as FOIS (Kτ = −0.183), SWAL-QOL (Kτ = −0.234), total symptom score (Kτ = −0.263), GMFCS (Kτ = 0.497), and (Kτ = 0.584) for level of assistance [42]. Aspect/Method: Convergent validity Results: There was a significant positive correlation (Kendall’s tau = 0.69, p < 0.01) between EDACS level and level of assistance required to bring food and fluid to the mouth and a statistically significant but only moderate positive correlation (Kendall’s tau = 0.5, p < 0.01) between the EDACS and the GMFCS [33]. | N/A | NR |
| EDSQ Easy Dysphagia Symptom Questionnaire Uhm, Kim [35] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s α coefficient was 0.785 [35] | NR | NR | Development study Following a review of existing questionnaires, the EDSQ was established by consensus of three physiatrists. We extracted 12 “yes/no” questions for dysphagia symptoms considering their easy applicability to older adults [35]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Showed significant correlations, using Spearman correlation analysis, with the MWST (r = −0.468, p = 0.001), the ASHA NOMS swallowing scale (r = −0.635, p < 0.001) and VDS (r = 0.449, p = 0.001) scales [35]. Aspect/Method: Diagnostic accuracy Results: According to the ROC curve analysis, the optimal cut-off score to maximize the sum of sensitivity and specificity was 5, with a sensitivity of 90.9% and a specificity of 67.5% [35]. | N/A | NR |
| FOIS Functional Oral Intake Scale Crary, Carnaby Mann [23] | NR | Aspect/Method: Inter-rater agreement Results: Kappa coefficient between paired judges ranged from κ = 0.86 to κ = 0.91, perfect agreement ranged from 85–95%, and Spearman’s rank correlations ranged from ρ = 0.98 to ρ = 0.99 [23]. | NR | Development study Initially, the scale included 10 items. After pilot application in a tertiary care teaching hospital, unused items were omitted, and the remaining 7 items were retained for subsequent psychometric analysis. Levels 1 through 3 relate to varying degrees of nonoral feeding; levels 4 through 7 relate to varying degrees of oral feeding without nonoral supplementation. These latter scale levels consider both diet modifications and patient compensations, but all levels focus on what the patient consumes by mouth on a daily basis [23]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: The FOIS score was significantly associated (χ², p, Cramer’s V correlation) with MRS (28.6, <0.001, 0.31), MBI (30.9, <0.001, 0.32), and the MASA (33.8, <0.001, 0.53) at admission; and then with MRS (64.9, <0.001, 0.49), MBI (64.6, <0.001, 0.49), and MASA (60.7, <0.001, 0.76) at 1-month post-stroke [23]. Aspect/Method: Hypothesis testing (reported as consensual validity) Results: Agreement with the predefined scale scores ranged from 81% to 98%. The Kendall concordance was 0.90 [23]. Aspect/Method: Convergent validity Results: The FOIS score was significantly associated (χ², p, Cramer’s V correlation) with both the presence of aspiration (30.17, <0.011, 0.40) and dysphagia (12.97, 0.011, 0.26) as well as dysphagia severity (56.48, <0.001, 0.54) but not significantly associated with aspiration severity [23]. Aspect/Method: Convergent validity Results: Using two-tailed Pearson correlations, between FOIS and PAS, r = −0.201 (p = 0.140) for semisolids and r = −0.218 (p = 0.110) for liquids. Between FOIS and pooling score, r = −0.355 (p = 0.008) for semisolids and r = −0.180 (p = 0.189) for liquids [43]. Aspect/Method: Diagnostic accuracy Results: When compared to PAS, for identifying dysphagia for liquids, FOIS had a sensitivity of 6.3% and a specificity of 94.9%, whilst for semisolids, these values were 6.1% and 95.5%, respectively. When compared with pooling score, sensitivity was 10% and specificity was 97.1% for liquids, whilst values were 13.6% and 100%, respectively, for semisolids [43]. Aspect/Method: Convergent validity Results: Using Spearman’s rank correlation rho at four time points, there was a weak and non-significant correlation (r = −0.20–0.13; p = 0.40–0.81) with PAS and a moderate significant correlation with EAT-10 (r = −0.53; p = 0.002) during treatment and (r = −0.56; p = 0.003) 3 months after treatment [44]. IR (see ASHA-NOMS [21], DSRS [26], EDACS [33], IDDSI-FDS [36], and SPEAD [30]) | N/A | NR |
| IDDSI-FDS International Dysphagia Diet Standardisation Initiative Functional Diet Scale Steele, Namasivayam-MacDonald [36] | NR | Aspect/Method: Inter-rater agreement Results: Using Kendall concordance, agreement was W = 0.873 overall and, across the successive quartile batches, was W = 0.88, W = 0.884, W = 0.896, and W = 0.819, respectively. Average ICCs per batch were 0.965, 0.966, 0.971, and 0.939, respectively, with 95% confidence interval boundaries of 0.872–0.976 [36]. | NR | Development study NR Content validity study Relevance: Respondents indicated general agreement with the bracketed range concept (59% in favour) and 28% of respondents recommended that tolerance of consistencies between the bracketed boundaries on the IDDSI framework should not be assumed, but confirmed during assessment on a case-by-case basis. There was strong agreement (77%) that the IDDSI Functional Diet Scale score should reflect the main diet recommendation and not reflect therapeutic advancement [36]. Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Strong correlation (Spearman correlation: ρ = 0.84, p < 0.001) IDDSI-FDS with FOIS scores for case scenarios including diet texture recommendations [36]. | N/A | NR |
| MASA Mann Assessment of Swallowing Ability Mann [27] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha α = 0.9166 [27] | Aspect/Method: Inter-rater agreement Results: Kappa coefficient was κ = 0.82 for dysphagia and κ = 0.75 for aspiration [27]. | NR | Development study A panel of 15 content experts identified items that they felt should be included in a clinical assessment of dysphagia and provided feedback for minor modifications [27]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: ROC curve analysis Results: In ROC analysis for predicting the development of pneumonia, the cut-off value was 170.5 (sensitivity 0.70, specificity 0.83; AUC 0.82, 95% CI 0.78–0.87, p < 0.01) for MASA [45]. Aspect/Method: Diagnostic accuracy Results: As a predictor of aspiration, the MASA had a specificity of 69.9% and a sensitivity of 71.4%. According to previous cognitive assessment, patients were divided into subgroups based on cognitive function. Sensitivity ranged from 50.0% for mild and moderate to 90.9% for severely impaired patients, whilst specificity ranged from 38.1% for severe to 86.7% for mildly impaired patients [24]. Aspect/Method: Predictive validity Results: As a predictor of aspiration, the MASA has a positive predictive value of 64.3% and a negative predictive value of 76.3%. According to previous cognitive assessment, patients were divided into subgroups based on cognitive function. PPV ranged from 33.3% for mild to 69.8% for severe impairment, whilst NPV ranged from 63.6% for moderate to 92.9% for mild impairment [24]. Aspect/Method: Convergent validity Results: Using Spearman’s correlation coefficient, there was a significant positive correlation (r = 0.961, p < 0.01) with the mMASA [24]. Aspect/Method: Diagnostic accuracy Results: As a predictor of aspiration, the ORR and %TNS were calculated for the MASA. When using “probable” as the cut-off, specificity was 74.4% (95% CI 63.2, 83.6), sensitivity was 64.6% (95% CI 49.5, 77.8), PPV = 60.8 (95% CI 46.1, 74.1), and NPV = 77.3 (95% CI 67.8, 86.9) for MASA’s ORR. When using “moderate-severe” as the cut-off, specificity was 85.9% (95% CI 76.2, 92.7), sensitivity was 16.7% (95% CI 7.5, 30.2), PPV = 42.1 (95% CI 20.3, 66.5), and NPV = 62.6 (95% CI 52.7, 71.8) for MASA’s %TNS [46]. Aspect/Method: ROC curve analysis Results: ROC analysis resulted in an ROC area of 0.50 for the %TNS and 0.72 for the ORR [46]. IR (see ASHA-NOMS [21], FOIS [23], and MASA-C [29]). | N/A | NR |
| MASA-C Mann Assessment of Swallowing Ability—Cancer Carnaby and Crary [29] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha α = 0.94 [29]. | Aspect/Method: Test-retest reliability Results: ICC = 0.96 at baseline and ICC = 0.92 at post-treatment [29]. Aspect/Method: Inter-rater agreement Results: ICC = 0.96 (95% CI 0.94–0.98) [29]. Aspect/Method: Intra-rater agreement Results: ICC = 0.94 (95% CI 0.91–0.97) [29]. | NR | Development study Developers of the MASA-C identified specific items via literature review and a panel of 5 expert reviewers rated the potential new items, then revised items were selected on the basis of correlation, with items included on the basis of correlation for Cronbach’s alpha of α = 0.85 [29]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | Aspect/Method: ROC curve analysis Results: Presence of dysphagia (score ≤ 185): AUC = 0.95 (0.84–0.99; p < 0.0001); Se = 83%, Sp = 96%. Likewise, predictive values (PPV = 95%, NPV = 86%) were strong. Presence of aspiration (score ≤ 176): AUC = 0.90 (0.793–0.971; p < 0.0001), with Se, Sp, PPV and NPV not reported [29]. Aspect/Method: Criterion Validity Results: Using Spearman correlations coefficient, a moderately strong (r = 0.699) correlation was found with MASA [29]. | Aspect/Method: Convergent validity Results: Using Spearman correlations coefficient, strong correlation (r = 0.8295) with FOIS, a moderate (r = 0.488) correlation with FACT H&N, and a modest correlation (r = −0.3901) with VFE [29]. Aspect/Method: Predictive validity Results: Interpretation of the final model (log odds) revealed that for every 10-point rise in MASA-C score, the odds of achieving a favourable outcome posttreatment rose by 15.49 times compared to patients not improving their MASA-C score [29]. | NR | Aspect/Method: EFA Results: Four factors containing >4 items were retained producing a 23-item measure. Results showed that all items loaded significantly on their respective factors, ranging from 0.7 to 0.90 for acute effects, 0.54 to 0.73 for pharyngeal function, 0.65 to 0.8 for oral function, and 0.47 to 0.85 for cognitive–motor function [29]. |
| MISA McGill Ingestive Skills Assessment Lambert, Gisel [37] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha α = 0.86–0.91 across the 5 subscales [37]. | Aspect/Method: Inter-rater agreement Results: ICC = 0.85 (95% CI 0.78-.090) for total MISA score and ICC = 0.68 (95 % CI 0.55–0.78)–0.88 (95% CI 0.82–0.92) across the 5 subscales [30] Aspect/Method: Inter-rater agreement Results: Person’s correlation coefficient was used for each subscale, with r = 0.95 (80% exact agreement) for “Positioning”, r = 0.97 (93%) for “Textures”, r = 0.92 (67%) for “Self-feeding, r = 0.92 (45%) for Solid Ingestion, and r = 0.95 (75%) for Liquid Ingestion [37]. | NR | Development study The development of the assessment began in 1996 with a review of the literature. To select items, a focus group of clinicians was assembled. At the end of item development, the assessment was named the McGill Ingestive Skills Assessment (MISA) and had 190 items in 7 scales. After a field test and item reduction, the adequacy of each of the items was examined. Items that had correlations >0.80 with at least one other item on the assessment were identified. Each pair of redundant items was inspected, and a judgment made whether to retain both items or eliminate one. If the items appeared to have a true redundancy, the item which was worded less clearly was eliminated [37]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Using Spearman correlations coefficient, a positive and significant moderate correlation (ρ = 0.45; p < 0.05) was found with the Functional Independence Measure and a positive yet weak correlation (ρ = 0.25, p < 0.05) was found with 3MS [32]. Aspect/Method: Contrasted groups validity Results: Using Wilcoxon Rank-Sum tests, p = 0.11 (p > 0.05) for participants taking psychoactive medication, p = 0.28 (p > 0.05) for participants with decubiti, and p = 0.01 (p < 0.05) for participants who wear dentures during meals [32]. Aspect/Method: Predictive validity Results: Survival analyses revealed that the MISA scores are predictive of death using a Cox proportional hazards model (hazard ratio = 0.960; 95% CI 0.940, 0.980), and of time to pulmonary infection using a flexible model. Scores on the Solid Ingestion and Self-feeding scales are predictive of death using the Cox model, and the Texture Management scale is predictive of death using the flexible model [47]. Aspect/Method: Contrasted groups validity Results: Using Spearman correlations, The MISA score correlated moderately with age (r = −0.58, p < 0.001) but was low with gender (r = −0.34, p < 0.02). Both were negative and only age was significant. The relationship with stroke severity (discharge destination) was significant (H = 12.7, df = 3, p < 0.005). Dysphagia status was highly significant (p < 0.0001), but location of lesion was not (p < 0.01). Correlations between the MISA score and first or repeated stroke, and between MISA score and location of lesion were low, negative, and non-significant (r = −0.07, p < 0.67 and r = −0.14, p < 0.35), respectively. Low and non-significant correlations were obtained between the MISA score and type of stroke (r = 0.06, p < 0.7) [48]. | N/A | NR |
| M-MASA/ mMASA Modified Mann Assessment of Swallowing Ability Antonios, Carnaby-Mann [22] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha α = 0.94 [22]. | Aspect/Method: Inter-rater agreement Results: Kappa coefficient of κ =0.76 (SE = 0.082) between neurologists [22]. | NR | Development study: Original MASA data were statistically reviewed to identify potential screening items. Screening items were selected on the basis of correlations with total (the correlation with the total score had to be at least 0.4), and each item’s individual Cronbach alpha (≥0.85). In addition, the items were considered with regard to the familiarity and use of each potential item within currently administered clinical neurologic assessments [22]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | Aspect/Method: ROC curve analysis using optimal cut-off point Results: The optimal cut point on the mMASA to identify dysphagia was 94 of 100 possible points. Using this cut-off point, AUC = 0.93 (95% CI: 0.89–0.97) for the first rater and AUC = 0.94 (95% CI: 0.87–0.96) for the second rater [22]. | Aspect/Method: Convergent validity Results: Using Spearman’s correlation coefficient, there was a moderate negative (r = −0.349, p = 0.044) correlation with PAS. Additionally, with cognitive function tests, significant correlations were shown, with ρ = 0.564 (p < 0.05) for MMSE, ρ = 0.641 (p < 0.05) for MoCA, and ρ = −0.676 (p < 0.05) for CDR [49]. Aspect/Method: Diagnostic accuracy Results: Based on results from the ROC analysis of the two raters, detection of dysphagia was high (sensitivity = 92% and 87%; specificity = 86.3% and 84.2%), whilst PPV was 79.4% and 75.8% and NPV was 95.3% and 92% [22]. | NR | NR |
| SFAM Swallowing portion of the Functional Assessment Measure Hall [38] | NR | Aspect/Method: Inter-rater agreement Results: ICC = 0.975 (p≤ 0.01) at admission and ICC = 0.964, (p≤ 0.01) at discharge as well as Spearman rho correlations of ρ = 0.899 (p < 0.01) at admission and ρ = 0.863 (p < 0.01) at discharge [50]. | NR | Development study NR Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Spearman rho correlations were performed on the SFAM and FOIS, and a strong significant relationship was found (ρ = 0.926, p < 0.01) at admission and (ρ = 0.706, p < 0.01) at discharge [50]. Aspect/Method: Convergent validity Results: Strong correlations (r = 0.779, p ≤ 0.001) with the food texture ratings at admission, and the SFAM levels and the liquid consistency ratings (r = 0.762, p ≤ 0.001) at admission. Moderately strong correlations (r = 0.673, p ≤ 0.001) were apparent between the SFAM levels and the food texture ratings at discharge as well as with the SFAM levels and the liquid consistency ratings (0.567, p ≤ 0.001) at discharge [51]. Aspect/Method: Predictive validity Results: When predicting discharge for age, 72% of younger (50 years old and younger) patients reached a SFAM Level 5, 6, or 7 (mild to no dysphagia) as compared to 51% of older patients. 59% of younger patients had a length of stay of 14 days or less as compared to 27% of the older patients. When predicting discharge for patients with a cognitive FIM score of 14 or lower, 82% had severe dysphagia (SFAM score of 1 or 2) as compared to 35% that had moderate dysphagia (SFAM score of 3 or 4). 61% had a length of stay of 15 days or more as compared to 39% who had a length of stay of 14 days or less [52]. | N/A | NR |
| SPEAD Swallowing Proficiency for Eating and Drinking Karsten, Hilgers [30] | NR | Aspect/Method: Test-retest reliability Results: ICC = 0.90 (0.86–0.94), 0.88 (0.83–0.92), 0.89 (0.83–0.93) of duration and ICC = 0.84 (0.77–0.90), 0.68 (0.56–0.78), 0.60 (0.46–0.73) of number of swallows for thin, thick and solid consistencies, respectively. ICC = 0.89 (0.83–0.93) for number of chews [30]. Aspect/Method: Intra-rater agreement Results: ICC = 1.00 (1.00–1.00), 0.98 (0.97–0.99), 0.98 (0.96–0.98) of duration and ICC = 0.99 (0.99–1.00), 0.96 (0.95–0.97), 0.96 (0.94–0.97) of number of swallows for thin, thick and solid consistencies, respectively. ICC = 1.00 (0.99–1.00) for number of chews [30]. Aspect/method: Inter-rater agreement Results: ICC = 0.98 (0.97–0.99), 0.97 (0.96–0.98), 0.95 (0.93–0.97) of duration and ICC = 0.93 (0.90–0.95), 0.74 (0.65–0.81), 0.75 (0.65–0.82) of number of swallows for thin, thick and solid consistencies, respectively. ICC = 0.98 (0.98–0.99) for number of chews [30]. | NR | Development study NR Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Spearman correlations coefficient was used with SPEAD-rate and subjective swallowing outcomes, with ρ = 0.71 (p < 0.001) for self-rated percentage eating and drinking speed, ρ = 0.72 (p < 0.001) for self-rated percentage swallow function, ρ = −0.68 (p < 0.001) for SWAL-QOL total score, and ρ = −0.70 for degree of dysphagia by SLP. Similarly, correlations were found with SPEAD-rate and objective swallowing outcomes, with ρ = 0.70 (p < 0.001) for FOIS, ρ = −0.51 (p = 0.001) for DIGEST grade, ρ = −0.50 (p = 0.001) for aspiration on VFS, and ρ = 0.49 (p < 0.001) for maximal mouth opening [30]. Aspect/Method: Divergent validity Results: Correlations of the SPEAD-rate with participant-reported dyspnoea, pain and fatigue were weak (ρ between 0.25 and 0.28), again using Spearman correlations coefficient [30]. Aspect/Method: Discriminant validity Results: As hypothesized, patients had a median SPEAD-rate of 2 g/s (range 0–10), compared to 6 g/s (range 2–11) for healthy participants corresponding to a large effect size of 0.56. When dividing participants into four groups based on degree of dysphagia rated by the SLP (no, mild, moderate and severe, with the healthy participants rated as no), SPEAD-rate decreases (p < 0.001) with increasing degree of dysphagia [30]. Aspect/Method: Diagnostic accuracy Results: When using the SPEAD-rate to discriminate between patients and healthy participants, the area under the ROC-curve was 0.82, with a cut-off value for optimal sensitivity and specificity ratio of 4.2 g/s (sensitivity 80% and specificity 79%). When using the SPEAD-rate to determine aspiration, the area under the ROC-curve was 0.79, with an optimal cut-off value of 1.2 g/s, giving 100% sensitivity and 57% specificity [30]. | N/A | NR |
| Swallowing Status Moorhead, Johnson [39] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s α for the overall scale = 0.954; values for when individual items were deleted ranged from α = 0.945 to α = 0.956 [25]. Aspect/Method: Results: Person reliability estimate = 0.905; indicating good internal consistency [53]. | Aspect/Method: Test-retest reliability Results: ICC reported per indicator with values ranging from ICC = 0.571 (0.258–0.776) to ICC = 1.00 (1.00–1.00) for initial evaluation and from ICC = 0.727 (0.410–0.874) to ICC = 1.00 (1.00–1.00) after 72 h [25]. | NR | Development study An integrative review was performed for the Conceptual Analysis, which enabled finding papers addressing this topic, in addition to dissertations, theses and books. The NOC indicators were revised, and conceptual and operational definitions were developed for each indicator. Additionally, for each magnitude, that is, for each of the five points on the Likert scale, an operational definition was established to help nurses during assessments [54]. Content validity study ICCs were used to determine agreement between nurses both with definitions, ranging from ICC = 0.899 (95% CI 0.848–0.934) to ICC = 1.00 (95% CI 1.00–1.00) across all indicators, and without definitions, ranging from ICC = −0.071 (95% CI −0.260–0.131) to ICC = 0.626 (95% CI 0.368–0.775) across all indicators [54]. Relevance: A panel of 11 judges examined the relevance and clarity of each indicator, with one indicator not reaching the CVI cut-off point of 0.80. This indicator was retained due to its importance to clinical practice according to the literature [54]. Comprehensibility: Regarding clarity, each indicator and respective definition was examined according to the following: −1 (inappropriate definition/indicator), 0 (somewhat appropriate definition/indicator), and +1 (appropriate definition/indicator). The judges had the liberty to suggest changes concerning the names of the indicators, on their grouping or exclusion [54]. Comprehensiveness: NR | N/A | Aspect/Method: IRT (2PPC Model) Results: The parametric bootstrap approximation to Pearson chi-squared goodness-of-fit measure found that values obtained in the sample are similar to those obtained from the model (p = 0.510). The fit on the two-way margins based on 2PPC model did not present discrepancies in percentages of adjustment among indicators (chi-square residuals < 3.5), denoting similarity between observed frequencies in sample and expected frequencies from the model. These results show good fit to the model and unidimensionality of the scale [25]. | Aspect/Method: Conducted Differential Item functioning (DIF) analysis for gender, age, type of stroke, and stroke severity [25]. Results: The measure did not show DIF for gender, age, type of stroke, and severity of stroke, indicating that these characteristics did not affect the final Swallowing Status outcome [25]. | Aspect/Method: Rasch analysis Results: The results showed good fit to the model and that the measure is unidimensional [25]. Analysis of standardized residuals in PCA indicates that the Rasch dimension explained 67.7%of data variance. It was slightly above guidelines for assessing unidimensionality via PCA (50%). The largest secondary dimension (the first contrast in the residuals) explained 8.4%. Many indicators presented disordered categorical response thresholds, with overlapping categories, which suggested that the scale of responses (5 points) was not appropriate and contributed to inadequate fit of items Changing from 5 points to 3 points showed the best fit for the items and people. Item difficulty for the NOC with 3 points ranged from −1.36 to 2.40 and infit statistics from 0.75 to 1.34 indicated good fitness [53]. |
| TOMASS Test of Masticating and Swallowing Solids Athukorala, Jones [40] | Aspect/Method: Cronbach’s alpha Results: Cronbach’s alpha ranged from α = 0.71 to α = 0.82 [55] Aspect/Method: Test-retest reliability Results: Cronbach’s alpha ranged from α = 0.94 to α = 0.99 [31]. | Aspect/Method: Inter-rater agreement Results: Values ranged from ICC = 0.96 (95% CI 0.927–0.979) to ICC = 1.0 across items for the clinical group and from ICC = 0.97 (95% CI 0.950–0.986) to ICC = 0.99 (95% CI 0.995–0.998) for the control group [56]. Aspect/Method: Intra-rater agreement Results: Values ranged from ICC = 0.97 (95% CI 0.954–0.987) to ICC = 1.0 across items for the clinical group and from ICC = 0.99 (95% CI 0.984–0.995) to ICC = 1.0 for the control group [56]. Aspect/Method: Inter-rater agreement Results: ICC > 0.95 for the number of masticatory cycles and time taken. The ICC = 0.73 for interrater reliability of the number of swallows recorded by instrumental assessment [31]. Aspect/Method: Test-retest reliability Results: ICC values ranged from ICC = 0.83 to ICC = 0.98 [31]. Aspect/Method: Inter-rater agreement Results: Median ICCs were reported with 95% confidence intervals for each outcome measure: ICC = 0.92 (0.75–0.91) for number of bites, ICC = 0.97 (0.92–0.96) for masticatory cycles, ICC = 1.00 (0.99–1.00) for total time, and ICC = 0.58 (0.51–0.67) for number of swallows, with 90% (93%-97%) exact agreement for signs of aspiration [57]. Aspect/Method: Intra-rater agreement Results: Median ICCs were reported with 95% confidence intervals for each outcome measure. For immediate agreement, ICC = 1.00 (0.99–1.00) for number of bites, ICC = 1.00 (0.98–1.00) for masticatory cycles, ICC = 1.00 (0.95–1.00) for total time, and ICC = 0.90 (0.87–0.97) for number of swallows, with 100% (96%-100%) exact agreement for signs of aspiration. For delayed agreement, ICC = 0.99 (0.91–1.00) for number of bites, ICC = 0.98 (0.96–0.99) for masticatory cycles, ICC = 1.00 (0.99–1.00) for total time, and ICC = 0.81 (0.71–0.87) for number of swallows, with 100% (94%-100%) exact agreement for signs of aspiration [57,58]. | NR | Development study TOMASS was developed from the timed water swallow test to assess the swallowing rate of solids. Within the initial small sample, surface electromyography (EMG) measures derived from the masseter muscles were highly correlated with visual observation of chewing cycles, with the average Pearson correlation coefficient across four measurement sessions at r = 0.93, p < 0.05 [40]. Content validity study Relevance: NR Comprehensibility: NR Comprehensiveness: NR | N/A | Aspect/Method: Convergent validity Results: Using Spearman correlations coefficient, a positive and significant moderate correlation between ‘number of swallows per cracker’ and mealtime duration (r = 0.49; p < 0.002; 95% CI = 0.20–0.70) and a positive and significant moderate correlation between ‘total time’ and mealtime duration (r = 0.41; p < 0.011; 95% CI= 0.10–0.65) were found. Bland-Altman plot between ‘number of swallows per cracker’ and ‘number of white-outs’ observed during FEES was −0.02 with 95% CI = −1.7 to 1 [56]. Aspect/Method: Known group validity Results: To analyse known-group validity, a Mann–Whitney U-test was used to compare the clinical and the control group, with U = 645 (p = 0.224) for discrete bites per cracker, U = 527.5 (p < 0.05) for masticatory cycles per cracker, U = 520.5 (p < 0.05) for swallows per cracker, and U = 457.5 (p < 0.05) for total time [56]. Aspect/Method: Hypothesis testing Results: The ICC value between objective and behavioural measures of the number of masticatory cycles was 0.99 with a 95% confidence interval from 0.98 to 0.99. For number of swallows, the ICC was 0.85 with a 95% confidence interval from 0.79 to 0.90. The ICC for time was 0.99 with a 95% confidence interval from 0.91 to 1.0 [31]. Aspect/Method: Contrasted groups validity Results: The effects of sex were significant across all variables (discrete bites, masticatory cycles and swallows per cracker, total time to ingest, masticatory cycles per bolus, and swallows per bolus) with the exception of the derived measures of average time per masticatory cycle and average time per swallow [31]. | N/A | NR |
| Measurement Instrument | RELIABILITY | VALIDITY | ||||||
|---|---|---|---|---|---|---|---|---|
| Internal Consistency | Reliability † | Measurement Error ‡ | Content Validity | Criterion Validity | Construct Validity | |||
| Hypothesis Testing * | Cross-Cultural Validity ** | Structural Validity *** | ||||||
| ASHA-NOMS DS | NR | NR | NR | NR | N/A | Yes ◊ | N/A | NR |
| DDS | Yes | Yes | NR | NR | N/A | Yes | N/A | Yes |
| DMSS | NR | NR | NR | NR | N/A | Yes ◊ | N/A | NR |
| DSRS | Yes | Yes | NR | Yes | N/A | Yes | N/A | NR |
| EDACS | NR | Yes | NR | Yes | N/A | Yes | N/A | NR |
| EDSQ | Yes | NR | NR | Yes | N/A | Yes | N/A | NR |
| FOIS | NR | Yes | NR | Yes | N/A | Yes ◊ | N/A | NR |
| IDDSI-FDS | NR | Yes | NR | Yes | N/A | Yes | N/A | NR |
| MASA | Yes | Yes | NR | Yes | N/A | Yes ◊ | N/A | NR |
| MASA-C | Yes | Yes | NR | Yes | Yes | Yes | NR | Yes |
| MISA | Yes | Yes | NR | Yes | N/A | Yes | N/A | NR |
| M-MASA/mMASA | Yes | Yes | NR | Yes | Yes | Yes | NR | NR |
| SFAM | NR | Yes | NR | NR | N/A | Yes | N/A | NR |
| SPEAD | NR | Yes | NR | NR | N/A | Yes | N/A | NR |
| Swallowing Status | Yes | Yes | NR | Yes | N/A | Yes | Yes | Yes |
| TOMASS | Yes | Yes | NR | Yes | N/A | Yes | N/A | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordier, R.; Speyer, R.; Martinez, M.; Parsons, L. Reliability and Validity of Non-Instrumental Clinical Assessments for Adults with Oropharyngeal Dysphagia: A Systematic Review. J. Clin. Med. 2023, 12, 721. https://doi.org/10.3390/jcm12020721
Cordier R, Speyer R, Martinez M, Parsons L. Reliability and Validity of Non-Instrumental Clinical Assessments for Adults with Oropharyngeal Dysphagia: A Systematic Review. Journal of Clinical Medicine. 2023; 12(2):721. https://doi.org/10.3390/jcm12020721
Chicago/Turabian StyleCordier, Reinie, Renée Speyer, Matthew Martinez, and Lauren Parsons. 2023. "Reliability and Validity of Non-Instrumental Clinical Assessments for Adults with Oropharyngeal Dysphagia: A Systematic Review" Journal of Clinical Medicine 12, no. 2: 721. https://doi.org/10.3390/jcm12020721