
Evaluation of the Performance of ACR TI-RADS Also Considering Those Nodules with No Indication of FNAC: A Single-Center Experience

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Institutional Guidelines for the Management of Thyroid Nodules
2.2. Case Selection
2.3. Measures and Reference Standard
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C.M. Very High Prevalence of Thyroid Nodules Detected by High Frequency (13 MHz) Ultrasound Examination. Eur. J. Clin. Investig. 2009, 39, 699–706. [Google Scholar] [CrossRef]
- Russ, G.; Leboulleux, S.; Leenhardt, L.; Hegedüs, L. Thyroid incidentalomas: Epidemiology, risk stratification with ultrasound and workup. Eur. Thyroid J. 2014, 3, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, J.P.; Morris, J.C.; Montori, V.M. Thyroid cancer: Zealous imaging has increased detection and treatment of low risk tumours. BMJ 2013, 347, f4706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grussendorf, M.; Ruschenburg, I.; Brabant, G. Malignancy rates in thyroid nodules: A long-term cohort study of 17,592 patients. Eur. Thyroid J. 2022, 11, e220027. [Google Scholar] [CrossRef]
- Durante, C.; Grani, G.; Lamartina, L.; Filetti, S.; Mandel, S.J.; Cooper, D.S. The diagnosis and management of thyroid nodules: A review. JAMA J. Am. Med. Assoc. 2018, 319, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Su, H.K.; dos Reis, L.L.; Lupo, M.A.; Milas, M.; Orloff, L.A.; Langer, J.E.; Brett, E.M.; Kazam, E.; Lee, S.L.; Minkowitz, G.; et al. Striving toward standardization of reporting of ultrasound features of thyroid nodules and lymph nodes: A multidisciplinary consensus statement. Thyroid 2014, 24, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- American Institute of Ultrasound in Medicine; American College of Radiology; Society for Pediatric Radiology; Society of Radiologists in Ultrasound. AIUM practice guideline for the performance of a thyroid and parathyroid ultrasound examination. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2013, 32, 1319–1329. [Google Scholar] [CrossRef] [Green Version]
- Aldrink, J.H.; Adler, B.; Haines, J.; Watkins, D.; Matthews, M.; Lubeley, L.; Wang, W.; King, D.R. Patients exposed to diagnostic head and neck radiation for the management of shunted hydrocephalus have a significant risk of developing thyroid nodules. Pediatr. Surg. Int. 2016, 32, 565–569. [Google Scholar] [CrossRef]
- Cahoon, E.K.; Nadyrov, E.A.; Polyanskaya, O.N.; Yauseyenka, V.V.; Veyalkin, I.V.; Yeudachkova, T.I.; Maskvicheva, T.I.; Minenko, V.F.; Liu, W.; Drozdovitch, V.; et al. Risk of thyroidnodules in residents of belarus exposed to chernobyl fallout as children and adolescents. J. Clin. Endocrinol. Metab. 2017, 102, 2207–2217. [Google Scholar] [CrossRef]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid imaging, reporting and data system (TI-RADS): White paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography Diagnosis and Imaging-Based Management of Thyroid Nodules: Revised Korean Society of Thyroid Radiology Consensus Statement and Recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedüs, L.; Paschke, R.; Valcavi, R.; Vitti, P.; Balafouta, S.T.; et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules—2016 Update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Ferrarazzo, G.; Camponovo, C.; Deandrea, M.; Piccardo, A.; Scappaticcio, L.; Trimboli, P. Suboptimal accuracy of ultrasound and ultrasound-based risk stratification systems in detecting medullary thyroid carcinoma should not be overlooked. findings from a systematic review with meta-analysis. Clin. Endocrinol. 2022, 97, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Castellana, M.; Piccardo, A.; Romanelli, F.; Grani, G.; Giovanella, L.; Durante, C. The ultrasound risk stratification systems for thyroid nodule have been evaluated against papillary carcinoma. A meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.H.; Suh, C.H.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Diagnostic performance of four ultrasound risk stratification systems: A systematic review and meta-analysis. Thyroid 2020, 30, 1159–1168. [Google Scholar] [CrossRef]
- Castellana, M.; Castellana, C.; Treglia, G.; Giorgino, F.; Giovanella, L.; Russ, G.; Trimboli, P. Performance of five ultrasound risk stratification systems in selecting thyroid nodules for FNA. J. Clin. Endocrinol. Metab. 2020, 105, dgz170. [Google Scholar] [CrossRef]
- Trimboli, P.; Ferrarazzo, G.; Deandrea, M.; Camponovo, C.; Romanelli, F.; Piccardo, A.; Durante, C. Interest of researchers in ultrasound systems for risk stratification of thyroid nodules (TIRADS): A systematic review. Clin. Transl. Imaging 2022, 10, 185–190. [Google Scholar] [CrossRef]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.D.; Newbold, K.; Papotti, M.G.; Berruti, A. Thyroid Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [Green Version]
- Melo, R.; Menis, F.; Calsavara, V.F.; Stefanini, F.S.; Novaes, T.; Saieg, M. The Impact of the Use of the ACR-TIRADS as a Screening Tool for Thyroid Nodules in a Cancer Center. Diagn. Cytopathol. 2022, 50, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.J.; Na, D.G.; Baek, J.H.; Sung, J.Y.; Kim, J.H.; Kang, S.Y. US Fine-Needle Aspiration Biopsy for Thyroid Malignancy: Diagnostic Performance of Seven Society Guidelines Applied to 2000 Thyroid Nodules. Radiology 2018, 287, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Magri, F.; Chytiris, S.; Croce, L.; Molteni, M.; Bendotti, G.; Gruosso, G.; Ngnitejeu, S.T.; Agozzino, M.; Rotondi, M.; Chiovato, L. Performance of the ACR TI-RADS and EU TI-RADS Scoring Systems in the Diagnostic Work-up of Thyroid Nodules in a Real-Life Series Using Histology as Reference Standard. Eur. J. Endocrinol. 2020, 183, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Lamartina, L.; Ascoli, V.; Bosco, D.; Biffoni, M.; Giacomelli, L.; Maranghi, M.; Falcone, R.; Ramundo, V.; Cantisani, V.; et al. Reducing the Number of Unnecessary Thyroid Biopsies while Improving Diagnostic Accuracy: Toward the “Right” TIRADS. J. Clin. Endocrinol. Metab. 2019, 104, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.L.; Du, J.R.; Wang, H.; Jin, C.X.; Sui, G.Q.; Yang, D.Y.; Lin, Y.Q.; Luo, Q.; Fu, P.; Li, H.Q.; et al. Comparison and Preliminary Discussion of the Reasons for the Differences in Diagnostic Performance and Unnecessary FNA Biopsies between the ACR TIRADS and 2015 ATA Guidelines. Endocrine 2019, 65, 121–131. [Google Scholar] [CrossRef]
- Sajisevi, M.; Caulley, L.; Eskander, A.; Du, Y.; Auh, E.; Karabachev, A.; Callas, P.; Conradie, W.; Martin, L.; Pasternak, J.; et al. Evaluating the Rising Incidence of Thyroid Cancer and Thyroid Nodule Detection Modes: A Multinational, Multi-Institutional Analysis. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 811–818. [Google Scholar] [CrossRef]


{kind=link}
| Age | 58 (48–66) |
| Sex | Female 80.2%; Male 19.8% |
| Positive Thyroid Autoimmunity | 10.5% |
| Maximum diameter (mm) | 15 (10–21) |
| ACR TI-RADS | TR1 n.33 (2.9%) |
| TR2 n.232 (20.5%) | |
| TR3 n.403 (35.6%) | |
| TR4 n.409 (36.1%) | |
| TR5 n.55 (4.9%) | |
| Cytology | TIR1 n.147 (13%) |
| TIR1C n.46 (4.1%) | |
| TIR2 n.781 (69%) | |
| TIR3A n.42 (3.7%) | |
| TIR3B n.43 (3.8%) | |
| TIR4 n.30 (2.6%) | |
| TIR5 n.43 (3.8%) | |
| Histology | Benign n.14 (16%) |
| Malignant n.73 (84%) |
| RON (According to FNAC) | ROM (According to Histology) | |||
|---|---|---|---|---|
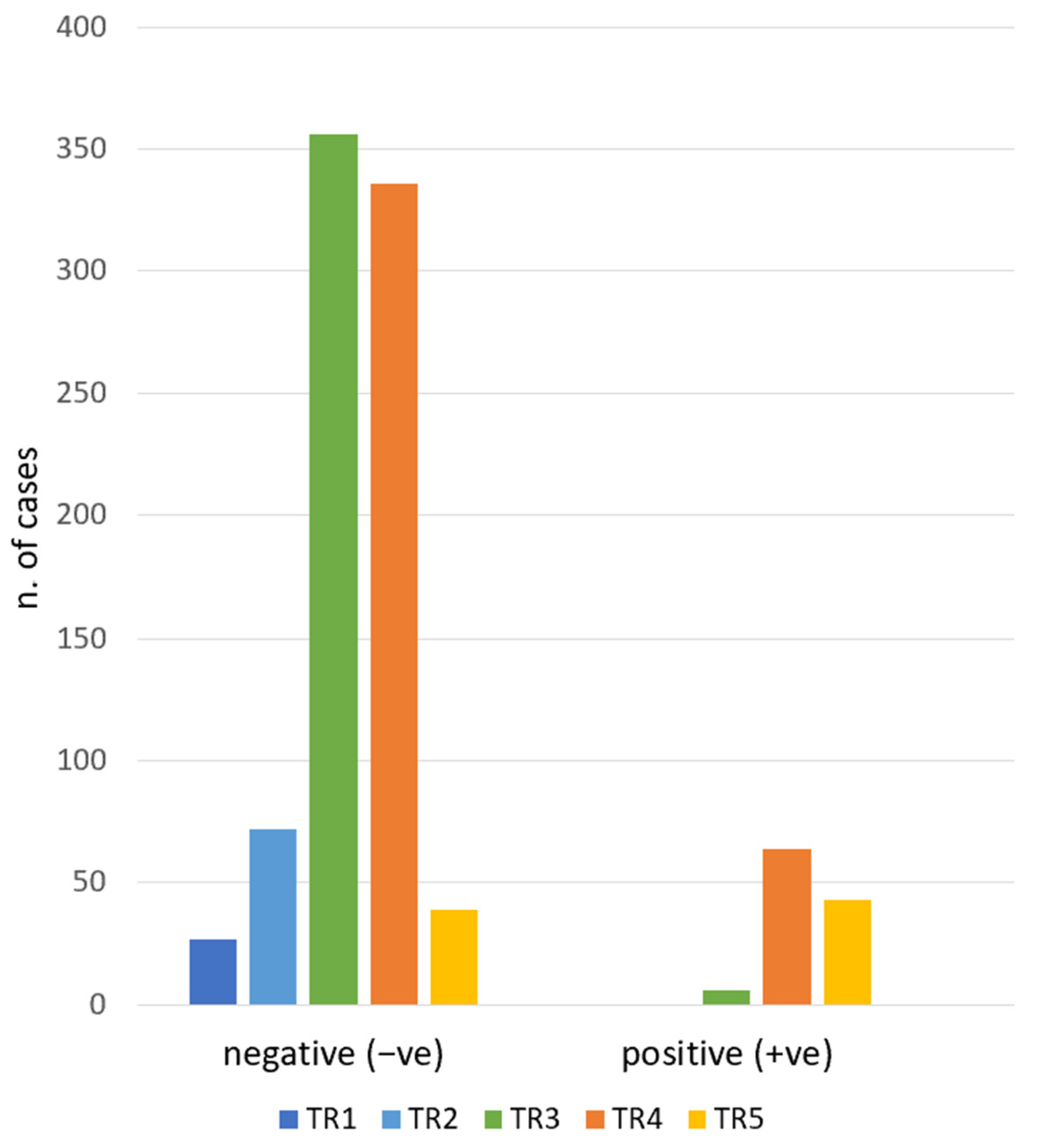
| TR1 | 0% | Negative n. 27 (100%) Positive n.0 (0%) | \ | \ |
| TR2 | 0% | Negative n.72 (100%) Positive n.0 (0%) | \ | \ |
| TR3 | 1.7% | Negative n.356 (98.3%) Positive n.6 (1.7%) | 50% | Benign n.1 (17%) Malignant n.1 (17%) Active surveillance n.2 (33%) Not available n.2 (33%) |
| TR4 | 16% | Negative n.336 (84%) Positive n.64 (16%) | 80% | Benign n.10 (15.6%) Malignant n.39 (60.9%) Active surveillance n.13 (20.3%) Not available n.2 (3.2%) |
| TR5 | 52% | Negative n.39 (48%) Positive n.43 (52%) | 92% | Benign n.3 (7%) Malignant n.33 (76.7%) Active surveillance n.6 (14%) Not available n.1 (2.3%) |
| “Not Indicated FNACs” | Cancers Founded | TNM | |
|---|---|---|---|
| TR1 (No FNAC) | n.27/27 (100% of total TR1) | \ | \ |
| TR2 (No FNAC) | n.72/72 (100% of total TR2) | \ | \ |
| TR3 (FNAC if >25 mm) | n.258/362 (71.3% of total TR3) | 1 | Papillary carcinoma n.1: T1b N0 |
| TR4 (FNAC if >15 mm) | n.243/400 (60.7% of total TR4) | 28 | Papillary carcinoma n.27: T1a N0 n.12 T1b N0 n.5 T1a (m) N0 n.4 T1b (m) N0 n.1 T1a N1a n.2 T1b N1a n.1 T1a N1b n.1 T1b N1b n.1 Uncertain malignant potential (UMP) n.1: T1a N0 |
| TR5 (FNAC if > 10 mm) | n.23/82 (28% of total TR5) | 13 | Papillary carcinoma n.12: T1a N0 n.6 T1b N0 n.1 T1a (m) N0 n.2 T1a N1a n.1 T1a (m) N1b n. 2 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) n.1: T1a N0 |
| “Not Indicated FNACs” | “Indicated FNACs” | |||
|---|---|---|---|---|
| RON | ROM | RON | ROM | |
| TR1 | 0% | \ | 0% | \ |
| TR2 | 0% | \ | 0% | \ |
| TR3 | 1.6% | 50% | 8% | No data available |
| TR4 | 16% | 90% | 15.3% | 61% |
| TR5 | 60% | 100% | 47% | 86.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amendola, S.; Wolde Sellasie, S.; Pedicini, F.; Carlini, M.; Russo, G.; Ossola, N.; Leoncini, A.; Botti, F.; Bonanno, E.; Trimboli, P.; et al. Evaluation of the Performance of ACR TI-RADS Also Considering Those Nodules with No Indication of FNAC: A Single-Center Experience. J. Clin. Med. 2023, 12, 398. https://doi.org/10.3390/jcm12020398
Amendola S, Wolde Sellasie S, Pedicini F, Carlini M, Russo G, Ossola N, Leoncini A, Botti F, Bonanno E, Trimboli P, et al. Evaluation of the Performance of ACR TI-RADS Also Considering Those Nodules with No Indication of FNAC: A Single-Center Experience. Journal of Clinical Medicine. 2023; 12(2):398. https://doi.org/10.3390/jcm12020398
Chicago/Turabian StyleAmendola, Stefano, Sium Wolde Sellasie, Francesco Pedicini, Massimo Carlini, Giulia Russo, Nicola Ossola, Andrea Leoncini, Flavia Botti, Elena Bonanno, Pierpaolo Trimboli, and et al. 2023. "Evaluation of the Performance of ACR TI-RADS Also Considering Those Nodules with No Indication of FNAC: A Single-Center Experience" Journal of Clinical Medicine 12, no. 2: 398. https://doi.org/10.3390/jcm12020398