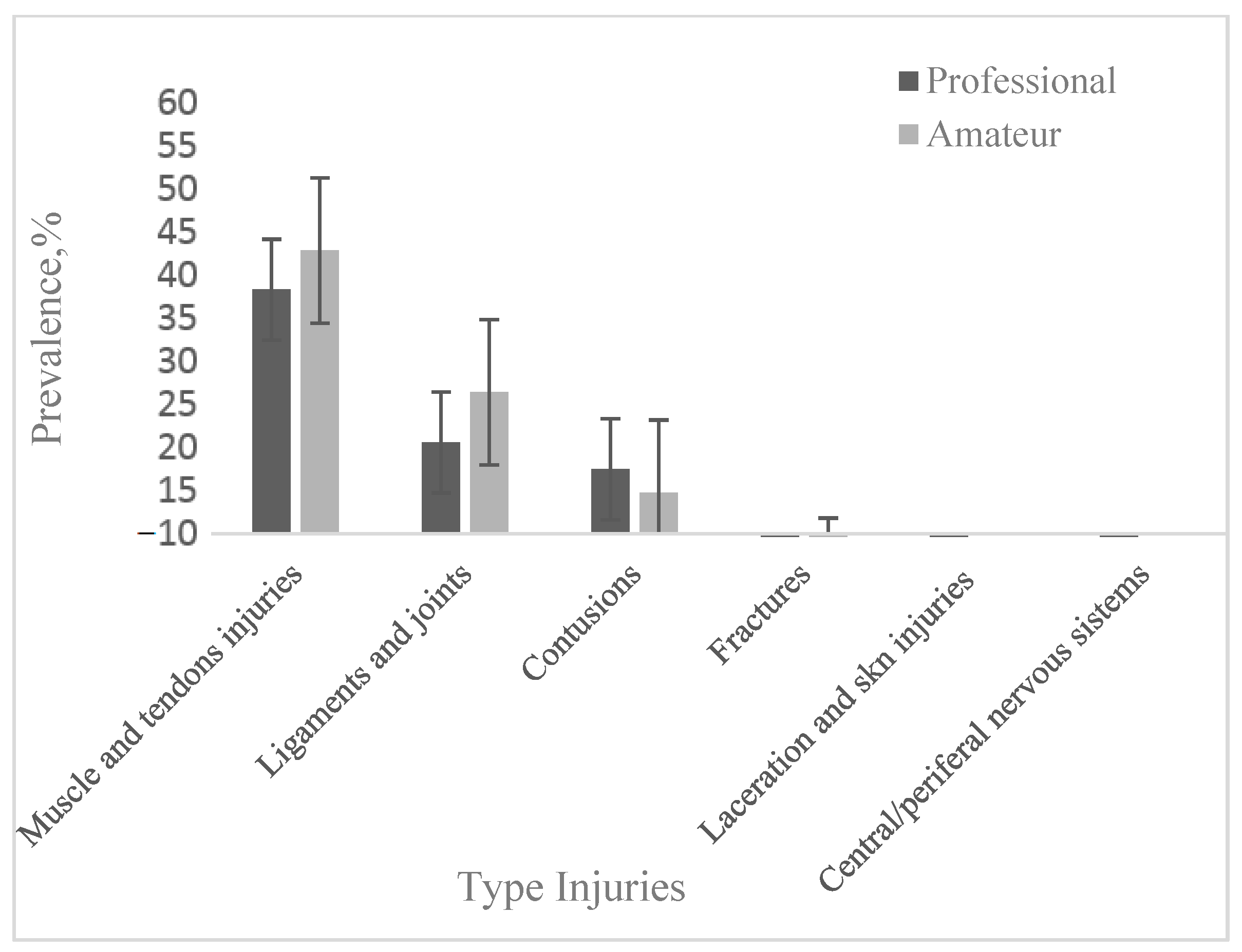
4.1. The Type of Injury
In our study, the most common types of injuries in professional football players were muscle and tendon injuries (prevalence 39.78 ± 11.8%), joint and ligament injuries (21.13 ± 4.14%) and contusions (17.86% ± 3.82). In amateur football players, the prevalence of muscle injuries was 44.56 ± 12.57% and that of joint and ligament injuries was27.62% ± 7.18; the prevalence of contusions was lower (15.0 ± 4.15%). Fractures were less frequent with a prevalence of 3.27 ± 0.89% in professional footballers and 3.05 ± 2.58% in amateurs. Lacerations and abrasions (2.42 ± 1.42%) and central/peripheral nervous system injuries (1.3 ± 1.16%) were reported only in professional football players (
Table 1 and
Table 2).
Our data on muscle injuries are consistent with the results of other studies stating that muscle injuries are the most common in football [
54,
55,
56,
57], representing more than 30% of injury types. Árnason et al. [
58] stated that muscle strains (29%), ligament sprains (22%) and contusions (20%) were the most common types of injury. The frequency of re-injury was significantly high, with 44% of strains and 58% of sprains recorded as re-injuries.
Palazon et al. [
20] found, for young male football players, that muscle/tendon injuries were the most frequent (IIR = 1.90/1000 h), followed by joint and ligament injuries (IIR = 0.97/1000 h) and contusions (IIR = 0.84/1000 h); bone fracture and stress, central/peripheral nervous system injuries, lacerations and skin injuries were the less common injury types. In young female football players, joint and ligament injuries (IIR = 2.36 injuries/1000 h) were the most common, followed by muscle/tendon injuries (IIR = 2.01 injuries/1000 h) and contusions (IIR = 0.93 injuries/1000 h). Bone stress fractures and injuries (IIR = 0.27 injuries/1000 h) were less common, and skin lacerations or central/peripheral nervous system injuries were not recorded. At the muscle and tendon level (two fibrous tissues that connect muscles to bones), the injuries consisted of strains/tears, which occur when the tissue is overstressed, mainly due to sudden acceleration or deceleration. Over 90% of muscle injuries affected the four major muscle groups of the lower extremity: hamstrings, adductors, quadriceps and gastrocnemius [
31]. Several studies have found that hamstring injuries predominate [
18,
19,
33,
47]. Roe et al. [
6] indicated for these injuries a prevalence of 21% and specified that the biceps femoris (84%) was more frequently injured than the semimembranosus (11%) and semitendinosus (5%) muscles. In elite players, Ekstrand et al. [
59] reported prevalences ranging from 12 to 16% of time-wasting injuries. Factors that increase the risk of hamstring muscle injury are: sports that involve extreme strain, running or sprinting; previous hamstring muscle injury; reduced flexibility; or muscle imbalance. Hamstring overuse injuries are common, especially in sports such as football, basketball and tennis, where running is combined with quick starts and stops. Hamstring injuries compromise individual performance and team success in many sports [
31,
59,
60,
61,
62,
63].
Quadriceps strains occur especially in sports that require repetitive kicking and sprinting efforts and are common in football in its various forms around the world [
64,
65,
66,
67]. Quadriceps muscle strains are prevalent in the Australian Football League (AFL), with each team reporting 1–2 new quadriceps strain injuries per season [
66]. There is a greater risk of hamstring injuries during the first season, while rectus femoris strains (29%) were more common than biceps femoris muscle injuries (11%) in the Premier League pre-season English and Australian Football League [
65]. In contrast, Ekstrand et al. [
13] found that quadriceps muscle strains were fairly constant throughout the season. Football players with quadriceps injuries miss more games than those with hamstring and groin injuries, and re-injury rates are high (17%).
Ankle sprains are the most common pathology in ankle injuries, accounting for 51–81% of all football-related ankle injuries [
14,
15,
16,
17,
68,
69]. Ankle sprains affect the lateral ligaments, the majority occurring during contact with players (59%), with the exception of goalkeepers, where 79% occur in non-contact situations [
70,
71]. Jain et al. [
72] indicated a 28.6% recurrence of anterior talofibular ligament injury.
The incidence of knee injuries during competition is 15–19% of all injuries. Of these, 35–37% are strains, 20–21% are sprains and 16–24% are contusions. Knee injuries represent 58% of all major injuries [
59,
73]. The most common knee injuries sustained in football include the anterior cruciate ligament (ACL; 14.2%), medial collateral ligament (MCL; 23%), tears [
74] and meniscal tears. The anterior cruciate ligament (ACL) of the knee is at risk of injury during sports involving cutting, jumping and pivoting movements, such as in American football and other sports [
75]. They appear in sports involving pivoting, such as football, basketball and handball in European teams, as well as gymnastics and alpine skiing. These can range from mild (small tears/sprain) to severe (when the ligament is completely torn). Both contact and non-contact injuries can occur [
76], with non-contact tears being more common when the limb is not in contact and combined with valgus and internal rotation trauma. There is evidence suggesting that the occurrence of ACL injuries is more prevalent among women compared to males, with incidence rates ranging from 2.4 to 9.7 times greater in female athletes engaged in equivalent sports [
77,
78,
79].
Acute ACL rupture is a common trauma, with an incidence of up to 84/100,000 people in the USA and 78/100,000 people in Sweden [
80]. According to the findings of Rothenberg et al. [
74], the yearly prevalence of the anterior cruciate ligament (ACL) damage among female football players ranges from 0.5% to 6.0%, whereas, among male football players, it ranges from 0.6% to 8.5%.
In professional sports, epidemiological studies of concussion have been reported in Australian Rules Football [
81,
82] and globally in football [
83,
84], Major League Baseball [
85], National Basketball Association [
86], National Hockey League [
87] and in rubies [
88]. Some studies that used publicly available data reported rates of 0.66 concussions/per game or 1.6 concussions/per game [
81,
89,
90,
91,
92,
93]. Variation in time frame and methodology led to the variation in reported incidences. Most head injuries in men’s professional football are caused by head-to-head and elbow-to-head contact [
94]. Within our study, only a few articles addressed the subtypes of football injuries [
18,
19,
47,
48,
95,
96].
4.2. Mechanism of Injury
In our systematic review, 25 studies (
Table 3) of professional football players and 5 studies of amateur football players (
Table 4) provided data comparing traumatic (acute) injuries with overuse injuries. The majority of football-related injuries had a traumatic mechanism, with a prevalence of 64.16 ± 15.34% in professionals and 76.88 ± 9.05% in amateurs that was 1.8 times higher and 3.36 times higher, respectively, compared to overuse injuries (35.60 ± 15.22%—professionals and 22.86 ± 8.74%—amateurs). In relation to the mechanism of injury, 15 professional and 5 amateur studies reported contact and non-contact injury data among professional and amateur male football players. In professional football players, a higher prevalence of contact injuries was recorded (50.70 ± 11.56 vs. 49.30 ± 11.56%), while in amateur football players, the prevalence was higher for non-contact injuries (55.04 ± 16.1 vs. 45.96 ± 16.1%). Several authors reported that more than two-thirds of football injuries are traumatic (67–80%), with the rest (33–20%) being caused by overuse [
4,
11,
97]. Moreover, about two-thirds of traumatic injuries are contact injuries, of which 12–28% are caused by foul play. Non-contact injuries accounted for 26–58% of all injuries [
14,
15,
97,
98], which are results that are close to the data presented by us. Sprouse et al. [
95] found a higher prevalence of contact injuries in senior football players than non-contact injuries (54% vs. 40%), indicating a higher match vs. training prevalence of contact injuries (63 vs. 40% in seniors and 70 vs. 40% in young people), as in the case of traumatic injuries. The situation is similar for women.
In elite players, contact injuries accounted for 33–42% of all acute injuries [
14,
15]. Only Luthje et al. [
73] found a higher proportion of contact injuries (79%). Studies of lower level players reported that 55–59% of acute injuries were contact injuries, while the comparable percentage for junior players was 42–53% [
14,
99,
100].
In young male football players, Palazon et al. [
20] state that the incidence rate for traumatic injuries (5.50 injuries/1000 h) was higher than for overuse injuries (1.10 injuries/1000 h), the incidence ratio being higher than what we found in male amateur footballers. Similar to men, in young female football players, the incidence rate for traumatic injuries (4.55 injuries/1000 h) was higher compared to that for overuse injuries (1.56 injuries/1000 h). Moreover, for young footballers of both sexes, the rates of incidence for non-contact injuries were superior to those with contact (3.48 and 2.39 injuries/1000 h vs. 2.77 and 1.92 injuries/1000 h).
In recent years, increased research has focused on overuse injuries among athletes involved in various competitive sports, finding a prevalence of 43–46.2% in volleyball [
101,
102,
103]; 26.2–29.3% rowing youths [
104,
105]; 82.6% in professional and amateur golf [
106]; 50% in basketball, 21.7% in field hockey; 25% in football [
107]. For basketball, Dick et al. [
108] reported the prevalence of contact injuries being 52.5% for matches and 43.6% for training, with values higher than non-contact injuries being 22.3% and 36.3%, respectively.
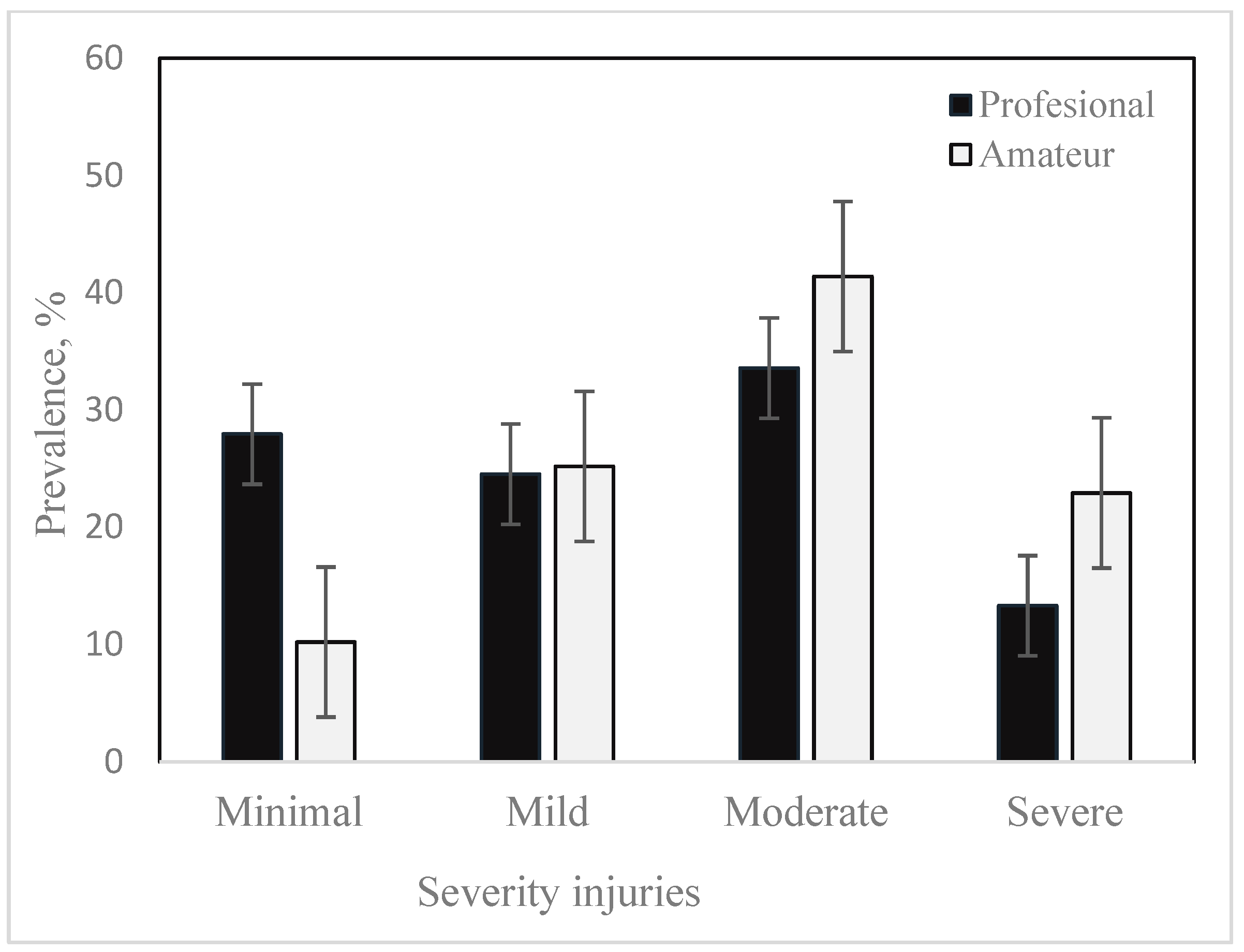
4.3. Severity of Injuries
Eligible studies that reported injury severity data in professional and amateur football players are listed in
Table 5 and
Table 6. The aggregate prevalences of minimal injuries were 27.94 ± 11,93% in professionals and 10.21 ± 7.77% in amateurs; mild—24.56 ± 6.71% vs. 25.19 ± 7.56%; moderate—33.57% ± 8.37 vs. 41.38 ± 7.56%; severe—13.32 ± 5.59% vs. 22.92 ± 9.0%. Sprouse et al. [
97] reported a prevalence of minor injuries in international football: 60% for senior players and 59% for youth football players, with 27% vs. 28% for moderate injuries and 12% vs. 9% for severe injuries, which also indicated 2% vs. 4% of major injuries. Those authors found no significant difference in the distribution of injuries between the match and practice, between seniors and youth for overall injury severity, injury severity during the match or injury severity at practice. The prevalences reported by [
21] for female football players with 18% minimal, 20% mild, 40% moderate and 21% severe injuries are closer to the values we reported for male amateur football players vs. professional ones. The same finding is in the case of the results published by [
109], who reported that in the first division of women’s football in Spain, 16% of injuries were minimal, 22% were mild, 40% were moderate and 23% were severe. In youth football players, most injuries were of minimal severity (1–3 days lost), but moderate injuries (incidence of 1.7 injuries/1000 h for men and 1.5 injuries/1000 h for women) and severe injuries (0.8 injuries/1000 h for men and 1.3 injuries/1000 h for women), indicated in the meta-analysis by [
20], may be a cause for concern.
The most serious injuries in football are bone injuries (tibia, fibula and metatarsal fractures), major ankle breaks or sprains, muscle injuries and those affecting ligaments or tendons. The rupture of the anterior cruciate ligament, tear of the medial lateral ligament and tear of the medial meniscus mark a football player’s career for life. Mild injuries with an absence of less than 7 days were mainly represented by traumatic injuries of the lower extremity, such as contusions or joint capsular and ligamentous injuries or painful overuse syndromes. The moderate ones were mainly structural muscle injuries in the thigh and pain syndromes related to the groin area, while the injuries with the longest absence were those affecting the knee [
110]. The results of our study showed that most injuries in male professional and amateur football players with a traumatic or non-contact mechanism are preventable. The implementation of neuromuscular training (NMT) programs can have positive effects on the incidence of injuries in adults [
111,
112,
113,
114]. A recent meta-analysis found that a football-specific NMT program reduced injury rates by 20–50% [
114]. Regarding ankle injuries, neuromuscular and proprioceptive intervention programs have been found to decrease injury risk by 35–50% in adult sports populations [
111,
112,
113]. Similar effects have been reported for young athletes. Two meta-analyses demonstrated a risk reduction for lower extremity injuries of approximately 25–35% [
113,
114].
4.4. New Versus Recurrent Lesions
The studies included in our review that reported the frequencies of recurrent injuries [
115,
116] are shown in
Table 3 for professional football players (21 studies) and in
Table 4 for amateur football players (6 studies). The cumulative frequency of re-injury for professional footballers was 15.26 ± 5.81%, 1.40% lower than that recorded for amateur footballers (16.66 ± 10.25%). The results we obtained are consistent with those reported by [
19], who indicated a recurrence of 16.6% for top-level football players; however, this was significantly different from the recurrence in elite (25%) and amateur football players (35.1%). The recurrence occurred in less than two months in all three categories of footballers. This may reflect a premature return to training/play and incomplete or inadequate rehabilitation. Those authors reported higher recurrent injury incidence rates in the match compared to training (3.22/3.72/4.36 vs. 0.58/1.52/1.54/1000 exposure hours for top level/elite/amateurs). The incidence of recurrent lesions was lower compared to the incidence of new lesions (1.3 vs. 7.0 lesions/1000 h of exposure) [
19]. For adult female football players, Lopez et al. [
117] indicated a lower incidence of recurrent lesions (1.8/1000 h) than the incidence of new lesions (4.6/1000 h of exposure). Rates for recurrent injuries in youth football players were lower than those for new injuries (0.8 injuries/1000 h for men and 1.4 injuries/1000 h for women) vs. 5.9 injuries/1000 h for men and 5.1 injuries/1000 h for women, respectively) [
20]. Van der Horst [
118], in an analysis of potential risk factors such as age, BMI body weight (BMI), injury history, “The FIFA11” intervention, playing position and surface, injured leg (dominant vs. non-dominant) and total exposure, found that these factors were not significantly associated with an increased risk of recurrent injury. The frequency of recurrent lesions described in this study of 12.9% is in accordance with previously published data on specific types of recurrent lesions. Recurrence incidence between 13.9 and 63.3% was reported for hamstring injuries, while the incidence of recurrent ankle injuries varied between 3 and 34% [
118,
119,
120]. Three specific sites of recurrent injury were identified, with the hamstring (26%), ankle (23%) and knee (14%) being the most common sites of recurrent injury. The recurrence of muscle injuries depended on the type of muscle and the category of footballers. Hägglund et al. [
48] indicated, for hamstrings, a prevalence of 22.7%, 15.7% and 12.5% for top-level, elite and amateur footballers, respectively. In the adductors, the most injuries were in elite footballers (14.2%), followed by top-level players (11.6%) and amateurs (15%). The quadriceps and calf muscles were affected to a lesser extent in top-level players and elites, with amateurs registering a prevalence of recurrent calf injuries of 12.5% [
48]. Wiggins et al. [
121] estimate that 1 in 4 young athletes (<20–25 years) who sustain an ACL injury and return to high-risk sports will go on to sustain another ACL injury at some point in their career. Recurrence proportions were higher in the second half of the competitive season for all cohorts [
48].
4.5. Game Level
In our review, several studies have shown differences between elites, sub-elites and amateur adult male players in terms of location, type and severity of injury, incidence of recurrent injury and days lost due to injury. Moreover, the variation of these indicators was noted depending on the country of origin of the football team (climate); type of competition—friendly matches or competitive matches (national, in world cups, European cups and Olympics); season; lawn type. In European male professional football, Waldén et al. [
122] reported that teams located in northern Europe, with countries that typically have milder summers and longer winters, had a prevalence of traumatic and overuse injuries that was different compared to teams from southern Europe with Mediterranean climates. Moreover, the incidence of anterior cruciate ligament (ACL) injuries, and, in particular, non-contact ACL injuries, was found to follow a reverse trend, with Mediterranean climate teams experiencing more ACL injuries. The injury severity profile indicates: minimal injuries—30.1 (36.20%); mild—27.1 (28.1%); moderate—32.8 (24.7%); severe—10 (11%). Twenty-two percent (18%) of lesions were early recurrences. Players injured in the first year had a higher risk of injury the following season compared to uninjured players (hazard ratio 2.7), those with a previous hamstring injury, groin injury or knee joint injury were two to three times more likely to suffer an identical injury the following season, while no such relationship was found for ankle sprains. Age was not associated with an increased risk of injury (Hägglund et al. [
48]. In sub-elite footballers in Australia, Whalan et al. [
123] reported a higher prevalence for muscle and ligament injuries (41% and 26%) and carried the highest injury burden (83 and 80 lost days/1000 h, respectively). The most common injuries were observed in the thigh (22%) and ankle (17%), with the prevalence of hamstring injuries (13%) being the highest. The risk of hamstring and calf muscle injury increases with age and more frequently towards the end of each half, suggesting that fatigue is a risk factor [
95]. The severity profile of the injury was: minimum—35%; mild—29%; moderate—28%; severe—8%. Recurrent injuries accounted for 20% of all injuries.
Between South American teams and European teams, Bengtsson et al. (2021) [
124] found significant differences in the incidence of ligament injuries in training (0.6 vs. 0.3/1000 h); differences in training culture between South America and Europe could influence injury epidemiology. Asian professional football is characterized by a high rate of ACL tears and hamstring injuries (54.4%) [
125], with recurrent lesions having a prevalence of 9.9% [
126].
Professional players had a lower incidence of moderate and severe injuries than amateur players, but a higher incidence of minimal injuries. These differences can be explained by the smaller number of players in amateur teams, with fewer options to replace injured or injury-prone players. Thus, amateur players had a higher match exposure per player than professionals by 17% [
127]. In the case of minor injuries in the amateur cohort, there is the possibility of their underreporting, due to the reduced contact between medical staff and players (2–3 times a week, during training and matches), which contrasts with the daily contact between medical staff and players in professional football. As a result, some minor amateur injuries may not be recorded due to players recovering from minor injuries in the meantime. Moreover, medical support is less consistent given the economic constraints of amateur teams, leading to delayed diagnoses and suboptimal rehabilitation, incomplete wound healing and/or neglect of minor injuries [
19,
128].
Each sport has a unique injury profile and risk of injury. Modern football involves continuous and intensive cycles of training and games, which predisposes players to higher injury risks and the most common overuse injuries. Football has been the focus of a number of randomized injury prevention trials with the aim of maintaining health, reducing costs and improving player performance [
129,
130,
131,
132,
133,
134]. The studies focused, in particular, on the prevention of knee sprains [
135,
136], anterior cruciate ligament injuries [
137], hamstring muscle strains in elite football players [
138,
139] and thigh pain [
140].
The programs included strength, balance and mobility training, proprioceptive training for semi-professional and amateur football players, physical exercise, educational intervention programs and supervision of players and coaches.
Cardoso-Marinho et al. [
141] consider football players’ perceptions of injury risk and prevention, as well as their recognition of injury risk factors (low muscle strength, lack of fitness, fatigue, overtraining and type/condition of surfaces; injury prevention factors such as warm-up, workload monitoring and strength and conditioning training) to be important.
Strategies to prevent moderate and severe injuries are important issues for professional and amateur football players and require further study in the future.
Comparing injury epidemiology in professional and amateur soccer provides valuable information on the relationship between injury characteristics and player abilities. The recorded differences regarding the type of injuries (
Table 1 and
Table 2); injury mechanisms (
Table 3 and
Table 4); and injury severity (
Table 5 and
Table 6) between professional and amateur soccer players can be explained by a different level of play, team size that can influence injury, injury risk and characteristics, limited number of training sessions per week for amateur soccer players, availability of medical support, differences between studies in terms of research populations and methodology used [
7,
42]. Training quality standards, development of muscle strength, endurance/coordination and different technical and tactical skills can be reasons for the differences found between the two categories of soccer players. Professional soccer players usually have better physical skills compared to amateur players, probably because of the higher physical demands in a professional soccer match [
142]. Cometti et al. [
143] note differences regarding knee flexor muscle strength and sprint speed over short distances. Moreover, inadequate recovery is an important causal factor in re-injury [
144]. Hagglund et al. [
48] found an inverse relationship between the level of play and recurrent injury. Players at top-level clubs showed a lower recurrence rate than those playing at lower level clubs. It is speculated that players at top-level clubs benefit from high-quality rehabilitation and support in return for play and competition, under the ongoing control of medical and physiotherapy teams providing sufficient rehabilitation time, which would contribute to lower rates of recurrence in professional players [
48]. Not all amateur soccer players have standard injury prevention and medical and physical therapy support. Differences in injury assessment and variations in the qualitative assessment of injury severity may influence the final classification of injuries.
Regarding the quality of study reporting, the mean STROBE quality scale score was 8.55 ± 0.5 (minimum = 5; maximum = 11), and for the NOS scale, the mean score was 7.25 ± 0.69 (minimum = 5; maximum = 8). No studies were excluded based on the STROBE quality scale and risk of bias [
25].
4.6. Limitation
The strength of this study is that it provides a general estimate of the type, severity, recurrence and mechanisms of injuries in amateur football compared to professional football. It highlights the poor attention paid to the millions of amateur footballers in terms of analyzing the prevalence and severity of injuries, as well as measures to prevent injuries in this category of footballers.
Several limitations were present in the current review. More eligible studies may not have been identified; this was motivated by the fact that the selection of studies was limited to articles published in English. Although the methodological quality assessments were performed by two independent reviewers, the assessment of study quality remains, however, subjective. The different definitions of the type and severity of injuries and their different expression [prevalence (%) or incidence (injuries/1000 h)] explain the inclusion in the systematic review of a small sample of eligible studies (especially in amateur football players) and reflect the inconsistent methodological approach between studies. We only documented data related to the main types of injuries, and did not address injuries stratified by subcategories (muscle type, joints and ligaments, and concussions). Although time loss is widely used to describe injury severity in epidemiology, the lack of data on the number of days lost to injury in most of the included studies made it impossible to report injury burden. We also did not highlight the prevalence of overuse complaints that do not cause time loss but may affect the athlete’s ability to perform on the football field. The analysis of the type and severity of injuries was not differentiated by the game, training and match phases or by the types of matches (league, national and international competitions). Future research should continue to record sports injury epidemiologic data using standardized methods and measurements to understand the injury profile and establish appropriate injury prevention programs.


 ,
, 





{kind=link}
{kind=link}