
Diagnostic Value of an Additional Sequence (Large-Field Coronal Stir) in a Routine Lumbar Spine MR Imaging Protocol to Investigate Lumbar Radiculopathy
 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
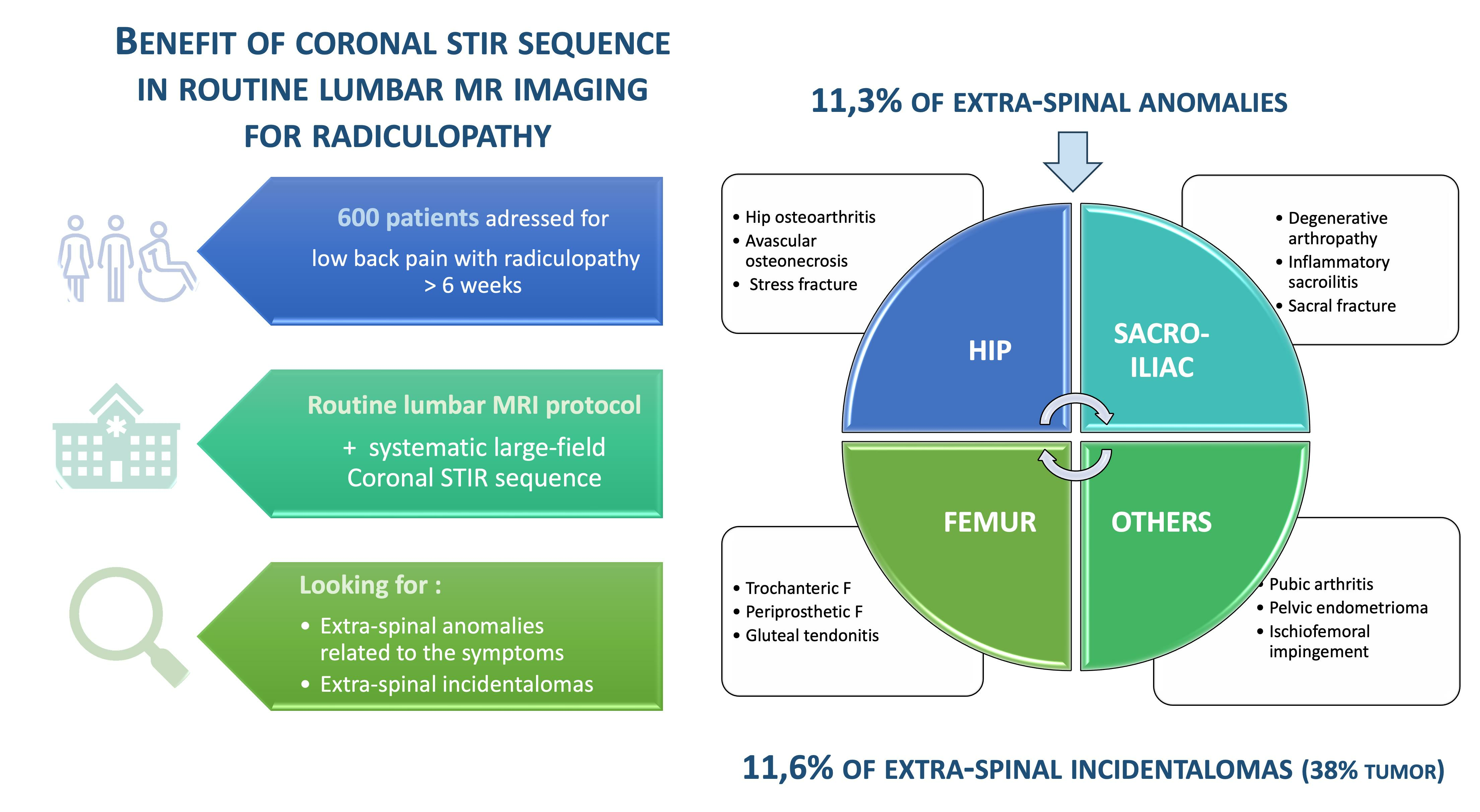
2.1. Study Population
2.2. MRI Protocol
2.3. Data Processing
- –
- The first reading involved the usual sequences centered on the lumbar spine, indicating whether or not there was an intervertebral disc hernia and/or spinal osteoarthritis that could explain the clinical lumbar radiculopathy.
- –
- The second reading involved only the coronal STIR sequence, indicating whether or not there was an ESA that could explain the clinical complaint and whether there was any clinically significant ESI unrelated to the reported symptoms.
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstantinou, K.; Hider, S.L.; Jordan, J.L.; Lewis, M.; Dunn, K.M.; Hay, E.M. The impact of low back-related leg pain on outcomes as compared with low back pain alone: A systematic review of the literature. Clin. J. Pain 2013, 29, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Harrisson, S.A.; Stynes, S.; Dunn, K.M.; Foster, N.E.; Konstantinou, K. Neuropathic Pain in Low Back-Related Leg Pain Patients: What Is the Evidence of Prevalence, Characteristics, and Prognosis in Primary Care? A Systematic Review of the Literature. J. Pain 2017, 18, 1295–1312. [Google Scholar] [CrossRef] [PubMed]
- Frymoyer, J.W. Lumbar disk disease: Epidemiology. Instr. Course Lect. 1992, 41, 217–223. [Google Scholar] [PubMed]
- Karine, P. High Authority for Health. March 2019. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2019-04/reco315_rapport_lombalgie_2019_04_02.pdf (accessed on 11 September 2023).
- Wassenaar, M.; van Rijn, R.M.; van Tulder, M.W.; Verhagen, A.P.; van der Windt, D.A.W.M.; Koes, B.W.; de Boer, M.R.; Ginai, A.Z.; Ostelo, R.W.J.G. Magnetic resonance imaging for diagnosing lumbar spinal pathology in adult patients with low back pain or sciatica: A diagnostic systematic review. Eur. Spine J. 2012, 21, 220–227. [Google Scholar] [CrossRef]
- Fukuda, K.; Kawakami, G. Proper use of MR imaging for evaluation of low back pain (radiologist’ view). Semin. Musculoskelet. Radiol. 2001, 5, 133–136. [Google Scholar] [CrossRef]
- Ailianou, A.; Fitsiori, A.; Syrogiannopoulou, A.; Toso, S.; Viallon, M.; Merlini, L.; Beaulieu, J.Y.; Vargas, M.I. Review of the principal extra spinal pathologies causing sciatica and new MRI approaches. Br. J. Radiol. 2012, 85, 672–681. [Google Scholar] [CrossRef]
- Ergun, T.; Lakadamyali, H. CT and MRI in the evaluation of extraspinal sciatica. Br. J. Radiol. 2010, 83, 791–803. [Google Scholar] [CrossRef]
- Völker, A.; Steinke, H.; Heyde, C.E. The Sacroiliac Joint as a Cause of Pain—Review of the Sacroiliac Joint Morphology and Models for Pain Genesis. Z. Orthop. Unfallchir. 2022, 160, 507–516. [Google Scholar] [CrossRef]
- Graul, I.; Vogt, S.; Strube, P.; Hölzl, A. Significance of Lumbar MRI in Diagnosis of Sacral Insufficiency Fracture. Glob. Spine J. 2021, 11, 1197–1201. [Google Scholar] [CrossRef]
- Grimaldi, A.; Mellor, R.; Hodges, P.; Bennell, K.; Wajswelner, H.; Vicenzino, B. Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Sports Med. 2015, 45, 1107–1119. [Google Scholar] [CrossRef]
- Morvan, G.; Vuillemin-Bodaghi, V.; Wybier, M.; Mathieu, P.; Busson, J.; Haddad, A. The “de Sèze” magnetic imaging. J. Radiol. 2007, 88 Pt 1, 943–946. [Google Scholar] [CrossRef] [PubMed]
- Vassalou, E.E.; Spanakis, K.; Tsifountoudis, I.P.; Karantanas, A.H. MR Imaging of the Hip: An Update on Bone Marrow Edema. Semin. Musculoskelet. Radiol. 2019, 23, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Khoury, N.J.; Birjawi, G.A.; Chaaya, M.; Hourani, M.H. Use of limited MR protocol (coronal STIR) in the evaluation of patients with hip pain. Skelet. Radiol. 2003, 32, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Laporte, C.; Albert, J.D.; Duvauferrier, R.; Bertaud, V.; Gouillou, M.; Guillin, R. MRI Investigation of Radiating Pain in the Lower Limbs: Value of an Additional Sequence Dedicated to the Lumbosacral Plexus and Pelvic Girdle. Am. J. Roentgenol. 2014, 203, 1280–1285. [Google Scholar] [CrossRef]
- Gleeson, T.G.; O’Connell, M.J.; Duke, D.; Ryan, M.; Ennis, R.; Eustace, S.J. Coronal oblique turbo STIR imaging of the sacrum and sacroiliac joints at routine MR imaging of the lumbar spine. Emerg. Radiol. 2005, 12, 38–43. [Google Scholar] [CrossRef]
- Mittal, P.; Mittal, A.; Mittal, K.; Gupta, R.; Gupta, S.; Kaur, R. Additional merit of coronal STIR imaging for MR imaging of lumbar spine. J. Craniovertebr. Junction Spine 2015, 6, 12. [Google Scholar] [CrossRef]
- Romeo, V.; Cavaliere, C.; Sorrentino, C.; Ponsiglione, A.; Ugga, L.; Barbuto, L.; Verde, F.; Covello, M. Clinical impact of coronal-STIR sequence in a routine lumbar spine MR imaging protocol to investigate low back pain. Medicine 2018, 97, e10789. [Google Scholar] [CrossRef]
- Semaan, H.B.; Bieszczad, J.E.; Obri, T.; Aldinger, P.K.; Bazerbashi, M.F.; Al-Natour, M.S.; Elgafy, H. Incidental Extraspinal Findings at Lumbar Spine Magnetic Resonance Imaging: A Retrospective Study. Spines 2015, 40, 1436–1443. [Google Scholar] [CrossRef]
- Khasawneh, R.A.; Mohaidat, Z.; Khasawneh, F.A.; Farah, A.; Gharaibeh, M.; El-Heis, M. Extraspinal findings prevalence and clinical significance in 4250 lumbar spine MRI exams. Sci. Rep. 2021, 11, 1190. [Google Scholar] [CrossRef]
- Blankenbaker, D.G.; Ullrick, S.R.; Davis, K.W.; De Smet, A.A.; Haaland, B.; Fine, J.P. Correlation of MRI findings with clinical findings of trochanteric pain syndrome. Skelet. Radiol. 2008, 37, 903–909. [Google Scholar] [CrossRef]
- Dupont, F.; Ltaief Boudrigua, A.; Pacaud, S. Contribution of tractography in the imaging of peripheral nerves. J. Imag. Diagn. Interv. 2023, 6, 148–154. [Google Scholar]
- Jeon, T.; Fung, M.M.; Koch, K.M.; Tan, E.T.; Sneag, D.B. Peripheral nerve diffusion tensor imaging: Overview, pitfalls, and future directions. J. Magn. Reson. Imaging 2018, 47, 1171–1189. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Mönch, S.; Riederer, I.; Zimmer, C.; Baum, T.; Kirschke, J.S. Imaging of the degenerative spine using a sagittal T2-weighted DIXON turbo spin-echo sequence. Eur. J. Radiol. 2020, 131, 109204. [Google Scholar] [CrossRef] [PubMed]
- Zanchi, F.; Richard, R.; Hussami, M.; Monier, A.; Knebel, J.F.; Omoumi, P. MRI of non-specific low back pain and/or lumbar radiculopathy: Do we need T1 when using a sagittal T2-weighted Dixon sequence? Eur. Radiol. 2020, 30, 2583–2593. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MRI Sequences | TE (ms) | RT (ms) | FOV (cm) | Gap (mm) | Thickness (mm) | Matrix | Acquisition Time (min) |
|---|---|---|---|---|---|---|---|
| 3D T2 | 137 | 1000 | 34 | 0.5 | 1 | 340 × 340 | 03:36 |
| Sag T1 | 8 | 453 | 35 | 0.5 | 3.5 | 416 × 320 | 00:55 |
| SagT2 DIXON | 85 | 3014 | 25 | 0.4 | 3.5 | 288 × 232 | 02:47 |
| Sag STIR | 104 | 2994 | 35 | 0.5 | 3.5 | 340 × 320 | 02:33 |
| Coro STIR | 130 | 6987 | 40 | 1 | 6.5 | 292 × 292 | 01:45 |
| Ax T2 | 108 | 2531 | 18 | 1 | 4 | 288 × 256 | 02:12 |
| Total (n = 600) | CoroSTIR – (n = 532) | CoroSTIR + (n = 68) | p-Value | |
|---|---|---|---|---|
| Patients | ||||
| Gender (%M/F) | 42/57 | 43/57 | 40/60 | 0.69 |
| Age | 54.1 [IQR 43-66] | 53.5 [IQR 42-65] | 58.8 [IQR 46-66] | 0.01 |
| Weight | 76.9 [IQR 67-85] | 76.8 [IQR 67.5-85] | 77.7 [IQR 66-86.5] | 0.57 |
| ATCD lumbar surgery (%) | 11.2 | 11.7 | 7.4 | 0.41 |
| Clinical | ||||
| Lateralization | D: 219 (36.5%) | D: 194 (36.5%) | D: 25 (36.8%) | 0.81 |
| G: 254 (42.3%) | G: 227 (42.7%) | G: 27 (39.7%) | ||
| B: 127 (21.2%) | B: 111 (20.9%) | B: 16 (23.5%) | ||
| Root topography | ||||
| Cruralgia | 93 (15.5%) | 77 (14.5%) | 16 (23.5%) | 0.07 |
| Sciatica | 213 (35.5%) | 193 (36.3%) | 20 (29.4%) | 0.28 |
| Buttock pain or truncated sciatica | 248 (41.3%) | 221 (41.5%) | 27 (39.7%) | 0.79 |
| Radiating pain without precision | 3 (0.5%) | 2 (0.4%) | 1 (1.5%) | 0.30 |
| Not known | 49 (8.2%) | 44 (8.3%) | 5 (7.4%) | 1 |
| Imaging | ||||
| Lumbar MRI cause to symptoms | 416 (69.3%) | 380 (71.4%) | 36 (52.9%) | 0.003 |
| Hip Joint | Congestive hip osteoarthritis | 17 |
| Stress femoral fracture | 4 | |
| Avascular femoral osteonecrosis | 1 | |
| Extensive acetabular edema | 1 | |
| Gluteal Muscles | Gluteal tendinobursitis | 21 |
| Sacroiliac Joint | Congestive degenerative arthropathy | 10 |
| Inflammatory sacroiliitis | 4 | |
| Sacral fracture | 1 | |
| Pubis | Septic arthritis of the pubis | 1 |
| Femur | Periprosthetic loosening fracture (total hip replacement) | 1 |
| Greater trochanter fracture | 1 | |
| Mixed Musculoskeletal Causes | Inflammatory sacroiliitis and gluteal tendinobursitis | 1 |
| Degenerative congestive sacroiliac arthropathy and gluteal tendinobursitis | 1 | |
| Others | Endometrioma with posterior deep pelvic endometriosis | 1 |
| Ischio-femoral impingement | 1 | |
| Retroperitoneal mass syndrome with urinary obstruction | 1 |
| Kidney | Atypical renal lesion 1 | 9 |
| Multicystic dysplasia, Polycystic kidney disease | 5 | |
| Liver | Non-cystic liver lesion 1 | 2 |
| Pelvis | Cystic or non-cystic ovarian lesion 1 | 15 |
| Prostatomegaly with struggle bladder | 11 | |
| Polymyomatous uterus | 4 | |
| Atypical uterine myoma 1 | 2 | |
| Indeterminate pelvic mass 1 | 1 | |
| Diffuse uterine adenomyosis | 1 | |
| Musculotendinous | Gluteal tendinobursitis 2 | 10 |
| Denervation edema on chronic root conflict 2 | 1 | |
| Intramuscular lesion (gluteus maximus) 1 | 1 | |
| Proximal iliotibial band enthesopathy 2 | 1 | |
| Osteoarticular | Congestive hip osteoarthritis 2 | 8 |
| Congestive degenerative sacroiliac arthropathy 2 | 8 | |
| Atypical bone lesion (iliac wing, femoral neck, sacrum) 1 | 3 | |
| Severe hip dysplasia 2 | 1 | |
| Congestive pubic osteoarthritis 2 | 1 | |
| Avascular femoral osteonecrosis 2 | 1 | |
| Others | Splenomegaly | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patriat, Q.; Prigent, F.-V.; Aho, S.; Lenfant, M.; Ramon, A.; Loffroy, R.; Lambert, A.; Ornetti, P. Diagnostic Value of an Additional Sequence (Large-Field Coronal Stir) in a Routine Lumbar Spine MR Imaging Protocol to Investigate Lumbar Radiculopathy. J. Clin. Med. 2023, 12, 6250. https://doi.org/10.3390/jcm12196250
Patriat Q, Prigent F-V, Aho S, Lenfant M, Ramon A, Loffroy R, Lambert A, Ornetti P. Diagnostic Value of an Additional Sequence (Large-Field Coronal Stir) in a Routine Lumbar Spine MR Imaging Protocol to Investigate Lumbar Radiculopathy. Journal of Clinical Medicine. 2023; 12(19):6250. https://doi.org/10.3390/jcm12196250
Chicago/Turabian StylePatriat, Quentin, François-Victor Prigent, Serge Aho, Marc Lenfant, André Ramon, Romaric Loffroy, Aurelien Lambert, and Paul Ornetti. 2023. "Diagnostic Value of an Additional Sequence (Large-Field Coronal Stir) in a Routine Lumbar Spine MR Imaging Protocol to Investigate Lumbar Radiculopathy" Journal of Clinical Medicine 12, no. 19: 6250. https://doi.org/10.3390/jcm12196250