

Heart Failure Remote Monitoring: A Review and Implementation How-To

Abstract
:1. Introduction
2. Remote Monitoring Devices
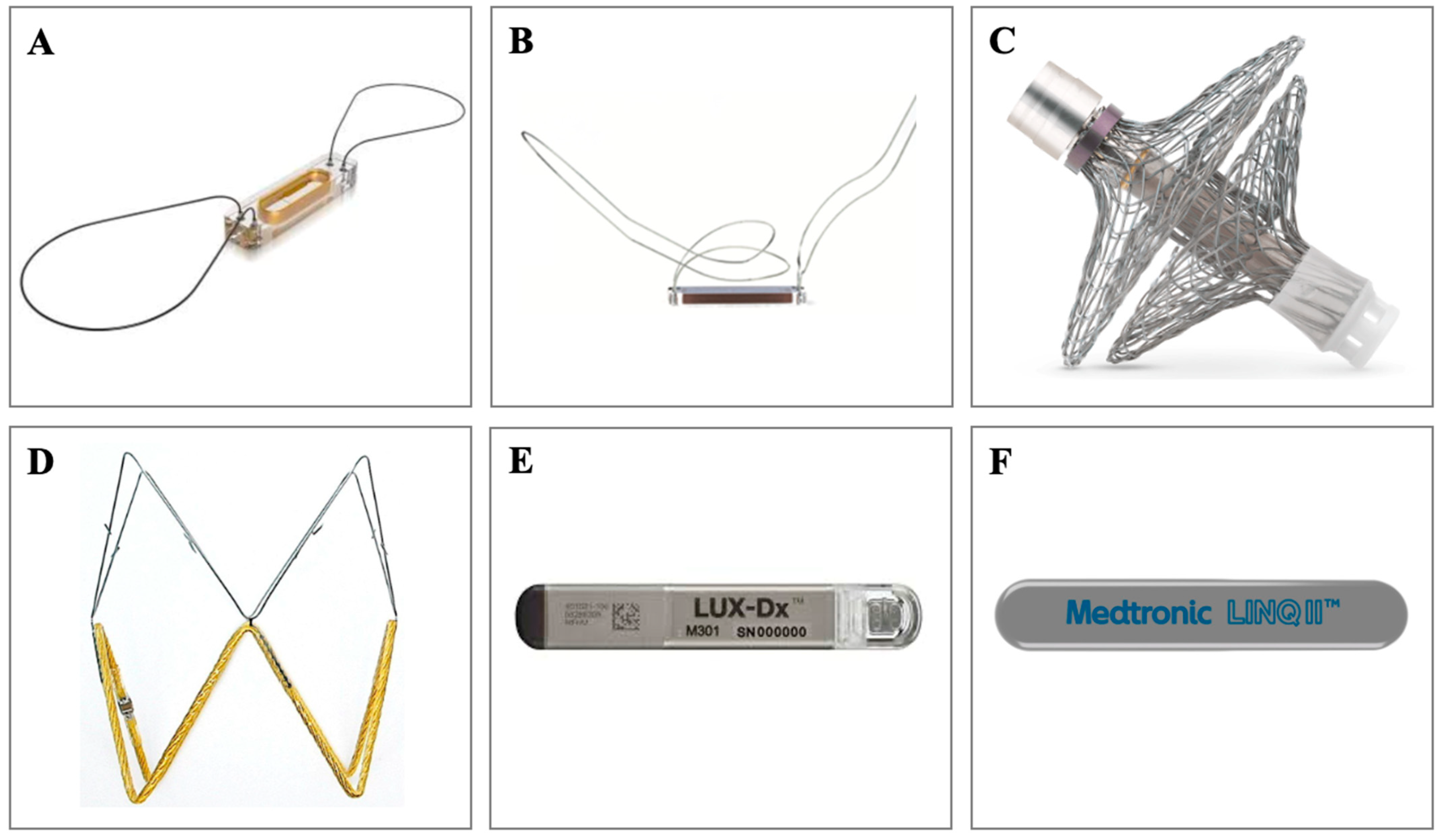
2.1. Implantable Pulmonary Artery Pressure (PAP) Monitoring Devices
2.2. Implantable Left Atrial Pressure (LAP) Monitoring Devices
2.3. Implantable Inferior Vena Cava (IVC) Monitoring Device
2.4. Insertable Cardiac Monitors (ICMs)
2.5. Cardiovascular Implantable Electronic Device (CIED) Monitoring
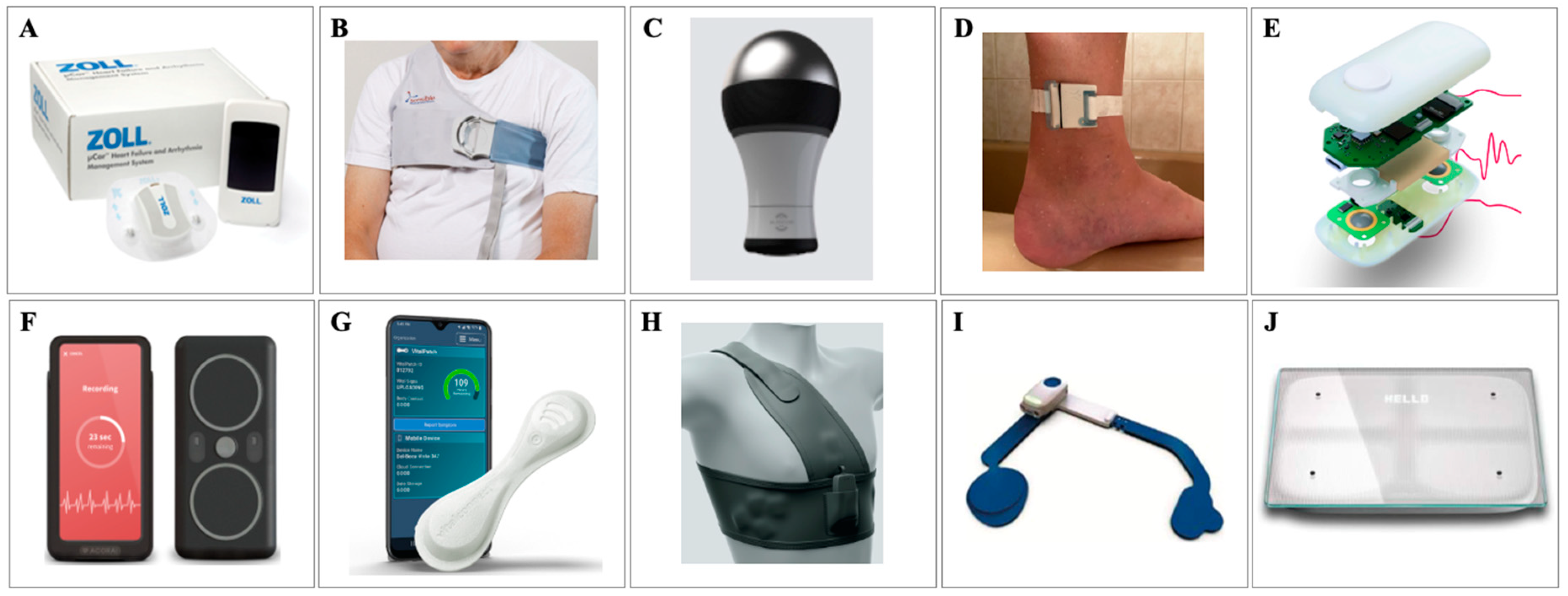
2.6. Wearable Devices
2.7. Real-World Implementation of an Effective RM Algorithm: A Clinical How-To
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Konstam, M.A.; Maddox, T.M.; Nichol, G.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef]
- Agarwal, M.A.; Fonarow, G.C.; Ziaeian, B. National Trends in Heart Failure Hospitalizations and Readmissions From 2010 to 2017. JAMA Cardiol. 2021, 6, 952–956. [Google Scholar] [CrossRef]
- Inglis, S.C.; Clark, R.A.; Dierckx, R.; Prieto-Merino, D.; Cleland, J.G. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst. Rev. 2015, 2015, CD007228. [Google Scholar] [CrossRef]
- Freund, O.; Caspi, I.; Alcalay, I.; Brezis, M.R.; Frydman, S.; Bornstein, G. An old diagnostic tool for new indications: Inpatient Holter ECG for conditions other than syncope or stroke. Sci. Rep. 2023, 13, 12510. [Google Scholar] [CrossRef]
- Schrier, R.W.; Abraham, W.T. Hormones and hemodynamics in heart failure. N. Engl. J. Med. 1999, 341, 577–585. [Google Scholar] [CrossRef]
- Adamson, P.B.; Abraham, W.T.; Aaron, M.; Aranda, J.M.; Bourge, R.C.; Smith, A.; Stevenson, L.W.; Bauman, J.G.; Yadav, J.S. CHAMPION trial rationale and design: The long-term safety and clinical efficacy of a wireless pulmonary artery pressure monitoring system. J. Card. Fail. 2011, 17, 3–10. [Google Scholar] [CrossRef]
- Givertz, M.M.; Stevenson, L.W.; Costanzo, M.R.; Bourge, R.C.; Bauman, J.G.; Ginn, G.; Abraham, W.T. Pulmonary Artery Pressure-Guided Management of Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2017, 70, 1875–1886. [Google Scholar] [CrossRef] [PubMed]
- Shavelle, D.M.; Desai, A.S.; Abraham, W.T.; Bourge, R.C.; Raval, N.; Rathman, L.D.; Heywood, J.T.; Jermyn, R.A.; Pelzel, J.; Jonsson, O.T.; et al. Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmonary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes from the CardioMEMS Post-Approval Study. Circ. Heart Fail. 2020, 13, e006863. [Google Scholar] [CrossRef] [PubMed]
- Zile, M.R.; Mehra, M.R.; Ducharme, A.; Sears, S.F.; Desai, A.S.; Maisel, A.; Paul, S.; Smart, F.; Grafton, G.; Kumar, S.; et al. Hemodynamically-Guided Management of Heart Failure Across the Ejection Fraction Spectrum: The GUIDE-HF Trial. JACC Heart Fail. 2022, 10, 931–944. [Google Scholar] [CrossRef] [PubMed]
- Lindenfeld, J.; Abraham, W.T.; Maisel, A.; Zile, M.; Smart, F.; Costanzo, M.R.; Mehra, M.R.; Ducharme, A.; Sears, S.F.; Desai, A.S.; et al. Hemodynamic-GUIDEd management of Heart Failure (GUIDE-HF). Am. Heart J. 2019, 214, 18–27. [Google Scholar] [CrossRef]
- Angermann, C.E.; Assmus, B.; Anker, S.D.; Asselbergs, F.W.; Brachmann, J.; Brett, M.; Brugts, J.J.; Ertl, G.; Ginn, G.; Hilker, L.; et al. Pulmonary artery pressure-guided therapy in ambulatory patients with symptomatic heart failure: The CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur. J. Heart Fail. 2020, 22, 1891–1901. [Google Scholar] [CrossRef]
- Brugts, J.J.; Radhoe, S.P.; Clephas, P.R.D.; Aydin, D.; van Gent, M.W.F.; Szymanski, M.K.; Rienstra, M.; Heuvel, M.H.v.D.; da Fonseca, C.A.; Linssen, G.C.M.; et al. Remote haemodynamic monitoring of pulmonary artery pressures in patients with chronic heart failure (MONITOR-HF): A randomised clinical trial. Lancet 2023, 401, 2113–2123. [Google Scholar] [CrossRef]
- Sharif, F.; Rosenkranz, S.; Bartunek, J.; Kempf, T.; Assmus, B.; Mahon, N.G.; Mullens, W. Safety and efficacy of a wireless pulmonary artery pressure sensor: Primary endpoint results of the SIRONA 2 clinical trial. ESC Heart Fail. 2022, 9, 2862–2872. [Google Scholar] [CrossRef]
- Mullens, W.; Sharif, F.; Dupont, M.; Rothman, A.M.; Wijns, W. Digital health care solution for proactive heart failure management with the Cordella Heart Failure System: Results of the SIRONA first-in-human study. Eur. J. Heart Fail. 2020, 22, 1912–1919. [Google Scholar] [CrossRef]
- Guichard, J.L.; Cowger, J.A.; Chaparro, S.V.; Kiernan, M.S.; Mullens, W.; Mahr, C.; Mullin, C.; Forouzan, O.; Hiivala, N.J.; Sauerland, A.; et al. Rationale and Design of the Proactive-HF Trial for Managing Patients with NYHA Class III Heart Failure by Using the Combined Cordella Pulmonary Artery Sensor and the Cordella Heart Failure System. J. Card. Fail. 2023, 29, 171–180. [Google Scholar] [CrossRef]
- D’Amario, D.; Meerkin, D.; Restivo, A.; Ince, H.; Sievert, H.; Wiese, A.; Schaefer, U.; Trani, C.; Bayes-Genis, A.; Leyva, F.; et al. Safety, usability, and performance of a wireless left atrial pressure monitoring system in patients with heart failure: The VECTOR-HF trial. Eur. J. Heart Fail. 2023, 25, 902–911. [Google Scholar] [CrossRef]
- Perl, L.; Meerkin, D.; D’Amario, D.; Ben Avraham, B.; Ben Gal, T.; Weitsman, T.; Hasin, T.; Ince, H.; Feickert, S.; D’Ancona, G.; et al. The V-LAP System for Remote Left Atrial Pressure Monitoring of Patients with Heart Failure: Remote Left Atrial Pressure Monitoring. J. Card. Fail. 2022, 28, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, W.S.; Wetterling, F.; Testani, J.M.; Borlaug, B.A.; Fudim, M.; Damman, K.; Gray, A.; Gaines, P.; Poloczek, M.; Madden, S.; et al. Safety and performance of a novel implantable sensor in the inferior vena cava under acute and chronic intravascular volume modulation. Eur. J. Heart Fail. 2023, 25, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Ivey-Miranda, J.B.; Wetterling, F.; Gaul, R.; Sheridan, S.; Asher, J.L.; Rao, V.S.; Maulion, C.; Mahoney, D.; Mebazaa, A.; Gray, A.P.; et al. Changes in inferior vena cava area represent a more sensitive metric than changes in filling pressures during experimental manipulation of intravascular volume and tone. Eur. J. Heart Fail. 2022, 24, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Varma, N.; Wilkoff, B. Device features for managing patients with heart failure. Heart Fail. Clin. 2011, 7, 215–225. [Google Scholar] [CrossRef]
- Hindricks, G.; Taborsky, M.; Glikson, M.; Heinrich, U.; Schumacher, B.; Katz, A.; Brachmann, J.; Lewalter, T.; Goette, A.; Block, M.; et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): A randomised controlled trial. Lancet 2014, 384, 583–590. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.-A.; Cleland, J.G.F.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar] [CrossRef]
- Abraham, W.T.; Compton, S.; Haas, G.; Foreman, B.; Canby, R.C.; Fishel, R.; McRae, S.; Toledo, G.B.; Sarkar, S.; Hettrick, D.A.; et al. Intrathoracic impedance vs daily weight monitoring for predicting worsening heart failure events: Results of the Fluid Accumulation Status Trial (FAST). Congest. Heart Fail. 2011, 17, 51–55. [Google Scholar] [CrossRef]
- Brachmann, J.; Böhm, M.; Rybak, K.; Klein, G.; Butter, C.; Klemm, H.; Schomburg, R.; Siebermair, J.; Israel, C.; Sinha, A.-M.; et al. Fluid status monitoring with a wireless network to reduce cardiovascular-related hospitalizations and mortality in heart failure: Rationale and design of the OptiLink HF Study (Optimization of Heart Failure Management using OptiVol Fluid Status Monitoring and CareLink). Eur. J. Heart Fail. 2011, 13, 796–804. [Google Scholar] [CrossRef]
- Böhm, M.; Drexler, H.; Oswald, H.; Rybak, K.; Bosch, R.; Butter, C.; Klein, G.; Gerritse, B.; Monteiro, J.; Israel, C.; et al. Fluid status telemedicine alerts for heart failure: A randomized controlled trial. Eur. Heart J. 2016, 37, 3154–3163. [Google Scholar] [CrossRef]
- Whellan, D.J.; Ousdigian, K.T.; Al-Khatib, S.M.; Pu, W.; Sarkar, S.; Porter, C.B.; Pavri, B.B.; O’Connor, C.M. Combined heart failure device diagnostics identify patients at higher risk of subsequent heart failure hospitalizations: Results from PARTNERS HF (Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients with Heart Failure) study. J. Am. Coll. Cardiol. 2010, 55, 1803–1810. [Google Scholar] [CrossRef]
- Morgan, J.M.; Kitt, S.; Gill, J.; McComb, J.M.; Ng, G.A.; Raftery, J.; Roderick, P.; Seed, A.; Williams, S.G.; Witte, K.K.; et al. Remote management of heart failure using implantable electronic devices. Eur. Heart J. 2017, 38, 2352–2360. [Google Scholar] [CrossRef] [PubMed]
- Boehmer, J.P.; Hariharan, R.; Devecchi, F.G.; Smith, A.L.; Molon, G.; Capucci, A.; An, Q.; Averina, V.; Stolen, C.M.; Thakur, P.H.; et al. A Multisensor Algorithm Predicts Heart Failure Events in Patients with Implanted Devices: Results from the MultiSENSE Study. JACC Heart Fail. 2017, 5, 216–225. [Google Scholar] [CrossRef] [PubMed]
- D’onofrio, A.; Solimene, F.; Calò, L.; Calvi, V.; Viscusi, M.; Melissano, D.; Russo, V.; Rapacciuolo, A.; Campana, A.; Caravati, F.; et al. Combining home monitoring temporal trends from implanted defibrillators and baseline patient risk profile to predict heart failure hospitalizations: Results from the SELENE HF study. Eurospace 2022, 24, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Varma, N.; Kacet, S.; Lewalter, T.; Søgaard, P.; Guédon-Moreau, L.; Proff, J.; Gerds, T.A.; Anker, S.D.; Torp-Pedersen, C. Daily remote monitoring of implantable cardioverter-defibrillators: Insights from the pooled patient-level data from three randomized controlled trials (IN-TIME, ECOST, TRUST). Eur. Heart J. 2017, 38, 1749–1755. [Google Scholar] [CrossRef]
- Boehmer, J.P.; Cremer, S.; Abo-Auda, W.S.; Stokes, D.R.; Hadi, A.; McCann, P.J.; Burch, A.E.; Bonderman, D. Impact of Heart Failure Management Using Thoracic Fluid Monitoring from a Novel Wearable Sensor: Results of the Benefits of Microcor (μCor™) in Ambulatory Decompensated Heart Failure (BMAD) Trial. In Proceedings of the American College of Cardiology Annual Scientific Session, New Orleans, LA, USA, 4–6 May 2023. [Google Scholar]
- Lala, A.; Barghash, M.H.; Giustino, G.; Alvarez-Garcia, J.; Konje, S.; Parikh, A.; Ullman, J.; Keith, B.; Donehey, J.; Mitter, S.S.; et al. Early use of remote dielectric sensing after hospitalization to reduce heart failure readmissions. ESC Heart Fail. 2021, 8, 1047–1054. [Google Scholar] [CrossRef]
- Abraham, W.T.; Anker, S.; Burkhoff, D.; Cleland, J.; Gorodeski, E.; Jaarsma, T.; Small, R.; Lindenfeld, J.; Miller, A.; Ogenstad, S.; et al. Primary Results of the Sensible Medical Innovations Lung Fluid Status Monitor Allows Reducing Readmission Rate of Heart Failure Patients (smile) Trial. J. Card. Fail. 2019, 25, 938. [Google Scholar] [CrossRef]
- Fudim, M.; Mirro, M.; Cheng, H.M. Audicor Remote Patient Monitoring: FDA Breakthrough Device and Technology for Heart Failure Management. Basic Transl. Sci. 2022, 7, 313–315. [Google Scholar] [CrossRef]
- Sung, S.-H.; Huang, C.-J.; Cheng, H.-M.; Huang, W.-M.; Yu, W.-C.; Chen, C.-H. Effect of Acoustic Cardiography-guided Management on 1-year Outcomes in Patients with Acute Heart Failure. J. Card. Fail. 2020, 26, 142–150. [Google Scholar] [CrossRef]
- Kessler, D. A Novel Approach Using Continuous Monitoring of Peripheral Edema in Heart Failure Patients Allows Recognition of Acute Decompensation Early in the Window of Intervention. J. Card. Fail. 2022, 28, S119. [Google Scholar] [CrossRef]
- Neill, L.; Etemadi, M.; Klein, L.; Inan, O.T. Novel Noninvasive Biosensors and Artificial Intelligence for Optimized Heart Failure Management. JACC Basic Transl. Sci. 2022, 7, 316–318. [Google Scholar] [CrossRef]
- Shandhi, M.H.; Fan, J.; Heller, J.A.; Etemadi, M.; Klein, L.; Inan, O.T. Estimation of Changes in Intracardiac Hemodynamics Using Wearable Seismocardiography and Machine Learning in Patients with Heart Failure: A Feasibility Study. IEEE Trans. Biomed. Eng. 2022, 69, 2443–2455. [Google Scholar] [CrossRef] [PubMed]
- Mace, M.I. A Novel Multisensor Device for Absolute Intracardiac Pressure Measurement, Detection, and Management of Heart Failure. JACC Basic Transl. Sci. 2023, 8, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Stehlik, J.; Schmalfuss, C.; Bozkurt, B.; Nativi-Nicolau, J.; Wohlfahrt, P.; Wegerich, S.; Rose, K.; Ray, R.; Schofield, R.; Deswal, A.; et al. Continuous Wearable Monitoring Analytics Predict Heart Failure Hospitalization: The LINK-HF Multicenter Study. Circ. Heart Fail. 2020, 13, e006513. [Google Scholar] [CrossRef] [PubMed]
- Kennel, P.J.; Rosenblum, H.; Axsom, K.M.; Alishetti, S.; Brener, M.; Horn, E.; Kirtane, J.A.; Lin, E.; Griffin, J.M.; Maurer, M.S.; et al. Remote Cardiac Monitoring in Patients with Heart Failure: A Review. JAMA Cardiol. 2022, 7, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Fudim, M.; Yazdi, D.; Egolum, U.; Haghighat, A.; Kottam, A.; Sauer, A.J.; Shah, H.; Kumar, P.; Rakita, V.; Centen, C.; et al. Use of a Cardiac Scale to Predict Heart Failure Events: Design of SCALE-HF 1. Circ. Heart Fail. 2023, 16, e010012. [Google Scholar] [CrossRef] [PubMed]
- Cowie, M.R.; Sarkar, S.; Koehler, J.; Whellan, D.J.; Crossley, G.H.; Tang, W.H.W.; Abraham, W.T.; Sharma, V.; Santini, M. Development and validation of an integrated diagnostic algorithm derived from parameters monitored in implantable devices for identifying patients at risk for heart failure hospitalization in an ambulatory setting. Eur. Heart J. 2013, 34, 2472–2480. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.A.; Sharma, V.; McCann, M.; Koehler, J.; Tsang, B.; Zieroth, S. Prospective evaluation of integrated device diagnostics for heart failure management: Results of the TRIAGE-HF study. ESC Heart Fail. 2018, 5, 809–817. [Google Scholar] [CrossRef]
- Zile, M.R.; Kahwash, R.; Sarkar, S.; Koehler, J.; Butler, J. Temporal Characteristics of Device-Based Individual and Integrated Risk Metrics in Patients with Chronic Heart Failure. JACC Heart Fail. 2023, 11, 143–156. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Study | Patient Population | Data Collection and Storage | Frequency of Data Monitoring and Data Management | Outcome |
|---|---|---|---|---|---|
| Implantable pulmonary artery pressure monitoring devices | |||||
| CardioMEMS | CHAMPION (2007–2010) | 550 patients with NYHA class III HF across 64 sites in the U.S. |
|
|
|
| Postapproval study (2014–2017) | 1200 patients with NYHA class III HF and prior HFH within 12 months across 104 sites in the U.S. |
|
| ||
| GUIDE-HF (2018–2022) | 1000 patients with NYHA class II–IV HF and prior HFH within 12 months or elevated BNP across 118 sites in the U.S. and Canada |
|
| ||
| MEMS-HF (2016–2020) | 234 patients with NYHA class III HF across 31 sites in Europe |
|
| ||
| MONITOR-HF (2019–2022) | 348 patients with NYHA III and prior HFH across 25 sites in the Netherlands |
|
| ||
| Cordella endotronix | SIRONA (2017–2019) | 15 patients with NYHA class III HF in Europe |
|
|
|
| SIRONA II (2019–2021) | 81 patients with NYHA class III HF in Europe |
| |||
| PROACTIVE-HF (2020-estimated 9/2023) | 456 patients with NYHA class III HF currently enrolled across 79 sites in the U.S. and Europe |
|
| ||
| Implantable left atrial pressure monitoring devices | |||||
| Vectorius V-LAP | VECTOR-HF (2019-estimated 12/2023) | 24 patients with NYHA class III HF across two sites in Europe |
|
|
|
| Implantable inferior vena cava monitoring devices | |||||
| FIRE1 | FUTURE-HF (NCT04203576) (2019-estimated 8/2023) | Goal enrollment of 50 patients with HF and prior HFH within 6 months across 10 sites in Europe |
|
|
|
| Implantable cardiac monitors | |||||
| LUX-Dx ICM | TRENDS (NCT04790344) (2021-estimated 5/2026) | Goal enrollment of 525 patients with NYHA class II–III HF across 74 sites in the U.S. |
|
|
|
| Reveal LINQ ICM | ALLEVIATE-HF (NCT04452149) (2020-estimated 11/2024) | Goal enrollment of 700 patients with NYHA class II–III across 59 sites in the U.S. |
|
|
|
| Device | Study | Patient Population | Data Collection and Storage | Frequency of Data Monitoring and Data Management | Outcome |
|---|---|---|---|---|---|
| Cardiovascular Implantable Electronic Device (CIED) Monitoring | |||||
| CIEDs | FAST (2003–2008) | 156 patients with NYHA class III–IV HF and a Medtronic CIED |
|
|
|
| OptiLINK HF (2008–2014) | 1002 patients with NYHA class II–III HF, a Medtronic CIED, prior HFH within 12 months, recent diuretic treatment, or elevated BNP across 1 site in Europe |
|
|
| |
| PARTNERS-HF (2004–2008) | 694 patients with NYHA class III–IV HF and Medtronic CIED across 93 sites in the U.S. |
|
|
| |
| REM-HF (2011–2014) | 1650 patients with NYHA class II–IV HF with a CIED |
|
|
| |
| MULTISENSE (2010–2014) | 900 patients with NYHA class II–III HF with a CIED across 99 sites in Europe, Asia, and the U.S. |
|
|
| |
| SELENE HF (2012–2017) | 918 patients with NYHA class II–III HF across 34 sites in Europe |
|
|
| |
| TRUST (2005–2009), ECOST (2007–2010), IN-TIME (2007–2012) | 2405 patients with HF and varying inclusion criteria across 171 sites in Europe and the U.S. |
|
|
| |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobe, E.A.; McVeigh, T.; Hameed, I.; Fudim, M. Heart Failure Remote Monitoring: A Review and Implementation How-To. J. Clin. Med. 2023, 12, 6200. https://doi.org/10.3390/jcm12196200
Kobe EA, McVeigh T, Hameed I, Fudim M. Heart Failure Remote Monitoring: A Review and Implementation How-To. Journal of Clinical Medicine. 2023; 12(19):6200. https://doi.org/10.3390/jcm12196200
Chicago/Turabian StyleKobe, Elizabeth A., Todd McVeigh, Ishaque Hameed, and Marat Fudim. 2023. "Heart Failure Remote Monitoring: A Review and Implementation How-To" Journal of Clinical Medicine 12, no. 19: 6200. https://doi.org/10.3390/jcm12196200