Decoding Sepsis-Induced Disseminated Intravascular Coagulation: A Comprehensive Review of Existing and Emerging Therapies

 ,
,
Abstract
:1. Introduction
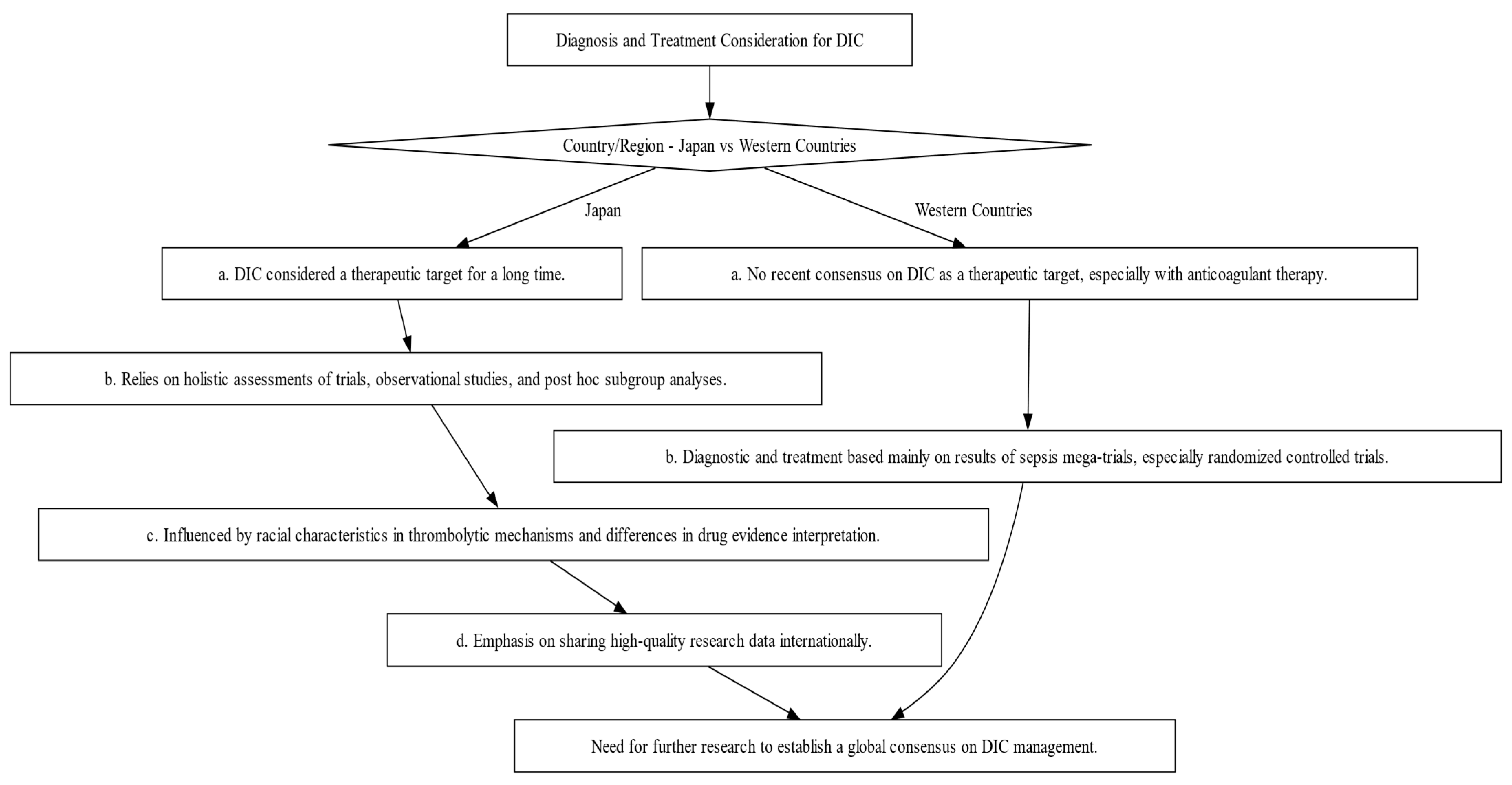
2. Comparative Analysis of DIC Diagnosis and Treatment: Eastern vs. Western Approaches
3. Can Sepsis-Induced DIC Patients Benefit from Corticosteroids?
4. Evidence from Studies: Rtm’s Effectiveness in Sepsis-Induced DIC
5. Vitamin C in Sepsis and DIC: Promise or Paradox?
6. Fibrinolytic Therapy in Sepsis-Induced DIC: A Potential Game-Changer?
7. Platelet Transfusion in Sepsis-Induced DIC: Navigating Controversy and Conflicting Evidence
8. Immunomodulatory Therapy: G-CSF, GM-CSF, IFN-γ, MSCs in Sepsis, DIC, and Their Implications for Clinical Practice & Severe COVID-19
9. The Controversy Surrounding Anticoagulant Therapy for Sepsis and DIC Management: An In-Depth Analysis
9.1. Summary of Previous Research
9.2. Study Hypothesis, Significance, and Unanswered Questions
9.3. Antithrombin and Combination Therapy
9.4. Optimal Therapeutic Targets and Considerations in Anticoagulant Therapy
9.5. Biomarkers, Machine Learning, and Emerging Trends in Sepsis Diagnosis and DIC Management
9.6. Challenges and Future Perspectives
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Tsantes, A.G.; Parastatidou, S.; Tsantes, E.A.; Bonova, E.; Tsante, K.A.; Mantzios, P.G.; Vaiopoulos, A.G.; Tsalas, S.; Konstantinidi, A.; Houhoula, D. Sepsis-Induced Coagulopathy: An Update on Pathophysiology, Biomarkers, and Current Guidelines. Life 2023, 13, 350. [Google Scholar] [CrossRef] [PubMed]
- Giustozzi, M.; Ehrlinder, H.; Bongiovanni, D.; Borovac, J.A.; Guerreiro, R.A.; Gąsecka, A.; Papakonstantinou, P.E.; Parker, W.A.E. Coagulopathy and Sepsis: Pathophysiology, Clinical Manifestations and Treatment. Blood Rev. 2021, 50, 100864. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.S.; Mannino, D.M.; Eaton, S.; Moss, M. The Epidemiology of Sepsis in the United States from 1979 through 2000. N. Engl. J. Med. 2003, 348, 1546–1554. [Google Scholar] [CrossRef]
- Iba, T.; Di Nisio, M.; Thachil, J.; Wada, H.; Asakura, H.; Sato, K.; Saitoh, D. A Proposal of the Modification of Japanese Society on Thrombosis and Hemostasis (JSTH) Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria for Sepsis-Associated DIC. J. Clin. Appl. Thromb. Hemost. 2018, 24, 439–445. [Google Scholar] [CrossRef]
- Iba, T.; Umemura, Y.; Watanabe, E.; Wada, T.; Hayashida, K.; Kushimoto, S. Diagnosis of Sepsis-induced Disseminated Intravascular Coagulation and Coagulopathy. J. Acute Med. Surg. 2019, 6, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, A.P.; Bernard, G.R. Treating Patients with Severe Sepsis. N. Engl. J. Med. 1999, 340, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Watanabe, E.; Umemura, Y.; Wada, T.; Hayashida, K.; Kushimoto, S.; Japanese Surviving Sepsis Campaign Guideline Working Group for Disseminated Intravascular Coagulation; Wada, H. Sepsis-Associated Disseminated Intravascular Coagulation and Its Differential Diagnoses. J. Intensive Care 2019, 7, 32. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H. Haemostasis Inflammation and Thrombosis: Roles of Neutrophils, Platelets and Endothelial Cells and Their Interactions in Thrombus Formation during Sepsis. J. Thromb. Haemost. 2018, 16, 231–241. [Google Scholar] [CrossRef]
- Semeraro, N.; Ammollo, C.T.; Semeraro, F.; Colucci, M. Coagulopathy of Acute Sepsis. In Proceedings of the Seminars in Thrombosis and Hemostasis; Thieme Medical Publishers: Stuttgart, Germany, 2015; Volume 41, pp. 650–658. [Google Scholar]
- Engelmann, B.; Massberg, S. Thrombosis as an Intravascular Effector of Innate Immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef]
- Corrigan, J.J., Jr.; Ray, W.L.; May, N. Changes in the Blood Coagulation System Associated with Septicemia. N. Engl. J. Med. 1968, 279, 851–856. [Google Scholar] [CrossRef]
- Østerud, B.; Bjørklid, E. The Tissue Factor Pathway in Disseminated Intravascular Coagulation. In Proceedings of the Seminars in Thrombosis and Hemostasis; Thieme Medical Publishers, Inc.: Stuttgart, Germany, 2001; Volume 27, pp. 605–618. [Google Scholar]
- Nieman, M.T. Protease-Activated Receptors in Hemostasis. Blood J. Am. Soc. Hematol. 2016, 128, 169–177. [Google Scholar] [CrossRef]
- Ma, R.; Xie, R.; Yu, C.; Si, Y.; Wu, X.; Zhao, L.; Yao, Z.; Fang, S.; Chen, H.; Novakovic, V. Phosphatidylserine-Mediated Platelet Clearance by Endothelium Decreases Platelet Aggregates and Procoagulant Activity in Sepsis. Sci. Rep. 2017, 7, 4978. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Levi, M.; Toh, C.-H. Disseminated Intravascular Coagulation. J. Nat. Rev. Dis. Primers 2016, 2, 1–16. [Google Scholar]
- Levi, M.; van der Poll, T. Coagulation and Sepsis. Thromb. Res. 2017, 149, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Chris Nickson Sepsis Definitions and Diagnosis. Available online: https://litfl.com/sepsis-definitions-and-diagnosis/ (accessed on 3 November 2020).
- Wada, H.; Thachil, J.; Di Nisio, M.; Mathew, P.; Kurosawa, S.; Gando, S.; Kim, H.K.; Nielsen, J.D.; Dempfle, C.; Levi, M. Guidance for Diagnosis and Treatment of Disseminated Intravascular Coagulation from Harmonization of the Recommendations from Three Guidelines. J. Thromb. Haemost. 2013, 11, 761–767. [Google Scholar] [CrossRef]
- Di Nisio, M.; Baudo, F.; Cosmi, B.; D’Angelo, A.; De Gasperi, A.; Malato, A.; Schiavoni, M.; Squizzato, A. Diagnosis and Treatment of Disseminated Intravascular Coagulation: Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). J. Thromb. Res. 2012, 129, e177–e184. [Google Scholar] [CrossRef]
- Asakura, H.; Takahashi, H.; Uchiyama, T.; Eguchi, Y.; Okamoto, K.; Kawasugi, K.; Madoiwa, S.; Wada, H. Proposal for New Diagnostic Criteria for DIC from the Japanese Society on Thrombosis and Hemostasis. Thromb. J. 2016, 14, 42. [Google Scholar] [CrossRef]
- Gando, S.; Wada, H.; Thachil, J.; Scientific, T. Differentiating Disseminated Intravascular Coagulation (DIC) with the Fibrinolytic Phenotype from Coagulopathy of Trauma and Acute Coagulopathy of Trauma-Shock (COT/ACOTS). J. Thromb. Haemost. 2013, 11, 826–835. [Google Scholar] [CrossRef]
- Gando, S.; Hayakawa, M. Pathophysiology of Trauma-Induced Coagulopathy and Management of Critical Bleeding Requiring Massive Transfusion. In Proceedings of the Seminars in Thrombosis and Hemostasis; Thieme Medical Publishers: Stuttgart, Germany, 2015; pp. 155–165. [Google Scholar]
- Yu, M.; Nardella, A.; Pechet, L. Screening Tests of Disseminated Intravascular Coagulation: Guidelines for Rapid and Specific Laboratory Diagnosis. Crit. Care Med. 2000, 28, 1777–1780. [Google Scholar] [CrossRef]
- Disseminated Intravascular Coagulation—DIC. Choose the Right Test. Available online: https://arupconsult.com/content/disseminated-intravascular-coagulation (accessed on 9 September 2023).
- Disseminated Intravascular Coagulation (DIC). Causes & Symptoms. Available online: https://my.clevelandclinic.org/health/diseases/21836-disseminated-intravascular-coagulation-dic (accessed on 9 September 2023).
- Unar, A.; Bertolino, L.; Patauner, F.; Gallo, R.; Durante-Mangoni, E. Pathophysiology of Disseminated Intravascular Coagulation in Sepsis: A Clinically Focused Overview. Cells 2023, 12, 2120. [Google Scholar] [CrossRef]
- Iba, T.; Di Nisio, M.; Levy, J.H.; Kitamura, N.; Thachil, J. New Criteria for Sepsis-Induced Coagulopathy (SIC) Following the Revised Sepsis Definition: A Retrospective Analysis of a Nationwide Survey. BMJ Open 2017, 7, e017046. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Iba, T.; Eguchi, Y.; Ohtomo, Y.; Okamoto, K.; Koseki, K.; Mayumi, T.; Murata, A.; Ikeda, T.; Ishikura, H. A Multicenter, Prospective Validation of Disseminated Intravascular Coagulation Diagnostic Criteria for Critically Ill Patients: Comparing Current Criteria. Crit. Care Med. 2006, 34, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Ushio, N.; Wada, T.; Ono, Y.; Yamakawa, K. Sepsis-induced Disseminated Intravascular Coagulation: An International Estrangement of Disease Concept. Acute Med. Surg. 2023, 10, e00843. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Helms, J.; Connors, J.M.; Levy, J.H. The Pathophysiology, Diagnosis, and Management of Sepsis-Associated Disseminated Intravascular Coagulation. J. Intensive Care 2023, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Gibbison, B.; López-López, J.A.; Higgins, J.P.T.; Miller, T.; Angelini, G.D.; Lightman, S.L.; Annane, D. Corticosteroids in Septic Shock: A Systematic Review and Network Meta-Analysis. J. Crit. Care 2017, 21, 78. [Google Scholar] [CrossRef]
- Annane, D.; Bellissant, E.; Bollaert, P.E.; Briegel, J.; Keh, D.; Kupfer, Y. Corticosteroids for Treating Severe Sepsis and Septic Shock. J. Cochrane Database Syst. Rev. 2004, 1, 7. [Google Scholar]
- Salluh, J.I.F.; Povoa, P. Corticosteroids in Severe Sepsis and Septic Shock: A Concise Review. J. Shock. 2017, 47, 47–51. [Google Scholar] [CrossRef]
- Rochwerg, B.; Oczkowski, S.J.; Siemieniuk, R.A.C.; Agoritsas, T.; Belley-Cote, E.; D’Aragon, F.; Duan, E.; English, S.; Gossack-Keenan, K.; Alghuroba, M. Corticosteroids in Sepsis: An Updated Systematic Review and Meta-Analysis. J. Crit. Care Med. 2018, 46, 1411–1420. [Google Scholar] [CrossRef]
- Gazzaniga, G.; Tavecchia, G.A.; Bravi, F.; Scavelli, F.; Travi, G.; Campo, G.; Vandenbriele, C.; Tritschler, T.; Sterne, J.A.C.; Murthy, S. The Effect of Antithrombotic Treatment on Mortality in Patients with Acute Infection: A Meta-Analysis of Randomized Clinical Trials. J. Int. J. Cardiol. 2023, 383, 75–81. [Google Scholar] [CrossRef]
- Ni, Y.-N.; Liu, Y.-M.; Wang, Y.-W.; Liang, B.-M.; Liang, Z.-A. Can Corticosteroids Reduce the Mortality of Patients with Severe Sepsis? A Systematic Review and Meta-Analysis. Am. J. Emerg. Med. 2019, 37, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Song, H.; Zhai, R.; Song, G.; Li, H.; Ding, X.; Kan, Q.; Sun, T. Corticosteroids for Treating Sepsis in Adult Patients: A Systematic Review and Meta-Analysis. J. Front. Immunol. 2021, 12, 709155. [Google Scholar] [CrossRef] [PubMed]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R.; Hirayama, A.; Aoki, Y.; Aoki, N. Thrombomodulin Alfa in the Treatment of Infectious Patients Complicated by Disseminated Intravascular Coagulation: Subanalysis from the Phase 3 Trial. J. Shock. 2011, 35, 349–354. [Google Scholar] [CrossRef]
- Liu, X.; Wang, X.; Liu, X.; Hao, D.; Jaladat, Y.; Lu, F.; Sun, T.; Lv, C. Low-dose Heparin as Treatment for Early Disseminated Intravascular Coagulation during Sepsis: A Prospective Clinical Study. J. Exp. Ther. Med. 2014, 7, 604–608. [Google Scholar] [CrossRef]
- Wada, H.; Matsumoto, T.; Yamashita, Y. Diagnosis and Treatment of Disseminated Intravascular Coagulation (DIC) According to Four DIC Guidelines. J. Intensive Care 2014, 2, 15. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Francois, B.; Zabolotskikh, I.; Daga, M.K.; Lascarrou, J.-B.; Kirov, M.Y.; Pettilä, V.; Wittebole, X.; Meziani, F.; Mercier, E. Effect of a Recombinant Human Soluble Thrombomodulin on Mortality in Patients with Sepsis-Associated Coagulopathy: The SCARLET Randomized Clinical Trial. J. Jama 2019, 321, 1993–2002. [Google Scholar] [CrossRef] [PubMed]
- Yamakawa, K.; Murao, S.; Aihara, M. Recombinant Human Soluble Thrombomodulin in Sepsis-Induced Coagulopathy: An Updated Systematic Review and Meta-Analysis. J. Thromb. 2019, 119, 56–65. [Google Scholar] [CrossRef]
- Tagami, T.; Matsui, H.; Horiguchi, H.; Fushimi, K.; Yasunaga, H. Antithrombin and Mortality in Severe Pneumonia Patients with Sepsis-associated Disseminated Intravascular Coagulation: An Observational Nationwide Study. J. Thromb. Haemost. 2014, 12, 1470–1479. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Antithrombin Concentrate Use in Disseminated Intravascular Coagulation of Sepsis: Meta-analyses Revisited. J. Thromb. Haemost. 2018, 16, 455–457. [Google Scholar] [CrossRef]
- Iba, T.; Gando, S.; Thachil, J. Anticoagulant Therapy for Sepsis-associated Disseminated Intravascular Coagulation: The View from Japan. J. Thromb. Haemost. 2014, 12, 1010–1019. [Google Scholar] [CrossRef]
- Dhainaut, J.; Yan, S.B.; Joyce, D.E.; Pettilä, V.; Basson, B.; Brandt, J.T.; Sundin, D.P.; Levi, M. Treatment Effects of Drotrecogin Alfa (Activated) in Patients with Severe Sepsis with or without Overt Disseminated Intravascular Coagulation 1. J. Thromb. Haemost. 2004, 2, 1924–1933. [Google Scholar] [CrossRef]
- Aoki, N.; Matsuda, T.; Saito, H.; Takatsuki, K.; Okajima, K.; Takahashi, H.; Takamatsu, J.; Asakura, H.; Ogawa, N. A Comparative Double-Blind Randomized Trial of Activated Protein C and Unfractionated Heparin in the Treatment of Disseminated Intravascular Coagulation. J. Int. J. Hematol. 2002, 75, 540–547. [Google Scholar] [CrossRef]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A. High-Dose Antithrombin III in Severe Sepsis: A Randomized Controlled Trial. JAMA 2001, 286, 1869–1878. [Google Scholar] [CrossRef] [PubMed]
- Nishida, O.; Ogura, H.; Egi, M.; Fujishima, S.; Hayashi, Y.; Iba, T.; Imaizumi, H.; Inoue, S.; Kakihana, Y.; Kotani, J. The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2016 (J-SSCG 2016). J. Intensive Care 2018, 6, 7. [Google Scholar] [CrossRef]
- Yao, Y.Y.; Lin, L.L.; Gu, H.Y.; Wu, J.Y.; Niu, Y.M.; Zhang, C. Are Corticosteroids Beneficial for Sepsis and Septic Shock? Based on Pooling Analysis of 16 Studies. Front. Pharmacol. 2019, 10, 714. [Google Scholar] [CrossRef]
- Valeriani, E.; Squizzato, A.; Gallo, A.; Porreca, E.; Vincent, J.; Iba, T.; Hagiwara, A.; Di Nisio, M. Efficacy and Safety of Recombinant Human Soluble Thrombomodulin in Patients with Sepsis-associated Coagulopathy: A Systematic Review and Meta-analysis. J. Thromb. Haemost. 2020, 18, 1618–1625. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H. Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. Anesthesiol. 2020, 132, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, F.; Masse, M.-H.; Menard, J.; Sprague, S.; Pinto, R.; Heyland, D.K.; Cook, D.J.; Battista, M.-C.; Day, A.G.; Guyatt, G.H. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. N. Engl. J. Med. 2022, 386, 2387–2398. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Oudemans-van Straaten, H.M.; Berger, M.M. Vitamin Therapy in Critically Ill Patients: Focus on Thiamine, Vitamin C, and Vitamin D. J. Intensive Care Med. 2018, 44, 1940–1944. [Google Scholar] [CrossRef]
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef]
- Muhammad, M.; Jahangir, A.; Kassem, A.; Sattar, S.B.A.; Jahangir, A.; Sahra, S.; Niazi, M.R.K.; Mustafa, A.; Zia, Z.; Siddiqui, F.S. The Role and Efficacy of Vitamin C in Sepsis: A Systematic Review and Meta-Analysis. J. Adv. Respir. Med. 2022, 90, 281–299. [Google Scholar] [CrossRef] [PubMed]
- Truwit, J.D.; Hite, R.D.; Morris, P.E.; DeWilde, C.; Priday, A.; Fisher, B.; Thacker, L.R.; Natarajan, R.; Brophy, D.F.; Sculthorpe, R. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients with Sepsis and Severe Acute Respiratory Failure: The CITRIS-ALI Randomized Clinical Trial. J. JAMA 2019, 322, 1261–1270. [Google Scholar]
- Brown, J.; Robertson, C.; Sevilla, L.; Garza, J.; Rashid, H.; Benitez, A.C.; Shipotko, M.; Ali, Z. A Systematic Review and Meta-Analysis on Possible Role of Vitamin c in Sepsis. J. Cureus 2022, 14, e32886. [Google Scholar] [CrossRef] [PubMed]
- Ammar, M.A.; Ammar, A.A.; Condeni, M.S.; Bell, C.M. Vitamin C for Sepsis and Septic Shock. J. Am. J. Ther. 2021, 28, e649–e679. [Google Scholar] [CrossRef]
- Kashiouris, M.G.; L’Heureux, M.; Cable, C.A.; Fisher, B.J.; Leichtle, S.W.; Fowler, A.A. The Emerging Role of Vitamin C as a Treatment for Sepsis. J. Nutr. 2020, 12, 292. [Google Scholar] [CrossRef]
- Adelborg, K.; Larsen, J.B.; Hvas, A. Disseminated Intravascular Coagulation: Epidemiology, Biomarkers, and Management. J. Br. J. Haematol. 2021, 192, 803–818. [Google Scholar] [CrossRef]
- Carey, M.J.; Rodgers, G.M. Disseminated Intravascular Coagulation: Clinical and Laboratory Aspects. J. Am. J. Hematol. 1998, 59, 65–73. [Google Scholar] [CrossRef]
- Papageorgiou, C.; Jourdi, G.; Adjambri, E.; Walborn, A.; Patel, P.; Fareed, J.; Elalamy, I.; Hoppensteadt, D.; Gerotziafas, G.T. Disseminated Intravascular Coagulation: An Update on Pathogenesis, Diagnosis, and Therapeutic Strategies. J. Clin. Appl. Thromb. Hemost. 2018, 24, 8S–28S. [Google Scholar] [CrossRef]
- Wada, H.; Asakura, H.; Okamoto, K.; Iba, T.; Uchiyama, T.; Kawasugi, K.; Koga, S.; Mayumi, T.; Koike, K.; Gando, S. Expert Consensus for the Treatment of Disseminated Intravascular Coagulation in Japan. J. Thromb. Res. 2010, 125, 6–11. [Google Scholar] [CrossRef]
- Schouten, M.; van der Sluijs, K.F.; Gerlitz, B.; Grinnell, B.W.; Roelofs, J.J.T.H.; Levi, M.M.; van ’t Veer, C.; Poll, T.V.D. Activated Protein C Ameliorates Coagulopathy but Does Not Influence Outcome in Lethal H1N1 Influenza: A Controlled Laboratory Study. Crit. Care 2010, 14, R65. [Google Scholar] [CrossRef]
- Zeerleder, S.; Hack, C.E.; Wuillemin, W.A. Disseminated Intravascular Coagulation in Sepsis. J. Chest 2005, 128, 2864–2875. [Google Scholar] [CrossRef] [PubMed]
- Andrew, M.; Vegh, P.; Caco, C.; Kirpalani, H.; Jefferies, A.; Ohlsson, A.; Watts, J.; Saigal, S.; Milner, R.; Wang, E. A Randomized, Controlled Trial of Platelet Transfusions in Thrombocytopenic Premature Infants. J. Pediatr. 1993, 123, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Estcourt, L.J.; Desborough, M.J.R.; Hopewell, S.; Doree, C.; Stanworth, S.J. Comparison of Different Platelet Transfusion Thresholds Prior to Insertion of Central Lines in Patients with Thrombocytopenia. J. Cochrane Database Syst. Rev. 2015, 2015, CD011771. [Google Scholar]
- He, S.; Fan, C.; Ma, J.; Tang, C.; Chen, Y. Platelet Transfusion in Patients with Sepsis and Thrombocytopenia: A Propensity Score-Matched Analysis Using a Large ICU Database. J. Front. Med. 2022, 9, 830177. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, T.; Inoue, S.; Sakamoto, S.; Sumi, Y.; Nishida, O.; Hayashida, K.; Hara, Y.; Fukuda, T.; Matsushima, A.; Matsuda, A. The Anticoagulant Treatment for Sepsis Induced Disseminated Intravascular Coagulation; Network Meta-Analysis. J. Thromb. Res. 2018, 171, 136–142. [Google Scholar] [CrossRef]
- Muzaffar, S.N.; Baronia, A.K.; Azim, A.; Verma, A.; Gurjar, M.; Poddar, B.; Singh, R.K. Thromboelastography for Evaluation of Coagulopathy in Nonbleeding Patients with Sepsis at Intensive Care Unit Admission. Indian J. Crit. Care Med. Off. Publ. Indian Soc. Crit. Care Med. 2017, 21, 268. [Google Scholar]
- Christaki, E.; Giamarellos-Bourboulis, E.J. The Beginning of Personalized Medicine in Sepsis: Small Steps to a Bright Future. J. Clin. Genet. 2014, 86, 56–61. [Google Scholar] [CrossRef]
- Kudo, D.; Hayakawa, M.; Ono, K.; Yamakawa, K. Impact of Non-Anticoagulant Therapy on Patients with Sepsis-Induced Disseminated Intravascular Coagulation: A Multicenter, Case-Control Study. J. Thromb. Res. 2018, 163, 22–29. [Google Scholar] [CrossRef]
- Mohammad, R.A. Use of Granulocyte Colony-Stimulating Factor in Patients with Severe Sepsis or Septic Shock. J. Am. J. Health-Syst. Pharm. 2010, 67, 1238–1245. [Google Scholar] [CrossRef]
- Mathias, B.; Szpila, B.E.; Moore, F.A.; Efron, P.A.; Moldawer, L.L. A Review of GM-CSF Therapy in Sepsis. J. Med. 2015, 94, e2044. [Google Scholar] [CrossRef]
- Le Blanc, K.; Frassoni, F.; Ball, L.; Locatelli, F.; Roelofs, H.; Lewis, I.; Lanino, E.; Sundberg, B.; Bernardo, M.E.; Remberger, M. Mesenchymal Stem Cells for Treatment of Steroid-Resistant, Severe, Acute Graft-versus-Host Disease: A Phase II Study. J. Lancet 2008, 371, 1579–1586. [Google Scholar] [CrossRef]
- Weiss, A.R.R.; Dahlke, M.H. Immunomodulation by Mesenchymal Stem Cells (MSCs): Mechanisms of Action of Living, Apoptotic, and Dead MSCs. J. Front. Immunol. 2019, 10, 1191. [Google Scholar] [CrossRef] [PubMed]
- Elahi, K.C.; Klein, G.; Avci-Adali, M.; Sievert, K.D.; MacNeil, S.; Aicher, W.K. Human Mesenchymal Stromal Cells from Different Sources Diverge in Their Expression of Cell Surface Proteins and Display Distinct Differentiation Patterns. J. Stem Cells Int. 2016, 2016, 5646384. [Google Scholar] [CrossRef] [PubMed]
- Hass, R.; Kasper, C.; Böhm, S.; Jacobs, R. Different Populations and Sources of Human Mesenchymal Stem Cells (MSC): A Comparison of Adult and Neonatal Tissue-Derived MSC. J. Cell Commun. Signal. 2011, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- De Witte, S.F.H.; Lambert, E.E.; Merino, A.; Strini, T.; Douben, H.J.C.W.; O’Flynn, L.; Elliman, S.J.; De Klein, A.J.; Newsome, P.N.; Baan, C.C. Aging of Bone Marrow–and Umbilical Cord–Derived Mesenchymal Stromal Cells during Expansion. J. Cytotherapy 2017, 19, 798–807. [Google Scholar] [CrossRef]
- De Witte, S.F.H.; Merino, A.M.; Franquesa, M.; Strini, T.; Van Zoggel, J.A.A.; Korevaar, S.S.; Luk, F.; Gargesha, M.; O’Flynn, L.; Roy, D. Cytokine Treatment Optimises the Immunotherapeutic Effects of Umbilical Cord-Derived MSC for Treatment of Inflammatory Liver Disease. J. Stem Cell Res. Ther. 2017, 8, 140. [Google Scholar] [CrossRef]
- Eggenhofer, E.; Popp, F.C.; Mendicino, M.; Silber, P.; Van’T Hof, W.; Renner, P.; Hoogduijn, M.J.; Pinxteren, J.; van Rooijen, N.; Geissler, E.K. Heart Grafts Tolerized through Third-Party Multipotent Adult Progenitor Cells Can Be Retransplanted to Secondary Hosts with No Immunosuppression. J. Stem Cells Transl. Med. 2013, 2, 595–606. [Google Scholar] [CrossRef]
- Ge, W.; Jiang, J.; Arp, J.; Liu, W.; Garcia, B.; Wang, H.J.T. Regulatory T-Cell Generation and Kidney Allograft Tolerance Induced by Mesenchymal Stem Cells Associated with Indoleamine 2, 3-Dioxygenase Expression. J. Stem Cells Int. 2010, 90, 1312–1320. [Google Scholar] [CrossRef]
- Riquelme, P.; Haarer, J.; Kammler, A.; Walter, L.; Tomiuk, S.; Ahrens, N.; Wege, A.K.; Goecze, I.; Zecher, D.; Banas, B. TIGIT+ ITregs Elicited by Human Regulatory Macrophages Control T Cell Immunity. J. Nat. Commun. 2018, 9, 2858. [Google Scholar] [CrossRef]
- Takahashi, G.; Shibata, S.; Ishikura, H.; Miura, M.; Fukui, Y.; Inoue, Y.; Endo, S. Presepsin in the Prognosis of Infectious Diseases and Diagnosis of Infectious Disseminated Intravascular Coagulation: A Prospective, Multicentre, Observational Study. J. Eur. J. Anaesthesiol. EJA 2015, 32, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H.; Raj, A.; Warkentin, T.E. Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. Clin. Med. 2019, 8, 728. [Google Scholar] [CrossRef]
- Chang, P.; Liao, Y.; Guan, J.; Guo, Y.; Zhao, M.; Hu, J.; Zhou, J.; Wang, H.; Cen, Z.; Tang, Y. Combined Treatment with Hydrocortisone, Vitamin C, and Thiamine for Sepsis and Septic Shock: A Randomized Controlled Trial. J. Chest 2020, 158, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support Among Patients with Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef]
- Hwang, Y.S.; Suzuki, S.; Seita, Y.; Ito, J.; Sakata, Y.; Aso, H.; Sato, K.; Hermann, B.P.; Sasaki, K. Reconstitution of Prospermatogonial Specification in Vitro from Human Induced Pluripotent Stem Cells. Nat. Commun. 2020, 11, 5656. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, J.; Vassallo, A.V.; Patel, V.V.; Sullivan, J.B.; Cavanaugh, J.; Elbaga, Y. Outcomes of Metabolic Resuscitation Using Ascorbic Acid, Thiamine, and Glucocorticoids in the Early Treatment of Sepsis: The ORANGES Trial. J. Chest 2020, 158, 164–173. [Google Scholar] [CrossRef]
- Moskowitz, A.; Huang, D.T.; Hou, P.C.; Gong, J.; Doshi, P.B.; Grossestreuer, A.V.; Andersen, L.W.; Ngo, L.; Sherwin, R.L.; Berg, K.M.; et al. Effect of Ascorbic Acid, Corticosteroids, and Thiamine on Organ Injury in Septic Shock: The ACTS Randomized Clinical Trial. JAMA 2020, 324, 642–650. [Google Scholar] [CrossRef]
- Sevransky, J.E.; Rothman, R.E.; Hager, D.N.; Bernard, G.R.; Brown, S.M.; Buchman, T.G.; Busse, L.W.; Coopersmith, C.M.; DeWilde, C.; Ely, E.W.; et al. Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator- and Vasopressor-Free Days in Patients with Sepsis: The VICTAS Randomized Clinical Trial. JAMA 2021, 325, 742–750. [Google Scholar] [CrossRef]
- Müller, M.C.; Meijers, J.C.M.; Vroom, M.B.; Juffermans, N.P. Utility of Thromboelastography and/or Thromboelastometry in Adults with Sepsis: A Systematic Review. J. Crit. Care 2014, 18, R30. [Google Scholar] [CrossRef]
- Bolliger, D.; Seeberger, M.D.; Tanaka, K.A. Principles and Practice of Thromboelastography in Clinical Coagulation Management and Transfusion Practice. Transfus. Med. Rev. 2012, 26, 1–13. [Google Scholar] [CrossRef]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis—Pathophysiology and Therapeutic Concepts. J. Front. Med. 2021, 8, 609. [Google Scholar] [CrossRef]
- Peters van Ton, A.M.; Kox, M.; Abdo, W.F.; Pickkers, P. Precision Immunotherapy for Sepsis. J. Front. Immunol. 2018, 9, 1926. [Google Scholar] [CrossRef] [PubMed]
- Mithal, L.B.; Arshad, M.; Swigart, L.R.; Khanolkar, A.; Ahmed, A.; Coates, B.M. Mechanisms and Modulation of Sepsis-Induced Immune Dysfunction in Children. J. Pediatr. Res. 2022, 91, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Giarratano, A. Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. AboutOpen 2022, 9, 58–60. [Google Scholar] [CrossRef]
- Inata, Y. Should We Treat Sepsis-Induced DIC with Anticoagulants? J. Intensive Care 2020, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Kudo, D.; Hayakawa, M.; Iijima, H.; Yamakawa, K.; Saito, S.; Uchino, S.; Iizuka, Y.; Sanui, M.; Takimoto, K.; Mayumi, T. The Treatment Intensity of Anticoagulant Therapy for Patients with Sepsis-Induced Disseminated Intravascular Coagulation and Outcomes: A Multicenter Cohort Study. J. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619839154. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Tamura, T.; Sawatsubashi, Y. Sepsis and Disseminated Intravascular Coagulation. J. Intensive Care 2016, 4, 23. [Google Scholar] [CrossRef]
- Nasef, A.; Mathieu, N.; Chapel, A.; Frick, J.; François, S.; Mazurier, C.; Boutarfa, A.; Bouchet, S.; Gorin, N.-C.; Thierry, D. Immunosuppressive Effects of Mesenchymal Stem Cells: Involvement of HLA-G. J. Transplant. 2007, 84, 231–237. [Google Scholar] [CrossRef]
- Moll, G.; Geißler, S.; Catar, R.; Ignatowicz, L.; Hoogduijn, M.J.; Strunk, D.; Bieback, K.; Ringdén, O. Cryopreserved or Fresh Mesenchymal Stromal Cells: Only a Matter of Taste or Key to Unleash the Full Clinical Potential of MSC Therapy? J. Biobanking Cryopreserv. Stem Cells 2016, 951, 77–98. [Google Scholar]
- Luk, F.; Carreras-Planella, L.; Korevaar, S.S.; de Witte, S.F.H.; Borràs, F.E.; Betjes, M.G.H.; Baan, C.C.; Hoogduijn, M.J.; Franquesa, M. Inflammatory Conditions Dictate the Effect of Mesenchymal Stem or Stromal Cells on B Cell Function. J. Front. Immunol. 2017, 8, 1042. [Google Scholar] [CrossRef]
- Németh, K.; Leelahavanichkul, A.; Yuen, P.S.T.; Mayer, B.; Parmelee, A.; Doi, K.; Robey, P.G.; Leelahavanichkul, K.; Koller, B.H.; Brown, J.M. Bone Marrow Stromal Cells Attenuate Sepsis via Prostaglandin E2–Dependent Reprogramming of Host Macrophages to Increase Their Interleukin-10 Production. J. Nat. Med. 2009, 15, 42–49. [Google Scholar] [CrossRef]
- Obermajer, N.; Popp, F.C.; Soeder, Y.; Haarer, J.; Geissler, E.K.; Schlitt, H.J.; Dahlke, M.H. Conversion of Th17 into IL-17Aneg Regulatory T Cells: A Novel Mechanism in Prolonged Allograft Survival Promoted by Mesenchymal Stem Cell–Supported Minimized Immunosuppressive Therapy. J. Immunol. 2014, 193, 4988–4999. [Google Scholar] [CrossRef] [PubMed]
- Popp, F.C.; Eggenhofer, E.; Renner, P.; Slowik, P.; Lang, S.A.; Kaspar, H.; Geissler, E.K.; Piso, P.; Schlitt, H.J.; Dahlke, M.H. Mesenchymal Stem Cells Can Induce Long-Term Acceptance of Solid Organ Allografts in Synergy with Low-Dose Mycophenolate. J. Transplant. Immunol. 2008, 20, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Spaggiari, G.M.; Capobianco, A.; Abdelrazik, H.; Becchetti, F.; Mingari, M.C.; Moretta, L. Mesenchymal Stem Cells Inhibit Natural Killer–Cell Proliferation, Cytotoxicity, and Cytokine Production: Role of Indoleamine 2, 3-Dioxygenase and Prostaglandin E2. J. Blood J. Am. Soc. Hematol. 2008, 111, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Hoogduijn, M.J.; Baan, C.C.; Korevaar, S.S.; de Kuiper, R.; Yan, L.; Wang, L.; van Besouw, N.M. Adipose Tissue-Derived Mesenchymal Stem Cells Have a Heterogenic Cytokine Secretion Profile. J. Stem Cells Int. 2017, 2017, 4960831. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-L.; Leu, S.; Sung, H.-C.; Zhen, Y.-Y.; Cho, C.-L.; Chen, A.; Tsai, T.-H.; Chung, S.-Y.; Chai, H.-T.; Sun, C.-K. Impact of Apoptotic Adipose-Derived Mesenchymal Stem Cells on Attenuating Organ Damage and Reducing Mortality in Rat Sepsis Syndrome Induced by Cecal Puncture and Ligation. J. Transl. Med. 2012, 10, 1–14. [Google Scholar] [CrossRef]
- Baxter, M.A.; Wynn, R.F.; Jowitt, S.N.; Wraith, J.E.; Fairbairn, L.J.; Bellantuono, I. Study of Telomere Length Reveals Rapid Aging of Human Marrow Stromal Cells Following In Vitro Expansion. J. Stem Cells 2004, 22, 675–682. [Google Scholar] [CrossRef]
- Bartholomew, A.; Sturgeon, C.; Siatskas, M.; Ferrer, K.; McIntosh, K.; Patil, S.; Hardy, W.; Devine, S.; Ucker, D.; Deans, R. Mesenchymal Stem Cells Suppress Lymphocyte Proliferation in Vitro and Prolong Skin Graft Survival in Vivo. J. Exp. Hematol. 2002, 30, 42–48. [Google Scholar] [CrossRef]
- Bonab, M.M.; Alimoghaddam, K.; Talebian, F.; Ghaffari, S.H.; Ghavamzadeh, A.; Nikbin, B. Aging of Mesenchymal Stem Cell in Vitro. J. BMC Cell Biol. 2006, 7, 14. [Google Scholar] [CrossRef]
- Nadarajan, S.; Lambert, T.J.; Altendorfer, E.; Gao, J.; Blower, M.D.; Waters, J.C.; Colaiá Covo, M.P. Polo-like Kinase-Dependent Phosphorylation of the Synaptonemal Complex Protein SYP-4 Regulates Double-Strand Break Formation through a Negative Feedback Loop. Elife 2017, 6, e23437. [Google Scholar] [CrossRef]
- Deng, Y.; Zhang, Y.; Ye, L.; Zhang, T.; Cheng, J.; Chen, G.; Zhang, Q.; Yang, Y. Umbilical Cord-Derived Mesenchymal Stem Cells Instruct Monocytes towards an IL10-Producing Phenotype by Secreting IL6 and HGF. J. Sci. Rep. 2016, 6, 37566. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.M.; Sturm, M.J.; Leong, R.W.; Sparrow, M.P.; Segarajasingam, D.; Cummins, A.G.; Phillips, M.; Herrmann, R.P. A Phase 2 Study of Allogeneic Mesenchymal Stromal Cells for Luminal Crohn’s Disease Refractory to Biologic Therapy. J. Clin. Gastroenterol. Hepatol. 2014, 12, 64–71. [Google Scholar] [CrossRef] [PubMed]
- González, M.A.; Gonzalez–Rey, E.; Rico, L.; Büscher, D.; Delgado, M. Adipose-Derived Mesenchymal Stem Cells Alleviate Experimental Colitis by Inhibiting Inflammatory and Autoimmune Responses. J. Gastroenterol. 2009, 136, 978–989. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Yu, X.; Wang, Z.; Wang, F.; Wang, L.; Gao, H.; Chen, Y.; Zhao, W.; Jia, Z.; Yan, S. Long Term Effects of the Implantation of Wharton’s Jelly-Derived Mesenchymal Stem Cells from the Umbilical Cord for Newly-Onset Type 1 Diabetes Mellitus. J. Endocr. J. 2013, 60, 347–357. [Google Scholar] [CrossRef]
- Iba, T.; Umemura, Y.; Wada, H.; Levy, J.H. Roles of Coagulation Abnormalities and Microthrombosis in Sepsis: Pathophysiology, Diagnosis, and Treatment. J. Arch. Med. Res. 2021, 52, 788–797. [Google Scholar] [CrossRef]
- Reinders, M.E.J.; de Fijter, J.W.; Roelofs, H.; Bajema, I.M.; de Vries, D.K.; Schaapherder, A.F.; Claas, F.H.J.; van Miert, P.P.M.C.; Roelen, D.L.; van Kooten, C. Autologous Bone Marrow-Derived Mesenchymal Stromal Cells for the Treatment of Allograft Rejection after Renal Transplantation: Results of a Phase I Study. J. Stem Cells Transl. Med. 2013, 2, 107–111. [Google Scholar] [CrossRef]
- Schellenberg, A.; Lin, Q.; Schüler, H.; Koch, C.M.; Joussen, S.; Denecke, B.; Walenda, G.; Pallua, N.; Suschek, C.V.; Zenke, M. Replicative Senescence of Mesenchymal Stem Cells Causes DNA-Methylation Changes Which Correlate with Repressive Histone Marks. J. Aging 2011, 3, 873. [Google Scholar] [CrossRef]
- Yin, J.Q.; Zhu, J.; Ankrum, J.A. Manufacturing of Primed Mesenchymal Stromal Cells for Therapy. Nat. Biomed. Eng. 2019, 3, 90–104. [Google Scholar] [CrossRef]
- Da Meirelles, L.S.; Chagastelles, P.C.; Nardi, N.B. Mesenchymal Stem Cells Reside in Virtually All Post-Natal Organs and Tissues. J. Cell Sci. 2006, 119, 2204–2213. [Google Scholar] [CrossRef]
- Lin, H.-Y. The Severe COVID-19: A Sepsis Induced by Viral Infection? And Its Immunomodulatory Therapy. J. Chin. J. Traumatol. 2020, 23, 190–195. [Google Scholar] [CrossRef]
- Unar, A.; Imtiaz, M.; Trung, T.T.; Rafiq, M.; Fatmi, M.Q.; Jafar, T.H. Structural and Functional Analyses of SARS-CoV-2 RNA-Dependent RNA Polymerase Protein and Complementary vs. Synthetic Drugs against COVID-19 and the Exploration of Binding Sites for Docking, Molecular Dynamics Simulation, and Density Functional Theory Studies. Curr. Bioinform. 2022, 17, 632–656. [Google Scholar]
- Murao, S.; Yamakawa, K. A Systematic Summary of Systematic Reviews on Anticoagulant Therapy in Sepsis. J. Clin. Med. 2019, 8, 1869. [Google Scholar] [CrossRef]
- Freeman, B.D.; Zehnbauer, B.A.; Buchman, T.G. A Meta-Analysis of Controlled Trials of Anticoagulant Therapies in Patients with Sepsis. Shock 2003, 20, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Umemura, Y.; Yamakawa, K.; Ogura, H.; Yuhara, H.; Fujimi, S. Efficacy and Safety of Anticoagulant Therapy in Three Specific Populations with Sepsis: A Meta-analysis of Randomized Controlled Trials. J. Thromb. Haemost. 2016, 14, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Thachil, J.; Iba, T. The Application of Anticoagulant Therapy to Sepsis. J. Intensive Care 2017, 5, 32. [Google Scholar] [CrossRef]
- van der Poll, T.; Opal, S.M. Should All Septic Patients Be given Systemic Anticoagulation? No. Intensive Care Med. 2017, 43, 455–457. [Google Scholar] [CrossRef]
- Iba, T.; Arakawa, M.; Di Nisio, M.; Gando, S.; Anan, H.; Sato, K.; Ueki, Y.; Levy, J.H.; Thachil, J. Newly Proposed Sepsis-Induced Coagulopathy Precedes International Society on Thrombosis and Haemostasis Overt-Disseminated Intravascular Coagulation and Predicts High Mortality. J. Intensive Care Med. 2020, 35, 643–649. [Google Scholar] [CrossRef]
- Egi, M.; Ogura, H.; Yatabe, T.; Atagi, K.; Inoue, S.; Iba, T.; Kakihana, Y.; Kawasaki, T.; Kushimoto, S.; Kuroda, Y.; et al. The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2020 (J-SSCG 2020). Acute Med. Surg. 2021, 8, 659. [Google Scholar] [CrossRef]
- Yoshimura, J.; Yamakawa, K.; Ogura, H.; Umemura, Y.; Takahashi, H.; Morikawa, M.; Inoue, Y.; Fujimi, S.; Tanaka, H.; Hamasaki, T.; et al. Benefit Profile of Recombinant Human Soluble Thrombomodulin in Sepsis-Induced Disseminated Intravascular Coagulation: A Multicenter Propensity Score Analysis. Crit. Care 2015, 19, 78. [Google Scholar] [CrossRef]
- Carnicelli, A.P.; Hong, H.; Connolly, S.J.; Eikelboom, J.; Giugliano, R.P.; Morrow, D.A.; Patel, M.R.; Wallentin, L.; Alexander, J.H.; Cecilia Bahit, M.; et al. Direct Oral Anticoagulants Versus Warfarin in Patients with Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials with Interaction Testing by Age and Sex. Circulation 2022, 145, 242–255. [Google Scholar] [CrossRef]
- Guo, J.-Y.; Lin, H.-Y. Why Anticoagulant Studies on Sepsis Fail Frequently–––Start with SCARLET. Chin. J. Traumatol. 2023, 26, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.-F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin Alfa (Activated) in Adults with Septic Shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Antoniak, S. The Coagulation System in Host Defense. Res. Pract. Thromb. Haemost. 2018, 2, e12109. [Google Scholar] [CrossRef] [PubMed]
- Amaraneni, A.; Tadi, P.; Rettew, A.C. Anticoagulation Safety. StatPearls 2023. [Google Scholar]
- Kazmi, R.S.; Lwaleed, B.A. New Anticoagulants: How to Deal with Treatment Failure and Bleeding Complications. Br. J. Clin. Pharmacol. 2011, 72, 593–603. [Google Scholar] [CrossRef] [PubMed]
- McIlroy, G.; Smith, N.; Lokare, A.; Beale, K.; Kartsios, C. Treatment Failure in Patients Receiving Direct Oral Anticoagulants: Clinical Management and Outcomes from a Single-Center Review of 59 Consecutive Patients. Blood 2018, 132, 5058. [Google Scholar] [CrossRef]
- Galli, F.; Borghi, L.; Faioni, E.; Cavicchioli, M.; Ferrari Losi, J.; Vegni, E. Failure of the Anticoagulant Therapy and Psychological Distress: Still Far from a Bridge. Front. Psychol. 2018, 9, 1709. [Google Scholar] [CrossRef]
- Iba, T.; Nagaoka, I.; Boulat, M. The Anticoagulant Therapy for Sepsis-Associated Disseminated Intravascular Coagulation. Thromb. Res. 2013, 131, 383–389. [Google Scholar] [CrossRef]
- Schulman, S. How I Treat Recurrent Venous Thromboembolism in Patients Receiving Anticoagulant Therapy. Blood J. Am. Soc. Hematol. 2017, 129, 3285–3293. [Google Scholar] [CrossRef]
- Furugohri, T.; Sugiyama, N.; Morishima, Y.; Shibano, T. Antithrombin-Independent Thrombin Inhibitors, but Not Direct Factor Xa Inhibitors, Enhance Thrombin Generation in Plasma through Inhibition of Thrombin-Thrombomodulin-Protein C System. Thromb. Haemost. 2011, 106, 1076–1083. [Google Scholar]
- Obeagu, E.; Nwosu, D.; Obeagu, G. Antithrombin III: A Review. Int. J. Curr. Res. Biol. Med. 2022, 7, 20–27. [Google Scholar]
- Wu, C.-C.; Lan, H.-M.; Han, S.-T.; Chaou, C.-H.; Yeh, C.-F.; Liu, S.-H.; Li, C.-H.; Blaney, G.N.; Liu, Z.-Y.; Chen, K.-F. Comparison of Diagnostic Accuracy in Sepsis between Presepsin, Procalcitonin, and C-Reactive Protein: A Systematic Review and Meta-Analysis. J. Ann. Intensive Care 2017, 7, 91. [Google Scholar] [CrossRef] [PubMed]
- Kylat, R.I.; Ohlsson, A. Recombinant Human Activated Protein C for Severe Sepsis in Neonates. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Bernard, G.R.; Vincent, J.-L.; Laterre, P.-F.; LaRosa, S.P.; Dhainaut, J.-F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.; Helterbrand, J.D.; Ely, E.W. Efficacy and Safety of Recombinant Human Activated Protein C for Severe Sepsis. N. Engl. J. Med. 2001, 344, 699–709. [Google Scholar] [CrossRef]
- Levi, M. The Coagulant Response in Sepsis. Clin. Chest Med. 2008, 29, 627–642. [Google Scholar] [CrossRef]
- Casserly, B.; Gerlach, H.; Phillips, G.S.; Marshall, J.C.; Lemeshow, S.; Levy, M.M. Evaluating the Use of Recombinant Human Activated Protein C in Adult Severe Sepsis: Results of the Surviving Sepsis Campaign. Crit. Care Med. 2012, 40, 1417–1426. [Google Scholar] [CrossRef]
- Cannegieter, S.C.; Rosendaal, F.R.; Wintzen, A.R.; Van der Meer, F.J.M.; Vandenbroucke, J.P.; Briet, E. Optimal Oral Anticoagulant Therapy in Patients with Mechanical Heart Valves. N. Engl. J. Med. 1995, 333, 11–17. [Google Scholar] [CrossRef]
- Holbrook, A.; Schulman, S.; Witt, D.M.; Vandvik, P.O.; Fish, J.; Kovacs, M.J.; Svensson, P.J.; Veenstra, D.L.; Crowther, M.; Guyatt, G.H. Evidence-Based Management of Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e152S–e184S. [Google Scholar] [CrossRef]
- Yokoyama, N.; Takaki, S.; Yokose, M.; Kuwabara, K.; Anzai, A.; Hamada, T.; Kashiwagi, S.; Okamura, K.; Sugawara, Y.; Goto, T. A Question Is “What Are the Optimal Targets for Anticoagulant Therapies?”. J. Intensive Care 2020, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Target-Specific Oral Anticoagulants. Available online: https://www.uspharmacist.com/article/targetspecific-oral-anticoagulants (accessed on 8 September 2023).
- Anticoagulant Drugs: Uses, Types, and Side Effects. Available online: https://www.medicalnewstoday.com/articles/anticoagulant-drugs#how-they-work (accessed on 8 September 2023).
- Umerah Co, Momodu II. Anticoagulation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560651/ (accessed on 17 July 2023).
- Anticoagulants (Blood Thinners): What They Do, Types and Side Effects. Available online: https://my.clevelandclinic.org/health/treatments/22288-anticoagulants (accessed on 8 September 2023).
- Anticoagulant Medicines—NHS. Available online: https://www.nhs.uk/conditions/anticoagulants/ (accessed on 8 September 2023).
- Varadarajan, P. Anticoagulation. Cardiol. Board. Rev. 2023, 615–626. [Google Scholar] [CrossRef]
- Costello, R.A.; Nehring, S.M. Disseminated Intravascular Coagulation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441834/ (accessed on 20 January 2023).
- Faix, J.D. Biomarkers of Sepsis. Crit. Rev. Clin. Lab. Sci. 2013, 50, 23. [Google Scholar] [CrossRef] [PubMed]
- Teggert, A.; Datta, H.; Ali, Z. Biomarkers for Point-of-Care Diagnosis of Sepsis. Micromachines 2020, 11, 286. [Google Scholar] [CrossRef] [PubMed]
- Biron, B.M.; Ayala, A.; Lomas-Neira, J.L. Biomarkers for Sepsis: What Is and What Might Be? Biomark. Insights 2015, 10, 7. [Google Scholar] [CrossRef]
- Levi, M. Pathogenesis and Diagnosis of Disseminated Intravascular Coagulation. Int. J. Lab. Hematol. 2018, 40, 15–20. [Google Scholar] [CrossRef]
- Barichello, T.; Generoso, J.S.; Singer, M.; Dal-Pizzol, F. Biomarkers for Sepsis: More than Just Fever and Leukocytosis—A Narrative Review. Crit. Care 2022, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to Use Biomarkers of Infection or Sepsis at the Bedside: Guide to Clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef]
- Sardesai, A.U.; Tanak, A.S.; Krishnan, S.; Striegel, D.A.; Schully, K.L.; Clark, D.V.; Muthukumar, S.; Prasad, S. An Approach to Rapidly Assess Sepsis through Multi-Biomarker Host Response Using Machine Learning Algorithm. Sci. Rep. 2021, 11, 16905. [Google Scholar] [CrossRef]
- Komorowski, M.; Green, A.; Tatham, K.C.; Seymour, C.; Antcliffe, D. Sepsis Biomarkers and Diagnostic Tools with a Focus on Machine Learning. EBioMedicine 2022, 86, 104394. [Google Scholar] [CrossRef]
- Taneja, I.; Damhorst, G.L.; Lopez-Espina, C.; Zhao, S.D.; Zhu, R.; Khan, S.; White, K.; Kumar, J.; Vincent, A.; Yeh, L.; et al. Diagnostic and Prognostic Capabilities of a Biomarker and EMR-Based Machine Learning Algorithm for Sepsis. Clin. Transl. Sci. 2021, 14, 1578–1589. [Google Scholar] [CrossRef]
- Parkinson, E.; Liberatore, F.; Watkins, W.J.; Andrews, R.; Edkins, S.; Hibbert, J.; Strunk, T.; Currie, A.; Ghazal, P. Gene Filtering Strategies for Machine Learning Guided Biomarker Discovery Using Neonatal Sepsis RNA-Seq Data. Front. Genet. 2023, 14, 1158352. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Previous Sepsis Definitions (SIRS-Based) | Sepsis 3 Definition |
|---|---|---|
| Definition | Sepsis is SIRS + confirmed or presumed infections * | Sepsis is life-threatening organ dysfunction due to a dysregulated host response to infection |
| Organ Dysfunction Criteria | Based on individual clinical criteria (e.g., temperature, heart rate, respiratory rate, WBC count) | Organ dysfunction defined as an increase of 2 or more points in the Sequential Organ Failure Assessment (SOFA) score |
| Clinical Criteria | Relatively simple criteria (e.g., T > 38 C or <36 C, p > 90/min, RR > 20/min or PaCO2 < 32 mmHg, WBC > 12 or >10% immature band forms) | qSOFA (HAT) **: Hypotension (SBP ≤ 100 mmHg), Altered mental status (any GCS < 15), Tachypnea (RR ≥ 22) |
| Classification of Severity | Sepsis, Severe Sepsis, Septic Shock | Sepsis, Septic Shock (Severe Sepsis no longer exists) |
| Diagnostic Accuracy | Lack of sensitivity and specificity for diagnosing severe sepsis | Improved predictive validity and accuracy in diagnosing sepsis |
| Use in ICU Patients | SIRS criteria lacked sensitivity for defining sepsis in ICU patients | SOFA score superior to SIRS in predicting mortality in ICU patients |
| Use in Non-ICU Patients | Less accurate in predicting hospital mortality outside the ICU | Similar predictive performance in non-ICU patients |
| Global Applicability | Used globally, but lacks standardization and content validity | Development and validation conducted in high-income countries |
| Prognostic Value | Limited ability to predict patient outcomes and mortality | Enhanced ability to prognosticate patient outcomes and mortality risk |
| Emphasis on Infection Trigger | Inclusion of infection as a crucial component in sepsis diagnosis | Maintains the importance of infection in defining sepsis |
| Endorsement by Professional Orgs. | Various organizations endorsed previous definitions | Not universally endorsed by all organizations |
| Parameter (Units) | Diagnostic Method | Low-Risk Criteria (Score = 1) | Moderate-Risk Criteria (Score = 2) | High-Risk Criteria (Score = 3) | Interpretative Notes |
| Platelet Count (×10⁹ per L) | ISTH Overt DIC | 50–100 | N/A | <80 or 50% drop in 24 h 1 | Lower counts indicate severe clotting issues |
| JAAM DIC | <50 | N/A | N/A | - | |
| ISTH SIC | 100–150 | <100 | N/A | - | |
| Fibrin Degradation Products (FDP)/D-dimer (μg/mL) | ISTH Overt DIC | N/A | Moderate increase 2 | Strong increase 3 | Elevated levels suggest severe clotting issues |
| JAAM DIC | 10–25 | N/A | ≥25 | - | |
| ISTH SIC | N/A | N/A | N/A | - | |
| Prothrombin Time (PT) (seconds or PT-INR) | ISTH Overt DIC | 1.2–1.4 PT-INR | 3–6 s | ≥6 s | Longer times signify clotting dysfunction |
| JAAM DIC | 1.2–1.4 PT-INR | N/A | >1.4 PT-INR | - | |
| ISTH SIC | N/A | N/A | N/A | - | |
| Fibrinogen Levels (g/mL) | ISTH Overt DIC | N/A | N/A | <100 | Low levels indicate severe coagulation issues |
| JAAM DIC | N/A | N/A | N/A | - | |
| ISTH SIC | N/A | N/A | N/A | - | |
| SIRS Score | ISTH Overt DIC | N/A | N/A | N/A | - |
| JAAM DIC | >3 | N/A | N/A | Elevated scores indicate systemic inflammation | |
| ISTH SIC | N/A | N/A | N/A | - | |
| SOFA Score | ISTH Overt DIC | N/A | N/A | N/A | - |
| JAAM DIC | 1 | N/A | N/A | Score assesses multi-organ dysfunction | |
| ISTH SIC | 1 | ≥2 | N/A | - |
| Therapy | Mechanism of Action | Dosage and Administration | Efficacy | Adverse Effects | References |
|---|---|---|---|---|---|
| Unfractionated Heparin (UFH) | Anticoagulant | Dosage: Based on weight, typically 80 units/kg bolus followed by 18 units/kg/hr infusion | Limited high-quality evidence for use in sepsis-related DIC. Small trials show potential benefits in early-stage sepsis patients but not necessarily in sepsis DIC patients | Bleeding risk | [19,39,40,41] |
| Recombinant Soluble TM (rsTM) | Alleviates DIC and reduces mortality | Dosage: Varies, typically administered intravenously | More effective than UFH in alleviating DIC and reducing mortality in infectious DIC patients | NS * | [39,40,41,42,43] |
| Activated Protein C (APC) | Anticoagulant and anti-inflammatory agent; degrades extracellular histones | Dosage: Varies, typically administered intravenously | No significant difference in response rates compared to UFH for DIC; reduces bleeding risk and mortality | Bleeding risk | [44,45,46,47,48,49] |
| High-dose Antithrombin (AT) | Reduces mortality in DIC patients without significant bleeding events | Dosage: Varies, typically administered intravenously | No reduction in mortality in sepsis patients; increases bleeding risk | Increased bleeding risk | [44,45,49,50] |
| Corticosteroids | Unclear mechanism; potential benefits in sepsis-induced DIC | Dosage: Varies depending on the specific corticosteroid used and patient condition | Contrasting findings, inconclusive evidence. Some studies suggest potential benefits, while others show no significant impact or potential harm | Potential adverse effects: increased risk of infection, metabolic disturbances | [32,33,34,35,36,38,51] |
| Thrombomodulin alfa (rTM) | Binds to thrombin, activates protein C, downregulates coagulation | Dosage: Varies, typically administered intravenously | Reduction in overall mortality rates, minimized bleeding complications | NS * | [8,52,53] |
| Vitamin C | Potential antioxidant, anti-inflammatory, and anticoagulant properties | Dosage: Varies, typically administered intravenously | Inconclusive evidence. Some studies show potential benefits in certain parameters, while others show no significant impact or potential harm | NS * | [54,55,56,57,58,59,60,61] |
| Fibrinolytic Therapy | Reduces clot formation, improves organ perfusion | Dosage: Varies depending on the specific fibrinolytic agent used | Impact on clinical outcomes inconclusive; some studies show improvements in coagulation parameters, while others show no significant effect | Bleeding risk | [62,63,64,65,66,67] |
| Platelet Transfusion | Controversial; potential benefits in severe thrombocytopenia or active bleeding | Dosage: Varies depending on the patient’s platelet count and clinical condition | Evidence supporting efficacy is sparse; conflicting recommendations | Potential adverse effects: bleeding complications | [68,69,70,71,72,73] |
| Granulocyte Colony-Stimulating Factor (G-CSF) | Stimulates production and mobilization of neutrophils | Dosage: Varies, typically administered subcutaneously or intravenously | Potential benefits in improving coagulation parameters | NS * | [74,75,76,77] |
| Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF) | Acts on neutrophils and monocytes/macrophages | Dosage: Varies, typically administered subcutaneously or intravenously | Impact on sepsis-induced DIC not yet clearly defined | NS | [74,75] |
| Interferon-gamma (IFN-γ) | Improves coagulation abnormalities, shows a trend toward decreased mortality in sepsis-induced coagulopathy patients | Dosage: Varies, typically administered intravenously | Improved coagulation abnormalities, reduced DIC duration, potential decrease in mortality | NS | [53] |
| Mesenchymal Stem Cells (MSCs) | Immunomodulatory effects through cytokine secretion | Dosage: Varies, typically administered intravenously | Promising results in preclinical studies, potential to improve outcomes in sepsis-induced DIC | NS * | [78,79,80,81,82,83,84,85,86,87] |
| Aspect | PROWESS Trial | KyberSept Trial | OPTIMIST Trial | SSCG 2021 Guidelines | Should We Target Coagulation Abnormalities? |
|---|---|---|---|---|---|
| Primary Object | Evaluate activated protein C (drotrecogin alfa) for severe sepsis | Assess high-dose antithrombin therapy in severe sepsis | Study tifacogin, a recombinant tissue factor pathway inhibitor, in sepsis | Update clinical guidelines for sepsis and septic shock | N/A |
| Key Findings | No long-term benefit; risk of bleeding | No benefit; potential interaction with other anticoagulants like heparin | No benefit; complexity of sepsis noted | Eliminated pharmaceutical recommendations and omitted the term “DIC” | Subject of ongoing debate |
| Reasons for Failure | Risk-benefit profile questioned due to bleeding risks | Possible interaction with other anticoagulants like heparin | Sepsis too complex for single-target therapy | N/A | Complexity and heterogeneity of sepsis |
| Scientific Implications | Raised questions about the role of anticoagulants in sepsis treatment | Highlighted the need to understand the interaction between anticoagulants | Called for a broader understanding of sepsis beyond coagulation abnormalities | Indicates shift in understanding of sepsis and coagulopathy | Raised questions about the feasibility of targeting coagulation abnormalities |
| Considerations for Future Research | Need for trials with better risk stratification | Exploration of combination therapies | Need for multi-targeted approaches | N/A | Requires a more nuanced approach considering the multifaceted nature of sepsis |
| Study Name & Reference ID | Investigational Agent & Target Patient Population | Study Design & Participant Count | Classification of Bleeding Adverse Events | Incidence in Intervention Arm (%) | Incidence in Control Arm (%) | Statistical Significance | Remarks | Ref. |
|---|---|---|---|---|---|---|---|---|
| PROWESS | Recombinant Activated Protein C (rAPC); Patients with Severe Sepsis | Randomized Controlled Trial (RCT); N = 1690 | Any Type/Major | Any: 12.5%, Major: 3.5% | Any: 12.1%, Major: 2.0% | Any: p = 0.84, Major: p = 0.06 | Treatment and control groups are similar in bleeding rates | [144,150] |
| PROWESS-SHOCK | rAPC; Patients with Severe Sepsis and Shock | RCT; N = 1666 | Any Type/Major | Any: 8.6%, Major: 1.2% | Any: 4.8%, Major: 1.0% | Any: p = 0.002, Major: p = 0.81 | Significant increase in any type of bleeding; no significant difference in major bleeding. | [29,144] |
| KyberSept | High-dose Antithrombin; Patients with Severe Sepsis | RCT; N = 2314 | Any Type/Major | Any: 22.0%, Major: 10.0% | Any: 12.8%, Major: 5.7% | RR: 1.71 (95% CI: 1.42–2.06), Major: RR: 1.75 (95% CI: 1.32–2.33) | Significantly higher bleeding risk associated with antithrombin; caution advised. | [49,144] |
| Iba et al. | Supplemental-dose Antithrombin; Patients with Septic DIC | Non-Randomized Phase-4 Trial; N = 729 | Any Type/Major | Any: 6.52%, Major: 1.71% | N/A | N/A | Control group absent; no comparative statistical analysis possible. | [144,151] |
| Online Data | Recombinant Thrombomodulin (rTM); Patients with Severe Sepsis | Phase-2B Trial; N = 741 | Major | Major: 6.7% | Major: 6.2% | Not Reported | Lack of significant statistical evaluation on bleeding. | [144,152] |
| Post-marketing Survey | Recombinant Thrombomodulin (rTM); Patients with Septic DIC | Phase-4 Trial; N = 2516 | Any Type | Any: 5.4% | N/A | N/A | Survey study; No control group for comparison. Possible. | [144,152] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unar, A.; Bertolino, L.; Patauner, F.; Gallo, R.; Durante-Mangoni, E. Decoding Sepsis-Induced Disseminated Intravascular Coagulation: A Comprehensive Review of Existing and Emerging Therapies. J. Clin. Med. 2023, 12, 6128. https://doi.org/10.3390/jcm12196128
Unar A, Bertolino L, Patauner F, Gallo R, Durante-Mangoni E. Decoding Sepsis-Induced Disseminated Intravascular Coagulation: A Comprehensive Review of Existing and Emerging Therapies. Journal of Clinical Medicine. 2023; 12(19):6128. https://doi.org/10.3390/jcm12196128
Chicago/Turabian StyleUnar, Ahsanullah, Lorenzo Bertolino, Fabian Patauner, Raffaella Gallo, and Emanuele Durante-Mangoni. 2023. "Decoding Sepsis-Induced Disseminated Intravascular Coagulation: A Comprehensive Review of Existing and Emerging Therapies" Journal of Clinical Medicine 12, no. 19: 6128. https://doi.org/10.3390/jcm12196128