
Peripheral Blood Mononuclear Cells: A New Frontier in the Management of Patients with Diabetes and No-Option Critical Limb Ischaemia
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Features
2.2. Wound Assessment
2.3. The Wound Angiosome Concept
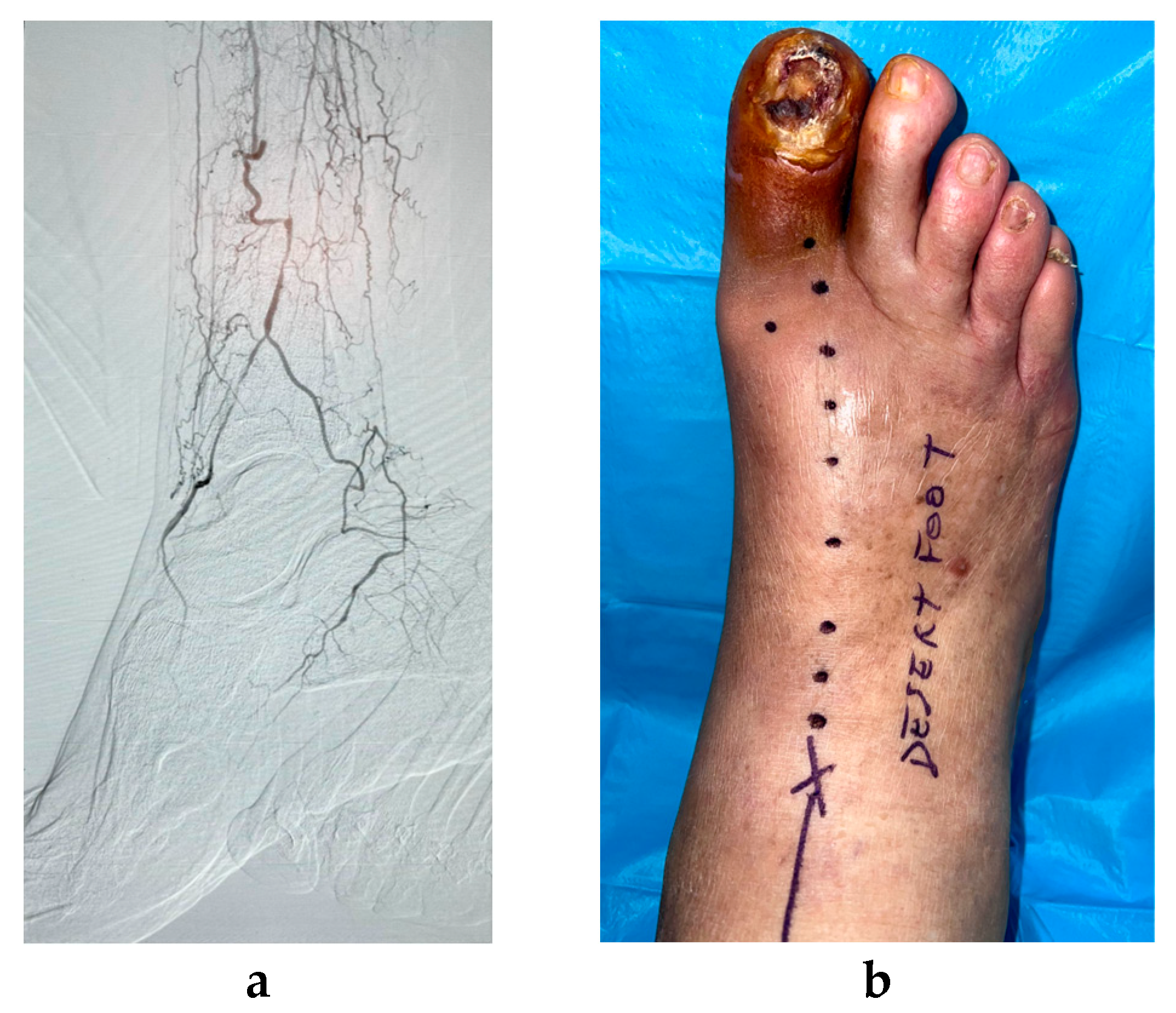
2.4. Description of the Cell Therapy Procedure
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meloni, M.; Izzo, V.; Giurato, L.; Lázaro-Martínez, J.L.; Uccioli, L. Prevalence, Clinical Aspects and Outcomes in a Large Cohort of Persons with Diabetic Foot Disease: Comparison between Neuropathic and Ischemic Ulcers. J. Clin. Med. 2020, 9, 1780. [Google Scholar] [CrossRef] [PubMed]
- Prompers, L.; Schaper, N.; Apelqvist, J.; Edmonds, M.; Jude, E.; Mauricio, D.; Uccioli, L.; Urbancic, V.; Bakker, K.; Holstein, P.; et al. Prediction of outcome in individuals with diabetic foot ulcers: Focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia 2008, 51, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Carinci, F.; Uccioli, L.; Massi Benedetti, M.; Klazinga, N.S. An in-depth assessment of diabetes-related lower extremity amputation rates 2000–2013 delivered by twenty-one countries for the data collection 2015 of the Organization for Economic Cooperation and Development (OECD). Acta Diabetol. 2020, 57, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Meloni, M.; Izzo, V.; Da Ros, V.; Morosetti, D.; Stefanini, M.; Brocco, E.; Giurato, L.; Gandini, R.; Uccioli, L. Characteristics and Outcome for Persons with Diabetic Foot Ulcer and No-Option Critical Limb Ischemia. J. Clin. Med. 2020, 9, 3745. [Google Scholar] [CrossRef]
- Ferraresi, R.; Mauri, G.; Losurdo, F.; Troisi, N.; Brancaccio, D.; Caravaggi, C.; Neri, L. BAD transmission and SAD distribution: A new scenario for critical limb ischemia. J. Cardiovasc. Surg. 2018, 59, 655–664. [Google Scholar] [CrossRef]
- Ferraresi, R.; Ucci, A.; Pizzuto, A.; Losurdo, F.; Caminiti, M.; Minnella, D.; Casini, A.; Clerici, G.; Montero-Baker, M.; Mills, J. A Novel Scoring System for Small Artery Disease and Medial Arterial Calcification Is Strongly Associated with Major Adverse Limb Events in Patients with Chronic Limb-Threatening Ischemia. J. Endovasc. Ther. 2021, 28, 194–207. [Google Scholar] [CrossRef]
- Meloni, M.; Morosetti, D.; Giurato, L.; Stefanini, M.; Loreni, G.; Doddi, M.; Panunzi, A.; Bellia, A.; Gandini, R.; Brocco, E.; et al. Foot Revascularization Avoids Major Amputation in Persons with Diabetes and Ischaemic Foot Ulcers. J. Clin. Med. 2021, 10, 3977. [Google Scholar] [CrossRef]
- Dubský, M.; Jirkovská, A.; Bem, R.; Fejfarová, V.; Pagacová, L.; Nemcová, A.; Sixta, B.; Chlupac, J.; Peregrin, J.H.; Syková, E.; et al. Comparison of the effect of stem cell therapy and percutaneous transluminal angioplasty on diabetic foot disease in patients with critical limb ischemia. Cytotherapy 2014, 16, 1733–1738. [Google Scholar] [CrossRef]
- Dubský, M.; Jirkovská, A.; Bem, R.; Nemcová, A.; Fejfarová, V.; Jude, E.B. Cell therapy of critical limb ischemia in diabetic patients—State of art. Diabetes Res. Clin. Pract. 2017, 126, 263–271. [Google Scholar] [CrossRef]
- Armstrong, D.G. The University of Texas Diabetic Foot Classification System. Ostomy Wound Manag. 1996, 42, 60–61. [Google Scholar]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 2007, 45 (Suppl. S), S5–S67. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A.; IWGDF Editorial Board. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1). [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Senneville, É.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1). [Google Scholar] [CrossRef]
- Taylor, G.I.; Palmer, J.H. The vascular territories (angiosomes) of the body: Experimental study and clinical applications. Br. J. Plast. Surg. 1987, 40, 113–141. [Google Scholar] [CrossRef]
- Attinger, C.E.; Evans, K.K.; Bulan, E.; Blume, P.; Cooper, P. Angiosomes of the foot and ankle and clinical implications for limb salvage: Reconstruction, incisions, and revascularization. Plast. Reconstr. Surg. 2006, 117 (Suppl. S7), 261S–293S. [Google Scholar] [CrossRef]
- Biancari, F.; Juvonen, T. Angiosome-targeted lower limb revascularization for ischemic foot wounds: Systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 517–522. [Google Scholar] [CrossRef]
- Alexandrescu, V.; Hubermont, G. Primary infragenicular angioplasty for diabetic neuroischemic foot ulcers following the angiosome distribution: A new paradigm for the vascular interventionist? Diabetes Metab. Syndr. Obes. 2011, 4, 327–336. [Google Scholar] [CrossRef]
- Clemens, M.W.; Attinger, C.E. Angiosomes and wound care in the diabetic foot. Foot Ankle Clin. 2010, 15, 439–464. [Google Scholar] [CrossRef]
- Alexandrescu, V.A.; Hubermont, G.; Philips, Y.; Guillaumie, B.; Ngongang, C.; Vandenbossche, P.; Azdad, K.; Ledent, G.; Horion, J. Selective primary angioplasty following an angiosome model of reperfusion in the treatment of Wagner 1-4 diabetic foot lesions: Practice in a multidisciplinary diabetic limb service. J. Endovasc. Ther. 2008, 15, 580–593. [Google Scholar] [CrossRef]
- Spaltro, G.; Straino, S.; Gambini, E.; Bassetti, B.; Persico, L.; Zoli, S.; Zanobini, M.; Capogrossi, M.C.; Spirito, R.; Quarti, C.; et al. Characterization of the Pall Celeris system as a point-of-care device for therapeutic angiogenesis. Cytotherapy 2015, 17, 1302–1313. [Google Scholar] [CrossRef] [PubMed]
- Scatena, A.; Petruzzi, P.; Maioli, F.; Lucaroni, F.; Ambrosone, C.; Ventoruzzo, G.; Liistro, F.; Tacconi, D.; Di Filippi, M.; Attempati, N.; et al. Autologous Peripheral Blood Mononuclear Cells for Limb Salvage in Diabetic Foot Patients with No-Option Critical Limb Ischemia. J. Clin. Med. 2021, 10, 2213. [Google Scholar] [CrossRef] [PubMed]
- Panunzi, A.; Madotto, F.; Sangalli, E.; Riccio, F.; Sganzaroli, A.B.; Galenda, P.; Bertulessi, A.; Barmina, M.F.; Ludovico, O.; Fortunato, O.; et al. Results of a prospective observational study of autologous peripheral blood mononuclear cell therapy for no-option critical limb-threatening ischemia and severe diabetic foot ulcers. Cardiovasc. Diabetol. 2022, 21, 196. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Demirdal, T.; Emir, B. Meta-analysis of risk factors for amputation in diabetic foot infections. Diabetes Metab. Res. Rev. 2019, 35, e3165. [Google Scholar] [CrossRef]
- Ndip, A.; Lavery, L.A.; Boulton, A.J. Diabetic foot disease in people with advanced nephropathy and those on renal dialysis. Curr. Diabetes Rep. 2010, 10, 283–290. [Google Scholar] [CrossRef]
- Apelqvist, J.; Elgzyri, T.; Larsson, J.; Löndahl, M.; Nyberg, P.; Thörne, J. Factors related to outcome of neuroischemic/ischemic foot ulcer in diabetic patients. J. Vasc. Surg. 2011, 53, 1582–1588. [Google Scholar] [CrossRef]
- Dubský, M.; Husáková, J.; Bem, R.; Jirkovská, A.; Němcová, A.; Fejfarová, V.; Sutoris, K.; Kahle, M.; Jude, E.B. Comparison of the impact of autologous cell therapy and conservative standard treatment on tissue oxygen supply and course of the diabetic foot in patients with chronic limb-threatening ischemia: A randomized controlled trial. Front. Endocrinol. 2022, 13, 888809. [Google Scholar] [CrossRef]
- Besnier, M.; Gasparino, S.; Vono, R.; Sangalli, E.; Facoetti, A.; Bollati, V.; Cantone, L.; Zaccagnini, G.; Maimone, B.; Fuschi, P.; et al. miR-210 enhances the therapeutic potential of bone-marrow-derived circulating proangiogenic cells in the setting of limb ischemia. Mol. Ther. 2018, 26, 1694–1705. [Google Scholar] [CrossRef]
- Mathiyalagan, P.; Liang, Y.; Kim, D.; Misener, S.; Thorne, T.; Kamide, C.E.; Klyachko, E.; Losordo, D.W.; Hajjar, R.J.; Sahoo, S. Angiogenic mechanisms of human CD34(+) stem cell exosomes in the repair of ischemic hindlimb. Circ. Res. 2017, 120, 1466–1476. [Google Scholar] [CrossRef]
- Gu, Y.; Rampin, A.; Alvino, V.V.; Spinetti, G.; Madeddu, P. Cell therapy for critical limb ischemia: Advantages, limitations, and new perspectives for treatment of patients with critical diabetic vasculopathy. Curr. Diabetes Rep. 2021, 21, 11. [Google Scholar] [CrossRef]
- Rigato, M.; Monami, M.; Fadini, G.P. Autologous Cell Therapy for Peripheral Arterial Disease: Systematic Review and Meta-Analysis of Randomized, Nonrandomized, and Noncontrolled Studies. Circ. Res. 2017, 120, 1326–1340. [Google Scholar] [CrossRef] [PubMed]
- Jetten, N.; Roumans, N.; Gijbels, M.J.; Romano, A.; Post, M.J.; de Winther, M.P.J.; Van Der Hulst, R.R.W.J.; Xanthoulea, S. Wound Administration of M2-Polarized Macrophages Does Not Improve Murine Cutaneous Healing Responses. PLoS ONE 2014, 9, e102994. [Google Scholar] [CrossRef] [PubMed]
- Jetten, N.; Verbruggen, S.; Gijbels, M.J.; Post, M.J.; De Winther, M.P.J.; Donners, M.M.P.C. Anti-inflammatory M2, but not pro-inflammatory M1 macrophages promote angiogenesis in vivo. Angiogenesis 2014, 17, 109–118. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria |
|
| Exclusion criteria |
|
| Foot Angiosome and Anatomical Vascular Site of Cell Injection | Wound Location |
|---|---|
| Posterior tibial artery |
|
| |
| Anterior tibial artery |
|
| |
| Peroneal artery |
|
|
| Variable | Value |
|---|---|
| Age (years) | 74.8 ± 5.8 |
| Sex (male) n (%) | 39/55 (70.9) |
| Diabetes (type 2) n (%) | 51/55 (92.7) |
| Diabetes duration (years) | 22.1 ± 7.7 |
| HbA1c mmol/mol (%) | 58 ± 9 (7.4 ± 3) |
| Dyslipidaemia n (%) | 29 (52.7) |
| Hypertension n (%) | 53 (96.3) |
| ESRD n (%) | 4 (7.3) |
| IHD n (%) | 47 (85.4) |
| Heart failure n (%) | 5 (9.1) |
| CVD n (%) | 21 (38.2) |
| Smoke | 4 (7.3) |
| Hb (gr/dL) | 12.1 ± 1.2 |
| Ulcer size (>5 cm2) n (%) | 41 (74.5) |
| Depth (bone involvement) | 36 (65.4%) |
| Infection n (%) | 45 (81.8) |
| Osteomyelitis n (%) | 28 (50.9) |
| Gangrene n (%) | 49 (89.1) |
| Heel location n (%) | 13 (23.6) |
| Texas University Classification | |
| 2 (3.6%) 1 (1.8%) 8 (14.5%) 1 (1.8%) 15 (27.3) 28 (50.9) |
| Primary Outcomes | Value |
|---|---|
| Healed and survived n (%) | 38 (69.1) |
| Healed and deceased n (%) | 2 (3.6) |
| Not healed and deceased n (%) | 6 (10.9) |
| Not healed and amputated n (%) | 9 (16.4) |
| Secondary Outcomes | Before PB-MNC | After PB-MNC | p-Value |
|---|---|---|---|
| TcPO2 (mmHg) | 17 ± 11 | 41 ± 12 | <0.0001 |
| Pain (NRS) | 6.8 ± 1.7 | 2.8 ± 1.7 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meloni, M.; Giurato, L.; Andreadi, A.; Bellizzi, E.; Bellia, A.; Lauro, D.; Uccioli, L. Peripheral Blood Mononuclear Cells: A New Frontier in the Management of Patients with Diabetes and No-Option Critical Limb Ischaemia. J. Clin. Med. 2023, 12, 6123. https://doi.org/10.3390/jcm12196123
Meloni M, Giurato L, Andreadi A, Bellizzi E, Bellia A, Lauro D, Uccioli L. Peripheral Blood Mononuclear Cells: A New Frontier in the Management of Patients with Diabetes and No-Option Critical Limb Ischaemia. Journal of Clinical Medicine. 2023; 12(19):6123. https://doi.org/10.3390/jcm12196123
Chicago/Turabian StyleMeloni, Marco, Laura Giurato, Aikaterini Andreadi, Ermanno Bellizzi, Alfonso Bellia, Davide Lauro, and Luigi Uccioli. 2023. "Peripheral Blood Mononuclear Cells: A New Frontier in the Management of Patients with Diabetes and No-Option Critical Limb Ischaemia" Journal of Clinical Medicine 12, no. 19: 6123. https://doi.org/10.3390/jcm12196123