
Cardiovascular Disease and Stroke in Immune TTP–Challenges and Opportunities

Abstract
:1. Introduction
2. Cardiovascular Involvement in Acute iTTP
3. Cardiovascular Disease Burden in Chronic iTTP
3.1. Cardiovascular Disease Contributes to Shortened Survival in iTTP Survivors
3.2. Epidemiology of Stroke and Myocardial Infarction in iTTP Survivors
3.3. Silent Cerebral Infarction in iTTP Survivors and Impact on Functional Outcomes
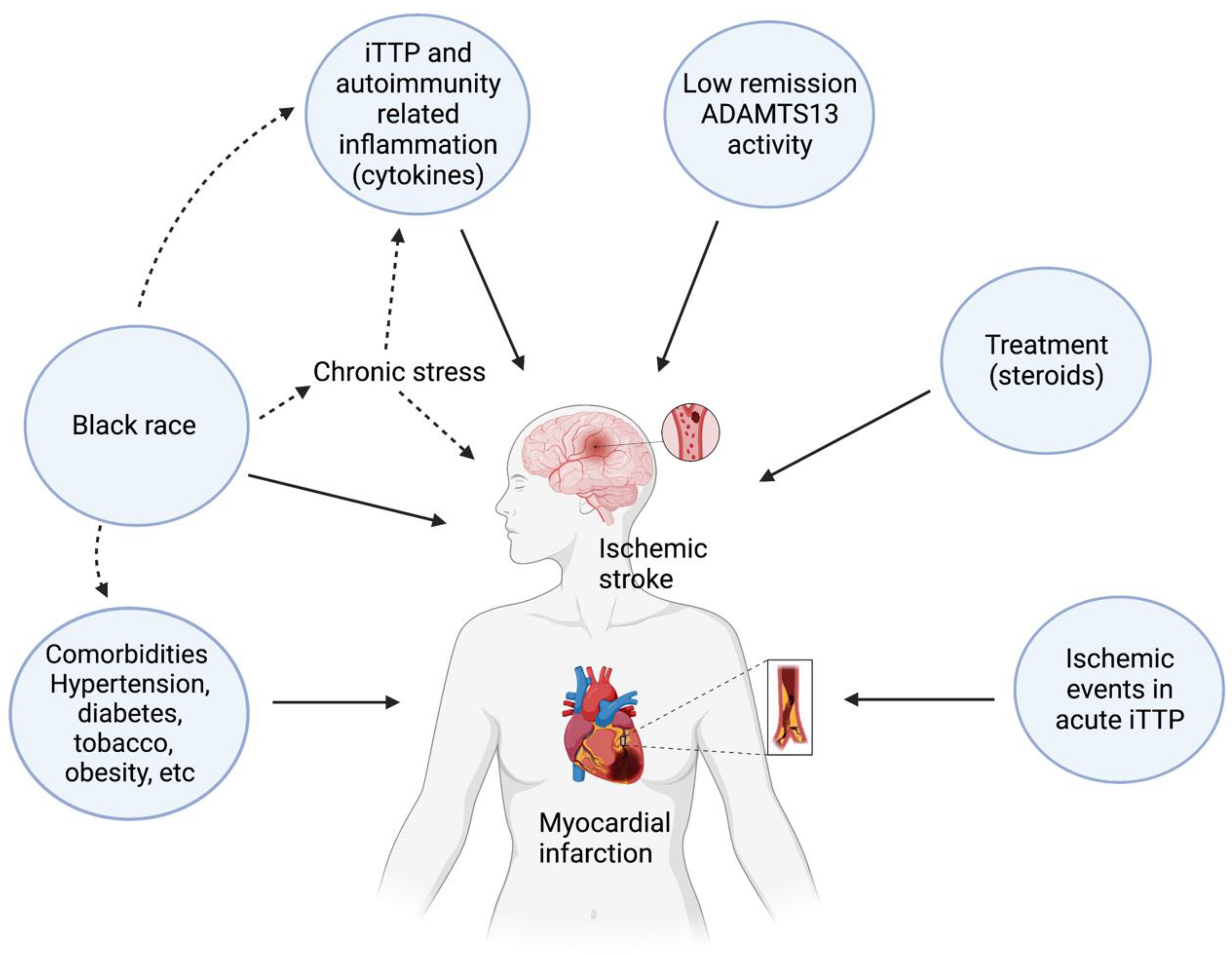
3.4. Factors Contributing to Risk of CV Disease in iTTP
3.5. Future Directions—Opportunities to Improve Cardiovascular and Neurologic Outcomes

{kind=link}
| Study | Site (s) | N | Female Sex | Race | Median Age (Years) | Median Follow-Up | Cardiovascular Outcomes |
|---|---|---|---|---|---|---|---|
| Deford 2013 [6] | Oklahoma Registry | 57 | 79% | White: 63% Black: 37% | 39 (range 9–71) | 7.8 years | 19% mortality |
| Upreti 2019 [15] | Johns Hopkins Registry | 137 | 67.9% | White: 38% Black: 62% | 48.8 (IQR 35.3, 60.3) | 3.08 years | Stroke during remission in 13.1% |
| Brodsky 2021 [14] | Ohio State University and Johns Hopkins Registries | 181 | 71.3% | White: 45.9% Black: 53% Other: 1.1% | 39 (IQR 27–51) | 7.6 years | 23.7% MACE rate in clinical remission. |
| Sukumar 2022 [12] | Ohio State University and Johns Hopkins Registries | 222 | 70.3% | White: 46.8% Black: 50.5% Other: 2.7% | 42 (IQR 29–55) | 4.5 years | Mortality 222.8 per 100 patient-years (1.8 times higher than age and sex-matched control cohort). Cardiovascular disease and iTTP relapse (27.6% each) were leading causes of death. |
| Chaturvedi 2023 [35] | Neurologic Sequelae of iTTP (NeST) Study, Johns Hopkins | 36 | 64.3% | White: 14.3% Black: 66.7% Other: 4.8% | 48 (IQR 34–56) | 5.5 (IQR 1.5–9.3) | 50% had silent cerebral infarction on brain MRI |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moschcowitz, E. An acute febrile pleiochromic anemia with hyaline thrombosis of the terminal arterioles and capillaries: An undescribed disease. 1925. Mt. Sinai J. Med. 2003, 70, 352–355. [Google Scholar] [PubMed]
- Joly, B.S.; Coppo, P.; Veyradier, A. Thrombotic thrombocytopenic purpura. Blood 2017, 129, 2836–2846. [Google Scholar] [CrossRef] [PubMed]
- Bell, W.R.; Braine, H.G.; Ness, P.M.; Kickler, T.S. Improved survival in thrombotic thrombocytopenic purpura–hemolytic uremic syndrome. Clinical experience in 108 patients. N. Engl. J. Med. 1991, 325, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Rock, G.A.; Shumak, K.H.; Buskard, N.A.; Blanchette, V.S.; Kelton, J.G.; Nair, R.C.; Spasoff, R.A.; Canadian Apheresis Study Group. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N. Engl. J. Med. 1991, 325, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Abbas, H.; McCrae, K.R. Increased morbidity during long-term follow-up of survivors of thrombotic thrombocytopenic purpura. Am. J. Hematol. 2015, 90, E208. [Google Scholar] [CrossRef] [PubMed]
- Deford, C.C.; Reese, J.A.; Schwartz, L.H.; Perdue, J.J.; Hovinga, J.A.K.; Lämmle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Multiple major morbidities and increased mortality during long-term follow-up after recovery from thrombotic thrombocytopenic purpura. Blood 2013, 122, 2023–2029, quiz 2142. [Google Scholar] [CrossRef] [PubMed]
- Page, E.E.; Hovinga, J.A.K.; Terrell, D.R.; Vesely, S.K.; George, J.N. Thrombotic thrombocytopenic purpura: Diagnostic criteria, clinical features, and long-term outcomes from 1995 through 2015. Blood Adv. 2017, 1, 590–600. [Google Scholar] [CrossRef]
- Selvakumar, S.; Liu, A.; Chaturvedi, S. Immune thrombotic thrombocytopenic purpura: Spotlight on long-term outcomes and survivorship. Front. Med. 2023, 10, 1137019. [Google Scholar] [CrossRef]
- Nichols, L.; Berg, A.; Rollins-Raval, M.A.; Raval, J.S. Cardiac injury is a common postmortem finding in thrombotic thrombocytopenic purpura patients: Is empiric cardiac monitoring and protection needed? Ther. Apher. Dial. 2015, 19, 87–92. [Google Scholar] [CrossRef]
- Wiernek, S.L.; Jiang, B.; Gustafson, G.M.; Dai, X. Cardiac implications of thrombotic thrombocytopenic purpura. World J. Cardiol. 2018, 10, 254–266. [Google Scholar] [CrossRef]
- George, J.N. TTP: Long-term outcomes following recovery. Hematol. Am. Soc. Hematol. Educ. Program 2018, 2018, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Sukumar, S.; Brodsky, M.A.; Hussain, S.; Yanek, L.R.; Moliterno, A.R.; Brodsky, R.A.; Cataland, S.R.; Chaturvedi, S. Cardiovascular disease is a leading cause of mortality among TTP survivors in clinical remission. Blood Adv. 2022, 6, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Borogovac, A.; George, J.N. Stroke and myocardial infarction in hereditary thrombotic thrombocytopenic purpura: Similarities to sickle cell anemia. Blood Adv. 2019, 3, 3973–3976. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.A.; Sukumar, S.; Selvakumar, S.; Yanek, L.; Hussain, S.; Mazepa, M.A.; Braunstein, E.M.; Moliterno, A.R.; Kickler, T.S.; Brodsky, R.A.; et al. Major adverse cardiovascular events in survivors of immune-mediated thrombotic thrombocytopenic purpura. Am. J. Hematol. 2021, 96, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Upreti, H.; Kasmani, J.; Dane, K.; Braunstein, E.M.; Streiff, M.B.; Shanbhag, S.; Moliterno, A.R.; Sperati, C.J.; Gottesman, R.F.; Brodsky, R.A.; et al. Reduced ADAMTS13 activity during TTP remission is associated with stroke in TTP survivors. Blood 2019, 134, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Alwan, F.; Vendramin, C.; Liesner, R.; Clark, A.; Lester, W.; Dutt, T.; Thomas, W.; Gooding, R.; Biss, T.; Watson, H.G.; et al. Characterization and treatment of congenital thrombotic thrombocytopenic purpura. Blood 2019, 133, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- van Dorland, H.A.; Taleghani, M.M.; Sakai, K.; Friedman, K.D.; George, J.N.; Hrachovinova, I.; Knöbl, P.N.; von Krogh, A.S.; Schneppenheim, R.; Aebi-Huber, I.; et al. The International Hereditary Thrombotic Thrombocytopenic Purpura Registry: Key findings at enrollment until 2017. Haematologica 2019, 104, 2107–2115. [Google Scholar] [CrossRef]
- Morici, N.; Cantoni, S.; Panzeri, F.; Sacco, A.; Rusconi, C.; Stucchi, M.; Oliva, F.; Cattaneo, M. von Willebrand factor and its cleaving protease ADAMTS13 balance in coronary artery vessels: Lessons learned from thrombotic thrombocytopenic purpura. A narrative review. Thromb. Res. 2017, 155, 78–85. [Google Scholar] [CrossRef]
- Hawkins, B.M.; Abu-Fadel, M.; Vesely, S.K.; George, J.N. Clinical cardiac involvement in thrombotic thrombocytopenic purpura: A systematic review. Transfusion 2008, 48, 382–392. [Google Scholar] [CrossRef]
- Wahla, A.S.; Ruiz, J.; Noureddine, N.; Upadhya, B.; Sane, D.C.; Owen, J. Myocardial infarction in thrombotic thrombocytopenic purpura: A single-center experience and literature review. Eur. J. Haematol. 2008, 81, 311–316. [Google Scholar] [CrossRef]
- Balasubramaniyam, N.; Kolte, D.; Palaniswamy, C.; Yalamanchili, K.; Aronow, W.S.; McClung, J.A.; Khera, S.; Sule, S.; Peterson, S.J.; Frishman, W.H. Predictors of in-hospital mortality and acute myocardial infarction in thrombotic thrombocytopenic purpura. Am. J. Med. 2013, 126, 1016.e1–1016.e7. [Google Scholar] [CrossRef] [PubMed]
- Balasubramaniyam, N.; Yandrapalli, S.; Kolte, D.; Pemmasani, G.; Janakiram, M.; Frishman, W.H. Cardiovascular Complications and Their Association with Mortality in Patients with Thrombotic Thrombocytopenic Purpura. Am. J. Med. 2020, 134, e89–e97. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.; McEwan, J.R.; Longair, I.; Hughes, S.; Cohen, H.; Machin, S.; Scully, M. Cardiac involvement in acute thrombotic thrombocytopenic purpura: Association with troponin T and IgG antibodies to ADAMTS 13. J. Thromb. Haemost. 2009, 7, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, Y.; Boelle, P.Y.; Baudin, B.; Ederhy, S.; Gras, J.; Galicier, L.; Patricia, Z. Cardiac troponin-I on diagnosis predicts early death and refractoriness in acquired thrombotic thrombocytopenic purpura. Experience of the French Thrombotic Microangiopathies Reference Center. J. Thromb. Haemost. 2015, 13, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; King, K.E.; Takemoto, C.M.; Ness, P.M.; Tobian, A.A. Prognostic risk-stratified score for predicting mortality in hospitalized patients with thrombotic thrombocytopenic purpura: Nationally representative data from 2007 to 2012. Transfusion 2016, 56, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Echocardiography; American Heart Association; American Society of Nuclear Cardiology; Heart Failure Society of America; Heart Rhythm Society; Society for Cardiovascular Angiography and Interventions; Society of Critical Care Medicine; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. J. Am. Soc. Echocardiogr. 2011, 24, 229–267. [Google Scholar]
- Elverdi, T.; Ozer Cerme, M.D.; Aydin, T.; Eskazan, A.E. Do patients with immune-mediated thrombotic thrombocytopenic purpura receiving caplacizumab need antithrombotic therapy? Expert. Rev. Clin. Pharmacol. 2021, 14, 1183–1188. [Google Scholar] [CrossRef]
- Ho, H.H.; Minutello, R.; Juliano, N.; Wong, S.C. A rare cause of acute myocardial infarction: Thrombotic thrombocytopenic purpura. Int. J. Cardiol. 2009, 133, e1–e2. [Google Scholar] [CrossRef]
- Scully, M.; Yarranton, H.; Liesner, R.; Cavenagh, J.; Hunt, B.; Benjamin, S.; Bevan, D.; Mackie, I.; Machin, S. Regional UK TTP registry: Correlation with laboratory ADAMTS 13 analysis and clinical features. Br. J. Haematol. 2008, 142, 819–826. [Google Scholar] [CrossRef]
- Tomich, C.; Debruxelles, S.; Delmas, Y.; Sagnier, S.; Poli, M.; Olindo, S.; Renou, P.; Rouanet, F.; Sibon, I. Immune-Thrombotic Thrombocytopenic Purpura is a Rare Cause of Ischemic Stroke in Young Adults: Case Reports and Literature Review. J. Stroke Cerebrovasc. Dis. 2018, 27, 3163–3171. [Google Scholar] [CrossRef]
- Prevel, R.; Roubaud-Baudron, C.; Gourlain, S.; Jamme, M.; Peres, K.; Benhamou, Y.; Galicier, L.; Azoulay, E.; Poullin, P.; Provôt, F.; et al. Immune thrombotic thrombocytopenic purpura in older patients: Prognosis and long-term survival. Blood 2019, 134, 2209–2217. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Simpson, A.; Bhagnani, T.; Leeper, N.J.; Murphy, B.; Nordstrom, B.; Ting, W.; Zhao, Q.; Berger, J.S. Incidence and Cost of Major Adverse Cardiovascular Events and Major Adverse Limb Events in Patients with Chronic Coronary Artery Disease or Peripheral Artery Disease. Am. J. Cardiol. 2019, 123, 1893–1899. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.G.; Rha, S.; Yoon, S.G.; Choi, C.U.; Lee, M.W.; Kim, S.W. Association of Major Adverse Cardiac Events up to 5 Years in Patients with Chest Pain Without Significant Coronary Artery Disease in the Korean Population. J. Am. Heart Assoc. 2019, 8, e010541. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Tsao, C.W. Heart Disease and Stroke Statistics—2021 Update: A Report from the American Heart Association. Circulation 2021, 143, CIR0000000000000950. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Yu, J.; Brown, J.; Wei, A.; Gerber, G.; Pan, X.Z.; Chaturvedi, S. Silent cerebral infarction during immune TTP remission—prevalence, predictors, and impact on cognition. Blood 2023, 140 (Suppl. S1), 338–340. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, S.; Aspelund, T.; Kjartansson, O.; Gudmundsson, E.F.; Jonsdottir, M.K.; Eiriksdottir, G.; Launer, L.J. Incidence of Brain Infarcts, Cognitive Change, and Risk of Dementia in the General Population: The AGES-Reykjavik Study (Age Gene/Environment Susceptibility-Reykjavik Study). Stroke 2017, 48, 2353–2360. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Giambrone, A.; Gialdini, G.; Finn, C.B.; Delgado, D.; Gutierrez, J.; Wright, C.; Beiser, A.B.; Seshadri, S.; Pandya, A.; et al. Abstract WP165: Silent Brain Infarction and Risk of Future Stroke: A Systematic Review and Meta-Analysis. Stroke 2016, 47, 719–725. [Google Scholar] [CrossRef]
- Howard, M.A.; Duvall, D.; Terrell, D.R.; Christopher, A.T.; Thomas, I.; Holloway, N.; Vesely, S.K.; George, J.N. A support group for patients who have recovered from thrombotic thrombocytopenic purpura-hemolytic uremic syndrome (TTP-HUS): The six-year experience of the Oklahoma TTP-HUS Study Group. J. Clin. Apher. 2003, 18, 16–20. [Google Scholar] [CrossRef]
- George, J.N.; Terrell, D.R.; Swisher, K.K.; Vesely, S.K. Lessons learned from the oklahoma thrombotic thrombocytopenic purpura-hemolytic uremic syndrome registry. J. Clin. Apher. 2008, 23, 129–137. [Google Scholar] [CrossRef]
- Kennedy, A.S.; Lewis, Q.F.; Scott, J.G.; Hovinga, J.A.K.; Lämmle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Cognitive deficits after recovery from thrombotic thrombocytopenic purpura. Transfusion 2009, 49, 1092–1101. [Google Scholar] [CrossRef]
- Cataland, S.R.; Scully, M.A.; Paskavitz, J.; Maruff, P.; Witkoff, L.; Jin, M.; Wu, H.M. Evidence of persistent neurologic injury following thrombotic thrombocytopenic purpura. Am. J. Hematol. 2011, 86, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Falter, T.; Schmitt, V.; Herold, S.; Weyer, V.; von Auer, C.; Wagner, S.; Hefner, G.; Beutel, M.; Lackner, K.; Lämmle, B.; et al. Depression and cognitive deficits as long-term consequences of thrombotic thrombocytopenic purpura. Transfusion 2017, 57, 1152–1162. [Google Scholar] [CrossRef] [PubMed]
- Vermeer, S.E.; Koudstaal, P.J.; Oudkerk, M.; Hofman, A.; Breteler, M.M. Prevalence and risk factors of silent brain infarcts in the population-based rotterdam scan study. Stroke 2002, 33, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Schmidt, H.; Pichler, M.; Enzinger, C.; Petrovic, K.; Niederkorn, K.; Fazekas, F. C-reactive protein, carotid atherosclerosis, and cerebral small-vessel disease: Results of the Austrian Stroke Prevention Study. Stroke 2006, 37, 2910–2916. [Google Scholar] [CrossRef] [PubMed]
- Price, T.R.; Manolio, T.A.; Kronmal, R.A.; Kittner, S.J.; Yue, N.C.; Robbins, J.; Anton-Culver, H.; O’leary, D.H. Silent brain infarction on magnetic resonance imaging and neurological abnormalities in community-dwelling older adults. The Cardiovascular Health Study. CHS Collaborative Research Group. Stroke 1997, 28, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Howard, G.; Wagenknecht, L.E.; Cai, J.; Cooper, L.; Kraut, M.A.; Toole, J.F. Cigarette smoking and other risk factors for silent cerebral infarction in the general population. Stroke 1998, 29, 913–917. [Google Scholar] [CrossRef] [PubMed]
- DeCarli, C.; Massaro, J.; Harvey, D.; Hald, J.; Tullberg, M.; Au, R.; Beiser, A.; D’agostino, R.; Wolf, P.A. Measures of brain morphology and infarction in the framingham heart study: Establishing what is normal. Neurobiol. Aging 2005, 26, 491–510. [Google Scholar] [CrossRef]
- Das, R.R.; Seshadri, S.; Beiser, A.S.; Kelly-Hayes, M.; Au, R.; Himali, J.J.; Kase, C.S.; Benjamin, E.J.; Polak, J.F.; O’Donnell, C.J.; et al. Prevalence and correlates of silent cerebral infarcts in the framingham offspring study. Stroke 2008, 39, 2929–2935. [Google Scholar] [CrossRef]
- Fanning, J.P.; Wong, A.A.; Fraser, J.F. The epidemiology of silent brain infarction: A systematic review of population-based cohorts. BMC Med. 2014, 12, 119. [Google Scholar] [CrossRef]
- Vermeer, S.E.; Hollander, M.; van Dijk, E.J.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M. Silent brain infarcts and white matter lesions increase stroke risk in the general population: The Rotterdam Scan Study. Stroke 2003, 34, 1126–1129. [Google Scholar] [CrossRef]
- Pegelow, C.H.; Macklin, E.A.; Moser, F.G.; Wang, W.C.; Bello, J.A.; Miller, S.T.; Vichinsky, E.P.; DeBaun, M.R.; Guarini, L.; Zimmerman, R.A.; et al. Longitudinal changes in brain magnetic resonance imaging findings in children with sickle cell disease. Blood 2002, 99, 3014–3018. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef] [PubMed]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Prospective Studies Collaboration; Whitlock, G.; Lewington, S. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef]
- Martino, S.; Jamme, M.; Deligny, C.; Busson, M.; Loiseau, P.; Azoulay, E.; Galicier, L.; Pène, F.; Provôt, F.; Dossier, A.; et al. Thrombotic Thrombocytopenic Purpura in Black People: Impact of Ethnicity on Survival and Genetic Risk Factors. PLoS ONE 2016, 11, e0156679. [Google Scholar] [CrossRef]
- Feldman, C.H.; Hiraki, L.T.; Liu, J.; Fischer, M.A.; Solomon, D.H.; Alarcón, G.S.; Winkelmayer, W.C.; Costenbader, K.H. Epidemiology and sociodemographics of systemic lupus erythematosus and lupus nephritis among US adults with Medicaid coverage, 2000–2004. Arthritis Rheum. 2013, 65, 753–763. [Google Scholar] [CrossRef]
- Javed, Z.; Maqsood, M.H.; Yahya, T.; Amin, Z.; Acquah, I.; Valero-Elizondo, J.; Andrieni, J.; Dubey, P.; Jackson, R.K.; Daffin, M.A.; et al. Race, Racism, and Cardiovascular Health: Applying a Social Determinants of Health Framework to Racial/Ethnic Disparities in Cardiovascular Disease. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e007917. [Google Scholar] [CrossRef]
- Devareddy, A.; Sarraju, A.; Rodriguez, F. Health Disparities Across the Continuum of ASCVD Risk. Curr. Cardiol. Rep. 2022, 24, 1129–1137. [Google Scholar] [CrossRef]
- Mariotti, A.; MacLeod, R.; Hillert, E.-K.; Cameron, R.T.; Baillie, G.S.; Moscato, P.; Lustig, L.C.; Ponzielli, R.; Tang, P.S.; Sathiamoorthy, S.; et al. The effects of chronic stress on health: New insights into the molecular mechanisms of brain–body communication. Futur. Sci. OA 2015, 1, FSO23. [Google Scholar] [CrossRef] [PubMed]
- Surachman, A.; Jenkins, A.I.; Santos, A.R.; Almeida, D.M. Socioeconomic status trajectories across the life course, daily discrimination, and inflammation among Black and white adults. Psychoneuroendocrinology 2021, 127, 105193. [Google Scholar] [CrossRef] [PubMed]
- McClendon, J.; Chang, K.; Boudreaux, M.J.; Oltmanns, T.F.; Bogdan, R. Black-White racial health disparities in inflammation and physical health: Cumulative stress, social isolation, and health behaviors. Psychoneuroendocrinology 2021, 131, 105251. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, M.A.H.; de Maat, M.P.M.; Portegies, M.L.P.; Kavousi, M.; Hofman, A.; Turecek, P.L.; Rottensteiner, H.; Scheiflinger, F.; Koudstaal, P.J.; Ikram, M.A.; et al. Low ADAMTS13 activity is associated with an increased risk of ischemic stroke. Blood 2015, 126, 2739–2746. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, M.A.H.; Kavousi, M.; Ikram, M.A.; Hofman, A.; Ochoa, O.L.R.; Turecek, P.L.; Franco, O.H.; Leebeek, F.W.G.; de Maat, M.P.M. Low ADAMTS-13 activity and the risk of coronary heart disease—A prospective cohort study: The Rotterdam Study. J. Thromb. Haemost. 2016, 14, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, M.A.; Franco, O.H.; Ikram, M.A. Von Willebrand Factor, ADAMTS13, and the Risk of Mortality: The Rotterdam Study. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 2446–2451. [Google Scholar] [CrossRef] [PubMed]
- Federici, A.B.; Bader, R.; Pagani, S.; Colibretti, M.L.; Marco, L.; Mannucci, P.M. Binding of von Willebrand factor to glycoproteins Ib and IIb/IIIa complex: Affinity is related to multimeric size. Br. J. Haematol. 1989, 73, 93–99. [Google Scholar] [CrossRef]
- Noone, D.G.; Riedl, M.; Pluthero, F.G.; Bowman, M.L.; Liszewski, M.K.; Lu, L.; Quan, Y.; Balgobin, S.; Schneppenheim, R.; Schneppenheim, S.; et al. Von Willebrand factor regulates complement on endothelial cells. Kidney Int. 2016, 90, 123–134. [Google Scholar] [CrossRef]
- Turner, N.; Nolasco, L.; Nolasco, J.; Sartain, S.; Moake, J. Thrombotic microangiopathies and the linkage between von willebrand factor and the alternative complement pathway. Semin. Thromb. Hemost. 2014, 40, 544–550. [Google Scholar] [CrossRef]
- Jin, S.-Y.; Tohyama, J.; Bauer, R.C.; Cao, N.N.; Rader, D.J.; Zheng, X.L. Genetic ablation of adamts13 gene dramatically accelerates the formation of early atherosclerosis in a murine model. Arter. Thromb. Vasc. Biol. 2012, 32, 1817–1823. [Google Scholar] [CrossRef]
- Gandhi, C.; Khan, M.M.; Lentz, S.R.; Chauhan, A.K. ADAMTS13 reduces vascular inflammation and the development of early atherosclerosis in mice. Blood 2012, 119, 2385–2391. [Google Scholar] [CrossRef]
- Cuker, A.; Cataland, S.R.; Coppo, P.; de la Rubia, J.; Friedman, K.D.; George, J.N.; Knoebl, P.N.; Kremer Hovinga, J.A.; Lämmle, B.; Matsumoto, M.; et al. Redefining outcomes in immune TTP: An international working group consensus report. Blood 2021, 137, 1855–1861. [Google Scholar] [CrossRef]
- Scully, M.; Cataland, S.R.; Peyvandi, F.; Coppo, P.; Knöbl, P.; Kremer Hovinga, J.A.; Zeldin, R.K. Caplacizumab Treatment for Acquired Thrombotic Thrombocytopenic Purpura. N. Engl. J. Med. 2019, 380, 335–346. [Google Scholar] [CrossRef]
- de Maat, S.; Clark, C.C.; Barendrecht, A.D.; Smits, S.; van Kleef, N.D.; El Otmani, H.; Waning, M.; van Moorsel, M.V.A.; Szardenings, M.; Delaroque, N.; et al. Microlyse: A thrombolytic agent that targets VWF for clearance of microvascular thrombosis. Blood 2022, 139, 597–607. [Google Scholar] [CrossRef]
- Hie, M.; Gay, J.; Galicier, L.; Provôt, F.; Presne, C.; Poullin, P.; Bonmarchand, G.; Wynckel, A.; Benhamou, Y.; Vanhille, P.; et al. Preemptive rituximab infusions after remission efficiently prevent relapses in acquired thrombotic thrombocytopenic purpura. Blood 2014, 124, 204–210. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukumar, S.; Mazepa, M.A.; Chaturvedi, S. Cardiovascular Disease and Stroke in Immune TTP–Challenges and Opportunities. J. Clin. Med. 2023, 12, 5961. https://doi.org/10.3390/jcm12185961
Sukumar S, Mazepa MA, Chaturvedi S. Cardiovascular Disease and Stroke in Immune TTP–Challenges and Opportunities. Journal of Clinical Medicine. 2023; 12(18):5961. https://doi.org/10.3390/jcm12185961
Chicago/Turabian StyleSukumar, Senthil, Marshall A. Mazepa, and Shruti Chaturvedi. 2023. "Cardiovascular Disease and Stroke in Immune TTP–Challenges and Opportunities" Journal of Clinical Medicine 12, no. 18: 5961. https://doi.org/10.3390/jcm12185961