
Prolonged Ileus after Colorectal Surgery, a Systematic Review
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Search Strategy
2.3. Study Screening
2.4. Data Extraction
2.5. Data Synthesis
2.6. Risk of Bias Analysis
3. Results
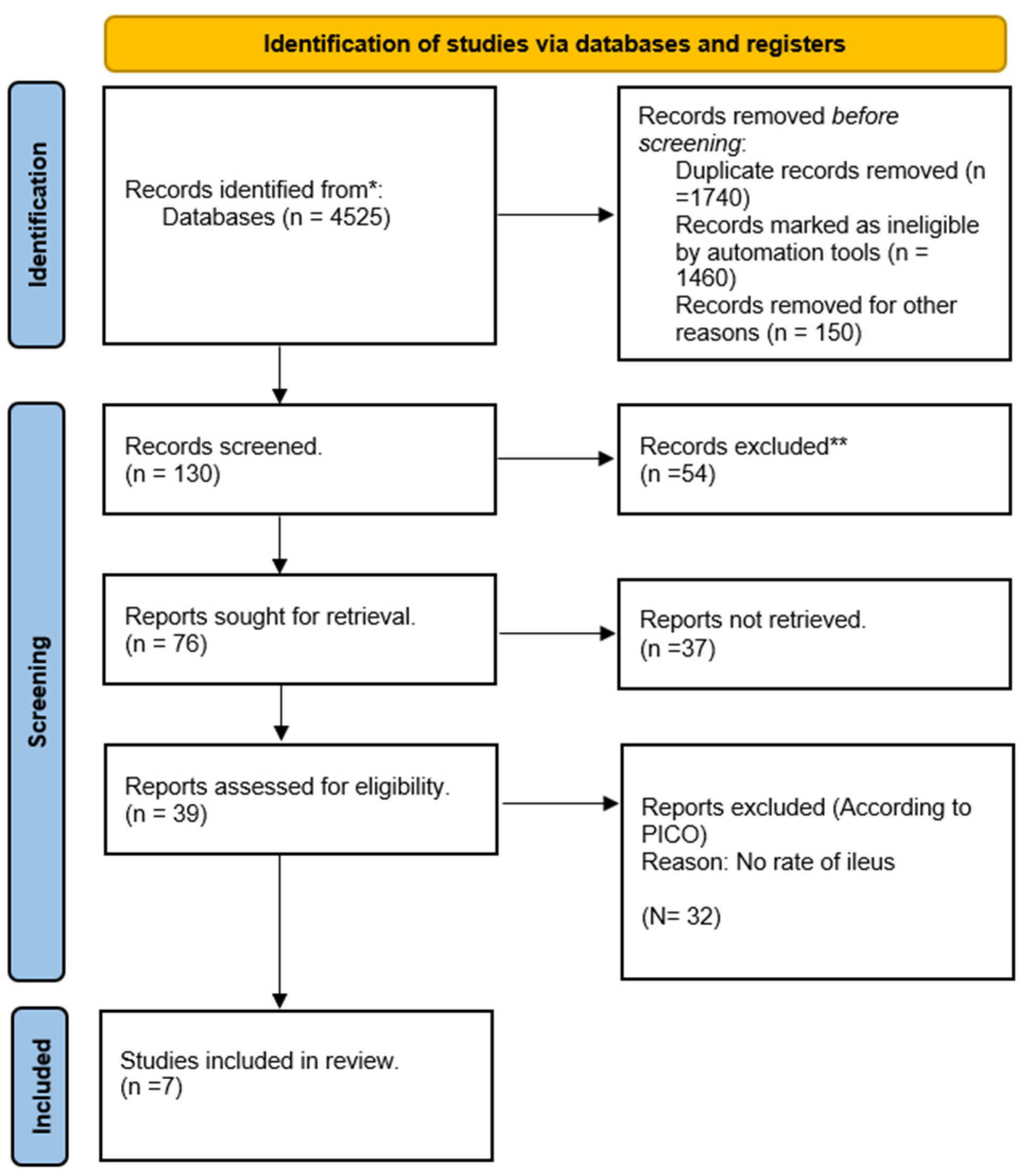
3.1. Search Results and Study Selection
3.2. Study Characteristics
3.3. Study Outcomes
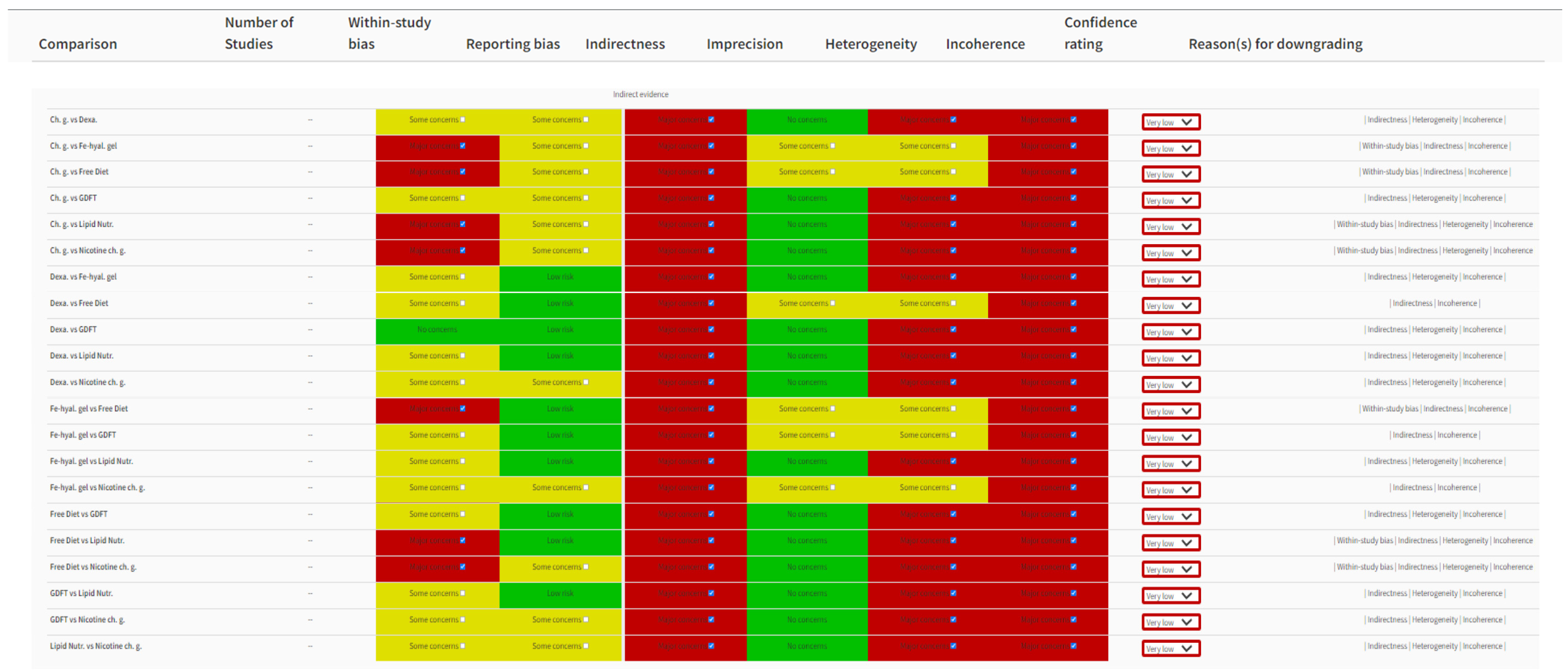
3.4. Risk of Bias (RoB) Outcomes
4. Discussion
4.1. Summary of Findings
4.2. Interpretation of Results
4.3. Strength and Limitations
4.4. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ovid MEDLINE(R) ALL <1946 to 4 April 2022> | |
|---|---|
| Search Statement | Results |
| exp Ileus/ | 5900 |
| ileus.ab,kf,ti. | 12,690 |
| 1 or 2 | 15,480 |
| exp Colon/su [Surgery] | 13,689 |
| exp Colorectal Surgery/ | 4051 |
| exp Rectum/su [Surgery] | 12,063 |
| exp Inflammatory Bowel Diseases/su [Surgery] | 11,163 |
| Diverticulitis, Colonic/su [Surgery] | 1731 |
| Diverticulum, Colon/su [Surgery] | 791 |
| Cecal Diseases/su [Surgery] | 1464 |
| exp Colorectal Neoplasms/su [Surgery] | 47,610 |
| exp Rectal Neoplasms/su [Surgery] | 21,676 |
| exp Cecal Neoplasms/su [Surgery] | 2054 |
| ((colorectal* adj6 surgery) or (colorectal adj6 surgical) or (colorectal adj6 resect*) or (colorectal adj6 laparoscop*) or (colorectal adj6 laparotom*)).ab,kf,ti. | 25,019 |
| ((colon* adj6 surgery) or (colon* adj6 surgical) or (colon* adj6 resect*) or (colon adj6 laparoscop*) or (colon adj6 laparotom*)).ab,kf,ti. | 20,924 |
| ((rectum adj6 surgery) or (rectum adj6 surgical) or (rectum adj6 resect*) or (rectum adj6 laparoscop*) or (rectum adj6 laparotom*)).ab,kf,ti. | 4669 |
| ((rectal adj6 surgery) or (rectal adj6 surgical) or (rectal adj6 resect*) or (rectal adj6 laparoscop*) or (rectal adj6 laparotom*)).ab,kf,ti. | 16,876 |
| ((“inflammatory bowel” adj6 surgery) or (“inflammatory bowel” adj6 surgical) or (“inflammatory bowel” adj6 resect*) or (“inflammatory bowel” adj6 laparoscop*) or (“inflammatory bowel” adj6 laparotom*)).ab,kf,ti. | 1119 |
| ((caecal adj6 surgery) or (caecal adj6 surgical) or (caecal adj6 resect*) or (caecal adj6 laparoscop*) or (caecal adj6 laparotom*)).ab,kf,ti. | 210 |
| ((caecum adj6 surgery) or (caecum adj6 surgical) or (caecum adj6 resect*) or (caecum adj6 laparoscop*) or (caecum adj6 laparotom*)).ab,kf,ti. | 146 |
| ((cecal adj6 surgery) or (cecal adj6 surgical) or (cecal adj6 resect*) or (cecal adj6 laparoscop*) or (cecal adj6 laparotom*)).ab,kf,ti. | 784 |
| ((cecum adj6 surgery) or (cecum adj6 surgical) or (cecum adj6 resect*) or (cecum adj6 laparoscop*) or (cecum adj6 laparotom*)).ab,kf,ti. | 525 |
| ((colitis adj6 surgery) or (colitis adj6 surgical) or (colitis adj6 resect*) or (colitis adj6 laparoscop*) or (colitis adj6 laparotom*)).ab,kf,ti. | 2585 |
| ((crohn* adj6 surgery) or (crohn* adj6 surgical) or (crohn* adj6 resect*) or (crohn* adj6 laparoscop*) or (crohn* adj6 laparotom*)).ab,kf,ti. | 3294 |
| Anal Canal/su [Surgery] | 6268 |
| ((anal adj6 surgery) or (anal adj6 surgical) or (anal adj6 resect*) or (anal adj6 laparoscop*) or (anal adj6 laparotom*)).ab,kf,ti. | 3148 |
| ((anus adj6 surgery) or (anus adj6 surgical) or (anus adj6 resect*) or (anus adj6 laparoscop*) or (anus adj6 laparotom*)).ab,kf,ti. | 736 |
| ((anorectal adj6 surgery) or (anorectal adj6 surgical) or (anorectal adj6 resect*) or (anorectal adj6 laparoscop*) or (anorectal adj6 laparotom*)).ab,kf,ti. | 1551 |
| ((bowel adj6 surgery) or (bowel adj6 surgical) or (bowel adj6 resect*) or (bowel adj6 laparoscop*) or (bowel adj6 laparotom*)).ab,kf,ti. | 17,631 |
| colectomy/ or proctocolectomy, restorative/ or cecostomy/ or colostomy/ or ileostomy/ or proctectomy/ | 35,635 |
| (“Hartmann’s” or Hartmanns or polypectomy or colectom* or hemicolectomy or ileostomy or proctocolectomy or panproctocolectomy or “pan procto-colectomy” or proctectomy or “anterior resection” or “abdominoperineal resection” or “abdomino-perineal resection” or colostomy or cecostomy).ab,kf,ti. | 45,348 |
| (“Ileoanal anastomos*” or “ileo-rectal anastomos*” or “coloanal anastomos*” or “colo-anal anatomos*”).ab,kf,ti. | 1438 |
| sigmoidectomy.ab,kf,ti. | 1131 |
| (strictureplasty or stricturoplasty).ab,kf,ti. | 431 |
| Colonic Polyps/su [Surgery] | 2983 |
| ((“colonic polyps” adj6 surgery) or (“colonic polyps” adj6 surgical) or (“colonic polyps” adj6 resect*)).ab,kf,ti. | 122 |
| or/4-36 | 156,074 |
| 3 and 37 | 3188 |
| randomized controlled trial.pt. | 563,321 |
| controlled clinical trial.pt. | 94,786 |
| (randomized or randomised or randomly or groups or placebo or trial).ab,ti. | 3,328,560 |
| 39 or 40 or 41 | 3,456,549 |
| 38 and 42 | 821 |
| exp animals/not humans.sh. | 4,983,455 |
| 43 not 44 | 795 |
| limit 45 to english language | 739 |
Appendix B

References
- Vather, R.; Trivedi, S.; Bissett, I. Defining postoperative ileus: Results of a systematic review and global survey. J. Gastrointest. Surg. 2013, 17, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Mattei, P.; Rombeau, J.L. Review of the pathophysiology and management of postoperative ileus. World J. Surg. 2006, 30, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, J.; Singh, A.A.; Ramachandran, B.; Habeeb, A.; Hudson, V.; Meyer, J.; Simillis, C.; Davies, R.J. Reducing ileus after colorectal surgery: A network meta-analysis of therapeutic interventions. Clin. Nutr. 2021, 40, 4772–4782. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.J.; Pericleous, A.; Downey, C.; Jayne, D.G. Postoperative ileus following major colorectal surgery. Br. J. Surg. 2018, 105, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.L.; Kelly, Y.M.; McKay, R.E.; Varma, M.G.; Sarin, A. Risk factors and outcomes associated with postoperative ileus following ileostomy formation: A retrospective study. Perioper. Med. 2021, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Wolthuis, A.M.; Bislenghi, G.; Fieuws, S.; de Buck van Overstraeten, A.; Boeckxstaens, G.; D’Hoore, A. Incidence of prolonged postoperative ileus after colorectal surgery: A systematic review and meta-analysis. Colorectal. Dis. 2016, 18, O1–O9. [Google Scholar] [CrossRef] [PubMed]
- Venara, A.; Neunlist, M.; Slim, K.; Barbieux, J.; Colas, P.A.; Hamy, A.; Meurette, G. Postoperative ileus: Pathophysiology, incidence, and prevention. J. Visc. Surg. 2016, 153, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.J.; Lee, M.J.; Blackwell, S.; Arnott, R.; Ten Broek, R.P.G.; Delaney, C.P.; Dudi-Venkata, N.N.; Hind, D.; Jayne, D.G.; Mellor, K.; et al. Tripartite Gastrointestinal Recovery Group. Establishing core outcome sets for gastrointestinal recovery in studies of postoperative ileus and small bowel obstruction: Protocol for a nested methodological study. Colorectal. Dis. 2020, 22, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Review Manager (RevMan), version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef]
- Zhang, T.; Xu, Y.; Yao, Y.; Jin, L.; Liu, H.; Zhou, Y.; Gu, L.; Ji, Q.; Zhu, W.; Gong, J. Randomized Controlled Trial: Perioperative Dexamethasone Reduces Excessive Postoperative Inflammatory Response and Ileus After Surgery for Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 1756–1765. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Izquierdo, J.C.; Trainito, A.; Mirzakandov, D.; Stein, B.L.; Liberman, S.; Charlebois, P.; Pecorelli, N.; Feldman, L.S.; Carli, F.; Baldini, G. Goal-directed Fluid Therapy Does Not Reduce Primary Postoperative Ileus after Elective Laparoscopic Colorectal Surgery: A Randomized Controlled Trial. Anesthesiology 2017, 127, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Han-Geurts, I.J.; Hop, W.C.; Kok, N.F.; Lim, A.; Brouwer, K.J.; Jeekel, J. Randomized clinical trial of the impact of early enteral feeding on postoperative ileus and recovery. Br. J. Surg. 2007, 94, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Lambrichts, D.P.V.; Boersema, G.S.A.; Tas, B.; Wu, Z.; Vrijland, W.W.; Kleinrensink, G.J.; Jeekel, J.; Lange, J.F.; Menon, A.G. Nicotine chewing gum for the prevention of postoperative ileus after colorectal surgery: A multicenter, double-blind, randomised, controlled pilot study. Int. J. Colorectal. Dis. 2017, 32, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Zaghiyan, K.; Felder, S.; Ovsepyan, G.; Murrell, Z.; Sokol, T.; Moore, B.; Fleshner, P. A prospective randomized controlled trial of sugared chewing gum on gastrointestinal recovery after major colorectal surgery in patients managed with early enteral feeding. Dis. Colon. Rectum. 2013, 56, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.G.; Smeets, B.J.J.; Nors, J.; Back, C.M.; Funder, J.A.; Sommer, T.; Laurberg, S.; Løve, U.S.; Leclercq, W.K.G.; Slooter, G.D.; et al. Perioperative lipid-enriched enteral nutrition versus standard care in patients undergoing elective colorectal surgery (SANICS II): A multicentre, double-blind, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2018, 3, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.L.; Jayne, D.G.; Seow-Choen, F.; Ng, Y.Y.; Eu, K.W.; Mustapha, N. A randomized controlled trial of 0.5% ferric hyaluronate gel (Intergel) in the prevention of adhesions following abdominal surgery. Ann. Surg. 2006, 243, 449–455. [Google Scholar] [CrossRef] [PubMed]




| Study | Year | Age: I/C (Median) | Sex: I/C (n) | Proce-Dure | Hemico-Lectomies (n) | Left Hemico-Lectomies/ Anterior (n) | Open/Laparoscopic/Robotic (n) | Intervention | Control |
|---|---|---|---|---|---|---|---|---|---|
| GomezIzquierdo [13] | 2017 | 63/61 | M: 31/33 F: 40/24 | Colorectal | 86 | 92 | Laparoscopic | Goal-directed fluid therapy | Traditional fluid therapy |
| HanGeurts [14] | 2007 | 63/67 | M: 36/25 F:32/35 | Colorectal | 33 | 27 | Open | Free diet | Conventional diet |
| Lambrichts [15] | 2017 | 67.5/69 | M: 14/6 F: 13/7 | Colorectal | 14 | 5 | Open: 4 Laparoscopic: 36 | Nicotine chewing gum | Normal chewing gum |
| Peters [17] | 2018 | 69/68 | M: 80/52 F: 52/55 | Colorectal | 94 | 106 | Open: 112 Laparoscopic: 153 | Nutrition lipid-enriched enteral nutrition | No perioperative nutrition |
| Tang [18] | 2006 | 65/67 | M: 17/15 F: 9/6 | Colorectal | 7 | 10 | Open: 29 | Ferric hyaluronate gel | No gel |
| Zaghiyan [16] | 2012 | 42.1/48.8 | M: 33/21 F: 34/26 | Colorectal | 13 | 15 | Open: 44 Laparoscopic: 70 | Chewing gum | No gum |
| Zhang [12] | 2022 | 39.84/42.60 | M: 89/62 F: 96/55 | Colorectal and others | 25 | 3 | Open: 26 Laparoscopic: 68 | Dexamethasone | Placebo |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shereef, A.; Raftery, D.; Sneddon, F.; Emslie, K.; Mair, L.; Mackay, C.; Ramsay, G.; Forget, P. Prolonged Ileus after Colorectal Surgery, a Systematic Review. J. Clin. Med. 2023, 12, 5769. https://doi.org/10.3390/jcm12185769
Shereef A, Raftery D, Sneddon F, Emslie K, Mair L, Mackay C, Ramsay G, Forget P. Prolonged Ileus after Colorectal Surgery, a Systematic Review. Journal of Clinical Medicine. 2023; 12(18):5769. https://doi.org/10.3390/jcm12185769
Chicago/Turabian StyleShereef, Anzil, David Raftery, Fraser Sneddon, Katy Emslie, Lyn Mair, Craig Mackay, George Ramsay, and Patrice Forget. 2023. "Prolonged Ileus after Colorectal Surgery, a Systematic Review" Journal of Clinical Medicine 12, no. 18: 5769. https://doi.org/10.3390/jcm12185769