

Vincristine-Induced Neuropathy in Patients Diagnosed with Solid and Hematological Malignancies: The Role of Dose Rounding
 , , and
, , and
Abstract
:1. Introduction
2. Methods
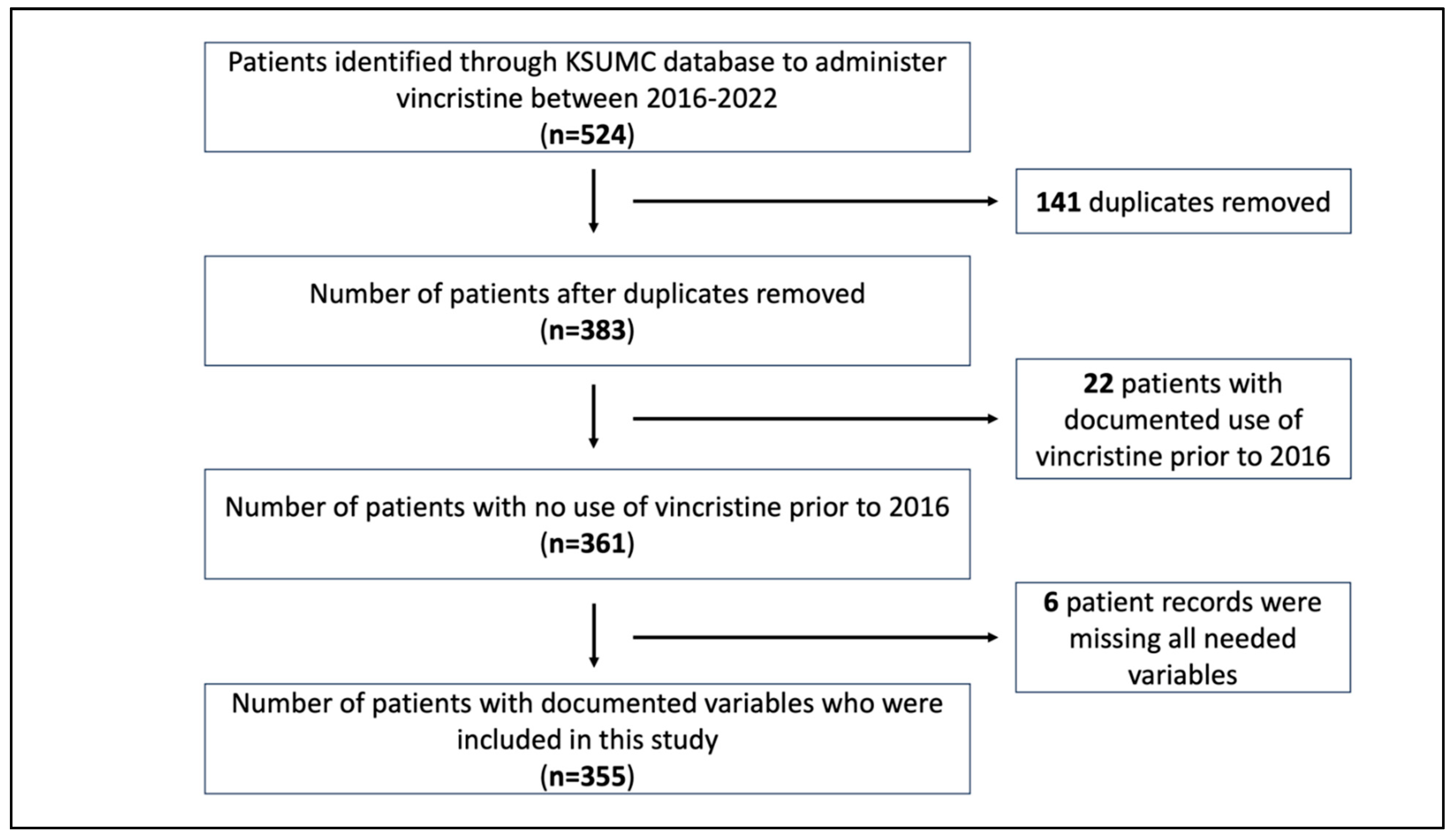
2.1. Subjects and Database
2.2. Study Design and Setting
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Enrolled Subjects
3.2. Factors Affecting the Frequency of Vincristine-Induced Neuropathy
3.3. Impact of Dose Rounding on the Incidence of Neuropathy
4. Discussion
4.1. Vincristine-Induced Neuropathy in Pediatric Patients
4.2. Vincristine-Induced Neuropathy in Adult Patients
4.3. Vincristine Dose Rounding and Neuropathy
5. Implications and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freireich, E.J.; Wiernik, P.H.; Steensma, D.P. The leukemias: A half-century of discovery. J. Clin. Oncol. 2014, 32, 3463–3469. [Google Scholar] [CrossRef]
- Dhyani, P.; Quispe, C.; Sharma, E.; Bahukhandi, A.; Sati, P.; Attri, D.C.; Szopa, A.; Sharifi-Rad, J.; Docea, A.O.; Mardare, I.; et al. Anticancer potential of alkaloids: A key emphasis to colchicine, vinblastine, vincristine, vindesine, vinorelbine and vincamine. Cancer Cell Int. 2022, 22, 206. [Google Scholar] [CrossRef]
- Gidding, C.E.; Kellie, S.J.; Kamps, W.A.; de Graaf, S.S. Vincristine revisited. Crit. Rev. Oncol. Hematol. 1999, 29, 267–287. [Google Scholar] [CrossRef]
- Zhou, X.J.; Rahmani, R. Preclinical and clinical pharmacology of vinca alkaloids. Drugs 1992, 44 (Suppl. S4), 1–69. [Google Scholar] [CrossRef]
- Anand, U.; Dey, A.; Chandel, A.K.S.; Sanyal, R.; Mishra, A.; Pandey, D.K.; De Falco, V.; Upadhyay, A.; Kandimalla, R.; Chaudhary, A.; et al. Cancer chemotherapy and beyond: Current status, drug candidates, associated risks and progress in targeted therapeutics. Genes Dis. 2022, 10, 1367–1401. [Google Scholar] [CrossRef]
- Legha, S.S. Vincristine neurotoxicity. Pathophysiology and management. Med. Toxicol. 1986, 1, 421–427. [Google Scholar] [CrossRef]
- Madsen, M.L.; Due, H.; Ejskjær, N.; Jensen, P.; Madsen, J.; Dybkær, K. Aspects of vincristine-induced neuropathy in hematologic malignancies: A systematic review. Cancer Chemother. Pharmacol. 2019, 84, 471–485. [Google Scholar] [CrossRef]
- Tuxen, M.K.; Hansen, S.W. Neurotoxicity secondary to antineoplastic drugs. Cancer Treat. Rev. 1994, 20, 191–214. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, G.; Sereno, M.; Miralles, A.; Casado-Sáenz, E.; Gutiérrez-Rivas, E. Chemotherapy-induced peripheral neuropathy: Clinical features, diagnosis, prevention and treatment strategies. Clin. Transl. Oncol. 2010, 12, 81–91. [Google Scholar] [CrossRef]
- Starobova, H.; Vetter, I. Pathophysiology of Chemotherapy-Induced Peripheral Neuropathy. Front. Mol. Neurosci. 2017, 10, 174. [Google Scholar] [CrossRef]
- Nazir, H.F.; AlFutaisi, A.; Zacharia, M.; Elshinawy, M.; Mevada, S.T.; Alrawas, A.; Khater, D.; Jaju, D.; Wali, Y. Vincristine-induced neuropathy in pediatric patients with acute lymphoblastic leukemia in Oman: Frequent autonomic and more severe cranial nerve involvement. Pediatr. Blood Cancer 2017, 64, 26677. [Google Scholar] [CrossRef]
- Gomber, S.; Dewan, P.; Chhonker, D. Vincristine induced neurotoxicity in cancer patients. Indian J. Pediatr. 2010, 77, 97–100. [Google Scholar] [CrossRef]
- van de Velde, M.E.; Kaspers, G.L.; Abbink, F.C.H.; Wilhelm, A.J.; Ket, J.C.F.; van den Berg, M.H. Vincristine-induced peripheral neuropathy in children with cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2017, 114, 114–130. [Google Scholar] [CrossRef]
- Dennison, J.B.; Jones, D.R.; Renbarger, J.L.; Hall, S.D. Effect of CYP3A5 expression on vincristine metabolism with human liver microsomes. J. Pharmacol. Exp. Ther. 2007, 321, 553–563. [Google Scholar] [CrossRef]
- Baxter, C.G.; Marshall, A.; Roberts, M.; Felton, T.W.; Denning, D.W. Peripheral neuropathy in patients on long-term triazole antifungal therapy. J. Antimicrob. Chemother. 2011, 66, 2136–2139. [Google Scholar] [CrossRef]
- van Schie, R.M.; Brüggemann, R.J.; Hoogerbrugge, P.M.; te Loo, D.M. Effect of azole antifungal therapy on vincristine toxicity in childhood acute lymphoblastic leukaemia. J. Antimicrob. Chemother. 2011, 66, 1853–1856. [Google Scholar] [CrossRef]
- Moriyama, B.; Henning, S.A.; Leung, J.; Falade-Nwulia, O.; Jarosinski, P.; Penzak, S.R.; Walsh, T.J. Adverse interactions between antifungal azoles and vincristine: Review and analysis of cases. Mycoses 2012, 55, 290–297. [Google Scholar] [CrossRef]
- Chillari, K.A.; Southward, J.; Harrigan, N. Assessment of the potential impact of dose rounding parenteral chemotherapy agents on cost savings and drug waste minimization. J. Oncol. Pharm. Pract. 2018, 24, 507–510. [Google Scholar] [CrossRef]
- Dela-Pena, J.C.; Eschenburg, K.A.; LaRocca, V.W.; Patel, D.; Hough, S.M. Financial Impact of an Automated Oncology Dose-Rounding Initiative: One-Year Analysis. JCO Clin. Cancer Inform. 2021, 5, 805–810. [Google Scholar] [CrossRef]
- Fahrenbruch, R.; Kintzel, P.; Bott, A.M.; Gilmore, S.; Markham, R. Dose Rounding of Biologic and Cytotoxic Anticancer Agents: A Position Statement of the Hematology/Oncology Pharmacy Association. J. Oncol. Pract. 2018, 14, e130–e136. [Google Scholar] [CrossRef]
- Jain, P.; Gulati, S.; Seth, R.; Bakhshi, S.; Toteja, G.S.; Pandey, R.M. Vincristine-induced neuropathy in childhood ALL (acute lymphoblastic leukemia) survivors: Prevalence and electrophysiological characteristics. J. Child Neurol. 2014, 29, 932–937. [Google Scholar] [CrossRef]
- Ramchandren, S.; Leonard, M.; Mody, R.J.; Donohue, J.E.; Moyer, J.; Hutchinson, R.; Gurney, J.G. Peripheral neuropathy in survivors of childhood acute lymphoblastic leukemia. J. Peripher. Nerv. Syst. 2009, 14, 184–189. [Google Scholar] [CrossRef]
- Tay, N.; Laakso, E.L.; Schweitzer, D.; Endersby, R.; Vetter, I.; Starobova, H. Chemotherapy-induced peripheral neuropathy in children and adolescent cancer patients. Front. Mol. Biosci. 2022, 9, 1015746. [Google Scholar] [CrossRef] [PubMed]
- Reinders-Messelink, H.A.; van Weerden, T.W.; Fock, J.M.; Gidding, C.E.; Vingerhoets, H.M.; Schoemaker, M.M.; Göeken, L.N.; Bökkerink, J.P.; Kamps, W.A. Mild axonal neuropathy of children during treatment for acute lymphoblastic leukaemia. Eur. J. Paediatr. Neurol. 2000, 4, 225–233. [Google Scholar] [CrossRef]
- Toopchizadeh, V.; Barzegar, M.; Rezamand, A.; Feiz, A.H. Electrophysiological consequences of vincristine contained chemotherapy in children: A cohort study. J. Pediatr. Neurol. 2009, 7, 351–356. [Google Scholar]
- Tunjungsari, D.A.; Gunawan, P.I.; Ugrasena, I.D.G. Risk Factors of Vincristine-Induced Peripheral Neuropathy in Acute Lymphoblastic Leukaemia Children. J. Med. Investig. 2021, 68, 232–237. [Google Scholar] [CrossRef]
- Rosenthal, S.; Kufman, S. Vincristine Neurotoxicity. Ann. Intern. Med. 1974, 80, 733–737. [Google Scholar] [CrossRef]
- Yalo, M.; Viget, C.; Derthe, B. Solutés de perfusions et accessoires Baxter. Etude relative à leur mise en place [Baxter infusion solutions and accessories. Implementation study]. Soins 1989, 531, 49–50. [Google Scholar]
- Grim, J.; Ticha, A.; Hyspler, R.; Valis, M.; Zadak, Z. Selected Risk Nutritional Factors for Chemotherapy-Induced Polyneuropathy. Nutrients 2017, 9, 535. [Google Scholar] [CrossRef] [PubMed]
- Sarris, A.; Hagemeister, F.; Romaguera, J.; Rodriguez, M.; McLaughlin, P.; Tsimberidou, A.; Medeiros, L.; Samuels, B.; Pate, O.; Oholendt, M.; et al. Liposomal vincristine in relapsed non-Hodgkin’s lymphomas: Early results of an ongoing phase II trial. Ann. Oncol. 2000, 11, 69–72. [Google Scholar] [CrossRef]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Kautio, A.L.; Haanpää, M.; Kautiainen, H.; Kalso, E.; Saarto, T. Burden of chemotherapy-induced neuropathy--a cross-sectional study. Support Care Cancer 2011, 19, 1991–1996. [Google Scholar] [CrossRef] [PubMed]
- Imam, E.A.; Ibrahim, A.; Palaian, S.; Ibrahim, M.I.M. Prevalence of vincristine induced-peripheral neuropathy among Sudanese cancer patients. J. Young Pharm. 2016, 8, 239–243. [Google Scholar] [CrossRef]
- Thackray, J.; Spatz, K.; Steinherz, P.G. Vincristine toxicity with co-administration of fluconazole: Long-term concerns. Pediatr. Blood Cancer 2017, 64, 26652. [Google Scholar] [CrossRef]
- Okada, N.; Hanafusa, T.; Sakurada, T.; Teraoka, K.; Kujime, T.; Abe, M.; Shinohara, Y.; Kawazoe, K.; Minakuchi, K. Risk Factors for Early-Onset Peripheral Neuropathy Caused by Vincristine in Patients With a First Administration of R-CHOP or R-CHOP-Like Chemotherapy. J. Clin. Med. Res. 2014, 6, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Dooley, M.J.; Singh, S.; Michael, M. Implications of dose rounding of chemotherapy to the nearest vial size. Support. Care Cancer 2004, 12, 653–656. [Google Scholar] [CrossRef]
- Ibrahim, N. Impact of dose rounding of cancer therapy on cost avoidance: A pilot study. Farmeconomia 2013, 14, 169–172. [Google Scholar] [CrossRef]
- Vandyke, T.H.; Athmann, P.W.; Ballmer, C.M.; Kintzel, P.E. Cost avoidance from dose rounding biologic and cytotoxic antineoplastics. J. Oncol. Pharm. Pract. 2017, 23, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, P.; Wallis, R. Dose-rounding of adjuvant chemotherapy for breast cancer: An audit of toxicity. J. Oncol. Pharm. Pract. 2010, 16, 251–255. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 355) | Pediatric (n = 147) | Adult (n = 206) | p-Value |
|---|---|---|---|---|
| n (Frequency %) | ||||
| Gender | 0.64 | |||
| Male | 215 (60.6) | 87 (40.7) | 127 (59.3) | |
| Female | 140 (39.4) | 60 (43.2) | 79 (56.8) | |
| Malignancies | 0.000 | |||
| Solid | 96 (27.0) | 69 (71.9) | 27 (28.1) | |
| Hematologic/lymphatic | 259 (73.0) | 78 (30.4) | 179 (69.6) | |
| Comorbidities * | 130 (36.6) | 23 (17.8) | 106 (82.2) | 0.000 |
| Comorbidities * | ||||
| Neurological | 18 (5.1) | 6 (33.3) | 12 (66.7) | 0.463 |
| Cardiovascular | 72 (20.3) | 7 (9.7) | 65 (90.3) | 0.000 |
| Respiratory | 15 (4.2) | 4 (26.7) | 11 (73.3) | 0.229 |
| Endocrinological | 56 (15.8) | 5 (8.9) | 51 (91.1) | 0.000 |
| Renal | 17 (4.8) | 1 (5.9) | 16 (94.1) | 0.002 |
| Other | 48 (13.5) | 6 (12.8) | 41 (87.2) | 0.000 |
| Total Comorbidities | 0.000 | |||
| 0 | 225 (63.5) | 124 (55.4) | 100 (44.6) | |
| 1 | 58 (16.3) | 18 (31.6) | 39 (68.4) | |
| 2 | 52 (14.6) | 4 (7.7) | 48 (92.3) | |
| 3 | 16 (4.5) | 1 (6.3) | 15 (93.8) | |
| 4 | 4 (1.1) | - | 4 (100) | |
| Parameters [Mean± SD] | ||||
| Age (years) * | 30.83 ± 26.6 | 5.32 ± 3.9 | 49.02 ± 20.1 | 0.000 |
| BMI * | 22.88 ± 7.7 | 16.68 ± 4.2 | 27.29 ± 6.5 | 0.000 |
| BSA * | 1.39 ± 0.6 | 0.80 ± 0.4 | 1.81 ± 0.3 | 0.000 |
| Hgb (g/L) * | 109.69 ± 23.8 | 104.22 ± 20.3 | 113.36 ± 25.4 | 0.000 |
| RBC (×109/L) * | 4.47 ± 5.7 | 4.11 ± 0.9 | 4.73 ± 7.4 | 0.326 |
| MCV (fL) * | 78.98 ± 12.3 | 76.60 ± 13.4 | 80.57 ± 11.3 | 0.003 |
| WBC (×109/L) * | 14.15 ± 34.3 | 16.41 ± 42.9 | 12.59 ± 26.6 | 0.306 |
| Neutrophil count (×109/L) * | 5.03 ± 4.6 | 4.71 ± 5.6 | 5.21 ± 3.9 | 0.337 |
| Lymphocyte count (×109/L) * | 4.14 ± 15.4 | 3.69 ± 3.6 | 4.47 ± 19.6 | 0.588 |
| NLR * | 4.54 ± 8.2 | 3.46 ± 9.4 | 5.19 ± 7.34 | 0.064 |
| Vit. D (nmol/L) * | 68.97 ± 75.1 | 68.80 ± 67.8 | 69.02 ± 77.3 | 0.993 |
| Vit. B12 * | 505.61 ± 459.2 | 350.2 ± 185.2 | 534.40 ± 481.4 | 0.161 |
| ALT (µ/L) * | 39.40 ± 84.2 | 31.56 ± 25.9 | 44.90 ± 106.9 | 0.153 |
| AST (µ/L) * | 38.56 ± 45.3 | 37.92 ± 27.4 | 38.95 ± 54.2 | 0.821 |
| Total Bilirubin (µmol/L) * | 11.28 ± 26.5 | 6.53 ± 7.0 | 14.54 ± 33.6 | 0.001 |
| Scr (µmol/L) * | 62.03 ± 62.5 | 35.45 ± 26.5 | 81.16 ± 73.2 | 0.000 |
| Characteristics | Variable/Occurrence | Neuropathy | p-Value | |
|---|---|---|---|---|
| Absent n (%) | Present n (%) | |||
| (a) | ||||
| Gender | M | 60 (69.0) | 27 (31.0) | 0.476 |
| F | 38 (63.3) | 22 (36.7) | ||
| Malignancy | Solid | 49 (71.0) | 20 (20.0) | 0.293 |
| Hematologic/lymphatic | 49 (62.8) | 29 (37.2) | ||
| Comorbidity | No | 85 (68.5) | 39 (31.5) | 0.261 |
| Yes | 13 (56.5) | 10 (43.5) | ||
| Comorbidities | ||||
| Neurological | No | 96 (68.1) | 45 (31.9) | 0.077 |
| Yes | 2 (33.3) | 4 (66.7) | ||
| Cardiovascular | No | 93 (66.4) | 47 (33.6) | 0.784 |
| Yes | 5 (66.7) | 2 (28.6) | ||
| Respiratory | No | 96 (67.1) | 47 (32.9) | 0.473 |
| Yes | 2 (50.0) | 2 (50.0) | ||
| Endocrinological | No | 95 (66.9) | 47 (33.1) | 0.748 |
| Yes | 3 (60.0) | 2 (40.0) | ||
| Renal | No | 97 (66.4) | 49 (33.6) | 0.478 |
| Yes | 1 (100.0) | 0 (0.0) | ||
| Others | No | 94 (66.7) | 47 (33.3) | 1.00 |
| Yes | 4 (66.7) | 2 (33.3) | ||
| Total comorbidity | 0 | 85 (68.5) | 39 (31.5) | 0.532 |
| 1 | 10 (55.6) | 8 (44.4) | ||
| 2 | 2 (50.0) | 2 (50.0) | ||
| 3 | 1 (100.0) | 0 (0.00) | ||
| Concurrent use of azole Antifungal | No | 97 (67.4) | 47 (32.6) | 0.216 |
| Yes | 1 (33.3) | 2 (66.7) | ||
| (b) | ||||
| Gender | M | 80 (63.0) | 47 (37.0) | 0.550 |
| F | 53 (67.1) | 26 (32.9) | ||
| Malignancy | Solid | 16 (59.3) | 11 (40.7) | 0.537 |
| Hematologic/lymphatic | 117 (65.4) | 62 (34.6) | ||
| Comorbidity | No | 69 (69.0) | 31 (31.0) | 0.196 |
| Yes | 64 (60.4) | 42 (39.6) | ||
| Comorbidities | ||||
| Neurological | No | 124 (63.9) | 70 (36.1) | 0.436 |
| Yes | 9 (75.0) | 4 (25.0) | ||
| Cardiovascular | No | 94 (66.7) | 47 (33.3) | 0.353 |
| Yes | 39 (60.0) | 26 (40.0) | ||
| Respiratory | No | 129 (66.2) | 66 (33.8) | 0.044 |
| Yes | 4 (36.4) | 7 (63.6) | ||
| Endocrinological | No | 107 (69.0) | 48 (31.0) | 0.019 |
| Yes | 26 (51.0) | 25 (49.0) | ||
| Renal | No | 121 (63.7) | 69 (36.3) | 0.363 |
| Yes | 12 (75.0) | 4 (25.0) | ||
| Others | No | 111 (67.3) | 54 (32.7) | 0.103 |
| Yes | 22 (53.7) | 19 (46.3) | ||
| Total comorbidity | 0 | 69 (69.0) | 31 (31.0) | 0.253 |
| 1 | 26 (66.7) | 13 (33.3) | ||
| 2 | 30 (62.5) | 18 (37.5) | ||
| 3 | 6 (40.0) | 9 (60.0) | ||
| 4 | 2 (50.0) | 2 (50.0) | ||
| Concurrent use of azole Antifungal | No | 128 (69.6) | 56 (30.4) | <0.001 |
| Yes | 5 (22.7) | 17 (77.3) | ||
| Parameter | Neuropathy | p-Value | |
|---|---|---|---|
| Absent | Present | ||
| Mean ± SD (n) | |||
| (a) | |||
| BMI | 16.4 ± 3.7 (98) | 17.3 ± 5.2 (49) | 0.220 |
| BSA | 0.76 ± 0.3 (98) | 0.89 ± 0.4 (49) | 0.038 |
| Hgb (g/L) * | 102.7 ± 21.8 (97) | 107.3 ± 16.5 (49) | 0.199 |
| RBC (×109/L) * | 4.11 ± 0.9 (96) | 4.1 ± 0.9 (48) | 0.84 |
| MCV (fL) * | 76.60 ± 13.8 (96) | 76.6 ± 12.6 (48) | 0.99 |
| WBC (×109/L) * | 16.8 ± 48.1 (97) | 15.6 ± 30.8 (49) | 0.875 |
| Neutrophil count (×109/L) * | 4.7 ± 5.6 (85) | 4.8 ± 5.5 (43) | 0.928 |
| Lymphocyte count (×109/L) * | 3.4 ± 2.6 (87) | 4.3 ± 4.9 (43) | 0.216 |
| NLR * | 3.8 ± 11.1 (85) | 2.7 ± 4.4 (43) | 0.533 |
| Vit. D (nmol/L) * | 79.3 ± 83.1 (7) | 50.4 ± 28.5 (4) | 0.525 |
| Vit.B12 * | 387.5 ± 190.9 (4) | 201.0 (1) | 0.447 |
| ALT (µ/L) * | 28.8 ± 20.4 (91) | 36.9 ± 33.9 (47) | 0.135 |
| AST (µ/L) * | 35.6 ± 22.9 (89) | 42.3 ± 34.2 (47) | 0.235 |
| Total Bilirubin (µmol/L) * | 5.5 ± 3.8 (92) | 8.6 ± 10.7 (46) | 0.062 |
| Scr (µmol/L) * | 32.2 ± 18.8 (93) | 41.6 ± 36.5 (49) | 0.044 |
| (b) | |||
| BMI * | 27.6 ± 6.7 (132) | 26.7 ± 6.0 (73) | 0.324 |
| BSA * | 1.8 ± 0.3 (132) | 1.8 ± 0.2 (73) | 0.291 |
| Hgb (g/L) | 115.4 ± 23.8 (133) | 109.7 ± 27.9 (73) | 0.128 |
| RBC (×109/L) * | 4.22 ± 0.9 (133) | 5.7 ± 12.5 (72) | 0.182 |
| MCV (fL) * | 81.2 ± 11.9 (133) | 79.5 ± 10.1 (72) | 0.324 |
| WBC (×109/L) * | 9.6 ± 14.68 (133) | 18.1 ± 39.75 (73) | 0.081 |
| Neutrophil count (×109/L) * | 4.9 ± 3.5 (129) | 5.8 ± 4.6 (69) | 0.110 |
| Lymphocyte count (×109/L) * | 2.9 ± 8.5 (128) | 7.3 ± 30.9 (70) | 0.136 |
| NLR * | 5.4 ± 8.00 (128) | 4.8 ± 6.1 (69) | 0.611 |
| Vit. D (nmol/L) * | 62.7 ± 83.5 (20) | 80.6 ± 70.8 (11) | 0.551 |
| Vit.B12 * | 403.9 ± 395.7 (14) | 674.9 ± 557.3 (13) | 0.155 |
| ALT (µ/L) * | 46.5 ± 129.7 (129) | 42.1 ± 46.5 (73) | 0.782 |
| AST (µ/L) * | 39.6 ± 59.2 (128) | 37.8 ± 44.9 (73) | 0.818 |
| Total Bilirubin (µmol/L) * | 16.5 ± 41.0 (131) | 11.0 ± 10.4 (72) | 0.260 |
| Scr (µmol/L) * | 84.4 ± 86.5 (124) | 75.4 ± 40.4 (69) | 0.419 |
| Nature of Dose Rounding | n (%) | Neuropathy | p-Value | |
|---|---|---|---|---|
| Absent n (%) | Present n (%) | |||
| (a) | ||||
| Rounding up ± no rounding | 28 (7.8) | 8 (28.6) | 20 (71.4) | <0.001 |
| Rounding down ± no rounding | 193 (54.3) | 142 (73.6) | 51 (26.4) | |
| No rounding at all | 34 (9.5) | 1 (2.9) | 33 (97.1) | |
| Mixed or missing | 100 (28.1) | 81 (81.0) | 19 (19.0) | |
| (b) | ||||
| Rounding up ± no rounding | 21 (14.2) | 5 (23.8) | 16 (76.2) | <0.001 |
| Rounding down ± no rounding | 57 (38.7) | 36 (63.2) | 21 (36.8) | |
| No rounding at all | 6 (4.0) | 1 (16.7) | 5 (83.3) | |
| Mixed or missing | 63 (42.8) | 56 (88.9) | 7 (11.1) | |
| (c) | ||||
| Rounding up ± no rounding | 7 (3.4) | 3 (42.9) | 4 (57.1) | <0.001 |
| Rounding down ± no rounding | 135 (65.5) | 105 (77.8) | 30 (22.2) | |
| No rounding at all | 28 (13.6) | 0 (0.0) | 28 (100) | |
| Mixed or missing | 36 (17.5) | 25 (69.4) | 11 (30.6) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alwhaibi, A.M.; Alshamrani, A.A.; Alenazi, M.A.; Altwalah, S.F.; Alameel, N.N.; Aljabali, N.N.; Alghamdi, S.B.; Bineid, A.I.; Alwhaibi, M.; Al Arifi, M.N. Vincristine-Induced Neuropathy in Patients Diagnosed with Solid and Hematological Malignancies: The Role of Dose Rounding. J. Clin. Med. 2023, 12, 5662. https://doi.org/10.3390/jcm12175662
Alwhaibi AM, Alshamrani AA, Alenazi MA, Altwalah SF, Alameel NN, Aljabali NN, Alghamdi SB, Bineid AI, Alwhaibi M, Al Arifi MN. Vincristine-Induced Neuropathy in Patients Diagnosed with Solid and Hematological Malignancies: The Role of Dose Rounding. Journal of Clinical Medicine. 2023; 12(17):5662. https://doi.org/10.3390/jcm12175662
Chicago/Turabian StyleAlwhaibi, Abdulrahman M., Ali A. Alshamrani, Miteb A. Alenazi, Shroog F. Altwalah, Nouf N. Alameel, Noura N. Aljabali, Sara B. Alghamdi, Abdulwahab I. Bineid, Monira Alwhaibi, and Mohamed N. Al Arifi. 2023. "Vincristine-Induced Neuropathy in Patients Diagnosed with Solid and Hematological Malignancies: The Role of Dose Rounding" Journal of Clinical Medicine 12, no. 17: 5662. https://doi.org/10.3390/jcm12175662