
Prognostic Impact of Modified H2FPEF Score in Patients Receiving Trans-Catheter Aortic Valve Replacement
 , , , and
, , , and
Abstract
:1. Background
2. Methods
2.1. Patient Selection
2.2. Calculation of H2FPEF Score
2.3. Other Baseline Characteristics
2.4. TAVR Procedure
2.5. Post-TAVR Course and Primary Outcome
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
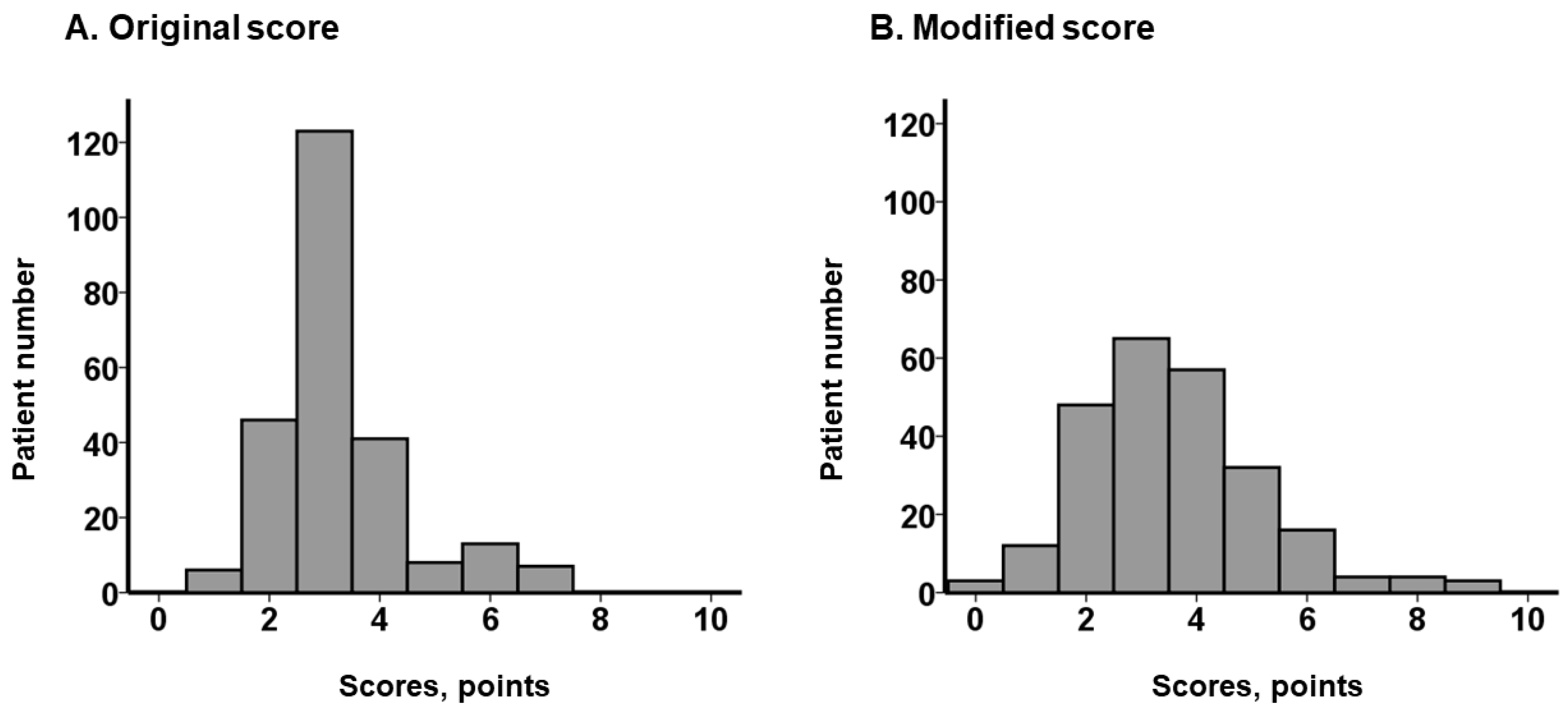
3.2. H2FPEF Score Calculation
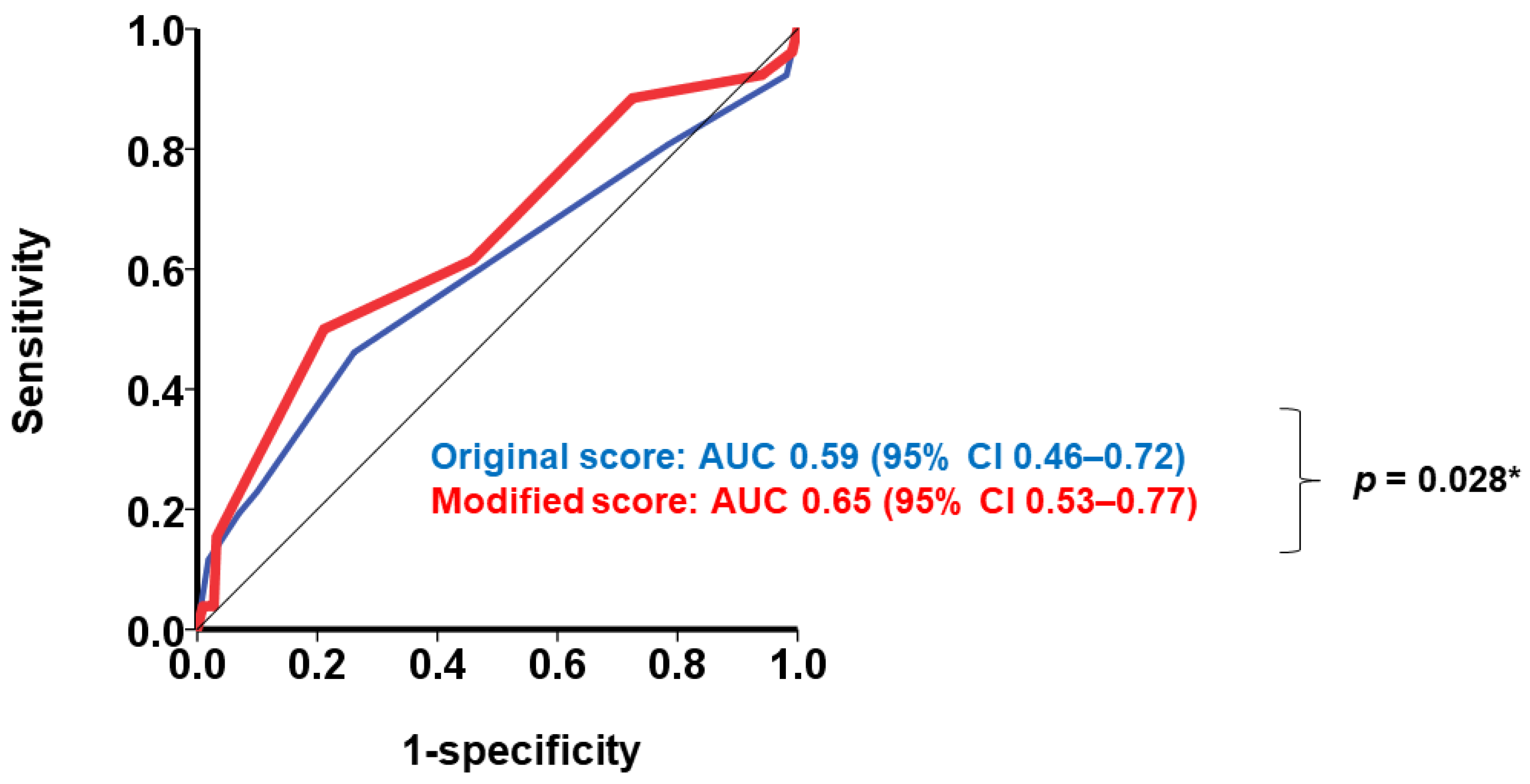
3.3. H2FPEF Score and Post-Procedural Clinical Outcome
3.4. Modified H2FPEF Score
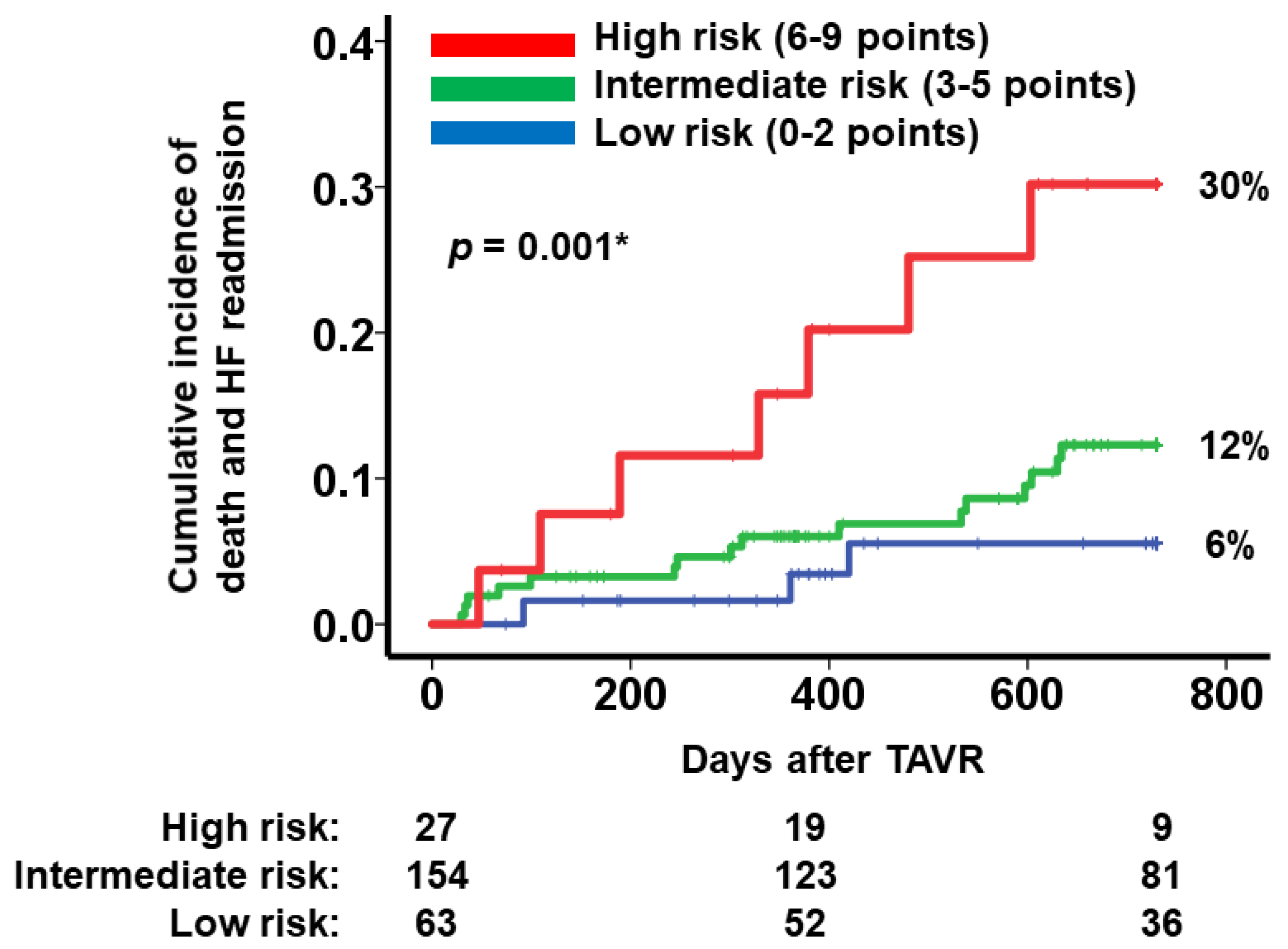
3.5. Prognostic Impact of the Modified H2FPEF Score
3.6. Stratification Using Modified H2FPEF Score
4. Discussion
4.1. HFpEF and H2FPEF Score
4.2. Prognostic Impact of H2FPEF Score
4.3. Clinical Implication of the Modified H2FPEF Score
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Osnabrugge, R.L.; Mylotte, D.; Head, S.J.; Van Mieghem, N.M.; Nkomo, V.T.; LeReun, C.M.; Bogers, A.J.; Piazza, N.; Kappetein, A.P. Aortic stenosis in the elderly: Disease prevalence and number of candidates for transcatheter aortic valve replacement: A meta-analysis and modeling study. J. Am. Coll. Cardiol. 2013, 62, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefevre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Kolte, D.; Vlahakes, G.J.; Palacios, I.F.; Sakhuja, R.; Passeri, J.J.; Inglessis, I.; Elmariah, S. Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients. J. Am. Coll. Cardiol. 2019, 74, 1532–1540. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef] [PubMed]
- Kalogeropoulos, A.S.; Redwood, S.R.; Allen, C.J.; Hurrell, H.; Chehab, O.; Rajani, R.; Prendergast, B.; Patterson, T. A 20-year journey in transcatheter aortic valve implantation: Evolution to current eminence. Front. Cardiovasc. Med. 2022, 9, 971762. [Google Scholar] [CrossRef] [PubMed]
- Tiyerili, V.; Sotemann, D.; Grothusen, C.; Eckel, C.; Becher, M.U.; Blumenstein, J.; Nef, H.; Mollmann, H. Latest Advances in Transcatheter Aortic Valve Implantation (2022). Surg. Technol. Int. 2022, 40, 221–225. [Google Scholar] [CrossRef]
- Achim, A.; Szucsborus, T.; Sasi, V.; Nagy, F.; Jambrik, Z.; Nemes, A.; Varga, A.; Homorodean, C.; Bertrand, O.F.; Ruzsa, Z. Safety and Feasibility of Distal Radial Balloon Aortic Valvuloplasty: The DR-BAV Study. JACC Cardiovasc. Interv. 2022, 15, 679–681. [Google Scholar] [CrossRef]
- Auffret, V.; Bakhti, A.; Leurent, G.; Bedossa, M.; Tomasi, J.; Belhaj Soulami, R.; Verhoye, J.P.; Donal, E.; Galli, E.; Loirat, A.; et al. Determinants and Impact of Heart Failure Readmission Following Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2020, 13, e008959. [Google Scholar] [CrossRef]
- Dayan, V.; Vignolo, G.; Magne, J.; Clavel, M.A.; Mohty, D.; Pibarot, P. Outcome and Impact of Aortic Valve Replacement in Patients With Preserved LVEF and Low-Gradient Aortic Stenosis. J. Am. Coll. Cardiol. 2015, 66, 2594–2603. [Google Scholar] [CrossRef]
- Ludwig, S.; Pellegrini, C.; Gossling, A.; Rheude, T.; Voigtlander, L.; Bhadra, O.D.; Linder, M.; Kalbacher, D.; Koell, B.; Waldschmidt, L.; et al. Prognostic value of the H(2) FPEF score in patients undergoing transcatheter aortic valve implantation. ESC Heart Fail. 2021, 8, 461–470. [Google Scholar] [CrossRef]
- Seoudy, H.; von Eberstein, M.; Frank, J.; Thomann, M.; Puehler, T.; Lutter, G.; Lutz, M.; Bramlage, P.; Frey, N.; Saad, M.; et al. HFA-PEFF score: Prognosis in patients with preserved ejection fraction after transcatheter aortic valve implantation. ESC Heart Fail. 2022, 9, 1071–1079. [Google Scholar] [CrossRef]
- Kvaslerud, A.B.; Gude, E.; Eriksen, G.; Andreassen, A.K.; Gullestad, L.; Broch, K. Diastolic Dysfunction Is Unmasked on Exercise in Patients With Asymptomatic, Severe Aortic Stenosis: An Invasive Hemodynamic Study. Circ. Heart Fail. 2022, 15, e009253. [Google Scholar] [CrossRef] [PubMed]
- Losi, M.A.; Izzo, R.; Stabile, E.; Sannino, A.; Canciello, G.; Giamundo, A.; Musella, F.; Cirillo, P.; Prastaro, M.; Galderisi, M.; et al. Diastolic dysfunction reduces stroke volume during daily’s life activities in patients with severe aortic stenosis. Int. J. Cardiol. 2015, 195, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Koifman, E.; Medvedofsky, D.; Didier, R.; Torguson, R.; Jerusalem, Z.; Kiramijyan, S.; Ben-Dor, I.; Wang, Z.; Goldstein, S.A.; Xu, L.; et al. Impact of Baseline Left Ventricular Diastolic Dysfunction in Patients With Severe Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2020, 125, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Sueta, D.; Yamamoto, E.; Nishihara, T.; Tokitsu, T.; Fujisue, K.; Oike, F.; Takae, M.; Usuku, H.; Takashio, S.; Arima, Y.; et al. H2FPEF Score as a Prognostic Value in HFpEF Patients. Am. J. Hypertens. 2019, 32, 1082–1090. [Google Scholar] [CrossRef]
- Redfield, M.M.; Borlaug, B.A. Heart Failure With Preserved Ejection Fraction: A Review. JAMA 2023, 329, 827–838. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Suzuki, S.; Kaikita, K.; Yamamoto, E.; Sueta, D.; Yamamoto, M.; Ishii, M.; Ito, M.; Fujisue, K.; Kanazawa, H.; Araki, S.; et al. H(2) FPEF score for predicting future heart failure in stable outpatients with cardiovascular risk factors. ESC Heart Fail. 2020, 7, 65–74. [Google Scholar] [CrossRef]
- Pedersen, A.L.D.; Povlsen, J.A.; Rasmussen, V.G.; Frederiksen, C.A.; Christiansen, E.H.; Terkelsen, C.J.; Vase, H.; Poulsen, S.H. Prognostic implications of residual left ventricular hypertrophy and systolic dysfunction in aortic stenosis following transcatheter aortic valve replacement. Int. J. Cardiovasc. Imaging 2023, 39, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Ueno, H.; Sobajima, M.; Kinugawa, K.; Watanabe, Y.; Yashima, F.; Tada, N.; Naganuma, T.; Yamawaki, M.; Yamanaka, F.; et al. Risk assessment in patients with left ventricular systolic dysfunction following transcatheter aortic valve replacement. J. Card. Surg. 2021, 36, 3673–3678. [Google Scholar] [CrossRef] [PubMed]
- Genereux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; Jaber, W.A.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Heart J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Tromp, J.; Teng, T.H.; Tay, W.T.; Hung, C.L.; Narasimhan, C.; Shimizu, W.; Park, S.W.; Liew, H.B.; Ngarmukos, T.; Reyes, E.B.; et al. Heart failure with preserved ejection fraction in Asia. Eur. J. Heart Fail. 2019, 21, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; Lam, C.S.P.; McMurray, J.J.V.; Redfield, M.M. How to Manage Heart Failure With Preserved Ejection Fraction: Practical Guidance for Clinicians. JACC Heart Fail. 2023, 11, 619–636. [Google Scholar] [CrossRef]
- Rao, V.N.; Zhao, D.; Allison, M.A.; Guallar, E.; Sharma, K.; Criqui, M.H.; Cushman, M.; Blumenthal, R.S.; Michos, E.D. Adiposity and Incident Heart Failure and its Subtypes: MESA (Multi-Ethnic Study of Atherosclerosis). JACC Heart Fail. 2018, 6, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, R.; Chamberlain, A.M.; Roger, V.L.; Redfield, M.M. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: A community-based study. Circulation 2013, 128, 1085–1093. [Google Scholar] [CrossRef]
- Kalich, B.A.; Allender, J.E.; Hollis, I.B. Medication Management of Patients Undergoing Transcatheter Aortic Valve Replacement. Pharmacotherapy 2018, 38, 122–138. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Sorimachi, H.; Harada, T.; Kagami, K.; Saito, Y.; Ishii, H. Epidemiology, Pathophysiology, Diagnosis, and Therapy of Heart Failure With Preserved Ejection Fraction in Japan. J. Card. Fail. 2023, 29, 375–388. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 244) | High Risk (n = 27) | Low and Intermediate Risk (n = 217) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 86 (82, 88) | 88 (86, 90) | 85 (81, 88) | <0.001 * |
| Male sex | 70 (29%) | 10 (37%) | 60 (28%) | 0.21 |
| Body mass index | 21.5 (19.1, 24.3) | 24.4 (21.8, 26.5) | 21.1 (19.0, 23.9) | 0.003 * |
| Systolic blood pressure, mmHg | 114 (105, 125) | 113 (103, 123) | 114 (105, 126) | 0.76 |
| Pulse rate, bpm | 71 (62, 77) | 70 (61, 73) | 71 (63, 78) | 0.71 |
| Comorbidity | ||||
| Hypertension | 178 (73%) | 24 (89%) | 154 (71%) | 0.039 * |
| Diabetes mellitus | 38 (16%) | 5 (19%) | 33 (15%) | 0.67 |
| Dyslipidemia | 116 (48%) | 10 (37%) | 106 (49%) | 0.16 |
| Atrial fibrillation | 25 (10%) | 17 (63%) | 8 (4%) | <0.001 * |
| Coronary heart disease | 63 (26%) | 5 (19%) | 58 (27%) | 0.24 |
| Peripheral artery disease | 52 (21%) | 8 (30%) | 44 (20%) | 0.2 |
| History of heart failure admission | 98 (40%) | 17 (63%) | 81 (37%) | 0.011 * |
| History of cardiac surgery | 12 (5%) | 1 (4%) | 11 (5%) | 0.75 |
| History of stroke | 33 (14%) | 6 (22%) | 27 (12%) | 0.18 |
| Laboratory data | ||||
| Serum albumin, g/dL | 3.8 (3.5, 4.0) | 3.8 (3.5, 3.9) | 3.8 (3.5, 4.0) | 0.99 |
| Hemoglobin, g/dL | 11.4 (10.0, 12.5) | 10.5 (10.0, 12.6) | 11.4 (10.0, 12.5) | 0.87 |
| Serum sodium, mEq/L | 140 (139, 142) | 141 (138, 143) | 140 (139, 142) | 0.64 |
| eGFR, mL/min/m2 | 49 (37, 62) | 45 (29, 51) | 50 (38, 64) | 0.14 |
| Plasma BNP, pg/mL | 218 (118, 530) | 184 (144, 495) | 223 (114, 554) | 0.85 |
| Echocardiography | ||||
| LVDd, mm | 46 (41, 51) | 47 (44, 51) | 45 (41, 50) | 0.28 |
| LVEF, % | 64 (54, 70) | 61 (53, 69) | 65 (54, 70) | 0.27 |
| LVEF <40% | 20 (8%) | 1 (4%) | 19 (8%) | 0.37 |
| Left atrial diameter, mm | 43 (38, 50) | 50 (45, 56) | 43 (37, 48) | <0.001 * |
| Aortic valve parameter | ||||
| Peak velocity, m/s | 4.4 (4.0, 4.9) | 4.2 (3.8, 4.5) | 4.5 (4.0, 4.9) | 0.013 * |
| Mean pressure gradient, mmHg | 46 (38, 57) | 40 (34, 45) | 47 (39, 59) | 0.002 * |
| Valve area, cm2 | 0.6 (0.4, 0.7) | 0.6 (0.5, 0.7) | 0.5 (0.4, 0.7) | 0.27 |
| Moderate or greater MR | 19 (8%) | 5 (19%) | 14 (6%) | 0.027 * |
| Moderate or greater AR | 22 (9%) | 3 (11%) | 19 (9%) | 0.69 |
| Moderate or greater TR | 11 (5%) | 5 (19%) | 6 (3%) | <0.001 * |
| E/e’ ratio | 16.3 (12.4, 23.1) | 17.5 (12.5, 20.5) | 16.1 (12.4, 23.3) | 0.92 |
| RVSP, mmHg | 31 (26, 37) | 39 (36, 43) | 30 (25, 35) | <0.001 * |
| Medication | ||||
| Beta-blocker | 74 (30%) | 7 (26%) | 67 (31%) | 0.39 |
| Renin-angiotensin system inhibitor | 152 (62%) | 16 (59%) | 136 (63%) | 0.44 |
| Mineralocorticoid receptor antagonist | 71 (29%) | 7 (26%) | 64 (29%) | 0.45 |
| Diuretics | 133 (55%) | 19 (70%) | 114 (52%) | 0.059 |
| Scores | ||||
| STS score | 5.2 (4.1, 7.4) | 5.9 (4.5, 7.7) | 5.2 (4.0, 7.4) | 0.32 |
| Modified H2FPEF score | 3 (2, 4) | 6 (6, 8) | 3 (2, 4) | <0.001 * |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| Age, years | 1.06 (0.97–1.15) | 0.19 | ||
| Male sex | 3.23 (1.49–7.14) | 0.003 * | 3.33 (1.51–7.14) | 0.003 * |
| Body mass index | 1.02 (1.00–1.03) | 0.008 * | 1.02 (1.00–1.03) | 0.016 * |
| Serum albumin, g/dL | 0.47 (0.20–1.12) | 0.088 | ||
| eGFR, mL/min/1.73 m2 | 0.99 (0.97–1.01) | 0.44 | ||
| Common logarithm of plasma BNP, pg/mL | 1.58 (0.69–3.64) | 0.28 | ||
| LVEF, % | 1.01 (0.98–1.04) | 0.58 | ||
| Heart failure history | 1.89 (0.87–4.12) | 0.11 | ||
| Atrial fibrillation | 2.36 (0.89–6.25) | 0.085 | ||
| Modified H2FPEF score, points | 1.30 (1.06–1.58) | 0.010 * | 1.22 (1.01–1.49) | 0.047 * |
| High Risk (n = 27) | Low and Intermediate Risk (n = 217) | p Value | |
|---|---|---|---|
| Bod mass index > 23 | 18 (67%) | 72 (33%) | 0.001 * |
| Hypertension | 24 (89%) | 154 (71%) | 0.034 * |
| Atrial fibrillation | 17 (63%) | 8 (4%) | <0.001 * |
| RVSP > 35 mmHg | 20 (74%) | 49 (23%) | <0.001 * |
| Age > 84 years | 26 (96%) | 118 (54%) | <0.001 * |
| E/e’ ratio > 9 | 26 (96%) | 202 (93%) | 0.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akao, K.; Imamura, T.; Tanaka, S.; Onoda, H.; Ushijima, R.; Sobajima, M.; Fukuda, N.; Ueno, H.; Kinugawa, K. Prognostic Impact of Modified H2FPEF Score in Patients Receiving Trans-Catheter Aortic Valve Replacement. J. Clin. Med. 2023, 12, 5396. https://doi.org/10.3390/jcm12165396
Akao K, Imamura T, Tanaka S, Onoda H, Ushijima R, Sobajima M, Fukuda N, Ueno H, Kinugawa K. Prognostic Impact of Modified H2FPEF Score in Patients Receiving Trans-Catheter Aortic Valve Replacement. Journal of Clinical Medicine. 2023; 12(16):5396. https://doi.org/10.3390/jcm12165396
Chicago/Turabian StyleAkao, Kousuke, Teruhiko Imamura, Shuhei Tanaka, Hiroshi Onoda, Ryuichi Ushijima, Mitsuo Sobajima, Nobuyuki Fukuda, Hiroshi Ueno, and Koichiro Kinugawa. 2023. "Prognostic Impact of Modified H2FPEF Score in Patients Receiving Trans-Catheter Aortic Valve Replacement" Journal of Clinical Medicine 12, no. 16: 5396. https://doi.org/10.3390/jcm12165396