
DOACs in the Anticoagulation of Mechanical Valves: A Systematic Review and Future Perspectives
 , ,
, ,
Abstract
:1. Introduction
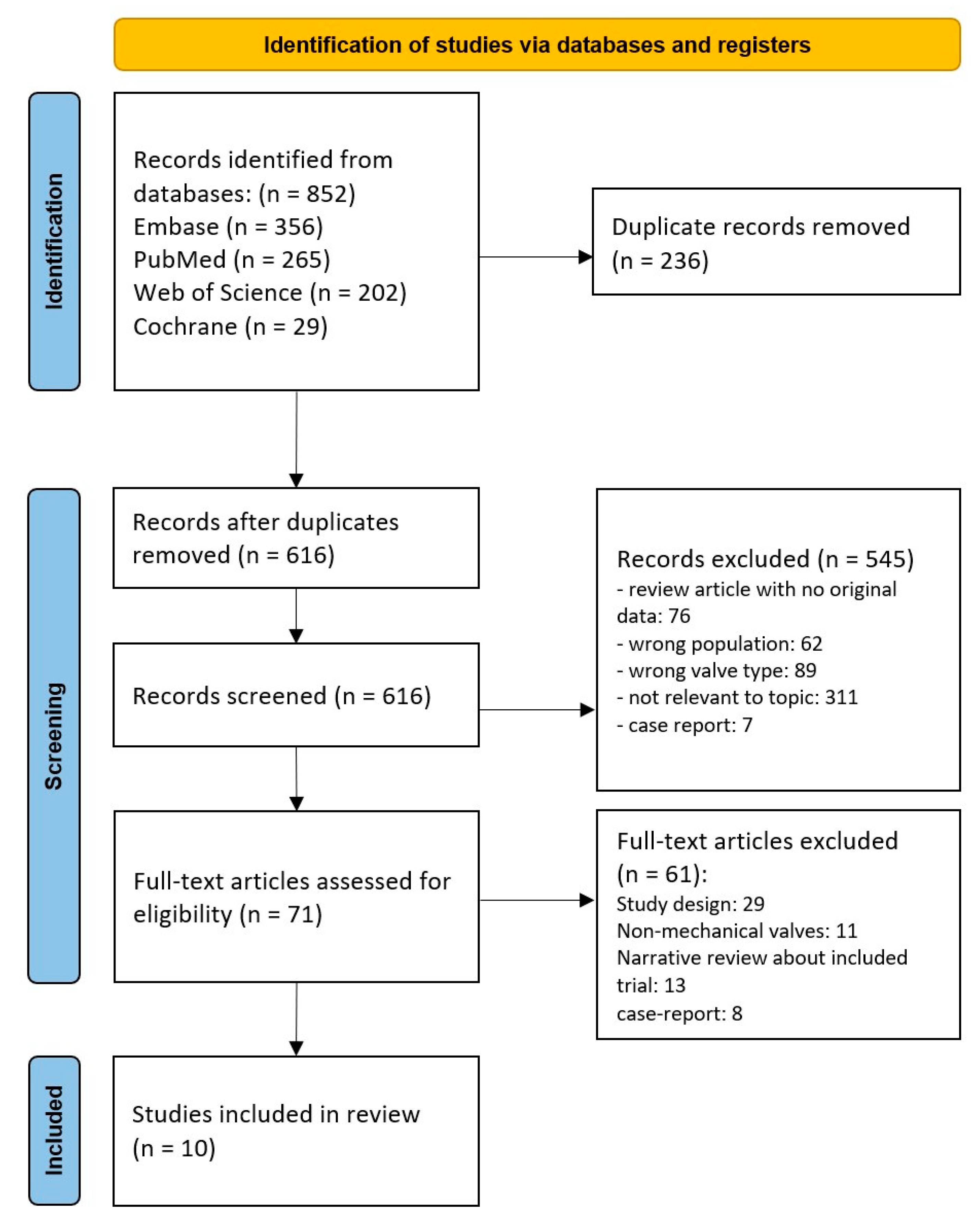
2. Materials and Methods
3. Results
3.1. Mechanism of Thrombosis in Mechanical Heart Valves
3.1.1. Surface-Related Factors
3.1.2. Hemodynamic Factors
3.1.3. Hemostasis-Related Factors
3.2. Mechanical Heart Valve Anticoagulation with DOACs: Animal and Human Studies
3.2.1. Dabigatran
3.2.2. Rivaroxaban
3.2.3. Apixaban
3.2.4. Edoxaban
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zühlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.T.; Boler, A.; Medina-Inojosa, J.R.; Scott, C.G.; Maurer, M.J.; Eleid, M.F.; Enriquez-Sarano, M.; Tribouilloy, C.; Michelena, H.I. Aortic Stenosis Progression, Cardiac Damage, and Survival: Comparison Between Bicuspid and Tricuspid Aortic Valves. JACC Cardiovasc. Imaging 2021, 14, 1113–1126. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.C.; Davidson, M.J.; Lamy, A.; Eikelboom, J.W. Antithrombotic management of patients with prosthetic heart valves: Current evidence and future trends. Lancet 2009, 374, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Durães, A.R.; Bitar, Y.D.S.; Lima, M.L.G.; Santos, C.C.; Schonhofen, I.S.; Filho, J.A.L.; Roever, L. Usefulness and Safety of Rivaroxaban in Patients Following Isolated Mitral Valve Replacement with a Mechanical Prosthesis. Am. J. Cardiol. 2018, 122, 1047–1050. [Google Scholar] [CrossRef]
- Ouzounian, M.; Mazine, A.; David, T.E. The Ross procedure is the best operation to treat aortic stenosis in young and middle-aged adults. J. Thorac. Cardiovasc. Surg. 2017, 154, 778–782. [Google Scholar] [CrossRef] [Green Version]
- Lester, P.A.; Coleman, D.M.; Diaz, J.A.; Jackson, T.O.; Hawley, A.E.; Mathues, A.R.; Grant, B.T.; Knabb, R.M.; Ramacciotti, E.; Frost, C.E.; et al. Apixaban Versus Warfarin for Mechanical Heart Valve Thromboprophylaxis in a Swine Aortic Heterotopic Valve Model. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 942–948. [Google Scholar] [CrossRef]
- Carrel, T.; Dembitsky, W.P.; de Mol, B.; Obrist, D.; Dreyfus, G.; Meuris, B.; Vennemann, B.; Lapeyre, D.; Schaff, H. Non-physiologic closing of bi-leaflet mechanical heart prostheses requires a new tri-leaflet valve design. Int. J. Cardiol. 2020, 304, 125–127. [Google Scholar] [CrossRef] [Green Version]
- Scotten, L.; Siegel, R. Importance of shear in prosthetic valve closure dynamics. J. Heart Valve Dis. 2011, 20, 664–672. [Google Scholar]
- Hylek, E.M. Complications of oral anticoagulant therapy: Bleeding and nonbleeding, rates and risk factors. Semin. Vasc. Med. 2003, 3, 271–278. [Google Scholar]
- Mekaj, A.Y.; Mekaj, Y.H.; Duci, S.B.; Miftari, E. New oral anticoagulants: Their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events. Ther. Clin. Risk Manag. 2015, 11, 967–977. [Google Scholar] [CrossRef] [Green Version]
- Levi, M. Self-management of anticoagulation. Expert Rev. Cardiovasc. Ther. 2008, 6, 979–985. [Google Scholar] [CrossRef]
- erret, L.; Couturier, J.; Rozon, A.; Saudrais-Janecek, S.; St-Onge, A.; Nguyen, A.; Basmadjian, A.; Tremblay, S.; Brouillette, D.; de Denus, S. Impact of a pharmacist-led warfarin self-management program on quality of life and anticoagulation control: A randomized trial. Pharmacotherapy 2012, 32, 871–879. [Google Scholar] [CrossRef]
- Tan, C.S.S.; Lee, S.W.H. Warfarin and food, herbal or dietary supplement interactions: A systematic review. Br. J. Clin. Pharmacol. 2021, 87, 352–374. [Google Scholar] [CrossRef]
- Harter, K.; Levine, M.; Henderson, S.O. Anticoagulation drug therapy: A review. West J. Emerg. Med. 2015, 16, 11–17. [Google Scholar] [CrossRef]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar]
- Gerfer, S.; Grandoch, M.; Wahlers, T.C.; Kuhn, E.W. Factor Xa Inhibitors for Patients after Mechanical Heart Valve Replacement? Thorac. Cardiovasc. Surg. 2021, 71, 189–194. [Google Scholar] [CrossRef]
- McKellar, S.H.; Abel, S.; Camp, C.L.; Suri, R.M.; Ereth, M.H.; Schaff, H.V. Effectiveness of dabigatran etexilate for thromboprophylaxis of mechanical heart valves. J. Thorac. Cardiovasc. Surg. 2011, 141, 1410–1416. [Google Scholar] [CrossRef] [Green Version]
- Schomburg, J.L.; Medina, E.M.; Lahti, M.T.; Bianco, R.W. Dabigatran versus Warfarin after Mechanical Mitral Valve Replacement in the Swine Model. J. Investig. Surg. 2012, 25, 150–155. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Brueckmann, M.; van de Werf, F. Dabigatran versus warfarin in patients with mechanical heart valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [Green Version]
- Greiten, L.E.; McKellar, S.H.; Rysavy, J.; Schaff, H.V. Effectiveness of rivaroxaban for thromboprophylaxis of prosthetic heart valves in a porcine heterotopic valve model. Eur. J. Cardio-Thorac. Surg. 2014, 45, 914–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roost, E.; Weber, A.; Alberio, L.; Englberger, L.; Reineke, D.; Keller, D.; Nagler, M.; Carrel, T. Rivaroxaban in patients with mechanical heart valves: A pilot study. Thromb. Res. 2020, 186, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Durães, A.R.; Bitar, Y.D.S.L.; Schonhofen, I.S.; Travassos, K.S.O.; Pereira, L.V.; Filho, J.A.L.; Neto, M.G.; Junior, R.A.; Roever, L. Rivaroxaban Versus Warfarin in Patients with Mechanical Heart Valves: Open-Label, Proof-of-Concept trial-The RIWA study. Am. J. Cardiovasc. Drugs 2020, 21, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Van Hoof, L.; Truyers, I.; Van Hauwermeiren, H.; Nachtergaele, B.; Langenaeken, T.; Jacquemin, M.; Rega, F.; Verhamme, P.; Meuris, B. Apixaban in a porcine model of mechanical valve thrombosis in pulmonary position-a pilot study. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac070. [Google Scholar] [CrossRef]
- Artivion Stops Clinical Trial for On-X Mechanical Valve. Available online: https://www.heart-valve-surgery.com/heart-surgery-blog/2022/10/05/proact-xa-clinical-trial-stopped/ (accessed on 3 April 2023).
- Jaffer, I.H.; Fredenburgh, J.C.; Hirsh, J.; Weitz, J.I. Medical device-induced thrombosis: What causes it and how can we prevent it? J. Thromb. Haemost. 2015, 13, S72–S81. [Google Scholar] [CrossRef]
- Turbill, P.; Beugeling, T.; Poot, A. Proteins involved in the Vroman effect during exposure of human blood plasma to glass and polyethylene. Biomaterials 1996, 17, 1279–1287. [Google Scholar] [CrossRef]
- Chaudhry, R.; Usama, S.M.; Babiker, H.M. Physiology, Coagulation Pathways; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Aimo, A.; Giugliano, R.P.; De Caterina, R. Non-Vitamin K Antagonist Oral Anticoagulants for Mechanical Heart Valves: Is the Door Still Open? Circulation 2018, 138, 1356–1365. [Google Scholar] [CrossRef]
- Noble, S.; Asgar, A.; Cartier, R.; Virmani, R.; Bonan, R. Anatomo-pathological analysis after CoreValve Revalving system implantation. EuroIntervention 2009, 5, 78–85. [Google Scholar] [CrossRef]
- Wolberg, A.S.; Aleman, M.M.; Leiderman, K.; Machlus, K.R. Procoagulant activity in hemostasis and thrombosis: Virchow’s triad revisited. Anesth. Analg. 2012, 114, 275–285. [Google Scholar] [CrossRef] [Green Version]
- Dasi, L.P.; Simon, H.A.; Sucosky, P.; Yoganathan, A.P. Fluid mechanics of artificial heart valves. Clin Exp Pharmacol Physiol. 2009, 36, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Salleh, N.M.; Zakaria, M.S.; Abd Latif, M.J. Reducing of Thrombosis in Mechanical Heart Valve through the Computational Method: A Review. J. Adv. Res. Fluid Mech. Therm. Sci. 2020, 65, 178–200. [Google Scholar]
- Dangas, G.D.; Weitz, J.I.; Giustino, G.; Makkar, R.; Mehran, R. Prosthetic Heart Valve Thrombosis. J. Am. Coll. Cardiol. 2016, 68, 2670–2689. [Google Scholar] [CrossRef]
- Roudaut, R.; Serri, K.; Lafitte, S. Thrombosis of prosthetic heart valves: Diagnosis and therapeutic considerations. Heart 2007, 93, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Gencbay, M.; Turan, F.; Degertekin, M.; Eksi, N.; Mutlu, B.; Unalp, A. High prevalence of hypercoagulable states in patients with recurrent thrombosis of mechanical heart valves. J. Heart Valve Dis. 1998, 7, 601–609. [Google Scholar]
- Seiler, C. Management and follow up of prosthetic heart valves. Heart 2004, 90, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Gayle, J.A.; Kaye, A.D.; Kaye, A.M.; Shah, R. Anticoagulants: Newer ones, mechanisms, and perioperative updates. Anesthesiol. Clin. 2010, 28, 667–679. [Google Scholar] [CrossRef]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Van Es, N.; Coppens, M.; Schulman, S.; Middeldorp, S.; Büller, H.R. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: Evidence from phase 3 trials. Blood 2014, 124, 1968–1975. [Google Scholar] [CrossRef]
- McKellar, S.H.; Thompson, J.L.; Schaff, H.V. A model of heterotopic aortic valve replacement for studying thromboembolism prophylaxis in mechanical valve prostheses. J. Surg. Res. 2007, 141, 1–6. [Google Scholar] [CrossRef]
- McKellar, S.H.; Thompson, J.L.; Garcia-Rinaldi, R.F.; MacDonald, R.J.; Sundt, T.M.; Schaff, H.V. Short- and long-term efficacy of aspirin and clopidogrel for thromboprophylaxis for mechanical heart valves: An in vivo study in swine. J. Thorac. Cardiovasc. Surg. 2008, 136, 908–914. [Google Scholar] [CrossRef] [Green Version]
- Olsen, A.K.; Hansen, A.K.; Jespersen, J.; Marckmann, P.; Bladbjerg, E.M. The pig as a model in blood coagulation and fibrinolysis research. Scand. J. Lab. Anim. Sci. 1999, 26, 214–224. [Google Scholar]
- Antonijevic, N.M.; Zivkovic, I.D.; Jovanovic, L.M.; Matic, D.M.; Kocica, M.J.; Mrdovic, I.B.; Kanjuh, V.I.; Culafic, M.D. Dabigatran—Metabolism, Pharmacologic Properties and Drug Interactions. Curr. Drug Metab. 2017, 18, 622–635. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maegdefessel, L.; Linde, T.; Krapiec, F.; Hamilton, K.; Steinseifer, U.; van Ryn, J.; Raaz, U.; Buerke, M.; Werdan, K.; Schlitt, A. In vitro comparison of dabigatran, unfractionated heparin, and low-molecular-weight heparin in preventing thrombus formation on mechanical heart valves. Thromb. Res. 2010, 126, e196–e200. [Google Scholar] [CrossRef]
- Jaffer, I.H.; Stafford, A.R.; Fredenburgh, J.C.; Whitlock, R.P.; Chan, N.C.; Weitz, J.I. Dabigatran is Less Effective Than Warfarin at Attenuating Mechanical Heart Valve-Induced Thrombin Generation. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2015, 4, e002322. [Google Scholar] [CrossRef] [Green Version]
- Desai, J.; Kolb, J.M.; Weitz, J.I.; Aisenberg, J. Gastrointestinal bleeding with the new oral anticoagulants—Defining the issues and the management strategies. Thromb. Haemost. 2013, 110, 205–212. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Kwong, L.M. Therapeutic potential of rivaroxaban in the prevention of venous thromboembolism following hip and knee replacement surgery: A review of clinical trial data. Vasc. Health Risk Manag. 2011, 7, 461–466. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, D.M.; O’Connell, N.M.; O’Donnell, J.S.; Path, F.R. Oral rivaroxaban for pulmonary embolism. N. Engl. J. Med. 2012, 366, 2525. [Google Scholar]
- Friedman, R.J. Novel oral anticoagulants for VTE prevention in orthopedic surgery: Overview of phase 3 trials. Orthopedics 2011, 34, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Emery, R.W.; Van Nooten, G.J.; Tesar, P.J. The initial experience with the ATS Medical mechanical cardiac valve prosthesis. Ann. Thorac. Surg. 2003, 75, 444–452. [Google Scholar] [CrossRef]
- Kelly, S.; Verdonck, P.; Vierendeels, J.; Riemslagh, K.; Dick, E.; Van Nooten, G. A Three-dimensional Analysis of Flow in the Pivot Regions of an ATS Bileaflet Valve. Int. J. Artif. Organs 1999, 22, 754–763. [Google Scholar] [CrossRef]
- Jaffer, I.H.; Weitz, J.I. Antithrombotic Drugs. In Hematology: Basic Principles and Practice; Elsevier: Amsterdam, The Netherlands, 2018; pp. 2168–2188. [Google Scholar]
- Byon, W.; Garonzik, S.; Boyd, R.A.; Frost, C.E. Apixaban: A Clinical Pharmacokinetic and Pharmacodynamic Review. Clin. Pharmacokinet. 2019, 58, 1265–1279. [Google Scholar] [CrossRef] [Green Version]
- Poulakos, M.; Walker, J.N.; Baig, U.; David, T. Edoxaban: A direct oral anticoagulant. Am. J. Health-Syst. Pharm. 2017, 74, 117–129. [Google Scholar] [CrossRef]
- Chen, A.; Stecker, E.; Warden, B.A. Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges. J. Am. Heart Assoc. 2020, 9, 17559. [Google Scholar] [CrossRef]
- Meuris, B.; Verbeken, E.; Flameng, W. Mechanical valve thrombosis in a chronic animal model: Differences between monoleaflet and bileaflet valves. J. Heart Valve Dis. 2005, 14, 96–104. [Google Scholar]
- Cohen, A.T.; Hill, N.R.; Luo, X.; Masseria, C.; Abariga, S.A.; Ashaye, A.O. A systematic review of network meta-analyses among patients with nonvalvular atrial fibrillation: A comparison of efficacy and safety following treatment with direct oral anticoagulants. Int. J. Cardiol. 2018, 269, 174–181. [Google Scholar] [CrossRef]
- Lau, W.C.; Torre, C.O.; Man, K.K.; Stewart, H.M.; Seager, S.; Van Zandt, M.; Reich, C.; Li, J.; Brewster, J.; Lip, G.Y.; et al. Comparative Effectiveness and Safety Between Apixaban, Dabigatran, Edoxaban, and Rivaroxaban Among Patients with Atrial Fibrillation: A Multinational Population-Based Cohort Study. Ann. Intern Med. 2022, 175, 1515–1524. [Google Scholar] [CrossRef]
- Jawitz, O.K.; Wang, T.Y.; Lopes, R.D.; Chavez, A.; Boyer, B.; Kim, H.; Anstrom, K.J.; Becker, R.C.; Blackstone, E.; Ruel, M.; et al. Rationale and design of PROACT Xa: A randomized, multicenter, open-label, clinical trial to evaluate the efficacy and safety of apixaban versus warfarin in patients with a mechanical On-X Aortic Heart Valve. Am. Heart J. 2020, 227, 91–99. [Google Scholar] [CrossRef]
- Wang, T.Y.; Svensson, L.G.; Wen, J.; Vekstein, A.; Gerdisch, M.; Rao, V.U.; Moront, M.; Johnston, D.; Lopes, R.D.; Chavez, A.; et al. Apixaban or Warfarin in Patients with an On-X Mechanical Aortic Valve. NEJM Evid. 2023, 2, 7. [Google Scholar] [CrossRef]
- Wu, Y.; Butchart, E.G.; Borer, J.S.; Yoganathan, A.; Grunkemeier, G.L. Clinical Evaluation of New Heart Valve Prostheses: Update of Objective Performance Criteria. Ann. Thorac. Surg. 2014, 98, 1865–1874. [Google Scholar] [CrossRef] [PubMed]
- Puskas, J.; Gerdisch, M.; Nichols, D.; Quinn, R.; Anderson, C.; Rhenman, B.; Fermin, L.; McGrath, M.; Kong, B.; Hughes, C.; et al. Reduced anticoagulation after mechanical aortic valve replacement: Interim results from the prospective randomized on-X valve anticoagulation clinical trial randomized Food and Drug Administration investigational device exemption trial. J. Thorac. Cardiovasc. Surg. 2014, 147, 1202–1211.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DIrect Oral Anticoagulation and mechaNical Aortic Valve—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT05687448 (accessed on 14 June 2023).
- Caldeira, D.; David, C.; Santos, A.T.; Costa, J.; Pinto, F.J.; Ferreira, J.J. Efficacy and safety of low molecular weight heparin in patients with mechanical heart valves: Systematic review and meta-analysis. J. Thromb. Haemost. 2014, 12, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Heras, M.; Chesebro, J.H.; Fuster, V.; Penny, W.J.; Grill, D.E.; Bailey, K.R.; Danielson, G.K.; Orszulak, T.A.; Pluth, J.R.; Puga, F.J.; et al. High risk of thromboemboli early after bioprosthetic cardiac valve replacement. J. Am. Coll. Cardiol. 1995, 25, 1111–1119. [Google Scholar] [CrossRef] [Green Version]
- Torella, M.; Aquila, I.; Chiodini, P.; Amarelli, C.; Romano, G.; Della Ratta, E.E.; De Feo, M.; Della Corte, A.; Indolfi, C.; Torella, D.; et al. Low-dose anticoagulation after isolated mechanical aortic valve replacement with Liva Nova Bicarbon prosthesis: A post hoc analysis of LOWERING-IT Trial. Sci. Rep. 2018, 8, 8405. [Google Scholar] [CrossRef] [Green Version]
- Larsson, M.; Rayzman, V.; Nolte, M.W.; Nickel, K.F.; Björkqvist, J.; Jämsä, A.; Hardy, M.P.; Fries, M.; Schmidbauer, S.; Hedenqvist, P.; et al. A factor XIIa inhibitory antibody provides thromboprotection in extracorporeal circulation without increasing bleeding risk. Sci. Transl. Med. 2014, 6, 222ra17. [Google Scholar] [CrossRef] [Green Version]
- Gallegos, R.P.; Rivard, A.L.; Suwan, P.T.; Black, S.; Bertog, S.; Steinseifer, U.; Armien, A.; Lahti, M.; Bianco, R. In-vivo experience with the Triflo trileaflet mechanical heart valve. J. Heart Valve Dis. 2006, 15, 791–799. [Google Scholar]
- Bruecker, C.; Li, Q. Possible Early Generation of Physiological Helical Flow Could Benefit the Triflo Trileaflet Heart Valve Prosthesis Compared to Bileaflet Valves. Bioengineering 2020, 7, 158. [Google Scholar] [CrossRef]


{kind=link}
| Reference | S. McKellar et al. (2011) [18] | J. Schomburg et al. (2012) [19] | J.W. Eikelboom et al. (2013) [20] |
|---|---|---|---|
| Setting | Swine heterotopic aorta descendens valve conduit | Swine mitral valve replacement | Human aortic- or mitral-valve replacement: -within the past 7 days -replacement at least 3 months earlier |
| Treatment groups | 10 swine: dabigatran 10 swine: enoxaparin 10 swine: no anticoagulation | 3 swine: no anticoagulation 5 swine: warfarin 11 swine: dabigatran | 84 patients: warfarin 168 patients: dabigatran |
| Dose | Enoxaparin 2 mg/kg BID SC Dabigatran 20 mg/kg BID PO | Warfarin INR 2–2.5 PO Dabigatran 20 mg/kg BID PO | Warfarin INR 2–3/2.5–3.5 * PO Dabigatran 20 mg/kg BID PO ** |
| Primary endpoint | Amount of valve thrombus at 30 days. | Animal survival at 90 days. | Trough plasma level of dabigatran |
| Results | 1 premature death in no anticoagulation group due to sepsis | Survival: -No anticoagulation: 18.7 days -Warfarin: 15.6 days -Dabigatran: 50.3 days | Terminated prematurely due to excess thromboembolic and bleeding events in the dabigatran group |
| Valve thrombus | No anticoagulation: 638 ± 895 mg Enoxaparin: 121 ± 128 mg Dabigatran: 19 ± 31 mg | 2/3 control group 2/5 warfarin group 8/10 dabigatran group | N/A |
| Bleeding | None observed | 2/5 warfarin group (hemopericardium) 2/10 dabigatran group | Any: dabigatran 27% vs. 12% warfarin (HR: 2.45 (1.23–4.86)) Major: dabigatran 4% vs. 2% warfarin (HR: 1.76 (0.36–8.46)) |
| Stroke | N/A | N/A | Dabigatran: 9 patients (5%) Warfarin: 0 patients (0%) |
| Myocardial infarction | N/A | N/A | Dabigatran: 3 patients (2%) Warfarin: 0 patients (0%) |
| Dabigatran level | N/A | N/A | Dabigatran 86% time in therapeutic range vs. warfarin 49–51% time in therapeutic range |
| Conclusion | Lowest thrombi weight in the dabigatran group. | Mortality benefit of dabigatran over warfarin or no anticoagulation. | The use of dabigatran in patients with mechanical heart valves was associated with increased rates of thromboembolic and bleeding complications, as compared with warfarin. |
| Reference | L. E. Greiten et al. (2014) [21] | A. R. Durães et al. (2018) [4] | Roost et al. (2020) [22] | A. R. Durães et al. (2020) [23] |
|---|---|---|---|---|
| Setting | Swine heterotopic descending aorta valve conduit | Human-isolated mitral valve replacement > 3 months postoperatively | Human mechanical aortic valve replacement | Human aortic, mitral, or both valve replacement > 3 months postoperatively. |
| Treatment groups | 10 swine: rivaroxaban 10 swine: enoxaparin 10 swine: no anticoagulation | 7 patients No control group | 10 patients No control group | 23 rivaroxaban: 12 mitral, 6 aortic, 5 both 21 warfarin: 14 mitral, 2 aortic, 5 both |
| Valves used | St. Jude Masters Series (St. Jude Medical, Inc., St. Paul, MN, USA) | Not specified | Medtronic Open Pivot | Not specified |
| Dose | Enoxaparin 2 mg/kg BID SC Rivaroxaban 2 mg/kg BID PO | Rivaroxaban 15 mg BID PO | Rivaroxaban 20 mg OD PO | Rivaroxaban 15 mg BID PO Warfarin INR 2–3/2.5–3.5 * PO |
| Primary endpoint | Amount of valve thrombus at 30 days. | Adverse events of any kind at 3 months of follow-up. | Composite of major thromboembolic or bleeding events as well as death at 6 months of follow-up. | 90 days of follow-up: Efficacy: composite of IS/TIA/SBI/SE Safety: major or clinically relevant non-major bleeding. |
| Results | No anticoagulation: thrombus 7/10 Enoxaparin: 8/10 Rivaroxaban: 4/10 | No adverse events of any kind. No difference in echo graphic parameters. Eradication of spontaneous echo contrast in 2 patients | No adverse events of any kind. No difference in echo graphic parameters. | 100% of follow-up and analysis in both groups. No statistical difference between rivaroxaban and warfarin in any outcome assessed. Numerically, rivaroxaban had a lower proportion of events. |
| Valve thrombus | No anticoagulation: 760 (0–2298) mg Enoxaparin: 717 (0–1490) mg Rivaroxaban: 210 (0–1337) mg | N/A | N/A | No signs of valve thrombosis or new intracardiac thrombus in either group. |
| Bleeding | None observed in either group | None observed | None observed | 6 minor bleedings in each group |
| Stroke | N/A | None observed | None observed | Rivaroxaban: 1 TIA Warfarin: 1 SBI, 2 IS |
| Myocardial infarction | N/A | None observed | None observed | Warfarin: 1 acute myocardial infarction resulting in death. |
| Rivaroxaban level | Cmax: 65–231 µg/L Cmin: 3.89–95.5 µg/L | Not measured | Not measured | Not measured |
| Conclusion | Rivaroxaban significantly reduced thrombus weight and platelet deposition. | Use of rivaroxaban in patients with unstable INR after mitral valve replacement may be feasible. | Rivaroxaban treatment was safe, efficient, and feasible for the prevention of thromboembolic events in low-risk patients who received a mechanical aortic heart valve. | Rivaroxaban 15 mg BID had similar thromboembolic and bleeding events to warfarin in patients with mechanical heart valves. |
| Reference | P. A. Lester et al. (2017) [6] | L. Van Hoof et al. (2022) [24] | PROACT-Xa (2023) [25] |
|---|---|---|---|
| Setting | Swine aortic heterotopic valve model | Swine mechanical valve in the pulmonary position. | Human aortic valve replacement >3 months postoperatively. |
| Treatment groups | 5 swine: apixaban PO 4 swine: apixaban infusion 3 swine: warfarin PO 4 swine: no anticoagulation | 2 swine: low dose 4 swine: intermediary dose 3 swine: high dose | 420-patient apixaban cohort 414-patient warfarin cohort |
| Valves used | Not specified | 21 mm On-X aortic valve | On-X aortic valve |
| Dose | Apixaban 1 mg/kg BID PO Apixaban 0.5 mg/kg bolus IV Warfarin 0.04–0.08 mg/kg (INR: 2–3) PO | Low dose: 5 mg BID for 10 weeks Intermediary dose: 5 mg BID for 6 weeks and then 10 mg BID for 4 weeks High dose: 15 mg BID for 10 weeks | Warfarin INR 2–3 PO Apixaban 5 mg BID * |
| Primary endpoint | Thrombus weight at 30 days for no anticoagulation and control groups. Thrombus weight at 14 days for apixaban infusion groups. | Thrombus presence and weight after 10 weeks. | Efficacy: valve thrombosis or valve-related thromboembolism Safety: major bleeding |
| Results | Apixaban PO: 3/5 thrombus Apixaban IV: 0/4 thrombus Warfarin PO: 2/3 thrombus | Low dose: 2/2 thrombus. Intermediate dose: 2/4 thrombus. High dose: 0/2 thrombus. | Terminated prematurely due to excess thromboembolic events in the apixaban cohort. |
| Valve thrombus | Apixaban PO: 357.5 ± 234.9 mg Apixaban IV: 61.1 ± 47.2 mg Warfarin 247.1 ± 134.3 mg No-anticoagulation: 1422 ± 676.4 mg | Low dose: 108.8 mg and 548.8 mg Intermediary dose: 65.5 mg and 41 mg. Two animals no thrombus. High dose: no thrombus. | Apixaban cohort: -3 valve thrombi -17 valve related thromboembolism -4.2%/patient-years Warfarin cohort: -0 valve thrombi -6 valve related thromboembolism -1.3%/patient-years |
| Bleeding | Apixaban PO: 0/5 Apixaban IV: 0/4 Warfarin: 2/3 Control group: 0/4 | None observed | Major bleeding: -apixaban: 3.6%/patient-years -warfarin: 4.5%/patient-years |
| Stroke | None observed | None observed | Apixaban: 17 (2.9%/patient-years) Warfarin: 0 (0%/patients-years) |
| Myocardial infarction | None observed | None observed | Apixaban: 0 (0%/patient-years) Warfarin: 1 (0.2%/patients-years) |
| Apixaban level | Cmax: 214.67 ng/mL (SD: 91.51) AUC: 1390.00 ng∙h/mL (SD: 564.02) | Median apixaban peak plasma concentration Low dose: 43.6 ng/mL (range 23.1–64) Intermediary dose: 49.9 ng/mL (range 39.9–61) High dose: 49.9 ng/mL (range 44.6–82.9) | Not available for apixaban vs. warfarin; 72.7% time in the therapeutic range |
| Conclusion | Apixaban significantly reduced thrombus weight compared to no anticoagulation. Apixaban swine did not demonstrate bleeding events. | The results of this study suggest that even in highly thrombogenic situations, apixaban can effectively prevent thrombosis in MHVs. The study also found that increasing the dose of apixaban led to a decrease in thrombus formation, without increasing bleeding events. | Apixaban did not demonstrate noninferiority to warfarin and is less effective than warfarin for the prevention of valve thrombosis or thromboembolism in patients with an On-X mechanical aortic valve. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Langenaeken, T.; Vanoppen, A.; Janssens, F.; Tanghe, L.; Verbrugghe, P.; Rega, F.; Meuris, B. DOACs in the Anticoagulation of Mechanical Valves: A Systematic Review and Future Perspectives. J. Clin. Med. 2023, 12, 4984. https://doi.org/10.3390/jcm12154984
Langenaeken T, Vanoppen A, Janssens F, Tanghe L, Verbrugghe P, Rega F, Meuris B. DOACs in the Anticoagulation of Mechanical Valves: A Systematic Review and Future Perspectives. Journal of Clinical Medicine. 2023; 12(15):4984. https://doi.org/10.3390/jcm12154984
Chicago/Turabian StyleLangenaeken, Tom, Arnaud Vanoppen, Fien Janssens, Loes Tanghe, Peter Verbrugghe, Filip Rega, and Bart Meuris. 2023. "DOACs in the Anticoagulation of Mechanical Valves: A Systematic Review and Future Perspectives" Journal of Clinical Medicine 12, no. 15: 4984. https://doi.org/10.3390/jcm12154984