
Patient-Reported Outcome Measures in Patients with Thrombotic Thrombocytopenic Purpura: A Systematic Review of the Literature
 and
and
Abstract
:1. Introduction
2. Materials and Methods
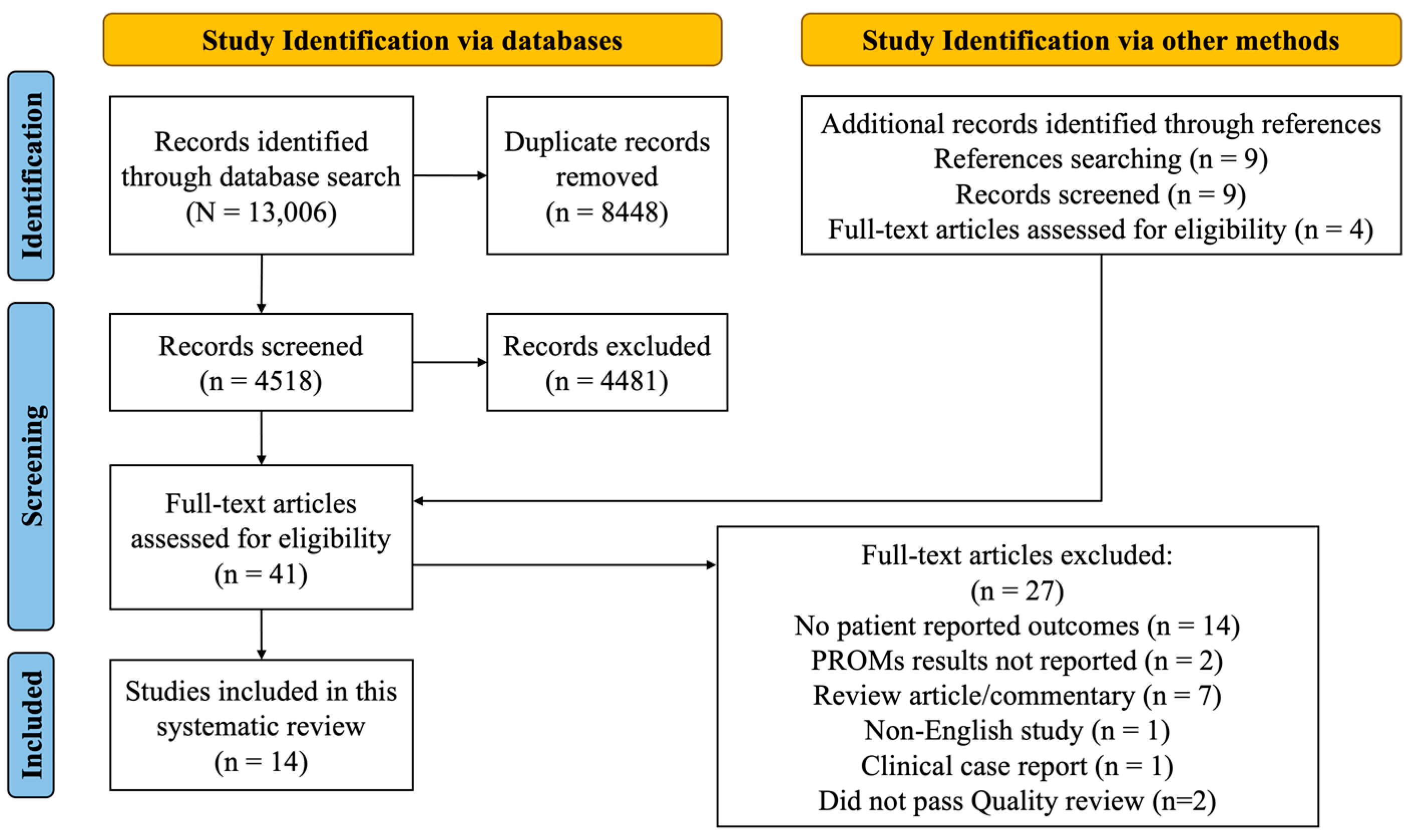
2.1. Search Strategy and Selection Criteria
2.2. Data Analysis
3. Results
3.1. Included Studies
3.2. PROMs in Published Studies
3.3. PROMs in Unpublished Studies
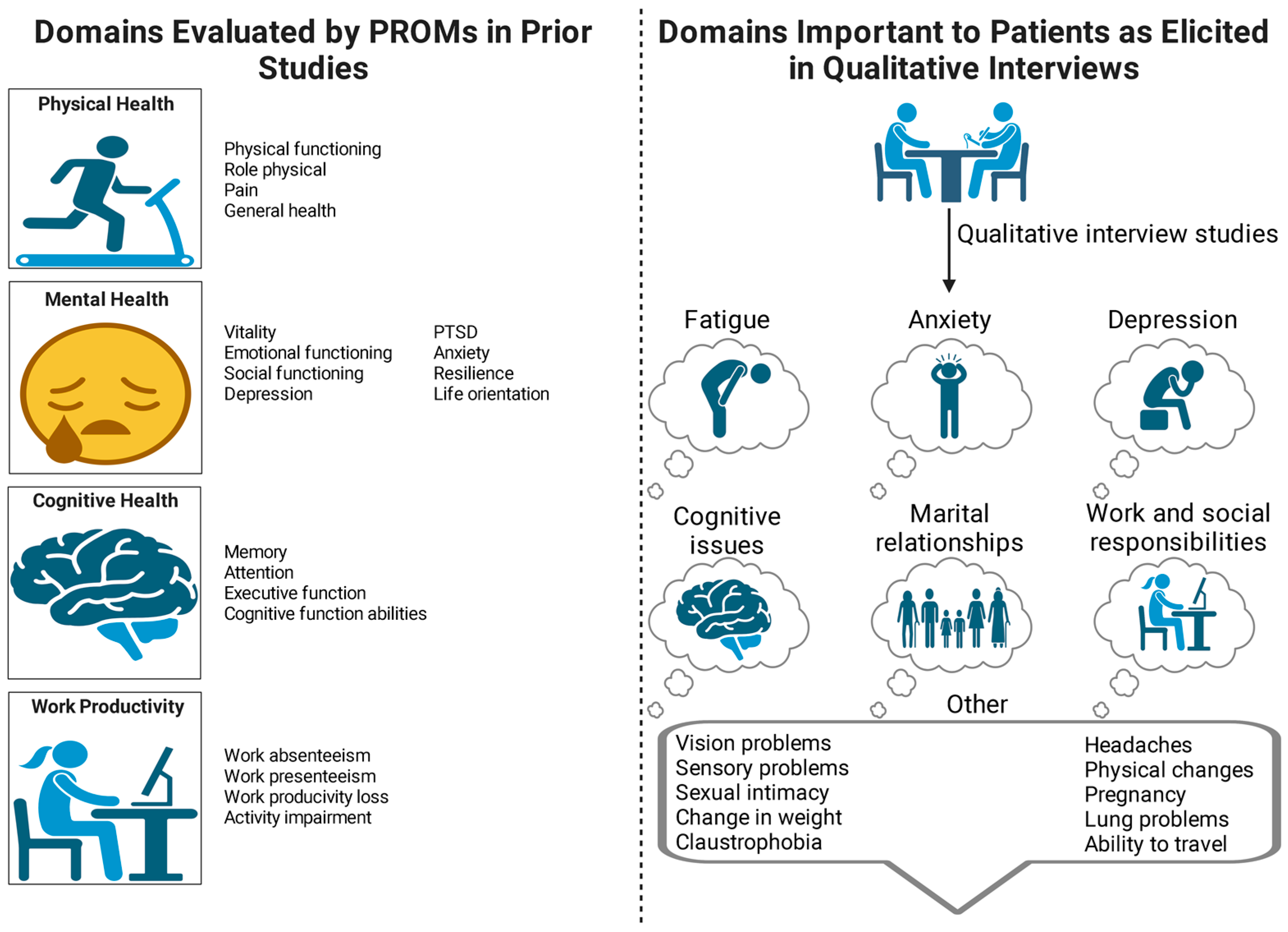
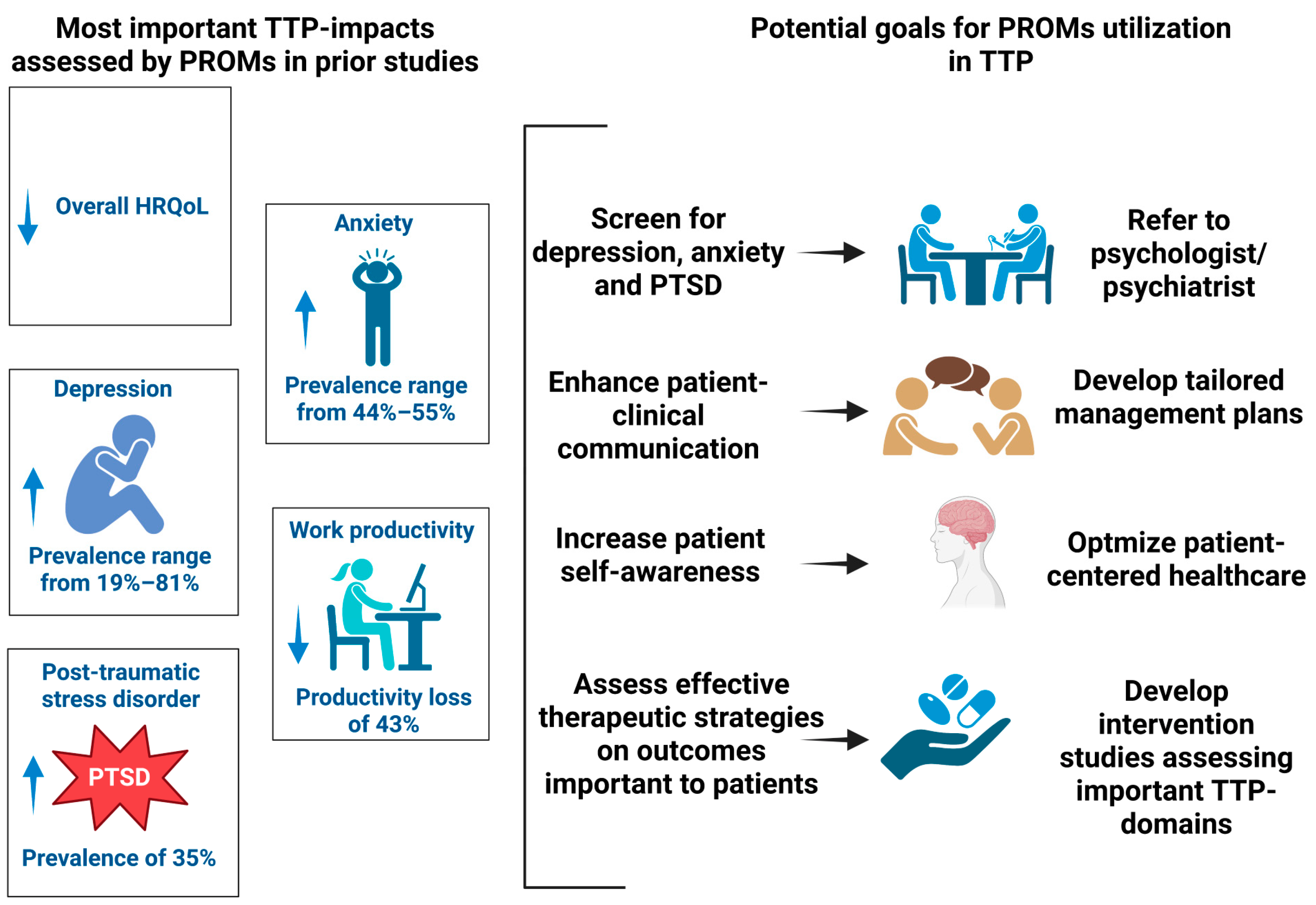
3.4. PROMs Capturing the Impact of TTP-Related Morbidity
3.5. Association between PROMs and TTP Episode Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Joly, B.S.; Coppo, P.; Veyradier, A. An Update on Pathogenesis and Diagnosis of Thrombotic Thrombocytopenic Purpura. Expert. Rev. Hematol. 2019, 12, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Lewis, Q.F.; Lanneau, M.S.; Mathias, S.D.; Terrell, D.R.; Vesely, S.K.; George, J.N. Long-Term Deficits in Health-Related Quality of Life after Recovery from Thrombotic Thrombocytopenic Purpura. Transfusion 2009, 49, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Cuker, A.; Cataland, S.R.; Coppo, P.; de la Rubia, J.; Friedman, K.D.; George, J.N.; Knoebl, P.N.; Kremer Hovinga, J.A.; Lämmle, B.; Matsumoto, M.; et al. Redefining Outcomes in Immune TTP: An International Working Group Consensus Report. Blood 2021, 137, 1855–1861. [Google Scholar] [CrossRef]
- Deford, C.C.; Reese, J.A.; Schwartz, L.H.; Perdue, J.J.; Kremer Hovinga, J.A.; Lämmle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Multiple Major Morbidities and Increased Mortality during Long-Term Follow-up after Recovery from Thrombotic Thrombocytopenic Purpura. Blood 2013, 122, 2023–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, S.; Podger, L.; Bottomley, C.; Rzepa, E.; Bailey, K.M.A.; Chandler, F. Survival after Acute Episodes of Immune-Mediated Thrombotic Thrombocytopenic Purpura (ITTP)—Cognitive Functioning and Health-Related Quality of Life Impact: A Descriptive Cross-Sectional Survey of Adults Living with ITTP in the United Kingdom. Hematology 2021, 26, 465–472. [Google Scholar] [CrossRef]
- Terrell, D.; Cataland, S.; Beebe, L.; Keller, S.; Panepinto, J.; Vesely, S.K.; George, J.; Kelley, R.A.; Cheney, M. Impact of Residual Effects and Complications of Thrombotic Thrombocytopenic Purpura (TTP) on Daily Living: A Qualitative Study. Blood 2019, 134, 931. [Google Scholar] [CrossRef]
- Han, B.; Page, E.E.; Stewart, L.M.; Deford, C.C.; Scott, J.G.; Schwartz, L.H.; Perdue, J.J.; Terrell, D.R.; Vesely, S.K.; George, J.N. Depression and Cognitive Impairment Following Recovery from Thrombotic Thrombocytopenic Purpura: Depression and Cognitive Impairment Following TTP. Am. J. Hematol. 2015, 90, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Saultz, J.N.; Wu, H.M.; Cataland, S. Headache Prevalence Following Recovery from TTP and AHUS. Ann. Hematol. 2015, 94, 1473–1476. [Google Scholar] [CrossRef]
- Falter, T.; Schmitt, V.; Herold, S.; Weyer, V.; von Auer, C.; Wagner, S.; Hefner, G.; Beutel, M.; Lackner, K.; Lämmle, B.; et al. Depression and Cognitive Deficits as Long-Term Consequences of Thrombotic Thrombocytopenic Purpura: Depression and cognitive deficits in TTP. Transfusion 2017, 57, 1152–1162. [Google Scholar] [CrossRef] [Green Version]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource [Internet]. Silver Spring (MD): Food and Drug Administration (US); 2016-. Glossary. 2016 Jan 28 [Updated 2021 Nov 29]. Co-Published by National Institutes of Health (US), Bethesda (MD). Available online: https://www.ncbi.nlm.nih.gov/books/NBK326791/ (accessed on 14 December 2022).
- Crego, N.; Masese, R.; Bonnabeau, E.; Douglas, C.; Rains, G.; Shah, N.; Tanabe, P. Patient Perspectives of Sickle Cell Management in the Emergency Department. Crit. Care Nurs. Q. 2021, 44, 160–174. [Google Scholar] [CrossRef]
- Kinahan, J.Y.; Graham, J.M.I.; Hébert, Y.V.; Sampson, M.; O’Hearn, K.; Klaassen, R.J. Patient-Reported Outcome Measures in Pediatric Non-Malignant Hematology: A Systematic Review. J. Pediatr. Hematol. Oncol. 2021, 43, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.; de la Rubia, J.; Pavenski, K.; Metjian, A.; Knöbl, P.; Peyvandi, F.; Cataland, S.; Coppo, P.; Kremer Hovinga, J.A.; Minkue Mi Edou, J.; et al. Long-term Follow-up of Patients Treated with Caplacizumab and Safety and Efficacy of Repeat Caplacizumab Use: Post-HERCULES Study. J. Thromb. Haemost. 2022, 20, 2810–2822. [Google Scholar] [CrossRef] [PubMed]
- Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims: Guidance for Industry. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims (accessed on 11 November 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Shamseer, L.; Tricco, A.C. Registration of Systematic Reviews in PROSPERO: 30,000 Records and Counting. Syst. Rev. 2018, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Covidence. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2022. Available online: https://www.covidence.org/ (accessed on 23 July 2022).
- Joanna Briggs Institute Checklists for Case Reports and Case Series. Available online: https://jbi.global/critical-appraisal-tools (accessed on 17 April 2023).
- Cataland, S.R.; Scully, M.A.; Paskavitz, J.; Maruff, P.; Witkoff, L.; Jin, M.; Uva, N.; Gilbert, J.C.; Wu, H.M. Evidence of Persistent Neurologic Injury Following Thrombotic Thrombocytopenic Purpura. Am. J. Hematol. 2011, 86, 87–89. [Google Scholar] [CrossRef]
- Riva, S.; Mancini, I.; Maino, A.; Ferrari, B.; Artoni, A.; Agosti, P.; Peyvandi, F. Long-Term Neuropsychological Sequelae, Emotional Wellbeing and Quality of Life in Patients with Acquired Thrombotic Thrombocytopenic Purpura. Haematologica 2020, 105, 1957–1962. [Google Scholar] [CrossRef] [Green Version]
- Alwan, F.; Mahdi, D.; Tayabali, S.; Cipolotti, L.; Lakey, G.; Hyare, H.; Scully, M. Cerebral MRI Findings Predict the Risk of Cognitive Impairment in Thrombotic Thrombocytopenic Purpura. Br. J. Haematol. 2020, 191, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, D.B.; Carey, R.W. The Cost of Surviving Thrombotic Thrombocytopenic Purpura: Case Report. J. Clin. Psychiatry 1984, 45, 477–479. [Google Scholar]
- Kennedy, A.S.; Lewis, Q.F.; Scott, J.G.; Kremer Hovinga, J.A.; Lämmle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Cognitive Deficits after Recovery from Thrombotic Thrombocytopenic Purpura. Transfusion 2009, 49, 1092–1101. [Google Scholar] [CrossRef]
- Clinical Outcome Study of ARC1779 Injection in Patients with Thrombotic Microangiopathy. Available online: https://clinicaltrials.gov/Ct2/Show/Study/NCT00726544 (accessed on 12 November 2022).
- Study to Assess Efficacy and Safety of Anti-von Willebrand Factor (VWF) Nanobody in Patients with Acquired Thrombotic Thrombocytopenic Purpura (ATTP) (TITAN). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT01151423 (accessed on 11 November 2022).
- The ConNeCT Study: Neurological Complications of TTP. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04981028 (accessed on 9 September 2022).
- Efficacy of a Personalized Caplacizumab Regimen Based on ADAMTS13 Activity Monitoring in Adult ATTP (CAPLAVIE). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04720261 (accessed on 9 September 2022).
- Dahlan, R.; McCormick, B.B.; Alkhattabi, M.; Gallo, K.; Clark, W.F.; Rock, G. Patients’ Quality of Life after Stopping Plasma Exchange: A Pilot Study. Transfus. Apher. Sci. 2014, 51, 137–140. [Google Scholar] [CrossRef]
- Alesci, S.R.; Schwan, V.; Miesbach, W.; Seifried, E.; Klinger, D. Rare Bleeding Disorders Are Associated with Depression and Anxiety. Hamostaseologie 2013, 33 (Suppl. S1), S64–S68. [Google Scholar] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 Total Score as a Single Measure of Health-Related Quality of Life: Scoping Review. SAGE Open Med. 2016, 4, 205031211667172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; van der Graaf, W.T.A.; van de Poll-Franse, L.V. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the “Real-World”: Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722–e732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, R.; Hinz, A. Reference Data for the Quality of Life Questionnaire EORTC QLQ-C30 in the General German Population. Eur. J. Cancer 2001, 37, 1345–1351. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; Haes, J.C.J.M.d.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Mystakidou, K.; Tsilika, E.; Parpa, E.; Kalaidopoulou, O.; Smyrniotis, V.; Vlahos, L. The EORTC Core Quality of Life Questionnaire (QLQ-C30, Version 3.0) in Terminally Ill Cancer Patients under Palliative Care: Validity and Reliability in a Hellenic Sample. Int. J. Cancer 2001, 94, 135–139. [Google Scholar] [CrossRef]
- Yang, M.; Rendas-Baum, R.; Varon, S.F.; Kosinski, M. Validation of the Headache Impact Test (HIT-6TM) across Episodic and Chronic Migraine. Cephalalgia 2011, 31, 357–367. [Google Scholar] [CrossRef]
- Kosinski, M.; Bayliss, M.S.; Bjorner, J.B.; Ware, J.E., Jr.; Garber, W.H.; Batenhorst, A.; Cady, R.; Dahlöf, C.G.H.; Dowson, A.; Tepper, S. A Six-Item Short-Form Survey for Measuring Headache Impact: The HIT-6. Qual. Life Res. 2003, 12, 963–974. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Plemmons, G. Depression and Suicide Screening. In Adolescent Health Screening: An Update in the Age of Big Data; Elsevier: Amsterdam, The Netherlands, 2019; pp. 135–149. ISBN 978-0-323-66130-0. [Google Scholar]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a Measure of Current Depression in the General Population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Strine, T.W.; Kroenke, K.; Dhingra, S.; Balluz, L.S.; Gonzalez, O.; Berry, J.T.; Mokdad, A.H. The Associations Between Depression, Health-Related Quality of Life, Social Support, Life Satisfaction, and Disability in Community-Dwelling US Adults. J. Nerv. Ment. Dis. 2009, 197, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric Properties of the Beck Depression Inventory: Twenty-Five Years of Evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Reeves, G.M.; Rohan, K.J.; Langenberg, P.; Snitker, S.; Postolache, T.T. Calibration of Response and Remission Cut-Points on the Beck Depression Inventory-Second Edition for Monitoring Seasonal Affective Disorder Treatment Outcomes. J. Affect. Disord. 2012, 138, 123–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Generalised Anxiety Disorder Assessment (GAD-7). Available online: https://www.corc.uk.net/Outcome-Experience-Measures/Generalised-Anxiety-Disorder-Assessment-Gad-7/#:~:Text=The%20GAD%2D7%20is%20a,1%2D2%20minutes%20to%20complete (accessed on 31 May 2023).
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- John Rush, A.; Giles, D.E.; Schlesser, M.A.; Fulton, C.L.; Weissenburger, J.; Burns, C. The Inventory for Depressive Symptomatology (IDS): Preliminary Findings. Psychiatry Res. 1986, 18, 65–87. [Google Scholar] [CrossRef]
- Rush, A.J.; Gullion, C.M.; Basco, M.R.; Jarrett, R.B.; Trivedi, M.H. The Inventory of Depressive Symptomatology (IDS): Psychometric Properties. Psychol. Med. 1996, 26, 477–486. [Google Scholar] [CrossRef]
- Cerimele, J.M.; Goldberg, S.B.; Miller, C.J.; Gabrielson, S.W.; Fortney, J.C. Systematic Review of Symptom Assessment Measures for Use in Measurement-Based Care of Bipolar Disorders. Psychiatr. Serv. 2019, 70, 396–408. [Google Scholar] [CrossRef]
- Brown, E.S.; Murray, M.; Carmody, T.J.; Kennard, B.D.; Hughes, C.W.; Khan, D.A.; Rush, A.J. The Quick Inventory of Depressive Symptomatology-Self-Report: A Psychometric Evaluation in Patients with Asthma and Major Depressive Disorder. Ann. Allergy Asthma Immunol. 2008, 100, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Parkitny, L.; McAuley, J. The Depression Anxiety Stress Scale (DASS). J. Physiother. 2010, 56, 204. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, S.; Oluwole, O.; Cataland, S.; McCrae, K.R. Post-Traumatic Stress Disorder and Depression in Survivors of Thrombotic Thrombocytopenic Purpura. Thromb. Res. 2017, 151, 51–56. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation: Posttraumatic Stress Disorder Checklist for DSM-5. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- PTSD Checklist for DSM-5 (PCL-5). Available online: https://www.ptsd.va.gov/Professional/Assessment/Adult-Sr/Ptsd-Checklist.Asp (accessed on 31 May 2023).
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) Developed and Tested Its First Wave of Adult Self-Reported Health Outcome Item Banks: 2005–2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mücke, F.J.; Hendriks, M.P.; Bien, C.G.; Grewe, P. Discrepancy between Subjective and Objective Memory Change after Epilepsy Surgery: Relation with Seizure Outcome and Depressive Symptoms. Front. Neurol. 2022, 13, 855664. [Google Scholar] [CrossRef] [PubMed]
- Beblo, T.; Kunz, M.; Brokate, B.; Scheurich, A.; Weber, B.; Albert, A.; Richter, P.; Lautenbacher, S. Entwicklung eines Fragebogens zur subjektiven Einschätzung der geistigen Leistungsfähigkeit (FLei) bei Patienten mit psychischen Störungen. Z. Neuropsychol. 2010, 21, 143–151. [Google Scholar] [CrossRef]
- Falter, T.; Böschen, S.; Schepers, M.; Beutel, M.; Lackner, K.; Scharrer, I.; Lämmle, B. Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura. J. Clin. Med. 2021, 10, 365. [Google Scholar] [CrossRef] [PubMed]
- FLEI. Available online: https://marketplace.schuhfried.com/En/FLEI (accessed on 31 May 2023).
- von Eisenhart Rothe, A.; Zenger, M.; Lacruz, M.E.; Emeny, R.; Baumert, J.; Haefner, S.; Ladwig, K.-H. Validation and Development of a Shorter Version of the Resilience Scale RS-11: Results from the Population-Based KORA–Age Study. BMC Psychol. 2013, 1, 25. [Google Scholar] [CrossRef] [Green Version]
- Wagnild, G.M.; Young, H.M. Development and Psychometric Evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing Optimism from Neuroticism (and Trait Anxiety, Self-Mastery, and Self-Esteem): A Reevaluation of the Life Orientation Test. J. Personal. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Revised Life Orientation Test (LOT-R). Available online: https://sparqtools.org/Mobility-Measure/Revised-Life-Orientation-Test-Lotr/ (accessed on 31 May 2023).
- Reilly, M.C.; Zbrozek, A.S.; Dukes, E.M. The Validity and Reproducibility of a Work Productivity and Activity Impairment Instrument. PharmacoEconomics 1993, 4, 353–365. [Google Scholar] [CrossRef]
- Tillett, W.; Lin, C.-Y.; Zbrozek, A.; Sprabery, A.T.; Birt, J. A Threshold of Meaning for Work Disability Improvement in Psoriatic Arthritis Measured by the Work Productivity and Activity Impairment Questionnaire. Rheumatol. Ther. 2019, 6, 379–391. [Google Scholar] [CrossRef] [Green Version]
- Page, E.E.; Jiang, Y.; Terrell, D.R.; Vesely, S.K.; George, J.N. Long-Term Outcomes of Health-Related Quality of Life Following Diverse Thrombotic Microangiopathy Syndromes: HRQOL Following Recovery from TMA. Am. J. Hematol. 2016, 91, E278–E279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrell, D.R.; Tolma, E.L.; Stewart, L.M.; Shirley, E.A. Thrombotic Thrombocytopenic Purpura Patients’ Attitudes toward Depression Management: A Qualitative Study. Health Sci. Rep. 2019, 2, e136. [Google Scholar] [CrossRef]
- Kelley, R.A.; Cheney, M.K.; Martin, C.M.; Cataland, S.R.; Quick, L.B.; Keller, S.; Vesely, S.K.; Llaneza, A.J.; Khawandanah, M.; Journeycake, J.; et al. Health Following Recovery from Immune Thrombotic Thrombocytopenic Purpura: The Patient’s Perspective. Blood Adv. 2022, 7, 1813–1822. [Google Scholar] [CrossRef]
- Oladapo, A.; Ito, D.; Hibbard, C.; Hare, T.; Krupnick, R.; Ewenstein, B. Development of a Patient-Reported Outcome (PRO) Instrument for Patients with Acquired Thrombotic Thrombocytopenic Purpura. Value Health 2018, 21, S257. [Google Scholar] [CrossRef]
- Oladapo, A.; Ito, D.; Hibbard, C.; Bean, S.; Krupnick, R.; Ewenstein, B. 22nd International Abstracts Book, PSY92 patient-reported outcome (PRO) instrument development for congenital thrombotic thrombocytopenic purpura (cTTP, upshaw-schulman syndrome [USS], hereditary thrombotic thrombocytopenic purpura, hTTP). Value Health 2017, 20, A225. [Google Scholar] [CrossRef]
- Kluzek, S.; Dean, B.; Wartolowska, K.A. Patient-Reported Outcome Measures (PROMs) as Proof of Treatment Efficacy. BMJ EBM 2022, 27, 153–155. [Google Scholar] [CrossRef]
- Churruca, K.; Pomare, C.; Ellis, L.A.; Long, J.C.; Henderson, S.B.; Murphy, L.E.D.; Leahy, C.J.; Braithwaite, J. Patient-reported Outcome Measures (PROMs): A Review of Generic and Condition-specific Measures and a Discussion of Trends and Issues. Health Expect. 2021, 24, 1015–1024. [Google Scholar] [CrossRef]
- Bele, S.; Mohamed, B.; Chugh, A.; Haverman, L.; Santana, M.-J. Impact of Using Patient-Reported Outcome Measures in Routine Clinical Care of Paediatric Patients with Chronic Conditions: A Systematic Review Protocol. BMJ Open 2019, 9, e027354. [Google Scholar] [CrossRef] [Green Version]
- Field, J.; Holmes, M.M.; Newell, D. PROMs Data: Can It Be Used to Make Decisions for Individual Patients? A Narrative Review. Patient Relat. Outcome Meas. 2019, 10, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Thestrup Hansen, S.; Kjerholt, M.; Friis Christensen, S.; Brodersen, J.; Hølge-Hazelton, B. User Experiences on Implementation of Patient Reported Outcome Measures (PROMs) in a Haematological Outpatient Clinic. J. Patient Rep. Outcomes 2020, 4, 87. [Google Scholar] [CrossRef] [PubMed]
- Willik, E.M.; Terwee, C.B.; Bos, W.J.W.; Hemmelder, M.H.; Jager, K.J.; Zoccali, C.; Dekker, F.W.; Meuleman, Y. Patient-reported Outcome Measures (PROMs): Making Sense of Individual PROM Scores and Changes in PROM Scores over Time. Nephrology 2021, 26, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Lordon, R.J.; Mikles, S.P.; Kneale, L.; Evans, H.L.; Munson, S.A.; Backonja, U.; Lober, W.B. How Patient-Generated Health Data and Patient-Reported Outcomes Affect Patient–Clinician Relationships: A Systematic Review. Health Inform. J. 2020, 26, 2689–2706. [Google Scholar] [CrossRef]
- Antunes, B.; Harding, R.; Higginson, I.J.; on behalf of EUROIMPACT. Implementing Patient-Reported Outcome Measures in Palliative Care Clinical Practice: A Systematic Review of Facilitators and Barriers. Palliat. Med. 2014, 28, 158–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marker, A.M.; Patton, S.R.; McDonough, R.J.; Feingold, H.; Simon, L.; Clements, M.A. Implementing Clinic-wide Depression Screening for Pediatric Diabetes: An Initiative to Improve Healthcare Processes. Pediatr. Diabetes 2019, 20, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Health Measures—Transforming How Health Is Measures. Available online: https://www.healthmeasures.net/Explore-Measurement-Systems/Promis (accessed on 9 June 2023).
- Singh, S.A.; Bakshi, N.; Mahajan, P.; Morris, C.R. What Is the Future of Patient-Reported Outcomes in Sickle-Cell Disease? Expert. Rev. Hematol. 2020, 13, 1165–1173. [Google Scholar] [CrossRef]
- Meadows, K.A. Patient-Reported Outcome Measures: An Overview. Br. J. Community Nurs. 2011, 16, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Kilgour, J.M.; Wali, G.; Gibbons, E.; Scherwath, A.; Barata Badiella, A.; Peniket, A.; Schoemans, H.; Matin, R.N. Systematic Review of Patient-Reported Outcome Measures in Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2020, 26, e113–e127. [Google Scholar] [CrossRef]
- FDA Patient-Focused Drug Development Guidance Series for Enhancing the Incorporation of the Patient’s Voice in Medical Product Development and Regulatory Decision Making. Available online: https://www.fda.gov/Drugs/Development-Approval-Process-Drugs/Fda-Patient-Focused-Drug-Development-Guidance-Series-Enhancing-Incorporation-Patients-Voice-Medical (accessed on 30 May 2023).




{kind=link}
{kind=link}
{kind=link}
| (a) | ||
|---|---|---|
| Measure Average Completion Time | Number of Items Recall Period | Domains Evaluated |
| SF-36 [5,30] ** <15 min [2] | 36 4 weeks | Physical Functioning |
| Bodily Pain | ||
| General Health | ||
| Vitality | ||
| Role Physical | ||
| Role Emotional | ||
| Social Functioning | ||
| Mental Health | ||
| QLQ-C30 [31,32,33] <9 min [34] | 30 1 week | Physical Functioning |
| Role Functioning | ||
| Cognitive Functioning | ||
| Emotional Functioning | ||
| Social Functioning | ||
| Global Quality of Life | ||
| Fatigue | ||
| Nausea/Vomiting | ||
| Pain | ||
| Appetite Loss | ||
| Diarrhea | ||
| Dyspnea | ||
| Constipation | ||
| Insomnia | ||
| Financial Impact | ||
| HIT-6 [8,35] <2 min [36] | 6 4 weeks | Pain |
| Role Functioning | ||
| Social Functioning | ||
| Vitality (Energy/Fatigue) | ||
| Cognition | ||
| Emotion Distress | ||
| (b) | ||
| Depression and Anxiety Instruments | ||
| PHQ-8/-9 [12,37] <5 min [37,38,39,40] | 8 or 9 *** 2 weeks | Depression |
| BDI-II [5,41] 5–10 min [42] | 21 2 weeks | Depression |
| GAD-7 [12,43] <2 min [44] | 7 2 weeks | Anxiety |
| HADS [5,45] <5 min [45] | 14 1 week | Depression |
| Anxiety | ||
| IDS-SR [46,47,48] <7 min [49] | 30 1 week | Depression |
| DASS [50] 10 to 20 min [51] | 42 1 week | Depression |
| Anxiety | ||
| Stress | ||
| Post-traumatic Stress Disorder Instrument | ||
| PCL-5 [52,53] 5–10 min [54] | 20 1 month | PTSD |
| Cognitive Function Instruments | ||
| PROMIS CFAS-SF6a [5,55] Time to complete NR | 6 1 week | Cognitive Function Abilities |
| Flei [9,56,57,58] 10 min [59] | 30 6 months | Attention |
| Memory | ||
| Executive Functions | ||
| Resilience and Life Orientation Instruments | ||
| RS-11 [60,61] Time to complete NR | 11 N/A | Mental Resistance |
| LOT-R [58,62] <3 min [63] | 10 N/A | Attitude to Life |
| Work Activity Instruments | ||
| WPAI-SHP [64,65] Time to complete NR | 6 1 week | Absenteeism |
| Presenteeism | ||
| Work Productivity Loss | ||
| Activity Impairment | ||
| Patient-Reported Domains/Impacts | Prior Studies Assessing Patient’s Perspective | Administered PROMs in Prior Studies | |||
|---|---|---|---|---|---|
| Oladapo et al. 2018 [69,70] | Holmes et al. 2005 [5] | Terrell et al. 2019 [6] | Kelley et al. 2022 [68] | ||
| Cognitive issues | N/A | X | X | X | FLei [9,58] PROMIS CFAS-SF6a [5] |
| Fatigue | X | X | X | X | QLQ-C30 [9] |
| Depression | N/A | X | X | X | PHQ-8/9 [4,6,21,58] BDI-II [6,7,52] IDS-SR [9] HADS [5,21] DASS [21] |
| Anxiety (including fear of relapse) | X | X | X | X | HADS [5,21] DASS [21] GAD-7 [9,21] |
| Impact on relationships/family | N/A | X | X | X | SF-36 [2,13,19,20] |
| Impact on social activities | N/A | X | X | X | SF-36 [2,13,19,20] QLQ-C30 [9] |
| Impact on work/career | X | X | X | X | WPAI-SHP [5] SF-36 [2,13,19,20] |
| Experience of flashbacks | N/A | X | N/A | N/A | Not assessed |
| PTSD | N/A | X | N/A | N/A | PCL-5 [52] |
| Lack of independence | N/A | X | N/A | N/A | Not assessed |
| Pain/Headache | X | N/A | N/A | X | HIT-6 [8,13] SF-36 [2,13,19,20] QLQ-C30 [9] |
| Bruising | X | N/A | N/A | N/A | Not assessed |
| Sensory problems | X | N/A | N/A | X | Not assessed |
| Lung problems | N/A | N/A | N/A | X | Not assessed |
| Claustrophobia | N/A | N/A | N/A | X | Not assessed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares Ferreira Junior, A.; Pinheiro Maux Lessa, M.; Kaplan, S.; Coles, T.M.; Terrell, D.R.; Onwuemene, O.A. Patient-Reported Outcome Measures in Patients with Thrombotic Thrombocytopenic Purpura: A Systematic Review of the Literature. J. Clin. Med. 2023, 12, 5155. https://doi.org/10.3390/jcm12155155
Soares Ferreira Junior A, Pinheiro Maux Lessa M, Kaplan S, Coles TM, Terrell DR, Onwuemene OA. Patient-Reported Outcome Measures in Patients with Thrombotic Thrombocytopenic Purpura: A Systematic Review of the Literature. Journal of Clinical Medicine. 2023; 12(15):5155. https://doi.org/10.3390/jcm12155155
Chicago/Turabian StyleSoares Ferreira Junior, Alexandre, Morgana Pinheiro Maux Lessa, Samantha Kaplan, Theresa M. Coles, Deirdra R. Terrell, and Oluwatoyosi A. Onwuemene. 2023. "Patient-Reported Outcome Measures in Patients with Thrombotic Thrombocytopenic Purpura: A Systematic Review of the Literature" Journal of Clinical Medicine 12, no. 15: 5155. https://doi.org/10.3390/jcm12155155