
Benefits of Paediatric to Adult Transition Programme in Inflammatory Bowel Disease: The BUTTERFLY Study of GETECCU and SEGHNP
 , , , , , , , , , , , , , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , , , , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection of Participating Centres
2.2. Patient Population
2.3. Study Outcomes
2.4. Data Collection
2.5. Definitions
2.5.1. Transition-Related Definitions
- Transition: Intentional and planned movement of adolescents and young adults suffering from chronic physical and medical conditions from child- to adult-oriented healthcare systems. We defined transition as a structured process involving the gastroenterologist, the paediatrician and a programme coordinator, as well as the parents and the IBD patient. At least one joint visit should have been carried out by those involved in the transition process.
- Transfer: Moment at which the medical attention was carried out by the gastroenterologist. We defined the transfer as the date of discharge from the paediatric clinic.
2.5.2. Clinical Definitions
- Type of hospital: Hospitals were clustered in conglomerates, taking into account different variables such as provision, offer of services, activity, complexity or teaching, which established the following three categories: (1) first-level hospital (less than 150 beds on average, hardly any high-tech resource and low complexity); (2) second-level hospital (of average size around 500 beds, medium complexity and some teaching activity); and (3) third-level hospital (large referral hospitals with great structural weight, full offer of services, great teaching and assistance activity and high complexity).
- Smoking status: Patients were considered “smokers” if they smoked more than seven cigarettes per week for at least six months and had smoked at least one cigarette in the six months prior to transfer. Patients were considered “ex-smokers” if they quit smoking at least six months before transfer. Patients were considered “non-smokers” if they never smoked or did so in very small amounts or occasionally. The smoking status was also categorised 12 months after transfer [18].
- IBD location and phenotype were defined according to the Paris classification [15].
- IBD activity: The Harvey–Bradshaw Index (HBI) [19] for Crohn’s disease (CD) and the partial Mayo score [20] for ulcerative colitis (UC) were used in the gastroenterologist setting. On the other hand, the Paediatric CD Activity Index (PCDAI) or the weighted PCDAI (wPCDAI) for CD [21] and the Paediatric UC Activity Index (PUCAI) [22] for UC were used in the paediatric setting. When endoscopy or radiological examination was available, the severity was graded as quiescent, mild, moderate or severe by local investigators.
- Biologic markers: Levels of C-reactive protein and faecal calprotectin were considered as high when >0.5 mg/dL and >250 µg/g, respectively.
- Patients lost to follow-up were defined as those who did not attend the gastroenterology unit during 12 months after transfer.
2.6. Statistical Analysis
3. Results
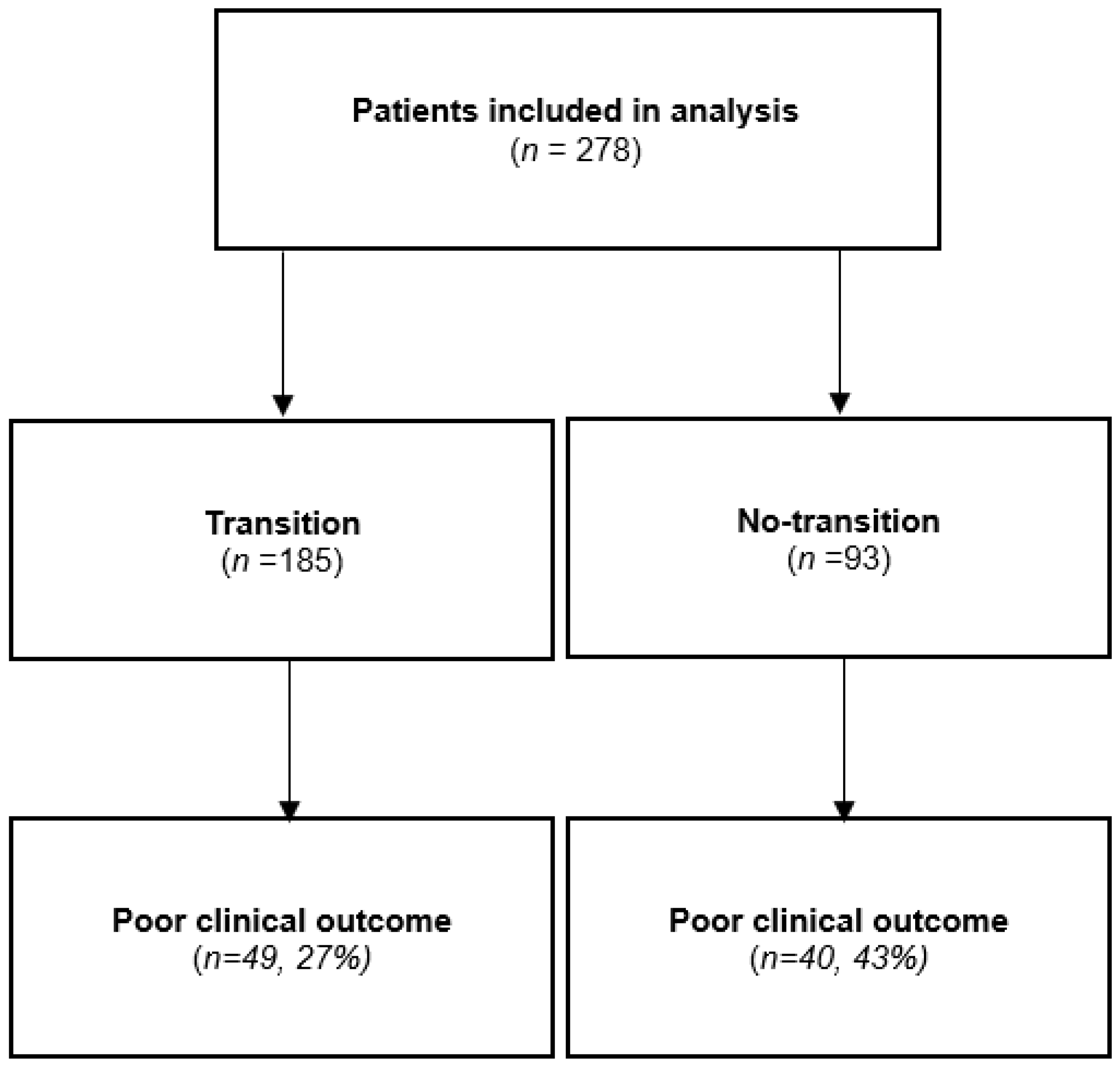
3.1. Patient Population
3.2. Characteristics of the Participating Hospitals
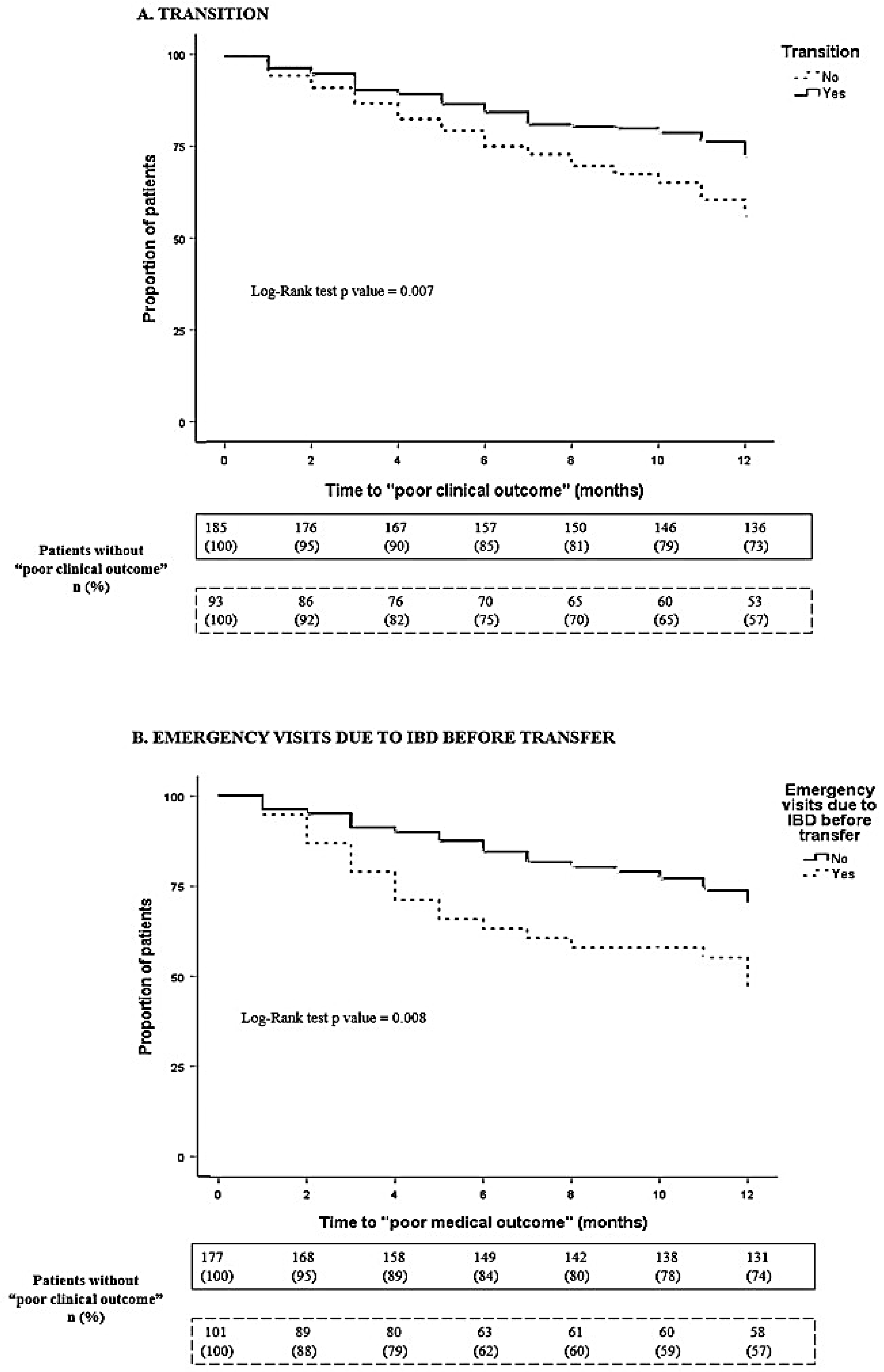
3.3. Clinical Outcomes
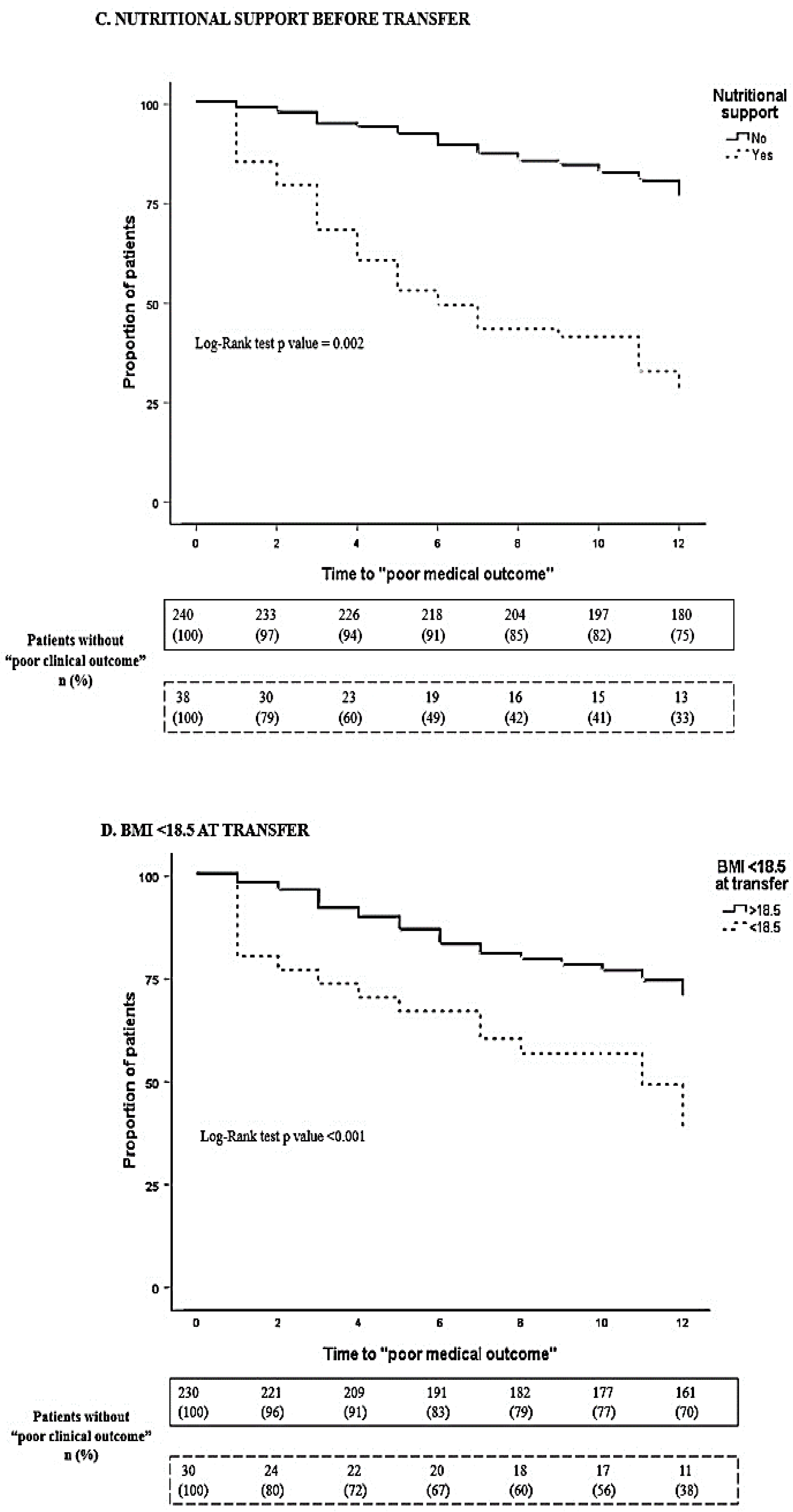
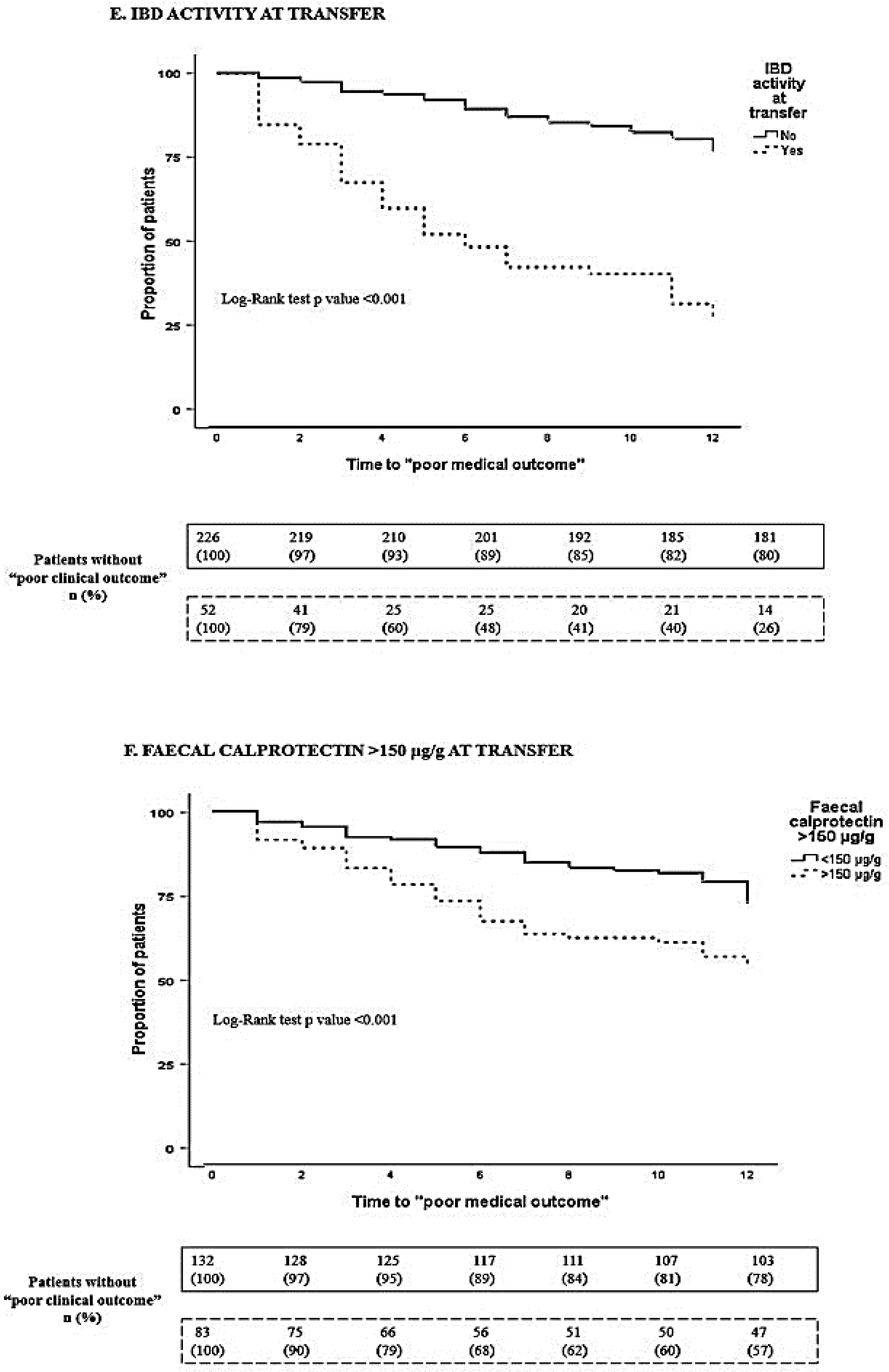
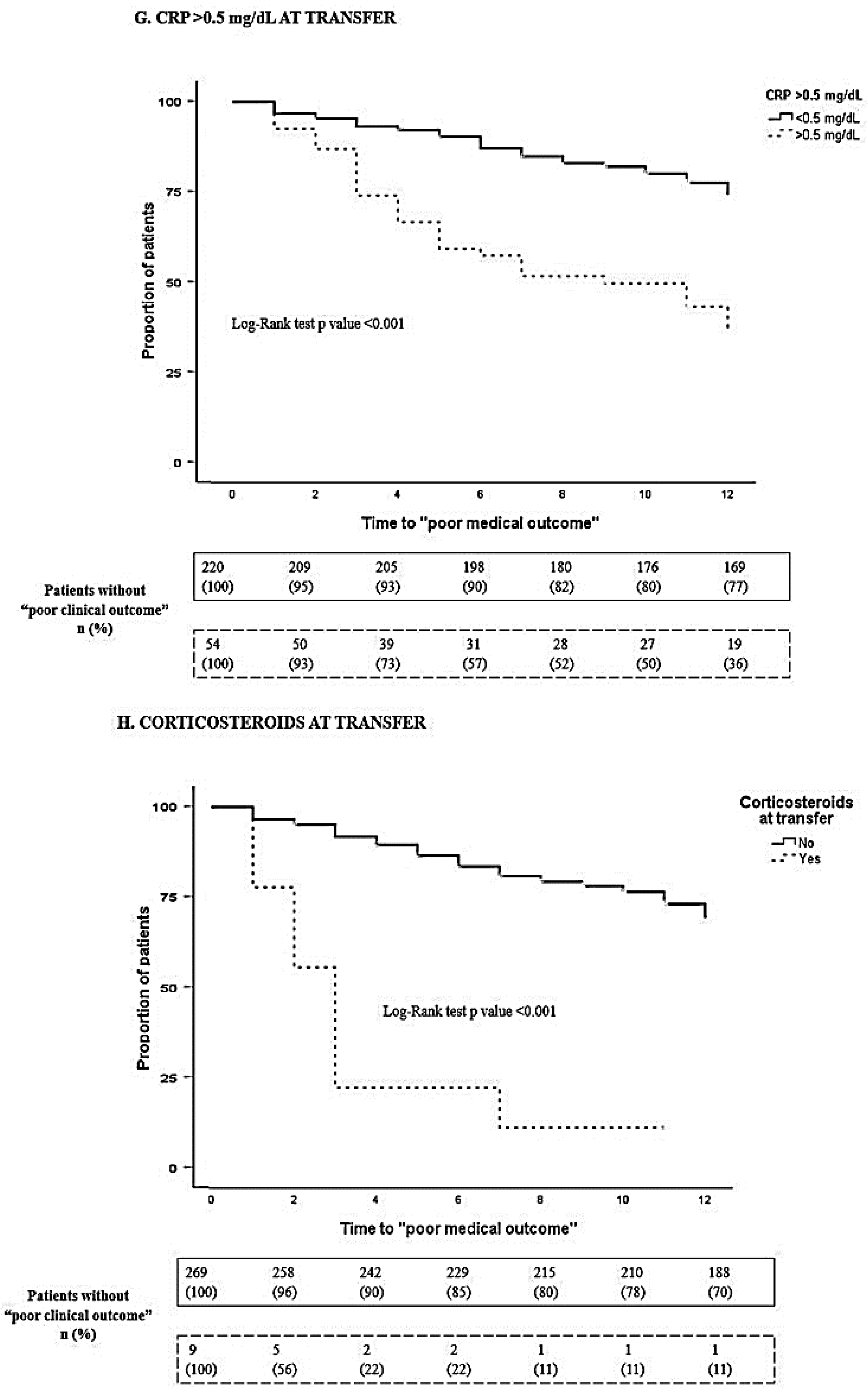
3.4. Predictive Factors of Poor Clinical Outcome after the Transfer
3.5. Patients Lost to Follow-Up
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Blum, R.W.; Garell, D.; Hodgman, C.H.; Jorissen, T.W.; Okinow, N.A.; Orr, D.P.; Slap, G.B. Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 1993, 14, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Fortinsky, K.J.; Gozdyra, P.; Van den Heuvel, M.; Van Limbergen, J.; Griffiths, A.M. Epidemiology of pediatric inflammatory bowel disease: A systematic review of international trends. Inflamm. Bowel Dis. 2011, 17, 423–439. [Google Scholar] [CrossRef] [PubMed]
- Martin-de-Carpi, J.; Rodriguez, A.; Ramos, E.; Jimenez, S.; Martinez-Gomez, M.J.; Medina, E.; Navas-Lopez, V.M.; on behalf of the SPIRIT-IBD Working Group of SEGHNP. The complete picture of changing pediatric inflammatory bowel disease incidence in Spain in 25 years (1985–2009): The EXPERIENCE registry. J. Crohn’s Colitis 2014, 8, 763–769. [Google Scholar] [CrossRef] [Green Version]
- Kuenzig, M.E.; Fung, S.G.; Marderfeld, L.; Mak, J.W.Y.; Kaplan, G.G.; Ng, S.C.; Wilson, D.C.; Cameron, F.; Henderson, P.; Kotze, P.G.; et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: Systematic Review. Gastroenterology 2022, 162, 1147–1159.e4. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.J.; Smith, P.J.; Cohen, R.; Collins, P.; Douds, A.; Forbes, V.; Gaya, D.R.; Johnston, B.T.; McKiernan, P.J.; Murray, C.D.; et al. UK guideline on transition of adolescent and young persons with chronic digestive diseases from paediatric to adult care. Gut 2017, 66, 988–1000. [Google Scholar] [CrossRef] [Green Version]
- Menon, T.; Afzali, A. Inflammatory Bowel Disease: A Practical Path to Transitioning From Pediatric to Adult Care. Am. J. Gastroenterol. 2019, 114, 1432–1440. [Google Scholar] [CrossRef]
- Van Rheenen, P.F.; Aloi, M.; Biron, I.A.; Carlsen, K.; Cooney, R.; Cucchiara, S.; Cullen, G.; Escher, J.C.; Kierkus, J.; Lindsay, J.O.; et al. European Crohn’s and Colitis Organisation Topical Review on Transitional Care in Inflammatory Bowel Disease. J. Crohn’s Colitis 2017, 11, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Italian Society of Paediatric Gastroenterology, Hepatology and Nutrition (SIGENP); Italian Association of Hospital Gastroenterologists and Endoscopists (AIGO); Italian Society of Endoscopy (SIED); Italian Society of Gastroenterology (SIGE); Elli, L.; Maieron, R.; Martelossi, S.; Guariso, G.; Buscarini, E.; Conte, D.; et al. Transition of gastroenterological patients from paediatric to adult care: A position statement by the Italian Societies of Gastroenterology. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2015, 47, 734–740. [Google Scholar] [CrossRef] [Green Version]
- Fu, N.; Bollegala, N.; Jacobson, K.; Kroeker, K.I.; Frost, K.; Afif, W.; El-Matary, W.; Fowler, S.A.; Griffiths, A.M.; Huynh, H.Q.; et al. Canadian Consensus Statements on the Transition of Adolescents and Young Adults with Inflammatory Bowel Disease from Pediatric to Adult Care: A Collaborative Initiative Between the Canadian IBD Transition Network and Crohn’s and Colitis Canada. J. Can. Assoc. Gastroenterol. 2022, 5, 105–115. [Google Scholar] [CrossRef]
- Baldassano, R.; Ferry, G.; Griffiths, A.; Mack, D.; Markowitz, J.; Winter, H. Transition of the patient with inflammatory bowel disease from pediatric to adult care: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 245–248. [Google Scholar] [CrossRef] [Green Version]
- Eros, A.; Soos, A.; Hegyi, P.; Szakacs, Z.; Eross, B.; Parniczky, A.; Mezosi, E.; Rumbus, Z.; Sarlos, P. Spotlight on Transition in Patients With Inflammatory Bowel Disease: A Systematic Review. Inflamm. Bowel Dis. 2020, 26, 331–346. [Google Scholar] [CrossRef] [Green Version]
- Gray, W.N.; Resmini, A.R.; Baker, K.D.; Holbrook, E.; Morgan, P.J.; Ryan, J.; Saeed, S.A.; Denson, L.A.; Hommel, K.A. Concerns, Barriers, and Recommendations to Improve Transition from Pediatric to Adult IBD Care: Perspectives of Patients, Parents, and Health Professionals. Inflamm. Bowel Dis. 2015, 21, 1641–1651. [Google Scholar] [CrossRef] [PubMed]
- Van den Brink, G.; van Gaalen, M.A.C.; de Ridder, L.; van der Woude, C.J.; Escher, J.C. Health Care Transition Outcomes in Inflammatory Bowel Disease: A Multinational Delphi Study. J. Crohn’s Colitis 2019, 13, 1163–1172. [Google Scholar] [CrossRef]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef] [Green Version]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Nunes, T.; Etchevers, M.J.; Merino, O.; Gallego, S.; Garcia-Sanchez, V.; Marin-Jimenez, I.; Menchen, L.; Barreiro-de Acosta, M.; Bastida, G.; Garcia, S.; et al. Does smoking influence Crohn’s disease in the biologic era? The TABACROHN study. Inflamm. Bowel Dis. 2013, 19, 23–29. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Lewis, J.D.; Chuai, S.; Nessel, L.; Lichtenstein, G.R.; Aberra, F.N.; Ellenberg, J.H. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm. Bowel Dis. 2008, 14, 1660–1666. [Google Scholar] [CrossRef] [Green Version]
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T.; et al. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Hyams, J.; Markowitz, J.; Lerer, T.; Mack, D.R.; Evans, J.; Pfefferkorn, M.; Rosh, J.; Kay, M.; Crandall, W.; et al. Appraisal of the pediatric ulcerative colitis activity index (PUCAI). Inflamm. Bowel Dis. 2009, 15, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- McCartney, S.; Lindsay, J.O.; Russell, R.K.; Gaya, D.R.; Shaw, I.; Murray, C.D.; Finney-Hayward, T.; Sebastian, S. Benefits of Structured Pediatric to Adult Transition in Inflammatory Bowel Disease: The TRANSIT Observational Study. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 208–214. [Google Scholar] [CrossRef]
- Testa, A.; Giannetti, E.; Rispo, A.; Rea, M.; Miele, E.; Scarpato, E.; Opramolla, A.; Nardone, O.M.; Imperatore, N.; Di Luna, I.; et al. Successful outcome of the transitional process of inflammatory bowel disease from pediatric to adult age: A five years experience. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2019, 51, 524–528. [Google Scholar] [CrossRef]
- Otto, C.; Tarnok, A.; Eros, A.; Szakacs, Z.; Vincze, A.; Farkas, N.; Sarlos, P. Planned Transition of Adolescent Patients with Inflammatory Bowel Disease Results in Higher Remission Rates. J. Pediatr. Nurs. 2019, 45, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Sattoe, J.N.T.; Peeters, M.A.C.; Haitsma, J.; van Staa, A.; Wolters, V.M.; Escher, J.C. Value of an outpatient transition clinic for young people with inflammatory bowel disease: A mixed-methods evaluation. BMJ Open 2020, 10, e033535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodhand, J.; Hedin, C.R.; Croft, N.M.; Lindsay, J.O. Adolescents with IBD: The importance of structured transition care. J. Crohn’s Colitis 2011, 5, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Cole, R.; Ashok, D.; Razack, A.; Azaz, A.; Sebastian, S. Evaluation of Outcomes in Adolescent Inflammatory Bowel Disease Patients Following Transfer From Pediatric to Adult Health Care Services: Case for Transition. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2015, 57, 212–217. [Google Scholar] [CrossRef]
- Schutz, L.; Radke, M.; Menzel, S.; Dabritz, J. Long-term implications of structured transition of adolescents with inflammatory bowel disease into adult health care: A retrospective study. BMC Gastroenterol. 2019, 19, 128. [Google Scholar] [CrossRef] [Green Version]
- Eros, A.; Dohos, D.; Veres, G.; Tarnok, A.; Vincze, A.; Teszas, A.; Zadori, N.; Gede, N.; Hegyi, P.; Sarlos, P. Effect of joint transition visits on quality of life in adolescents with inflammatory bowel diseases: A protocol for a prospective, randomised, multicentre, controlled trial (TRANS-IBD). BMJ Open 2020, 10, e038410. [Google Scholar] [CrossRef]
- Leung, Y.; Heyman, M.B.; Mahadevan, U. Transitioning the adolescent inflammatory bowel disease patient: Guidelines for the adult and pediatric gastroenterologist. Inflamm. Bowel Dis. 2011, 17, 2169–2173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreiro-de Acosta, M.; Gutierrez, A.; Zabana, Y.; Beltran, B.; Calvet, X.; Chaparro, M.; Domenech, E.; Esteve, M.; Panes, J.; Gisbert, J.P.; et al. Inflammatory bowel disease integral care units: Evaluation of a nationwide quality certification programme. The GETECCU experience. United Eur. Gastroenterol. J. 2021, 9, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Sanchez, C.; Tolin Hernani, M.D.M.; Alvarez Calatayud, G.; Miranda Cid, M.D.C.; Navas Lopez, V.M.; Marin Jimenez, I.; Menchen, L.A.; Garcia Fernandez, P.; Merino Sanchez-Canete, A. Status of transition care in inflammatory bowel disease in Spain. Different medical perspectives. Rev. Esp. Enfermedades Dig. Organo Of. Soc. Esp. Patol. Dig. 2019, 111, 833–838. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transition Group (n = 185) | No-Transition Group (n = 93) | p Value | ||
|---|---|---|---|---|
| Gender male, n (%) | 115 (62) | 54 (58) | N.S. | |
| Age at diagnosis, years (median, IQR) | 12 (1–17) | 12 (3–17) | N.S. | |
| Age at transfer, years (median, IQR) | 17 (14–20) | 16 (14–20) | <0.01 | |
| Disease duration at transfer, months (median, IQR) | 54 (12–211) | 51 (12–171) | N.S. | |
| Family history of IBD, n (%) | 26 (14) | 24 (26) | <0.05 | |
| Smokers, n (%) | 11 (6) | 3 (3) | N.S. | |
| EIM, n (%) | 30 (16) | 16 (17) | N.S. | |
| Psychiatric comorbidity, n (%) | 37 (20.1) | 8 (8.7) | <0.05 | |
| IBD type, n (%) | CD: 106 (57) UC: 73 (40) IBD unclassified: 6 (3) | CD: 52 (56) UC: 38 (41) IBD unclassified: 3 (3) | N.S. | |
| UC † (n = 120) | UC extent, n (%) | Ulcerative proctitis: 13 (17) Left-sided UC: 13 (17) Extensive UC: 11 (14) Pancolitis: 42 (52) | Ulcerative proctitis: 3 (7) Left-sided UC: 8 (19) Extensive UC: 8 (19) Pancolitis: 22 (55) | N.S. |
| UC severity, n (%) | Never severe: 51 (65) Ever severe: 28 (35) | Never severe: 30 (73) Ever severe: 11 (27) | N.S. | |
| CD (n = 158) | CD location, n (%) ‡ | Distal 1/3 ileal ± limited cecal disease: 25 (24) Colonic: 8 (8) Ileocolonic: 66 (62) Upper disease proximal to Treitz: 26 (25) Upper disease distal to Treitz: 11 (10) | Distal 1/3 ileal ± limited cecal disease: 7 (14) Colonic: 9 (17) Ileocolonic: 36 (69) Upper disease proximal to Treitz: 11 (21) Upper disease distal to Treitz: 1 (2) | N.S. |
| CD behaviour, n (%) | Inflammatory: 86 (81) Stricturing: 16 (15) Penetrating: 3 (3) Penetrating and stricturing: 1 (1) | Inflammatory: 47 (90) Stricturing: 2 (4) Penetrating: 3 (6) Penetrating and stricturing: 0 (0) | N.S. | |
| Growth delay, n (%) | 20 (19) | 6 (12) | N.S. | |
| Perianal disease, n (%) | 32 (30) | 10 (19) | N.S. | |
| Transition Group (n = 22) | No-Transition Group (n = 12) | p Value | |
|---|---|---|---|
| Third-level hospital (paediatric unit), n (%) | 17 (77) | 6 (50) | N.S. |
| Third-level hospital (gastroenterology unit), n (%) | 16 (73) | 6 (50) | N.S. |
| Paediatric IBD unit (yes), n (%) | 15 (68) | 1 (8) | <0.01 |
| Gastroenterology IBD unit (yes), n (%) | 22 (100) | 8 (67) | <0.01 |
| IBD patients followed-up in paediatric units (median, IQR) | 28 (43) | 15 (70) | N.S. |
| IBD patients followed-up in gastroenterology units (median, IQR) | 1700 (1126) | 1075 (1250) | N.S. |
| Transition programme starting date, n (%) | <2010: 1 (4) 2010–2015: 8 (37) 2016–2020: 12 (55) >2020: 1 (4) | NA | NA |
| Transfer type (no-transition), n (%) | NA | IBD specialist: 11 (92) General gastroenterologist: 1 (8) | NA |
| Number of patients transferred per year (median, IQR) | 3 (3) | NA | |
| Transition place, n (%) | Paediatric clinic: 3 (14) Gastroenterology clinic: 10 (45) Both clinic: 9 (41) | NA | NA |
| Number of joint visits (mean ± SD) | 1.5 ± 0.8 | NA | NA |
| Transition duration (median, IQR), months | 6 (6) | NA | NA |
| Professionals involved in transition, n (%) | Paediatrician and gastroenterologist: 21 (100) Paediatric nurse: 7 (33) Gastroenterology nurse 13 (62) Nutritionist: 1 (5) Social worker: 0 (0) | NA | NA |
| Paediatrician focused on IBD, n (%) | 19 (91) | NA | NA |
| Gastroenterologist focused on IBD, n (%) | 21 (100) | NA | NA |
| OUTCOMES BEFORE TRANSFER | |||
|---|---|---|---|
| Transition Group (n = 185) | No-Transition Group (n = 93) | p Value | |
| Emergency visits, n (%) | 57 (31) | 44 (47) | <0.01 |
| Hospitalisations, n (%) | 77 (42) | 44 (47) | N.S. |
| Surgeries, n (%) | 23 (12) | 7 (8) | N.S. |
| IBD-related treatments, n (%) | Aminosalicylates: 94 (51) Topic treatment: 50 (27) Corticosteroids: 91 (49) IMM: 145 (78) Biologic drugs: 100 (54) EEN: 58 (31) Apheresis: 5 (3) Nutritional support: 21 (11) | Aminosalicylates: 59 (63) Topic treatment: 28 (30) Corticosteroids: 55 (59) IMM: 76 (82) Biologic drugs: 38 (41) EEN:31 (33) Apheresis: 2 (2) Nutritional support: 17 (18) | <0.05 N.S. N.S. N.S. <0.05 N.S. N.S. N.S. |
| OUTCOMES ONE YEAR AFTER TRANSFER | |||
| IBD flare, n (%) | 41 (22) | 33 (36) | <0.05 |
| Emergency visits, n (%) | 18 (10) | 16 (17) | N.S. |
| Hospitalisations, n (%) | 6 (3) | 9 (10) | <0.05 |
| Surgeries, n (%) | 2 (1) | 3 (3) | N.S. |
| IBD-related treatments, n (%) | Aminosalicylates: 74 (40) Topic treatment: 20 (11) Corticosteroids: 9 (5) IMM: 95 (51) Biologic drugs: 98 (53) Nutritional support: 2 (1) | Aminosalicylates: 44 (47) Topic treatment: 7 (8) Corticosteroids: 15 (16) IMM: 58 (62) Biologic drugs: 44 (47) Nutritional support: 1 (1) | N.S. N.S. <0.01 N.S. N.S. N.S. |
| Factor | HR | 95% CI |
|---|---|---|
| No transition | 2.1 | 1.3–3.3 |
| IBD activity at transfer | 4.9 | 3.1–7.9 |
| BMI < 18.5 at transfer | 1.9 | 1.1–3.3 |
| Corticosteroids at transfer | 4.9 | 2.2–10.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubín de Célix, C.; Martín-de-Carpi, J.; Pujol-Muncunill, G.; Palomino, L.M.; Velasco Rodríguez-Belvís, M.; Martín-Masot, R.; Navas-López, V.M.; Ricart, E.; Casanova, M.J.; Rodríguez-Martínez, A.; et al. Benefits of Paediatric to Adult Transition Programme in Inflammatory Bowel Disease: The BUTTERFLY Study of GETECCU and SEGHNP. J. Clin. Med. 2023, 12, 4813. https://doi.org/10.3390/jcm12144813
Rubín de Célix C, Martín-de-Carpi J, Pujol-Muncunill G, Palomino LM, Velasco Rodríguez-Belvís M, Martín-Masot R, Navas-López VM, Ricart E, Casanova MJ, Rodríguez-Martínez A, et al. Benefits of Paediatric to Adult Transition Programme in Inflammatory Bowel Disease: The BUTTERFLY Study of GETECCU and SEGHNP. Journal of Clinical Medicine. 2023; 12(14):4813. https://doi.org/10.3390/jcm12144813
Chicago/Turabian StyleRubín de Célix, Cristina, Javier Martín-de-Carpi, Gemma Pujol-Muncunill, Laura María Palomino, Marta Velasco Rodríguez-Belvís, Rafael Martín-Masot, Víctor Manuel Navas-López, Elena Ricart, María José Casanova, Alejandro Rodríguez-Martínez, and et al. 2023. "Benefits of Paediatric to Adult Transition Programme in Inflammatory Bowel Disease: The BUTTERFLY Study of GETECCU and SEGHNP" Journal of Clinical Medicine 12, no. 14: 4813. https://doi.org/10.3390/jcm12144813