
Development of Antibodies to Ustekinumab Is Associated with Loss of Response in Patients with Inflammatory Bowel Disease
 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
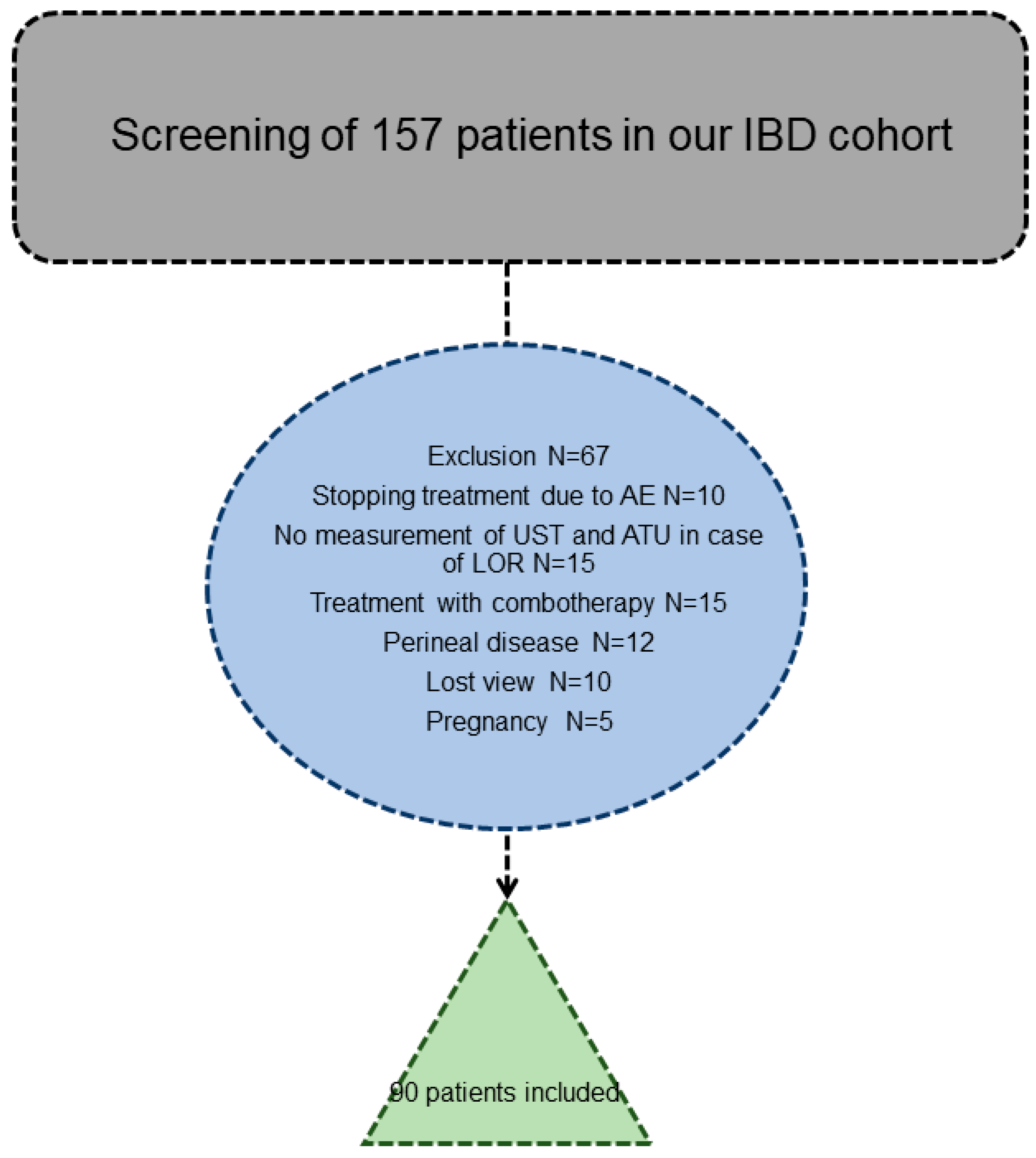
2.1. Study Design, Disease Outcomes and Patient Characteristics
2.2. Therapeutic Drug Monitoring
2.3. Statistical Analysis
3. Results
3.1. Patient’s Characteristics
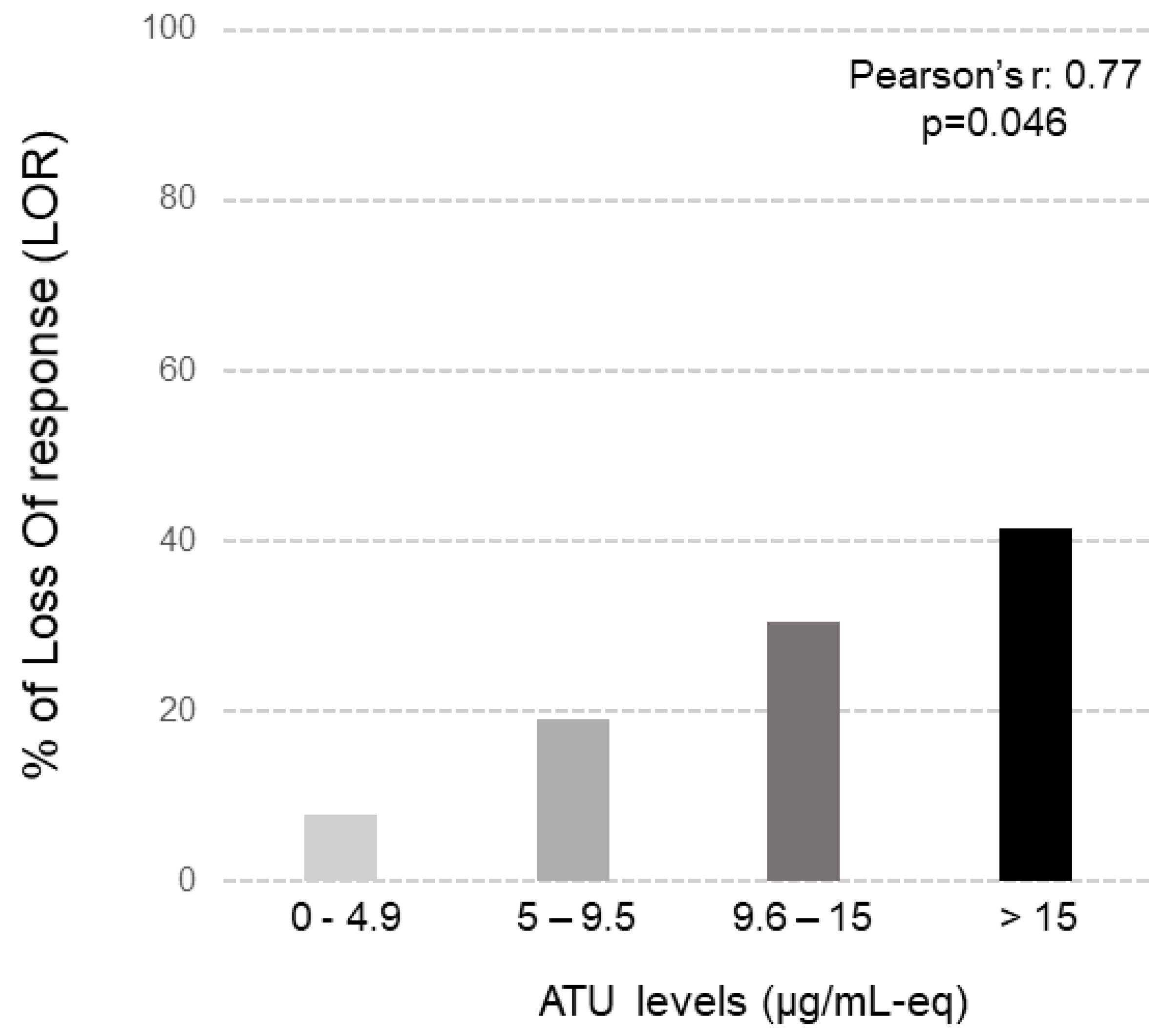
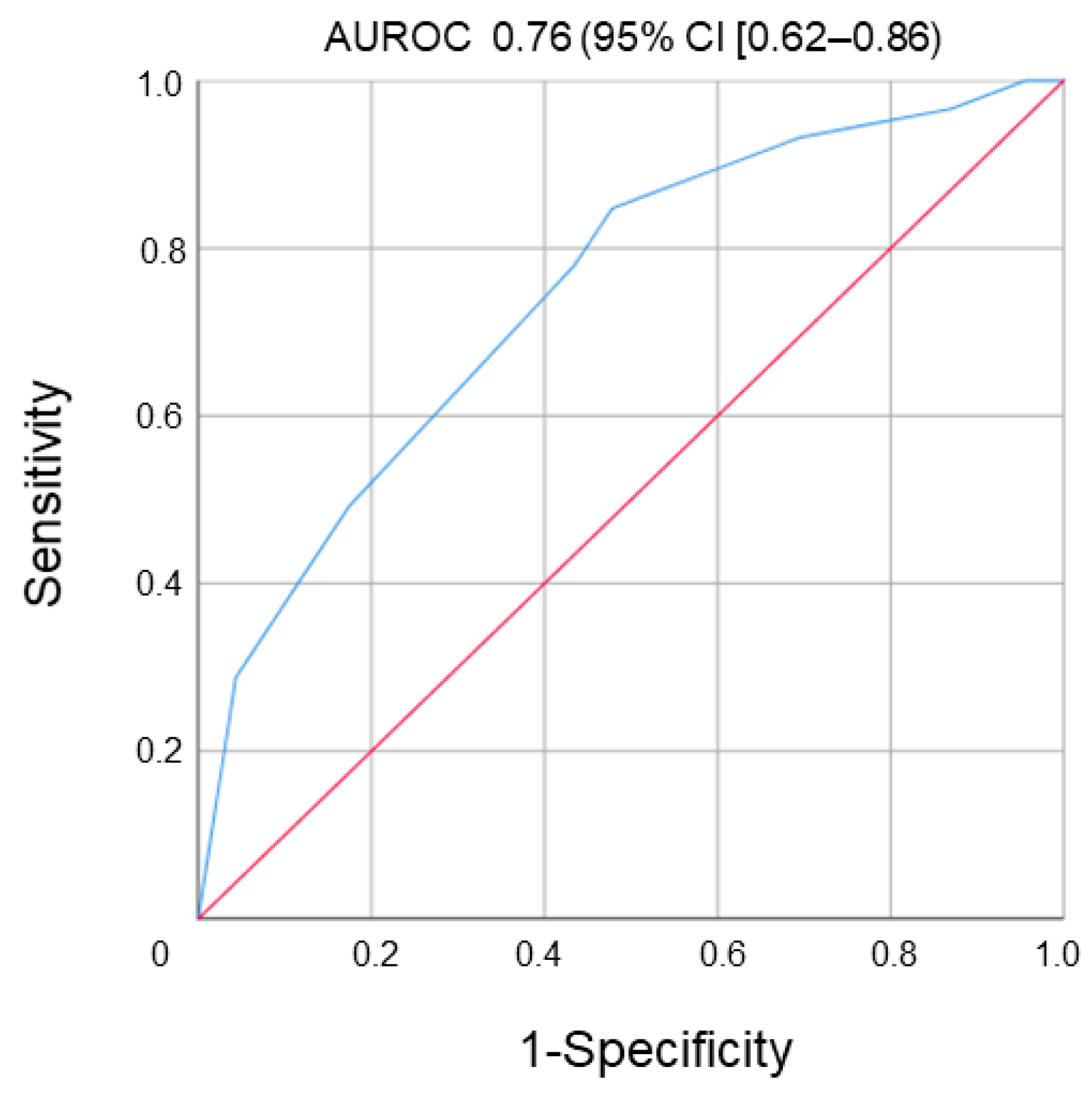
3.2. Therapeutic Drug Monitoring
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATU | antibodies to ustekinumab |
| CD | Crohn’s disease |
| CRP | C-reactive protein |
| LOR | loss of response |
| PK | pharmacokinetics |
| ROC | receiver operating characteristic |
| UST | ustekinumab |
| TNF | tumor necrosis factor |
| iv | intravenous |
| sc | subcutaneous |
| SCR | sustained clinical response |
| IQR | interquartile range |
References
- Kennedy, N.A.; Heap, G.A.; Green, H.D.; Hamilton, B.; Bewshea, C.; Walker, G.J.; Thomas, A.; Nice, R.; Perry, M.H.; Bouri, S.; et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: A prospective, multicentre, cohort study. Lancet Gastroenterol. Hepatol. 2019, 4, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Casteele, N.V.; Herfarth, H.; Katz, J.; Falck-Ytter, Y.; Singh, S. American Gastroenterological Association Institute Technical Review on the Role of Therapeutic Drug Monitoring in the Management of Inflammatory Bowel Diseases. Gastroenterology 2017, 153, 835–857.e6. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.-L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Fedorak, R.; Scherl, E.; Fleisher, M.R.; Katz, S.; Johanns, J.; Blank, M.; Rutgeerts, P. A Randomized Trial of Ustekinumab, a Human Interleukin-12/23 Monoclonal Antibody, in Patients With Moderate-to-Severe Crohn’s Disease. Gastroenterology 2008, 135, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Gasink, C.; Gao, L.-L.; Blank, M.A.; Johanns, J.; Guzzo, C.; Sands, B.E.; Hanauer, S.B.; Targan, S.; Rutgeerts, P.; et al. Ustekinumab Induction and Maintenance Therapy in Refractory Crohn’s Disease. N. Engl. J. Med. 2012, 367, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Xu, Z.; Gasink, C.; Jacobstein, D.; Szapary, P.; Johanns, J.; Gao, L.-L.; Davis, H.M.; Hanauer, S.B.; Feagan, B.G.; et al. Pharmacokinetics and Exposure Response Relationships of Ustekinumab in Patients With Crohn’s Disease. Gastroenterology 2018, 154, 1660–1671. [Google Scholar] [CrossRef] [PubMed]
- Hanžel, J.; Zdovc, J.; Kurent, T.; Sever, N.; Javornik, K.; Tuta, K.; Koželj, M.; Smrekar, N.; Novak, G.; Štabuc, B.; et al. Peak Concentrations of Ustekinumab After Intravenous Induction Therapy Identify Patients With Crohn’s Disease Likely to Achieve Endoscopic and Biochemical Remission. Clin. Gastroenterol. Hepatol. 2020, 19, 111–118.e10. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Xu, Z.; Marano, C.; O’brien, C.; Szapary, P.; Zhang, H.; Johanns, J.; Leong, R.W.; Hisamatsu, T.; Van Assche, G.; et al. Ustekinumab Pharmacokinetics and Exposure Response in a Phase 3 Randomized Trial of Patients With Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2020, 18, 2244–2255.e9. [Google Scholar] [CrossRef] [PubMed]
- Ungaro, R.C.; Yzet, C.; Bossuyt, P.; Baert, F.J.; Vanasek, T.; D’haens, G.R.; Joustra, V.W.; Panaccione, R.; Novacek, G.; Reinisch, W.; et al. Deep Remission at 1 Year Prevents Progression of Early Crohn’s Disease. Gastroenterology 2020, 159, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S.; Mazor, Y.; Yanai, H.; Ron, Y.; Kopylov, U.; Yavzori, M.; Picard, O.; Fudim, E.; Lahat, A.; Coscas, D.; et al. The decline of anti-drug antibody titres after discontinuation of anti-TNFs: Implications for predicting re-induction outcome in IBD. Aliment. Pharmacol. Ther. 2012, 35, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S.; Ungar, B.; Kopylov, U.; Lahat, A.; Yavzori, M.; Fudim, E.; Picard, O.; Peled, Y.; Eliakim, R.; Del Tedesco, E.; et al. Safety, efficacy and pharmacokinetics of vedolizumab in patients with simultaneous exposure to an anti-tumour necrosis factor. Aliment. Pharmacol. Ther. 2018, 47, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S.; Yavzori, M.; Benhar, I.; Fudim, E.; Picard, O.; Ungar, B.; Lee, S.; Kim, S.; Eliakim, R.; Chowers, Y. Cross-immunogenicity: Antibodies to infliximab in Remicade-treated patients with IBD similarly recognise the biosimilar Remsima. Gut 2016, 65, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S.; Yavzori, M.; Katz, L.; Kopylov, U.; Picard, O.; Fudim, E.; Coscas, D.; Bar-Meir, S.; Goldstein, I.; Chowers, Y. The immunogenic part of infliximab is the F(ab’)2, but measuring antibodies to the intact infliximab molecule is more clinically useful. Gut 2011, 60, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Mazor, Y.; Yavzori, M.; Fudim, E.; Katz, L.; Coscas, D.; Picard, O.; Chowers, Y.; Eliakim, R.; Ben-Horin, S. Clinical utility of antihuman lambda chain-based enzyme-linked immunosorbent assay (ELISA) versus double antigen ELISA for the detection of anti-infliximab antibodies. Inflamm. Bowel Dis. 2012, 18, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Hanauer, S.B.; Sandborn, W.J.; Feagan, B.G.; Gasink, C.; Jacobstein, D.; Zou, B.; Johanns, J.; Adedokun, O.J.; Sands, B.E.; Rutgeerts, P.; et al. IM-UNITI: Three-year Efficacy, Safety, and Immunogenicity of Ustekinumab Treatment of Crohn’s Disease. J. Crohn’s Colitis 2020, 14, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Philipp, S.; Menter, A.; Nikkels, A.; Barber, K.; Landells, I.; Eichenfield, L.; Song, M.; Randazzo, B.; Li, S.; Hsu, M.; et al. Ustekinumab for the treatment of moderate-to-severe plaque psoriasis in paediatric patients (≥6 to <12 years of age): Efficacy, safety, pharmacokinetic and biomarker results from the open-label CADMUS Jr study. Br. J. Dermatol. 2020, 183, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Puig, L.; Gottlieb, A.B.; Ritchlin, C.; Li, S.; Wang, Y.; Mendelsohn, A.M.; Song, M.; Zhu, Y.; Rahman, P.; et al. Maintenance of Clinical Efficacy and Radiographic Benefit Through Two Years of Ustekinumab Therapy in Patients With Active Psoriatic Arthritis: Results From a Randomized, Placebo-Controlled Phase III Trial. Arthritis Care Res. 2015, 67, 1739–1749. [Google Scholar] [CrossRef] [PubMed]
- Yzet, C.; Brazier, F.; Fumery, M. Reply. Clin. Gastroenterol. Hepatol. 2021, 19, 2214–2215. [Google Scholar] [CrossRef] [PubMed]
- Yzet, C.; Diouf, M.; Singh, S.; Brazier, F.; Turpin, J.; Nguyen-Khac, E.; Meynier, J.; Fumery, M. No Benefit of Concomitant Immunomodulator Therapy on Efficacy of Biologics That Are Not Tumor Necrosis Factor Antagonists in Patients With Inflammatory Bowel Diseases: A Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 668–679.e8. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; Barsky, M.; Ahmed, W.; Zullow, S.; Galati, J.; Jairath, V.; Narula, N.; Peerani, F.; Click, B.H.; Coburn, E.S.; et al. The Real-World Effectiveness and Safety of Ustekinumab in the Treatment of Crohn’s Disease: Results From the SUCCESS Consortium. Am. J. Gastroenterol. 2023, 118, 317–328. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total | No LOR | LOR | p |
|---|---|---|---|---|
| Sex Ratio male/Female | 1.1 | 1.0 | 1.1 | 0.870 |
| Age (years) Mean ± SD | 38.7 ± 6.3 | 37.4 ± 4.1 | 39.5 ± 7.2 | 0.760 |
| Disease duration (years) median, (IQR) | 8.5 (4.2–11.3) | 7.7 (3.9–10.6) | 9.9 (5.2–10.5) | 0.450 |
| Active smoking, n (%) | 54 (60) | 36 (66) | 18 (50) | 0.320 |
| IBD type, n (%) | 0.660 | |||
| CD | 78 (86) | 48 (88) | 30 (83) | |
| UC | 12 (14) | 6 (12) | 6 (17) | |
| CD behavior, n (%) | 0.320 | |||
| B1 | 24 (38) | 16 (33) | 8 (26) | |
| B2 | 18 (22) | 12 (25) | 6 (20) | |
| B3 | 36 (40) | 20 (41) | 16 (54) | |
| CD (location %) | 0.23 | |||
| L1 | 32 (41) | 20 (41) | 12 (40) | |
| L2 | 11 (14) | 9 (19) | 2 (7) | |
| L3 | 35 (45) | 19 (40) | 16 (53) | |
| UC extension, n (%) | 0.830 | |||
| E1 | 2 (17) | 1 (17) | 1 (17) | |
| E2 | 6 (50) | 4 (66) | 2 (34) | |
| E3 | 4 (33) | 1 (17) | 3 (49) | |
| CDAI at inclusion, median, (IQR) | 280 (240–330) | 270 (245–325) | 285 (250–340) | 0.540 |
| Full Mayo score, n | 8 (8–9) | 8 (7–8) | 8 (8–9) | 0.890 |
| Previous treatments, n (%) | ||||
| -at least 1 anti-TNF | 79 (80) | 49 (90) | 30 (83) | 0.210 |
| -2 anti-TNFs | 36 (40) | 21 (38) | 15 (41) | 0.670 |
| -Vedolizumab | 27 (30) | 11 (20) | 16 (45) | 0.040 |
| -AZA | 30 (33) | 21 (39) | 9 (25) | 0.030 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p | HR (95% CI) | p | HR (95% CI) | |
| Gender (male vs. female) | 0.870 | 0.95 (0.29–4.02) | ||
| Age | 0.760 | 0.88 (0.56–3.55) | ||
| Ustekinumab trough concentrations <4.5 µg/mL | 0.450 | 1.18 (0.74–4.23) | ||
| ATU ≥ 9.5 μg/mL-eq | 0.045 | 2.81 (1.35–4.91) | 0.022 | 2.54 (1.80–5.93) |
| UC vs. CD | 0.300 | 1.40 (0.74–2.65) | ||
| Prior vedolizumab therapy | 0.060 | 1.56 (0.98–1.39) | 0.019 | 2.78 (1.09–3.34) |
| Prior azathioprine therapy | 0.028 | 0.66 (0.52–0.82) | 0.014 | 0.54 (0.20–0.76) |
| Active smoking | 0.650 | 1.12 (0.40–3.55) | ||
| Duration of disease | 0.450 | 0.67 (0.26–9.21) | ||
| Prior use of two anti-TNFs | 0.670 | 1.12 (0.32–8.72) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roblin, X.; Duru, G.; Papamichael, K.; Cheifetz, A.S.; Kwiatek, S.; Berger, A.-E.; Barrau, M.; Waeckel, L.; Nancey, S.; Paul, S. Development of Antibodies to Ustekinumab Is Associated with Loss of Response in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2023, 12, 3395. https://doi.org/10.3390/jcm12103395
Roblin X, Duru G, Papamichael K, Cheifetz AS, Kwiatek S, Berger A-E, Barrau M, Waeckel L, Nancey S, Paul S. Development of Antibodies to Ustekinumab Is Associated with Loss of Response in Patients with Inflammatory Bowel Disease. Journal of Clinical Medicine. 2023; 12(10):3395. https://doi.org/10.3390/jcm12103395
Chicago/Turabian StyleRoblin, Xavier, Gérard Duru, Konstantinos Papamichael, Adam S. Cheifetz, Sandy Kwiatek, Anne-Emmanuelle Berger, Mathilde Barrau, Louis Waeckel, Stephane Nancey, and Stephane Paul. 2023. "Development of Antibodies to Ustekinumab Is Associated with Loss of Response in Patients with Inflammatory Bowel Disease" Journal of Clinical Medicine 12, no. 10: 3395. https://doi.org/10.3390/jcm12103395