
Assessment by Optical Coherence Tomography of Short-Term Changes in IOP-Related Structures Caused by Wearing Scleral Lenses

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scleral Contact Lenses
2.2. Measurement of IOP
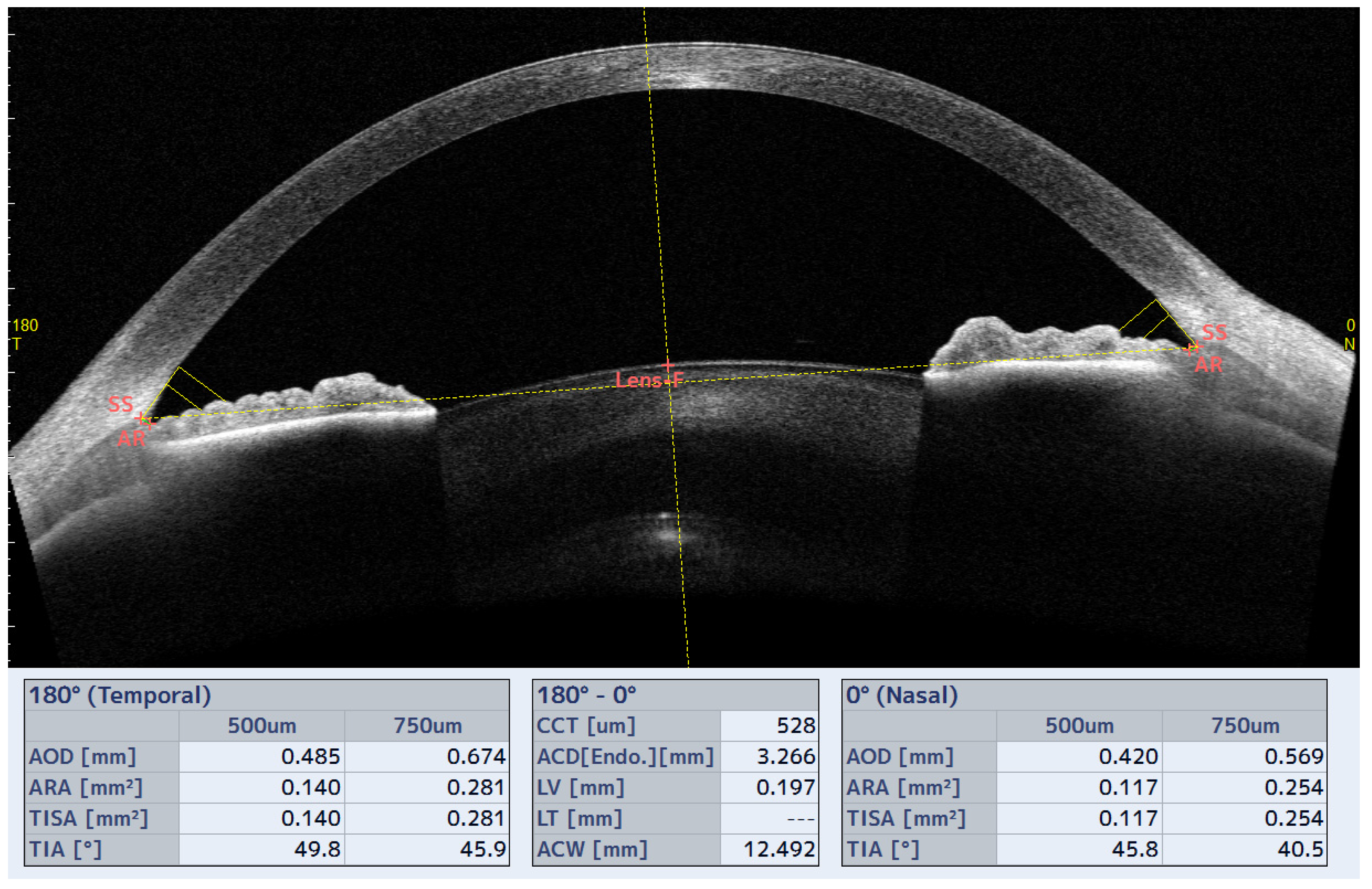
2.3. Measurement of Iridocorneal Angle (ICA) and Schlemm Channel (SC) Parameters
2.4. Measurement of Optic Nerve Head Parameters
2.5. Statistical Analysis
3. Results
3.1. Scleral Contact Lenses
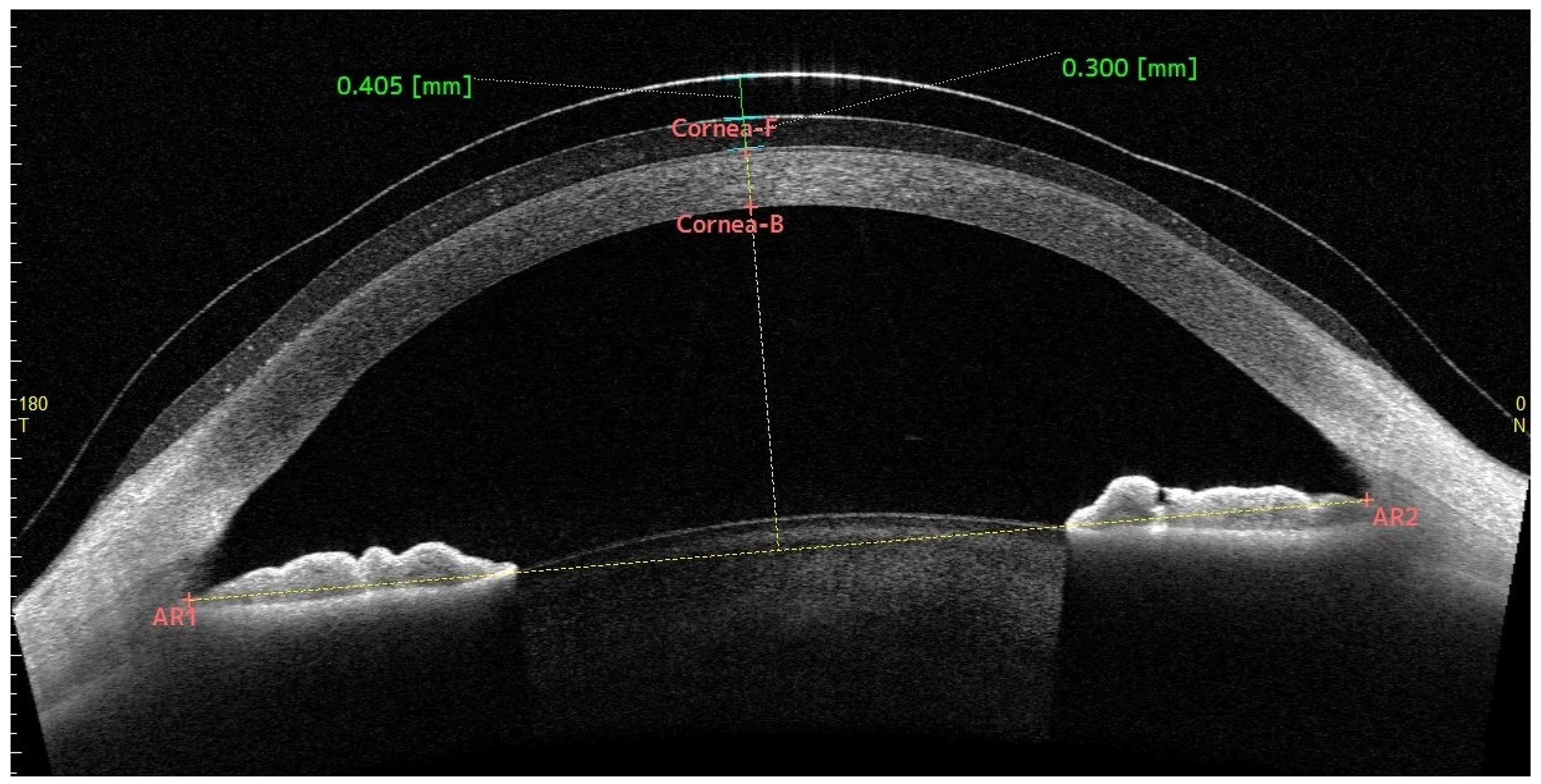
3.2. Central Fluid Reservoir
3.3. Central Corneal Thickness
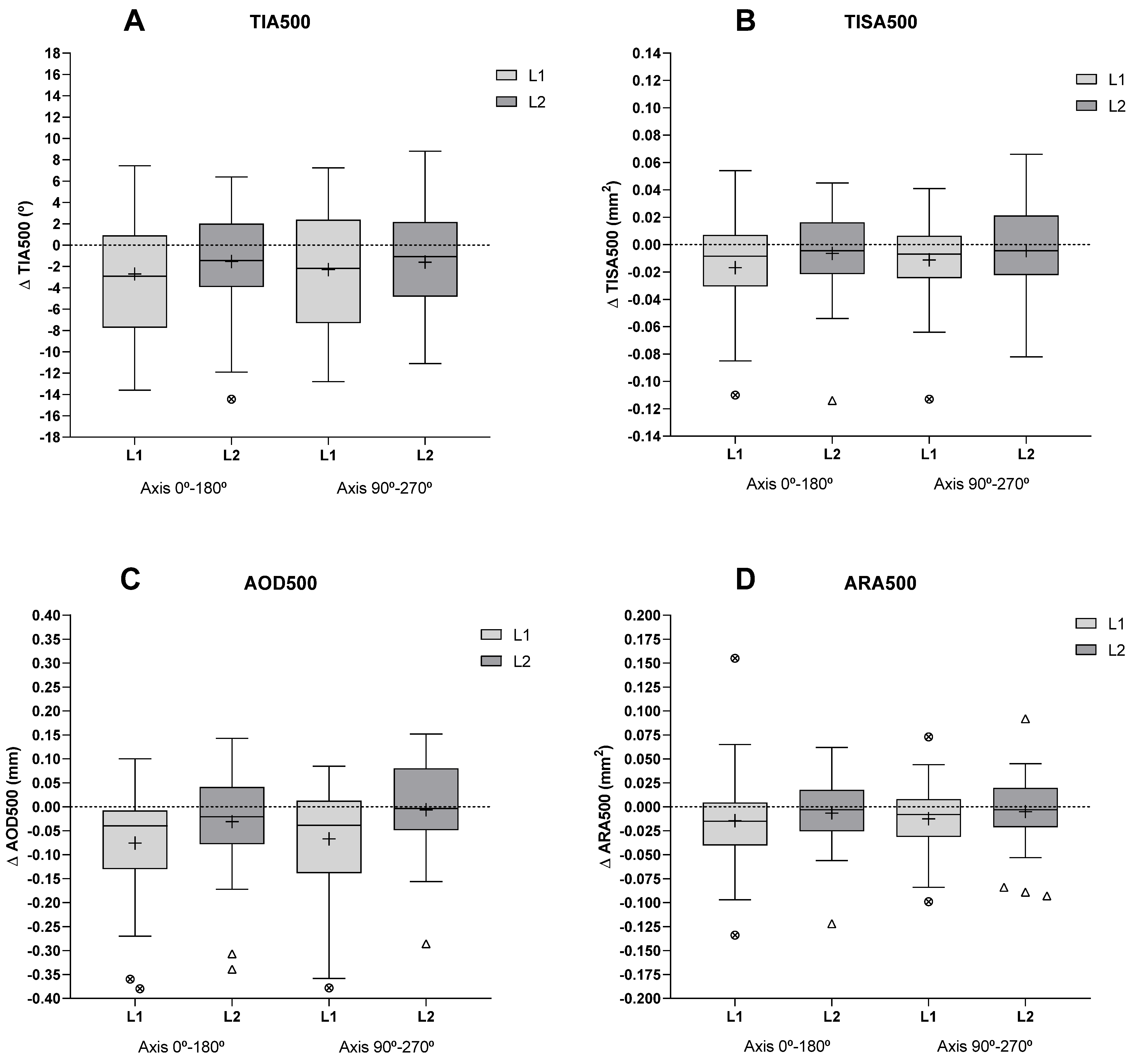
3.4. Iridocorneal Angle and Schlemm’s Canal Parameters
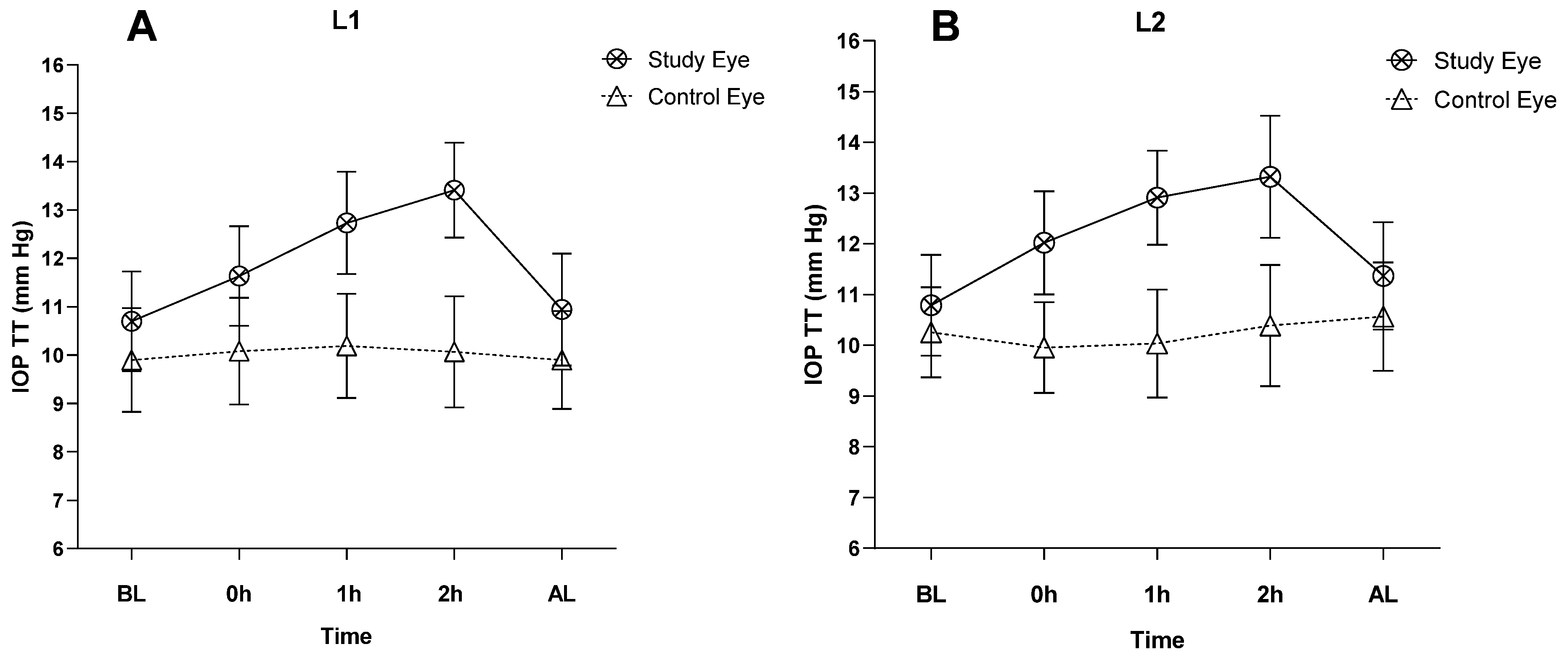
3.5. Intraocular Pressure (IOP)
3.6. Optic Nerve Head Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ΔIOP TT | ΔIOP PAT | ||||
|---|---|---|---|---|---|
| Lens | Correlation | p | Correlation | p | |
| ICA parameters | |||||
| ΔTIA500 0–180° axis (°) | L1 | 0.19 | 0.31 | −0.23 | 0.22 |
| L2 | −0.27 | 0.21 | 0.03 | 0.89 | |
| ΔTIA500 90–270° axis (°) | L1 | 0.24 | 0.21 | −0.26 | 0.17 |
| L2 | 0.02 | 0.94 | 0.19 | 0.32 | |
| ΔTISA500 0–180° axis (mm2) | L1 | 0.21 | 0.24 | −0.21 | 0.27 |
| L2 | −0.04 | 0.82 | 0.05 | 0.81 | |
| ΔTISA500 90–270° axis (mm2) | L1 | 0.22 | 0.25 | 0.05 | 0.79 |
| L2 | −0.11 | 0.57 | 0.22 | 0.25 | |
| ΔAOD500 0–180° axis (mm) | L1 | 0.32 | 0.09 | 0.08 | 0.69 |
| L2 | 0.13 | 0.50 | 0.05 | 0.81 | |
| ΔAOD500 90–270° axis (mm) | L1 | 0.29 | 0.12 | 0.15 | 0.42 |
| L2 | −0.04 | 0.83 | 0.15 | 0.43 | |
| ΔARA500 0–180° axis (mm2) | L1 | 0.14 | 0.46 | −0.12 | 0.52 |
| L2 | 0.10 | 0.59 | 0.08 | 0.66 | |
| ΔARA500 90–270° axis (mm2) | L1 | 0.10 | 0.59 | −0.09 | 0.64 |
| L2 | −0.10 | 0.59 | 0.04 | 0.85 | |
| ΔITC index (%) | L1 | 0.08 | 0.67 | 0.44 | 0.02 * |
| L2 | 0.09 | 0.64 | 0.45 | 0.01 * | |
| SC parameters | |||||
| SC Nasal Lenght (µm) | L1 | 0.07 | 0.71 | 0.05 | 0.78 |
| L2 | 0.26 | 0.16 | 0.16 | 0.42 | |
| SC Temp. Lenght (µm) | L1 | 0.29 | 0.12 | 0.19 | 0.32 |
| L2 | −0.11 | 0.58 | 0.05 | 0.81 | |
| SC Nasal Área (µm2) | L1 | −0.19 | 0.31 | 0.24 | 0.21 |
| L2 | 0.26 | 0.17 | 0.14 | 0.45 | |
| SC Temp. Área (µm2) | L1 | 0.00 | 1.00 | −0.03 | 0.87 |
| L2 | −0.07 | 0.71 | 0.03 | 0.88 | |
Appendix B
| Study Eye (Right Eye) | Control Eye (Left Eye) | |||||
|---|---|---|---|---|---|---|
| Parameters | Lens | Correlation | p | Correlation | p | |
| Δ IOP TT (mmHg) | ΔRNFL (µm) | L1 | −0.10 | 0.60 | −0.41 | 0.02 * |
| L2 | 0.04 | 0.85 | 0.15 | 0.42 | ||
| ΔNRA (µm2) | L1 | −0.37 | 0.04 * | 0.15 | 0.44 | |
| L2 | 0.00 | 0.99 | 0.25 | 0.19 | ||
| ΔNRV (µm3) | L1 | −0.34 | 0.07 | 0.07 | 0.73 | |
| L2 | 0.00 | 0.99 | 0.25 | 0.18 | ||
| Δ IOP PAT (mmHg) | ΔRNFL (µm) | L1 | 0.33 | 0.07 | −0.34 | 0.06 |
| L2 | 0.05 | 0.81 | −0.10 | 0.58 | ||
| ΔNRA (µm2) | L1 | 0.11 | 0.56 | 0.19 | 0.30 | |
| L2 | 0.13 | 0.50 | −0.35 | 0.06 | ||
| ΔNRV (µm3) | L1 | 0.12 | 0.52 | 0.25 | 0.19 | |
| L2 | −0.12 | 0.52 | −0.46 | 0.01 * | ||
References
- Michaud, L.; Samaha, D.; Giasson, C.J. Intra-Ocular Pressure Variation Associated with the Wear of Scleral Lenses of Different Diameters. Contact Lens Anterior Eye 2019, 42, 104–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fogt, J.S.; Nau, C.B.; Schornack, M.; Shorter, E.; Nau, A.; Harthan, J.S. Comparison of Pneumatonometry and Transpalpebral Tonometry Measurements of Intraocular Pressure during Scleral Lens Wear. Optom. Vis. Sci. 2020, 97, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Aitsebaomo, A.P.; Wong-Powell, J.; Miller, W.; Amir, F. Influence of Scleral Lens on Intraocular Pressure. J. Contact Lens Res. Sci. 2019, 3, e1–e9. [Google Scholar] [CrossRef] [Green Version]
- Formisano, M.; Franzone, F.; Alisi, L.; Pistella, S.; Spadea, L. Effects of Scleral Contact Lenses for Keratoconus Management on Visual Quality and Intraocular Pressure. Ther. Clin. Risk Manag. 2021, 17, 79–85. [Google Scholar] [CrossRef]
- Cheung, S.Y.; Collins, M.J.; Vincent, S.J. The Impact of Short-Term Fenestrated Scleral Lens Wear on Intraocular Pressure. Contact Lens Anterior Eye 2020, 43, 585–588. [Google Scholar] [CrossRef]
- Kramer, E.G.; Vincent, S.J. Intraocular Pressure Changes in Neophyte Scleral Lens Wearers: A Prospective Study. Contact Lens Anterior Eye 2020, 43, 609–612. [Google Scholar] [CrossRef]
- Porcar, E.; Montalt, J.C.; España-Gregori, E.; Peris-Martínez, C. Impact of Corneoscleral Contact Lens Usage on Corneal Biomechanical Parameters in Keratoconic Eyes. Eye Contact Lens 2019, 45, 318–323. [Google Scholar] [CrossRef]
- Walker, M.K.; Pardon, L.P.; Redfern, R.; Patel, N. IOP and Optic Nerve Head Morphology during Scleral Lens Wear. Optom. Vis. Sci. 2020, 97, 661–668. [Google Scholar] [CrossRef]
- Lam, A.K.C.; Lam, C.H.; Chan, R. The Validity of a Digital Eyelid Tonometer (TGDc-01) and Its Comparison with Goldmann Applanation Tonometry—A Pilot Study. Ophthalmic Physiol. Opt. 2005, 25, 205–210. [Google Scholar] [CrossRef]
- Doherty, M.D.; Carrim, Z.I.; O’Neill, D.P. Diaton Tonometry: An Assessment of Validity and Preference against Goldmann Tonometry. Clin. Exp. Ophthalmol. 2012, 40, e171–e175. [Google Scholar] [CrossRef]
- Wisse, R.P.L.; Peeters, N.; Imhof, S.M.; van der Lelij, A. Comparison of Diaton Transpalpebral Tonometer with Applanation Tonometry in Keratoconus. Int. J. Ophthalmol. 2016, 18, 395–398. [Google Scholar] [CrossRef]
- Lee, J.H.; Sanchez, L.R.; Porco, T.; Han, Y.; Campomanes, A.G.D.A. Correlation of Corneal and Scleral Pneumatonometry in Pediatric Patients. Ophthalmology 2018, 125, 1209–1214. [Google Scholar] [CrossRef] [Green Version]
- Kapamajian, M.A.; De Cruz, J.; Hallak, J.A.; Vajaranant, T.S. Correlation Between Corneal and Scleral Pneumatonometry: An Alternative Method for Intraocular Pressure Measurement. Am. J. Ophthalmol. 2013, 156, 902–906.e1. [Google Scholar] [CrossRef]
- Nau, C.B.; Schornack, M.M.; Mclaren, J.W.; Sit, A.J. Intraocular Pressure after 2 Hours of Small-Diameter Scleral Lens Wear. Eye Contact Lens 2016, 42, 350–353. [Google Scholar] [CrossRef] [Green Version]
- Fedotova, K.; Zhu, W.; Astakhov, S.Y.; Novikov, S.A.; Grabovetskiy, V.R.; Nikolaenko, V.P. Intraocular Pressure with Miniscleral Contact Lenses. Vestn. Oftalmol. 2021, 137, 52–58. [Google Scholar] [CrossRef]
- Esen, F.; Toker, E. Influence of Apical Clearance on Mini-Scleral Lens Settling, Clinical Performance, and Corneal Thickness Changes. Eye Contact Lens Sci. Clin. Pract. 2017, 43, 230–235. [Google Scholar] [CrossRef]
- Vincent, S.J.; Alonso-Caneiro, D.; Collins, M.J. Evidence on Scleral Contact Lenses and Intraocular Pressure. Clin. Exp. Optom. 2017, 100, 87–88. [Google Scholar] [CrossRef] [Green Version]
- McMonnies, C.W. A Hypothesis That Scleral Contact Lenses Could Elevate Intraocular Pressure. Clin. Exp. Optom. 2016, 99, 594–596. [Google Scholar] [CrossRef] [Green Version]
- Lotocky, J.; Cosgrove, J.; Slate, F. Do Scleral Lenses Suck? An Analysis of What Really Happens as Scleral Lenses “Settle”. In Proceedings of the Global Specialty Lens Symposium, Las Vegas, NV, USA, 25–27 January 2018. [Google Scholar]
- Fadel, D.; Kramer, E. Potential Contraindications to Scleral Lens Wear. Contact Lens Anterior Eye 2019, 42, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Bergmanson, J.P.G.; Martinez, J.G. Size Does Matter: What Is the Corneo-Limbal Diameter ? Clin. Exp. Optom. 2017, 100, 522–528. [Google Scholar] [CrossRef] [Green Version]
- Kauffman, M.J.; Gilmartin, C.A.; Bennett, E.S.; Bassi, C.J. A Comparison of the Short-Term Settling of Three Scleral Lens Designs. Optom. Vis. Sci. 2014, 91, 1462–1466. [Google Scholar] [CrossRef] [PubMed]
- Vincent, S.J.; Alonso-caneiro, D.; Collins, M.J.; Beanland, A.; Lam, L. Hypoxic Corneal Changes Following Eight Hours. Optom. Vis. Sci. 2016, 93, 293–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyun, Y.; Meng, C.; Kim, Y.H.; Tan, B.; Lin, M.C.; Radke, C.J. Central Corneal Edema with Scleral-Lens Wear. Curr. Eye Res. 2018, 43, 1305–1315. [Google Scholar] [CrossRef]
- Vincent, S.J.; Alonso-Caneiro, D.; Collins, M.J. Corneal Changes Following Short-Term Miniscleral Contact Lens Wear. Contact Lens Anterior Eye 2014, 37, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Michaud, L.; van der Worp, E.; Brazeau, D.; Warde, R.; Giasson, C.J. Predicting Estimates of Oxygen Transmissibility for Scleral Lenses. Contact Lens Anterior Eye 2012, 35, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Obinwanne, C.J.; Echendu, D.C.; Agbonlahor, O.; Dike, S. Changes in Scleral Tonometry and Anterior Chamber Angle after Short-Term Scleral Lens Wear. Optom. Vis. Sci. 2020, 97, 720–725. [Google Scholar] [CrossRef]
- Alonso-Caneiro, D.; Vincent, S.J.; Collins, M.J. Morphological Changes in the Conjunctiva, Episclera and Sclera Following Short-Term Miniscleral Contact Lens Wear in Rigid Lens Neophytes. Contact Lens Anterior Eye 2016, 39, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Samaha, D.; Michaud, L. Bruch Membrane Opening Minimum Rim Width Changes during Scleral Lens Wear. Eye Contact Lens 2021, 47, 295–300. [Google Scholar] [CrossRef]
- Pardon, L.P.; Harwerth, R.S.; Patel, N.B. Neuroretinal Rim Response to Transient Changes in Intraocular Pressure in Healthy Non-Human Primate Eyes. Exp. Eye Res. 2020, 193, 107978. [Google Scholar] [CrossRef]
- Shaffer, R.N. A New Classification of the Glaucomas. Trans. Am. Ophthalmol. Soc. 1960, 58, 219–225. [Google Scholar]
- Spaeth, G.L. The Normal Development of the Human Anterior Chamber Angle: A New System of Descriptive Grading. Trans. Ophthalmol. Soc. UK 1971, 91, 709–739. [Google Scholar]
- Caroline, J.P.; Andre, P.A. Scleral lens Settling. Contact Lens Spectr. 2012, 27, 1. [Google Scholar]
- Michaud, L. Variation of Clearance with Mini-Scleral Lenses. In Proceedings of the Global Specialty Lens Symposium, Las Vegas, NV, USA, 23–26 January 2014. [Google Scholar]
- Bergmanson, J.P. Clinical Ocular Anatomy and Physiology; Texas Eye Research and Technology Center: Houston, TX, USA, 2011. [Google Scholar]
- Mountford, J.; Carkeet, N.; Carney, L. Corneal Thickness Changes during Scleral Lens Wear: Effect of Gas Permeability. Int. Contact Lens Clin. 1994, 21, 19–22. [Google Scholar] [CrossRef]
- Bruce, A.S.; Brennan, N.A. Corneal Pathophysiology with Contact Lens Wear. Surv. Ophthalmol. 1990, 35, 25–58. [Google Scholar] [CrossRef]
- De Leon, J.M.S.; Tun, T.A.; Perera, S.A.; Aung, T. Angle Closure Imaging: A Review. Curr. Ophthalmol. Rep. 2013, 1, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Cumba, R.J.; Radhakrishnan, S.; Bell, N.P.; Nagi, K.S.; Chuang, A.Z.; Lin, S.C.; Mankiewicz, K.A.; Feldman, R.M. Reproducibility of Scleral Spur Identification and Angle Measurements Using Fourier Domain Anterior Segment Optical Coherence Tomography. J. Ophthalmol. 2012, 2012, 487309. [Google Scholar] [CrossRef] [Green Version]
- Macedo-de-Araújo, R.J.; van der Worp, E.; González-Méijome, J.M. In Vivo Assessment of the Anterior Scleral Contour Assisted by Automatic Profilometry and Changes in Conjunctival Shape after Miniscleral Contact Lens Fitting. J. Optom. 2019, 12, 131–140. [Google Scholar] [CrossRef]
- Fernández-Vigo, J.I.; De-Pablo-Gómez-De-Liaño, L.; Fernández-Vigo, C.; Sánchez-Guillén, I.; Santos-Bueso, E.; Martínez-de-la-Casa, J.M.; García-Feijóo, J.; Fernández-Vigo, J.Á. Quantification of Trabecular-Iris Contact and Its Prevalence by Optical Coherence Tomography in a Healthy Caucasian Population. Eur. J. Ophthalmol. 2017, 27, 417–422. [Google Scholar] [CrossRef]
- Mansouri, K.; Sommerhalder, J.; Shaarawy, T. Prospective Comparison of Ultrasound Biomicroscopy and Anterior Segment Optical Coherence Tomography for Evaluation of Anterior Chamber Dimensions in European Eyes with Primary Angle Closure. Eye 2010, 24, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Usui, T.; Tomidokoro, A.; Mishima, K.; Mataki, N.; Mayama, C.; Honda, N.; Amano, S.; Araie, M. Identification of Schlemm’s Canal and Its Surrounding Tissues by Anterior Segment Fourier Domain Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6934–6939. [Google Scholar] [CrossRef] [Green Version]
- Steglitz, K. Schlemm’s Canal under the Scanning Electron Microscope. Ophthalmic Res. 1971, 45, 37–45. [Google Scholar]
- Kagemann, L.; Wang, B.; Wollstein, G.; Ishikawa, H.; Nevins, J.E.; Nadler, Z.; Sigal, I.A.; Bilonick, R.A.; Schuman, J.S. IOP Elevation Reduces Schlemm’s Canal Cross-Sectional Area. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1805–1809. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Xu, J.; Wei, A.; Wen, W.; Chen, J.; Yu, X.; Sun, X. Spectral-Domain Optical Coherence Tomographic Assessment of Schlemm’s Canal in Chinese Subjects with Primary Open-Angle Glaucoma. Ophthalmology 2013, 120, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Kagemann, L.; Wollstein, G.; Ishikawa, H.; Bilonick, R.A.; Brennen, P.M.; Folio, L.S.; Gabriele, M.L.; Schuman, J.S. Identification and Assessment of Schlemm’s Canal by Spectral-Domain Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4054–4059. [Google Scholar] [CrossRef]
- Arora, R.; Bellamy, H.; Austin, M.W. Applanation Tonometry: A Comparison of the Perkins Handheld and Goldmann Slit Lamp-Mounted Methods. Clin. Ophthalmol. 2014, 8, 605–610. [Google Scholar] [CrossRef] [Green Version]
- Shahnazi, K.C.; Isozaki, V.L.; Chiu, G.B. Effect of Scleral Lens Wear on Central Corneal Thickness and Intraocular Pressure in Patients With Ocular Surface Disease. Eye Contact Lens Sci. Clin. Pract. 2019, 46, 341–347. [Google Scholar] [CrossRef]
- Baskaran, M.; Ho, S.W.; Tun, T.A.; How, A.C.; Perera, S.A.; Friedman, D.S.; Aung, T. Assessment of Circumferential Angle-Closure by the Iris-Trabecular Contact Index with Swept-Source Optical Coherence Tomography. Ophthalmology 2013, 120, 2226–2231. [Google Scholar] [CrossRef]
- Chong, R.S.; Sakata, L.M.; Narayanaswamy, A.K.; Ho, S.; He, M.; Baskaran, M.; Wong, T.Y.; Perera, S.A.; Aung, T. Relationship between Intraocular Pressure and Angle Configuration: An Anterior Segment OCT Study. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1650–1655. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.Y.; Burkemper, B.; Lewinger, J.P.; Jiang, X.; Pardeshi, A.A.; Richter, G.; Torres, M.; McKean-Cowdin, R.; Varma, R. Correlation between Intraocular Pressure and Angle Configuration Measured by OCT: The Chinese American Eye Study. Ophthalmol. Glaucoma 2018, 1, 158–166. [Google Scholar] [CrossRef]
- Bali, S.J.; Bhartiya, S.; Sobti, A.; Dada, T.; Panda, A. Comparative Evaluation of Diaton and Goldmann Applanation Tonometers. Ophthalmologica 2012, 228, 42–46. [Google Scholar] [CrossRef]
- Sánchez Pavón, I.; Cañadas, P.; Martin, R. Repeatability and Agreement of Intraocular Pressure Measurement among Three Tonometers. Clin. Exp. Optom. 2020, 103, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Molero-Senosiaín, M.; Morales-Fernández, L.; Saenz-Francés, F.; García-Feijoo, J.; Martínez-de-la-Casa, J.M. Analysis of Reproducibility, Evaluation, and Preference of the New IC100 Rebound Tonometer versus ICare PRO and Perkins Portable Applanation Tonometry. Eur. J. Ophthalmol. 2020, 30, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Shi, J.; Duan, X.; Fan, F. Transpalpebral Measurement of Intraocular Pressure Using the Diaton Tonometer versus Standard Goldmann Applanation Tonometry. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 1765–1770. [Google Scholar] [CrossRef]
- Patel, N.; McAllister, F.; Pardon, L.; Harwerth, R. The Effects of Graded Intraocular Pressure Challenge on the Optic Nerve Head. Exp. Eye Res. 2018, 169, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Fortune, B.; Yang, H.; Strouthidis, N.G.; Cull, G.A.; Grimm, J.L.; Downs, J.C.; Burgoyne, C.F. The Effect of Acute Intraocular Pressure Elevation on Peripapillary Retinal Thickness, Retinal Nerve Fiber Layer Thickness, and Retardance. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4719–4726. [Google Scholar] [CrossRef]
- Kamppeter, B.A.; Jonas, J.B. Fluctuations Depending on Time of Day in Measurements of the Optic Disc Using Confocal Laser Canning Tomography. Ophthalmologe 2006, 103, 40–42. [Google Scholar] [CrossRef]
- Ashraf, H.; Nowroozzadeh, M.H. Diurnal Variation of Retinal Thickness. Optom. Vis. Sci. 2014, 91, 615–623. [Google Scholar] [CrossRef]





| Characteristics | Value |
|---|---|
| Participants (n) | 30 |
| Sex (male/female) | 14/16 |
| CL wearers (yes/no) | 11/19 |
| Age (years) | 28.97 ± 5.62 |
| SAG-OC (0–180°) (µm) | 3751.80 ± 194.09 |
| SAG-OC (90–270°) (µm) | 3758.47 ± 189.50 |
| HVID (mm) | 12.09 ± 0.16 |
| SE (D) | −1.18 ± 1.39 |
| Before Lens (Mean ± SD) | After Lens (Mean ± SD) | Δ (Mean ± SD) | p | ||
|---|---|---|---|---|---|
| ICA parameters | |||||
| TIA500 0–180° (°) | L1 | 47.55 ± 14.19 | 44.80 ± 12.14 | −2.72 ± 5.33 | 0.01 * |
| L2 | 47.90 ± 13.74 | 46.43 ± 14.17 | −1.54 ± 4.86 | 0.09 | |
| TIA500 90–270° (°) | L1 | 46.71 ± 12.76 | 44.10 ± 12.50 | −2.30 ± 5.26 | 0.02 * |
| L2 | 46.46 ± 12.75 | 44.86 ± 12.59 | −1.60 ± 5.24 | 0.11 | |
| TISA500 0–180° (mm2) | L1 | 0.21 ± 0.08 | 0.20 ± 0.08 | −0.02 ± 0.04 | 0.01 * |
| L2 | 0.21 ± 0.08 | 0.20 ± 0.08 | −0.01 ± 0.03 | 0.38 | |
| TISA500 90–270° (mm2) | L1 | 0.20 ± 0.08 | 0.19 ± 0.07 | −0.01 ± 0.03 | 0.06 |
| L2 | 0.20 ± 0.07 | 0.19 ± 0.07 | 0.00 ± 0.04 | 0.43 | |
| AOD500 0–180° (mm) | L1 | 0.61 ± 0.24 | 0.53 ± 0.24 | −0.08 ± 0.12 | <0.01 * |
| L2 | 0.59 ± 0.24 | 0.56 ± 0.24 | −0.03 ± 0.11 | 0.14 | |
| AOD500 90–270° (mm) | L1 | 0.56 ± 0.23 | 0.49 ± 0.22 | −0.07 ± 0.12 | 0.00 * |
| L2 | 0.53 ± 0.18 | 0.52 ± 0.19 | −0.01 ± 0.10 | 0.72 | |
| ARA500 0–180° (mm2) | L1 | 0.23 ± 0.09 | 0.22 ± 0.09 | −0.02 ± 0.05 | 0.04 * |
| L2 | 0.22 ± 0.09 | 0.22 ± 0.08 | −0.01 ± 0.04 | 0.47 | |
| ARA500 90–270° (mm2) | L1 | 0.21 ± 0.08 | 0.20 ± 0.08 | −0.01 ± 0.04 | 0.09 |
| L2 | 0.21 ± 0.07 | 0.21 ± 0.07 | −0.01 ± 0.04 | 0.61 | |
| ITC index (%) | L1 | 3.26 ± 9.00 | 4.53 ± 12.08 | 1.28 ± 4.53 | 0.19 |
| L2 | 2.62 ± 7.92 | 4.03 ± 9.83 | 1.52 ± 7.99 | 0.15 | |
| SC parameters | |||||
| SC Nasal Lenght (µm) | L1 | 260.56 ± 51.87 | 252.91 ± 43.05 | −8.66 ± 50.57 | 0.36 |
| L2 | 261.51 ± 47.22 | 235.56 ± 37.96 | −25.96 ± 46.60 | 0.01 * | |
| SC Temp Lenght (µm) | L1 | 269.51 ± 54.99 | 261.56 ± 57.87 | −7.96 ± 42.96 | 0.32 |
| L2 | 275.71 ± 54.22 | 249.21 ± 55.76 | −26.50 ± 45.36 | <0.01 * | |
| SC Nasal Area (µm2) | L1 | 5411.11 ± 1603.84 | 4977.78 ± 1637.52 | −433.33 ± 1411.91 | 0.10 |
| L2 | 5777.78 ± 1967.81 | 4733.34 ± 1450.06 | −1044.44 ± 1852.27 | <0.01 * | |
| SC Temp. Area (µm2) | L1 | 6022.22 ± 1909.71 | 5111.11 ± 1749.29 | −911.11 ± 1324.49 | <0.01 * |
| L2 | 5944.45 ± 1830.11 | 5088.89 ± 1623.42 | −855.56 ± 1601.45 | 0.01 * |
| Study Eye (Right Eye) | Control Eye (Left Eye) | ||||||
|---|---|---|---|---|---|---|---|
| Time | IOP (Mean ± SD) | Δ IOP (Mean ± SD) | p | IOP (Mean ± SD) | Δ IOP (Mean ± SD) | p | |
| L1 | BL | 11.09 ± 1.66 | - | - | 11.14 ± 1.75 | - | - |
| AL | 11.54 ± 2.82 | 0.46 ± 1.07 | 0.02 * | 11.09 ± 1.66 | −0.06 ± 0.77 | 0.87 | |
| L2 | BL | 11.02 ± 1.63 | - | - | 11.61 ± 1.79 | - | - |
| AL | 11.25 ± 1.86 | 0.23 ± 1.16 | 0.44 | 11.29 ± 1.86 | −0.32 ± 1.16 | 0.04 * | |
| Study Eye (Right Eye) | Control Eye (Left Eye) | ||||||
|---|---|---|---|---|---|---|---|
| Time | IOP (Mean ± SD) | ΔIOP (Mean ± SD) | p | IOP (Mean ± SD) | Δ IOP (Mean ± SD) | p | |
| L1 | BL | 10.70 ± 2.80 | - | - | 9.90 ± 2.92 | - | - |
| 0 h | 11.63 ± 2.82 | 0.93 ± 2.34 | 0.04 | 10.08 ± 3.00 | 0.18 ± 1.32 | 1.00 | |
| 1 h | 12.73 ± 2.87 | 2.03 ± 1.79 | <0.01 * | 10.19 ± 2.93 | 0.29 ± 1.19 | 1.00 | |
| 2 h | 13.25 ± 3.26 | 2.55 ± 2.04 | <0.01 * | 10.07 ± 3.13 | 0.17 ± 1.68 | 1.00 | |
| AL | 10.95 ± 3.15 | 0.24 ± 1.69 | 1.00 | 9.90 ± 2.76 | 0.00 ± 1.31 | 1.00 | |
| L2 | BL | 10.79 ± 2.66 | - | - | 10.56 ± 2.38 | - | - |
| 0 h | 12.02 ± 2.73 | 1.23 ± 1.49 | <0.01 * | 9.96 ± 2.40 | −0.30 ± 1.35 | 1.00 | |
| 1 h | 12.91 ± 2.49 | 2.12 ± 1.99 | <0.01 * | 10.03 ± 2.85 | −0.22 ± 1.86 | 1.00 | |
| 2 h | 13.32 ± 3.22 | 2.53 ± 2.22 | <0.01 * | 10.39 ± 3.20 | 0.13 ± 1.89 | 1.00 | |
| AL | 11.37 ± 2.84 | 0.58 ± 1.38 | 0.29 | 10.57 ± 2.85 | 0.31 ± 1.32 | 1.00 | |
| Study Eye (Right Eye) | Control Eye (Left Eye) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Before (Mean ± SD) | After (Mean ± SD) | Δ (Mean ± SD) | p | Before (Mean ± SD) | After (Mean ± SD) | Δ (Mean ± SD) | p | ||
| L1 | RNFLt (µm) | 107.76 ± 10.60 | 108.04 ± 10.25 | 0.28 ± 2.32 | 0.51 | 109.02 ± 9.90 | 109.04 ± 9.80 | 0.20 ± 2.06 | 0.96 |
| NRA (mm2) | 1.67 ± 0.39 | 1.63 ± 0.42 | −0.04 ± 0.12 | 0.09 | 1.64 ± 0.34 | 1.65 ± 0.35 | 0.01 ± 0.15 | 0.65 | |
| NRV (mm3) | 0.24 ± 0.08 | 0.23 ± 0.09 | −0.01 ± 0.03 | 0.34 | 0.24 ± 0.11 | 0.24 ± 0.11 | 0.00 ± 0.03 | 0.66 | |
| L2 | RNFL (µm) | 106.95 ± 9.50 | 106.70 ± 10.64 | −0.26 ± 2.82 | 0.62 | 108.23 ± 10.35 | 107.93 ± 9.93 | −0.30 ± 3.48 | 0.64 |
| NRA (mm2) | 1.65 ± 0.41 | 1.64 ± 0.42 | −0.01 ± 0.12 | 0.71 | 1.65 ± 0.34 | 1.66 ± 0.34 | 0.01 ± 0.11 | 0.93 | |
| NRV (mm3) | 0.23 ± 0.09 | 0.23 ± 0.09 | 0.00 ± 0.02 | 0.45 | 0.23 ± 0.10 | 0.24 ± 0.11 | 0.01 ± 0.02 | 0.15 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Queiruga-Piñeiro, J.; Barros, A.; Lozano-Sanroma, J.; Fernández-Vega Cueto, A.; Rodríguez-Uña, I.; Merayo-LLoves, J. Assessment by Optical Coherence Tomography of Short-Term Changes in IOP-Related Structures Caused by Wearing Scleral Lenses. J. Clin. Med. 2023, 12, 4792. https://doi.org/10.3390/jcm12144792
Queiruga-Piñeiro J, Barros A, Lozano-Sanroma J, Fernández-Vega Cueto A, Rodríguez-Uña I, Merayo-LLoves J. Assessment by Optical Coherence Tomography of Short-Term Changes in IOP-Related Structures Caused by Wearing Scleral Lenses. Journal of Clinical Medicine. 2023; 12(14):4792. https://doi.org/10.3390/jcm12144792
Chicago/Turabian StyleQueiruga-Piñeiro, Juan, Alberto Barros, Javier Lozano-Sanroma, Andrés Fernández-Vega Cueto, Ignacio Rodríguez-Uña, and Jesús Merayo-LLoves. 2023. "Assessment by Optical Coherence Tomography of Short-Term Changes in IOP-Related Structures Caused by Wearing Scleral Lenses" Journal of Clinical Medicine 12, no. 14: 4792. https://doi.org/10.3390/jcm12144792