
COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
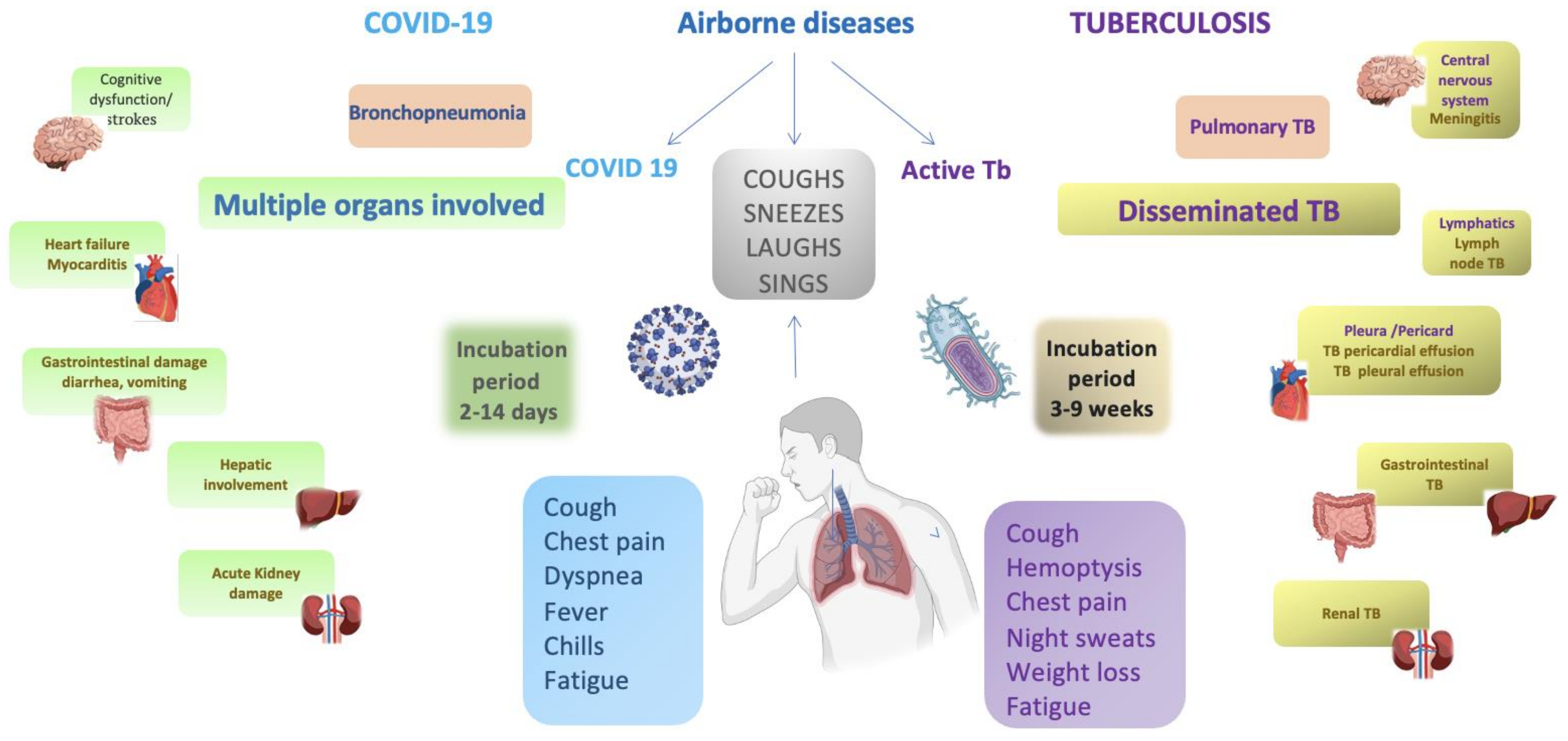
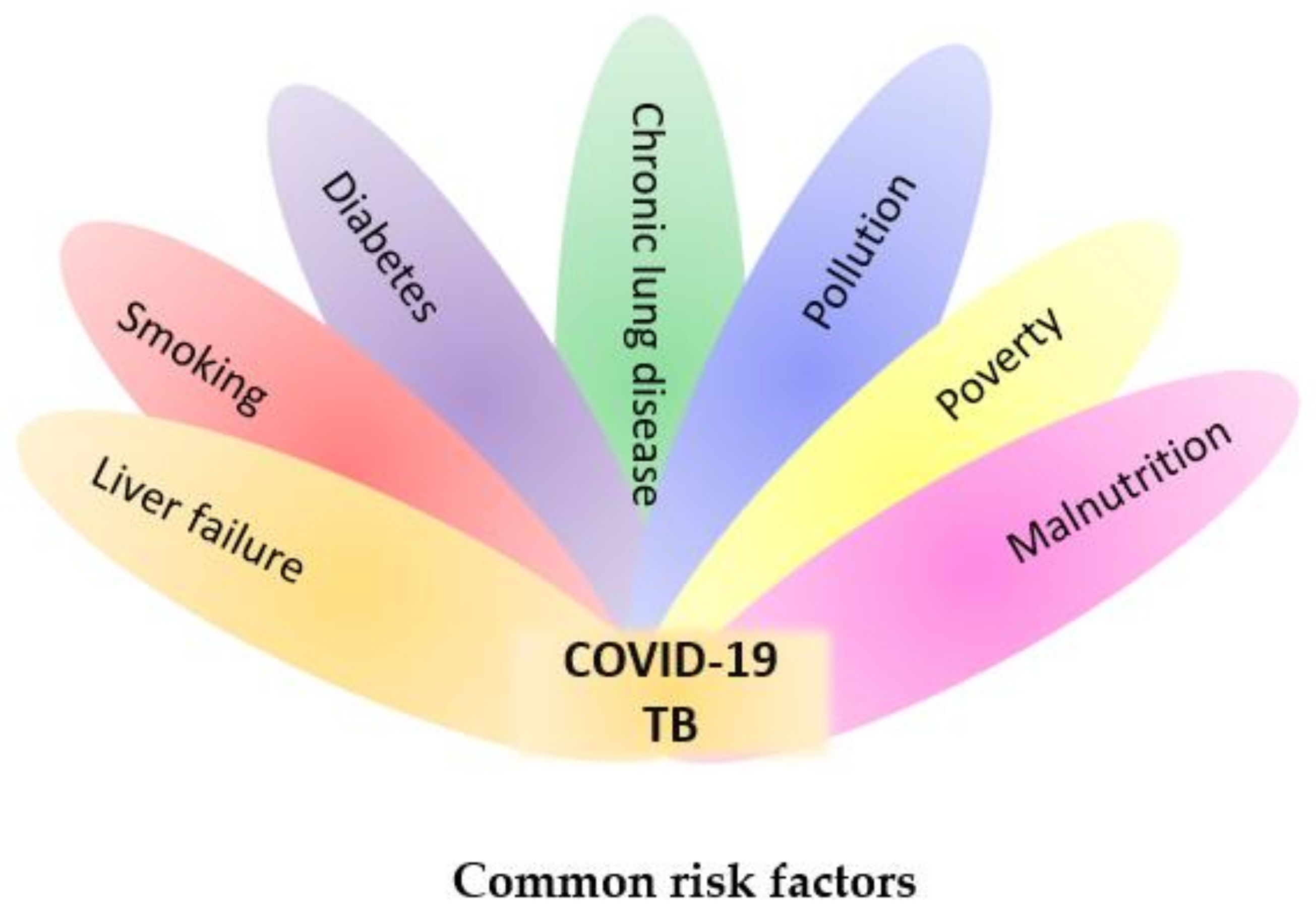
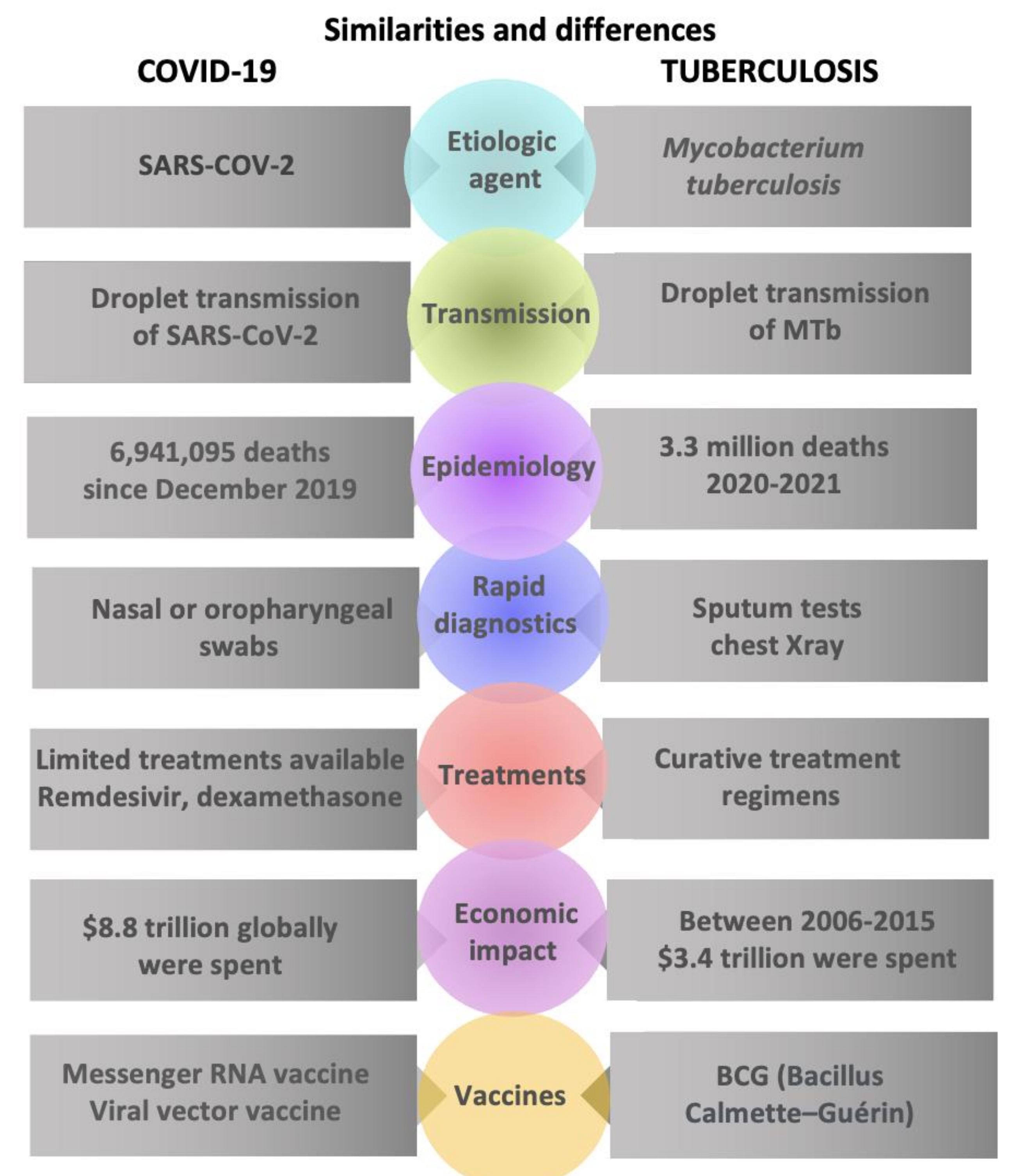
2. Epidemiological Overlap
3. Impact on Diagnosis and Screening
4. Co-Infection and Clinical Management
5. Lessons Learned
6. Looking Forward: Post-Pandemic Challenges for Tuberculosis and Advancements in Vaccine Development
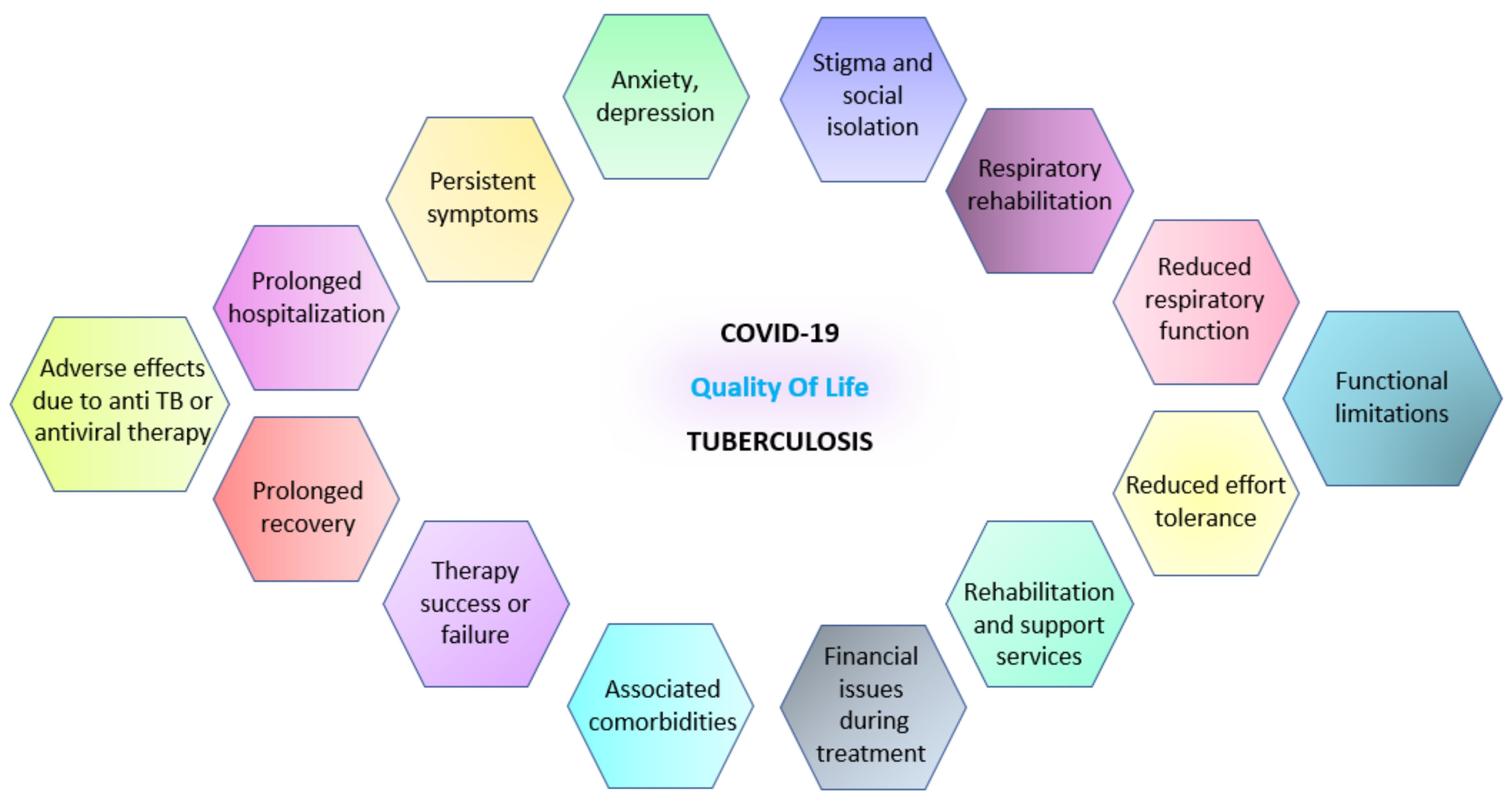
7. Life Quality
7.1. During Infection
7.2. After Infection
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA J. Am. Med. Assoc. 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Dis- ease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.W.M.; Goletti, D. Impact of the global COVID-19 outbreak on the management of other communicable diseases. Int. J. Tuberc. Lung Dis. 2020, 24, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Kasaeva, T.; Swaminathan, S. COVID-19’s devastating effect on tuberculosis care—A path to recovery. N. Engl. J. Med. 2022, 386, 1490–1493. [Google Scholar] [CrossRef]
- Loveday, M.; Cox, H.; Evans, D.; Furin, J.; Ndjeka, N.; Osman, M.; Naidoo, K.; for the National TB Think Tank ‘Optimising TB Treatment Outcomes’ Task Team. Opportunities from a new disease for an old threat: Extending COVID-19 efforts to address tuberculosis in South Africa. S. Afr. Med. J. 2020, 110, 1160–1167. [Google Scholar] [CrossRef]
- Tale, S.; Meitei Soibam, P. Care of tuberculosis patients in the times of COVID-19. Indian J. Tuberc. 2021, 68, 285–286. [Google Scholar] [CrossRef]
- Pai, M. Tuberculosis and COVID-19: Fighting a Deadly Syndemic; Forbes: Jersey City, NJ, USA, 2020; Available online: https://www.forbes.com/sites/madhukarpai/2020/09/26/tuberculosis-and-covid-19-fighting-a-deadly-syndemic/ (accessed on 12 June 2023).
- Trajman, A.; Felker, I.; Alves, L.C.; Coutinho, I.; Osman, M.; Meehan, S.A.; Singh, U.B.; Schwartz, Y. The COVID-19 and TB syndemic: The way forward. Int. J. Tuberc. Lung Dis. 2022, 26, 710–719. [Google Scholar] [CrossRef]
- Hopewell, P.C.; Reichman, L.B.; Castro, K.G. Parallels and Mutual Lessons in Tuberculosis and COVID-19 Transmission, Prevention, and Control. Emerg. Infect. Dis. 2021, 27, 681–686. [Google Scholar] [CrossRef]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Hopewell, P.C. Factors influencing the transmission and infectivity of Mycobacterium tuberculosis: Implication for clinical and public health management of tuberculosis. In Respiratory Infections; Sande, M.A., Root, R.K., Hudson, L.D., Eds.; Churchill Livingstone Inc.: New York, NY, USA, 1986; pp. 191–216. [Google Scholar]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A review of viral, host, and environmental factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Hadler, S.C.; Castro, K.G.; Dowdle, W.; Hicks, L.; Noble, G.; Ridzon, R. Epidemic Intelligence Service investigations of respiratory illness, 1946–2005. Am. J. Epidemiol. 2011, 174, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- A Yates, T.; Khan, P.Y.; Knight, G.M.; Taylor, J.G.; McHugh, T.D.; Lipman, M.; White, R.G.; Cohen, T.; Cobelens, F.G.; Wood, R.; et al. The transmission of Mycobacterium tuberculosis in high burden settings. Lancet Infect. Dis. 2016, 16, 227–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ. Res. 2020, 188, 109819. [Google Scholar] [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 Variants; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/health-topics/typhoid/tracking-SARS-CoV-2-variants (accessed on 12 June 2023).
- Morawska, L.; Milton, D.K. Is it time to address airborne transmission of COVID-19. Clin. Infect. Dis. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Kline, S.E.; Hedemark, L.L.; Davies, S.F. Outbreak of tuberculosis among regular patrons of a neighborhood bar. N. Engl. J. Med. 1995, 333, 222–227. [Google Scholar] [CrossRef]
- Valway, S.E.; Sanchez, M.P.; Shinnick, T.F.; Orme, I.; Agerton, T.; Hoy, D.; Jones, J.S.; Westmoreland, H.; Onorato, I.M. An outbreak involving extensive transmission of a virulent strain of Mycobacterium tuberculosis. N. Engl. J. Med. 1998, 338, 633–639. [Google Scholar] [CrossRef]
- Biswas, S.S.; Awal, S.S.; Awal, S.K. COVID-19 and pulmonary tuberculosis—A diagnostic dilemma. Radiol. Case Rep. 2021, 16, 3255–3259. [Google Scholar] [CrossRef]
- Herrera, M.T.; Guzmán-Beltrán, S.; Bobadilla, K.; Santos-Mendoza, T.; Flores-Valdez, M.A.; Gutiérrez-González, L.H.; González, Y. Human Pulmonary Tuberculosis: Understanding the Immune Response in the Bronchoalveolar System. Biomolecules 2022, 12, 1148. [Google Scholar] [CrossRef]
- Gibson, P.G.; Qin, L. Puah SHCOVID-19 acute respiratory distress syndrome (ARDS): Clinical features differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef]
- Brosnahan, S.B.; Jonkman, A.H.; Kugler, M.C.; Munger, J.S.; Kaufman, D.A. COVID-19 and Respiratory System Disorders: Current Knowledge, Future Clinical and Translational Research Questions. Arter. Thromb. Vasc. Biol. 2020, 40, 2586–2597. [Google Scholar] [CrossRef] [PubMed]
- Aslan, A.; Aslan, C.; Zolbanin, N.M.; Jafari, R. Acute respiratory distress syndrome in COVID-19: Possible mechanisms and therapeutic management. Pneumonia 2021, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, A.J.; Klinton, J.S.; Oga-Omenka, C.; Heitkamp, P.; Nawina Nyirenda, C.; Furin, J.; Pai, M. Tuberculosis in times of COVID-19. J. Epidemiol. Community Health 2022, 76, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R.; Lee, C.T. Identifying and interrupting super spreading events-implications for control of severe acute respiratory syndrome coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1059–1066. [Google Scholar] [CrossRef]
- Patra, K.; Batabyal, S.; Mandal, K.; Ghose, D.; Sarkar, J. Tuberculosis and COVID-19: A combined global threat to human civilization. Clin. Epidemiol. Glob. Health 2022, 15, 101031. [Google Scholar] [CrossRef]
- Carwile, M.E.; Hochberg, N.S.; Sinha, P. Undernutrition is feeding the tuberculosis pandemic: A perspective. J. Clin. Tuberc. Other Mycobact. Dis. 2022, 27, 100311. [Google Scholar] [CrossRef]
- Jassat, W.; Cohen, C.; Tempia, S.; Masha, M.; Goldstein, S.; Kufa, T.; Murangandi, P.; Savulescu, D.; Walaza, S.; Bam, J.-L.; et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV 2021, 8, e554–e567. [Google Scholar] [CrossRef]
- Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa. Risk factors for coronavirus disease 2019 (COVID-19) death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- Singh, P.; Saket, V.K.; Kachhi, R. Diagnosis of TB: From conventional to modern molecular protocols. Front. Biosci. 2019, 11, 38–60. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimi, N.; Delaunay-Moisan, A.; Hill, C.; Le Teuff, G.; Rupprecht, J.F.; Thuret, J.Y.; Chaltiel, D.; Potier, M.C. Screening for SARS-CoV-2 by RT-PCR: Saliva or nasopharyngeal swab? Rapid review and meta-analysis. PLoS ONE 2021, 16, e0253007. [Google Scholar] [CrossRef] [PubMed]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Shaar, B.A.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Meghji, J.; Simpson, H.; Squire, S.B.; Mortimer, K. A systematic review of the prevalence and pattern of imaging defined post-TB lung disease. PLoS ONE 2016, 11, e0161176. [Google Scholar] [CrossRef] [Green Version]
- Cioboata, R.; Nicolosu, D.; Streba, C.T.; Vasile, C.M.; Olteanu, M.; Nemes, A.; Gheorghe, A.; Calarasu, C.; Turcu, A.A. Post-COVID-19 Syndrome Based on Disease Form and Associated Comorbidities. Diagnostics 2022, 12, 2502. [Google Scholar] [CrossRef]
- Hsu, D.; Irfan, M.; Jabeen, K.; Iqbal, N.; Hasan, R.; Migliori, G.B.; Zumla, A.; Visca, D.; Centis, R.; Tiberi, S. Post tuberculosis treatment infectious complications. Int. J. Infect. Dis. 2020, 92, S41–S45. [Google Scholar] [CrossRef] [Green Version]
- Oga-Omenka, C.; Sassi, A.; Vasquez, N.A.; Baruwa, E.; Rosapep, L.; Daniels, B.; Olusola-Faleye, B.; Huria, L.; Adamu, A.; Johns, B.; et al. Tuberculosis service disruptions and adaptations during the first year of the COVID-19 pandemic in the private health sector of two urban settings in Nigeria-A mixed methods study. PLoS Glob. Public Health 2023, 3, e0001618. [Google Scholar] [CrossRef]
- Muñiz-Salazar, R.; Le, T.; Cuevas-Mota, J.; González-Fagoaga, J.E.; Zapata-Garibay, R.; Ruiz-Tamayo, P.S.; Robles-Flores, J.; Garfein, R.S. Impact of COVID-19 on tuberculosis detection and treatment in Baja California, México. Front. Public Health 2022, 10, 921596. [Google Scholar] [CrossRef]
- Bäckdahl, T.; Sharma, M. Knowledge and transmission risk awareness of tuberculosis among the pilgrims attending a religious mass gathering in India: A cross-sectional study. BMC Public Health 2021, 21, 2141. [Google Scholar] [CrossRef]
- Dewi, C.; Barclay, L.; Passey, M.; Wilson, S. Improving knowledge and behaviours related to the cause, transmission and prevention of Tuberculosis and early case detection: A descriptive study of community led Tuberculosis program in Flores, Indonesia. BMC Public Health 2016, 16, 740. [Google Scholar] [CrossRef] [Green Version]
- Malik, A.A.; Hussain, H.; Maniar, R.; Safdar, N.; Mohiuddin, A.; Riaz, N.; Pasha, A.; Khan, S.; Kazmi, S.S.H.; Kazmi, E.; et al. Integrated Tuberculosis and COVID-19 Activities in Karachi and Tuberculosis Case Notifications. Trop. Med. Infect. Dis. 2022, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Ftouni, R.; AlJardali, B.; Hamdanieh, M.; Ftouni, L.; Salem, N. Challenges of Telemedicine during the COVID-19 pandemic: A systematic review. BMC Med. Inform. Decis. Mak. 2022, 22, 207. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens. Int. 2021, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Perveen, S.; Negi, A.; Sharma, R. Evolution of tuberculosis diagnostics: From molecular strategies to nanodiagnostics. Tuberculosis 2023, 140, 102340. [Google Scholar] [CrossRef] [PubMed]
- Lawn, S.D.; Mwaba, P.; Bates, M.; Piatek, A.; Alexander, H.; Marais, B.J.; Cuevas, L.E.; McHugh, T.D.; Zijenah, L.; Kapata, N.; et al. Advances in tuberculosis diagnostics: The Xpert MTB/RIF assay and future prospects for a point-of-care test. Lancet Infect. Dis. 2013, 13, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subbaraman, R.; de Mondesert, L.; Musiimenta, A.; Pai, M.; Mayer, K.H.; Thomas, B.E.; Haberer, J. Digital adherence technologies for the management of tuberculosis therapy: Mapping the landscape and research priorities. BMJ Glob. Health 2018, 3, e001018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; White, R.G. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [CrossRef]
- Cilloni, L.; Fu, H.; Vesga, J.F.; Dowdy, D.; Pretorius, C.; Ahmedov, S.; Nair, S.A.; Mosneaga, A.; Masini, E.; Sahu, S.; et al. The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis. EClinicalMedicine 2020, 28, 100603. [Google Scholar] [CrossRef]
- Hargreaves, J.R.; Boccia, D.; Evans, C.A.; Adato, M.; Petticrew, M.; Porter, J.D. The social determinants of tuberculosis: From evidence to action. Am. J. Public Health 2011, 101, 654–662. [Google Scholar] [CrossRef]
- Chandrasekaran, P.; Saravanan, N.; Bethunaickan, R.; Tripathy, S. Malnutrition: Modulator of Immune Responses in Tuberculosis. Front. Immunol. 2017, 8, 1316. [Google Scholar] [CrossRef] [Green Version]
- VanValkenburg, A.; Kaipilyawar, V.; Sarkar, S.; Lakshminarayanan, S.; Cintron, C.; Prakash Babu, S.; Knudsen, S.; Joseph, N.M.; Horsburgh, C.R.; Sinha, P.; et al. Malnutrition leads to increased inflammation and expression of tuberculosis risk signatures in recently exposed household contacts of pulmonary tuberculosis. Front. Immunol. 2022, 13, 1011166. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; George, A.A.; Sahu, K.K.; Lal, A.; Abraham, G. Tuberculosis and COVID-19 Co-infection: An Updated Review. Acta Biomed. 2020, 92, e2021025. [Google Scholar] [CrossRef] [PubMed]
- Sahu, K.K.; Mishra, A.K.; Martin, K.; Chastain, I. COVID-19 and restrictive lung disease: A deadly combo to trip off the fine balance. Monaldi Arch. Chest Dis. 2020, 90, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Motta, I.; Centis, R.; D’Ambrosio, L.; García-García, J.M.; Goletti, D.; Gualano, G.; Lipani, F.; Palmieri, F.; Sánchez-Montalvá, A.; Pontali, E.; et al. Tuberculosis, COVID-19 and migrants: Preliminary analysis of deaths occurring in 69 patients from two cohorts. Pulmonology 2020, 26, 233–240. [Google Scholar] [CrossRef]
- Tadolini, M.; Codecasa, L.R.; García-García, J.M.; Blanc, F.-X.; Borisov, S.; Alffenaar, J.-W.; Andréjak, C.; Bachez, P.; Bart, P.-A.; Belilovski, E.; et al. Active tuberculosis, sequelae and COVID-19 co-infection: First cohort of 49 cases. Eur. Respir. J. 2020, 56, 2001398. [Google Scholar] [CrossRef]
- Sadanshiv, M.; George, A.A.; Mishra, A.K.; Kuriakose, C.K. Rifampicin-induced immune allergic reaction. Trop. Doct. 2018, 48, 156–159. [Google Scholar] [CrossRef]
- Mishra, A.K.; Sahu, K.K.; Sargent, J. Cardiac drugs and outcome in COVID-19. QJM 2020, 113, 523–524. [Google Scholar] [CrossRef] [Green Version]
- Flores-Lovon, K.; Ortiz-Saavedra, B.; Cueva-Chicaña, L.A.; Aperrigue-Lira, S.; Montes-Madariaga, E.S.; Soriano-Moreno, D.R.; Bell, B.; Macedo, R. Immune responses in COVID-19 and tuberculosis coinfection: A scoping review. Front. Immunol. 2022, 13, 992743. [Google Scholar] [CrossRef]
- Greiwe, J. Telemedicine Lessons Learned During the COVID-19 Pandemic. Curr. Allergy Asthma Rep. 2022, 22, 1–5. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Omboni, S.; Padwal, R.S.; Alessa, T.; Benczúr, B.; Green, B.B.; Hubbard, I.; Kario, K.; Khan, N.A.; Konradi, A.; Logan, A.G.; et al. The worldwide impact of telemedicine during COVID-19: Current evidence and recommendations for the future. Connect. Health 2022, 1, 7–35. [Google Scholar] [CrossRef] [PubMed]
- Bouabida, K.; Lebouché, B.; Pomey, M.P. Telehealth and COVID-19 Pandemic: An Overview of the Telehealth Use, Advantages, Challenges, and Opportunities during COVID-19 Pandemic. Healthcare 2022, 10, 2293. [Google Scholar] [CrossRef] [PubMed]
- Aghdam, M.R.F.; Vodovnik, A.; Hameed, R.A. Role of Telemedicine in Multidisciplinary Team Meetings. J. Pathol. Inform. 2019, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.A.; DiazGranados, D.; Dietz, A.S.; Benishek, L.E.; Thompson, D.; Pronovost, P.J.; Weaver, S.J. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. Am. Psychol. 2018, 73, 433–450. [Google Scholar] [CrossRef]
- Geese, F.; Schmitt, K.-U. Interprofessional Collaboration in Complex Patient Care Transition: A Qualitative Multi-Perspective Analysis. Healthcare 2023, 11, 359. [Google Scholar] [CrossRef]
- Alene, K.A.; Wangdi, K.; Clements, A.C.A. Impact of the COVID-19 Pandemic on Tuberculosis Control: An Overview. Trop. Med. Infect. Dis. 2020, 5, 123. [Google Scholar] [CrossRef]
- Togun, T.; Kampmann, B.; Stoker, N.G.; Lipman, M. Anticipating the impact of the COVID-19 pandemic on TB patients and TB control programmes. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 21. [Google Scholar] [CrossRef]
- Dheda, K.; Perumal, T.; Moultrie, H.; Perumal, R.; Esmail, A.; Scott, A.J.; Udwadia, Z.; Chang, K.C.; Peter, J.; Pooran, A.; et al. The intersecting pandemics of tuberculosis and COVID-19: Population-level and patient-level impact, clinical presentation, and corrective interventions. Lancet Respir. Med. 2022, 10, 603–622. [Google Scholar] [CrossRef]
- Chavda, V.P.; Soni, S.; Vora, L.K.; Soni, S.; Khadela, A.; Ajabiya, J. mRNA-Based Vaccines and Therapeutics for COVID-19 and Future Pandemics. Vaccines 2022, 10, 2150. [Google Scholar] [CrossRef]
- Brisse, M.; Vrba, S.M.; Kirk, N.; Liang, Y.; Ly, H. Emerging Concepts and Technologies in Vaccine Development. Front. Immunol. 2020, 11, 583077. [Google Scholar] [CrossRef]
- Luca, S.; Mihaescu, T. History of BCG Vaccine. Maedica 2013, 8, 53–58. [Google Scholar] [PubMed]
- Fritschi, N.; Curtis, N.; Ritz, N. Bacille Calmette Guérin (BCG) and new TB vaccines: Specific, cross-mycobacterial and off-target effects. Paediatr. Respir. Rev. 2020, 36, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Kuan, R.; Muskat, K.; Peters, B.; Lindestam Arlehamn, C.S. Is mapping the BCG vaccine-induced immune responses the key to improving the efficacy against tuberculosis? J. Intern. Med. 2020, 288, 651–660. [Google Scholar] [CrossRef]
- Andersen, P.; Doherty, T. The success and failure of BCG—Implications for a novel tuberculosis vaccine. Nat. Rev. Microbiol. 2005, 3, 656–662. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.; Sulaiman, S.A.; Shafie, A.A.; Asif, M.; Sarfraz, M.K.; Low, H.C.; Babar, Z.U. Impact of tuberculosis treatment on health-related quality of life of pulmonary tuberculosis patients: A follow-up study. Health Qual. Life Outcomes 2014, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visca, D.; Tiberi, S.; Pontali, E.; Spanevello, A.; Migliori, G.B. Tuberculosis in the time of COVID-19: Quality of life and digital innovation. Eur. Respir. J. 2020, 56, 2001998. [Google Scholar] [CrossRef]
- Daniels, K.J.; Irusen, E.; Pharaoh, H.; Hanekom, S. Post-tuberculosis health-related quality of life, lung function and exercise capacity in a cured pulmonary tuberculosis population in the Breede Valley District, South Africa. S. Afr. J. Physiother. 2019, 75, 1319. [Google Scholar] [CrossRef]
- Al-Kayali, R.S.; Kashkash, M.F.; Alhussein Alhajji, A.H.; Khouri, A. Activation of tuberculosis in recovered COVID-19 patients: A case report. Ann. Med. Surg. 2023, 85, 280–283. [Google Scholar] [CrossRef]
- Visca, D.; Ong, C.W.M.; Tiberi, S.; Centis, R.; D’Ambrosio, L.; Chen, B.; Mueller, J.; Mueller, P.; Duarte, R.; Dalcolmo, M.; et al. Tuberculosis and COVID-19 inter-action: A review of biological, clinical and public health effects. Pulmonology 2021, 27, 151–165. [Google Scholar] [CrossRef]
- Nightingale, R.; Carlin, F.; Meghji, J.; McMullen, K.; Evans, D.; van der Zalm, M.M.; Anthony, M.G.; Bittencourt, M.; Byrne, A.; du Preez, K.; et al. Post-TB health and wellbeing. Int. J. Tuberc. Lung Dis. 2023, 27, 248–283. [Google Scholar] [CrossRef] [PubMed]
- Meghji, J.; Lesosky, M.; Joekes, E.; Banda, P.; Rylance, J.; Gordon, S.; Jacob, J.; Zonderland, H.; MacPherson, P.; Corbett, E.L.; et al. Patient outcomes associated with post-tuberculosis lung damage in Malawi: A prospective cohort study. Thorax 2020, 75, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Everaerts, S.; Heyns, A.; Langer, D.; Beyens, H.; Hermans, G.; Troosters, T.; Gosselink, R.; Lorent, N.; Janssens, W. COVID-19 recovery: Benefits of multidisciplinary respiratory rehabilitation. BMJ Open Respir. Res. 2021, 8, e000837. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sánchez-Alcaraz Martínez, B.J.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Mills, T.; Marks, E.; Reynolds, T.; Cieza, A. Rehabilitation: Essential along the Continuum of Care. In Disease Control Priorities: Improving Health and Reducing Poverty, 3rd ed.; Jamison, D.T., Gelband, H., Horton, S., Jha, P., Laxminarayan, R., Mock, C.N., Nugent, R., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; Chapter 15. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525298/ (accessed on 12 June 2023).




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cioboata, R.; Biciusca, V.; Olteanu, M.; Vasile, C.M. COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective. J. Clin. Med. 2023, 12, 4784. https://doi.org/10.3390/jcm12144784
Cioboata R, Biciusca V, Olteanu M, Vasile CM. COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective. Journal of Clinical Medicine. 2023; 12(14):4784. https://doi.org/10.3390/jcm12144784
Chicago/Turabian StyleCioboata, Ramona, Viorel Biciusca, Mihai Olteanu, and Corina Maria Vasile. 2023. "COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective" Journal of Clinical Medicine 12, no. 14: 4784. https://doi.org/10.3390/jcm12144784